Unit 3: Helminthes (Cestodes)
57
Lecture 3+4+5+6+7+8 – Order
Cyclophyllidea
Taenia saginata
Synonyms:
Beef tapeworm, Taeniarhynchus saginata.
Disease:
Taeniasis saginata.
Habitat:
Adult tapeworm is attached to the wall of small
intestine of man.
Morphology:
It is white tape like warm adult worm 5 meters long with
1000 -2OOO- proglottids.
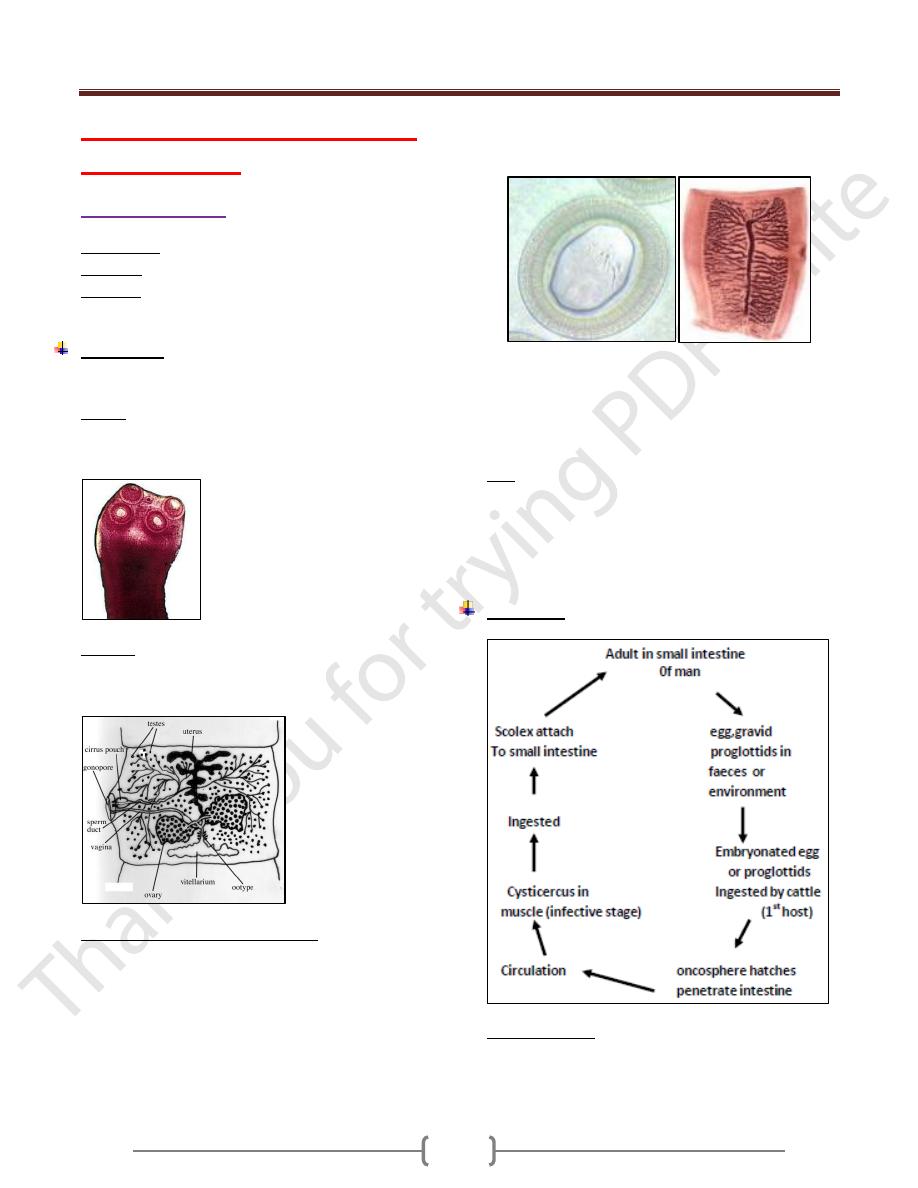
Scolex: pyriform with 4 muscular suckers, no rostellum,
no hooks, there is a slight apical depression (unarmed tape
worms).
Strobila: neck, lmmature proglottids, mature
prohglottidds, about 12 mm in width with a full set of
male and female reproductive organs.
Male & Female Reproducti ve organs :
Ovary, bilobed, vagina, ootype, vitellaria, behind the
ovaries, blind uterus.
Testes, 300-400 follicle, vasa efferentia coiled vas deferense,
cirrus, genital pore on the lateral margin of the segment.
The genital pore on the lateral margin of the segment
alternate irregularly between the right & left margins.
As the segments move towards the posterior end of the
worm, they become more elongated & narrower (gravid.seg.)
In the gravid segment the uterus consist of central
longitudinal stem with 15-20 lateral branches on each side
which intern sub branch.
The terminal proglottid become separated singly or in
small groups and pass out with the stool.
Egg are liberated by rupture of the ripe proglottid 80,000
eggs in single proglottid, infected person can discharge
about 500,000 egg /day.
Egg: spherical 31 to 43 µm in diameter have thin
transparent outer, embryonal envelope .and thick brown
shell, composed of many slender rodes cemented together
, within the shell is a hexacanth embryo , which has 3
pairs of lancet shaped hooklets .
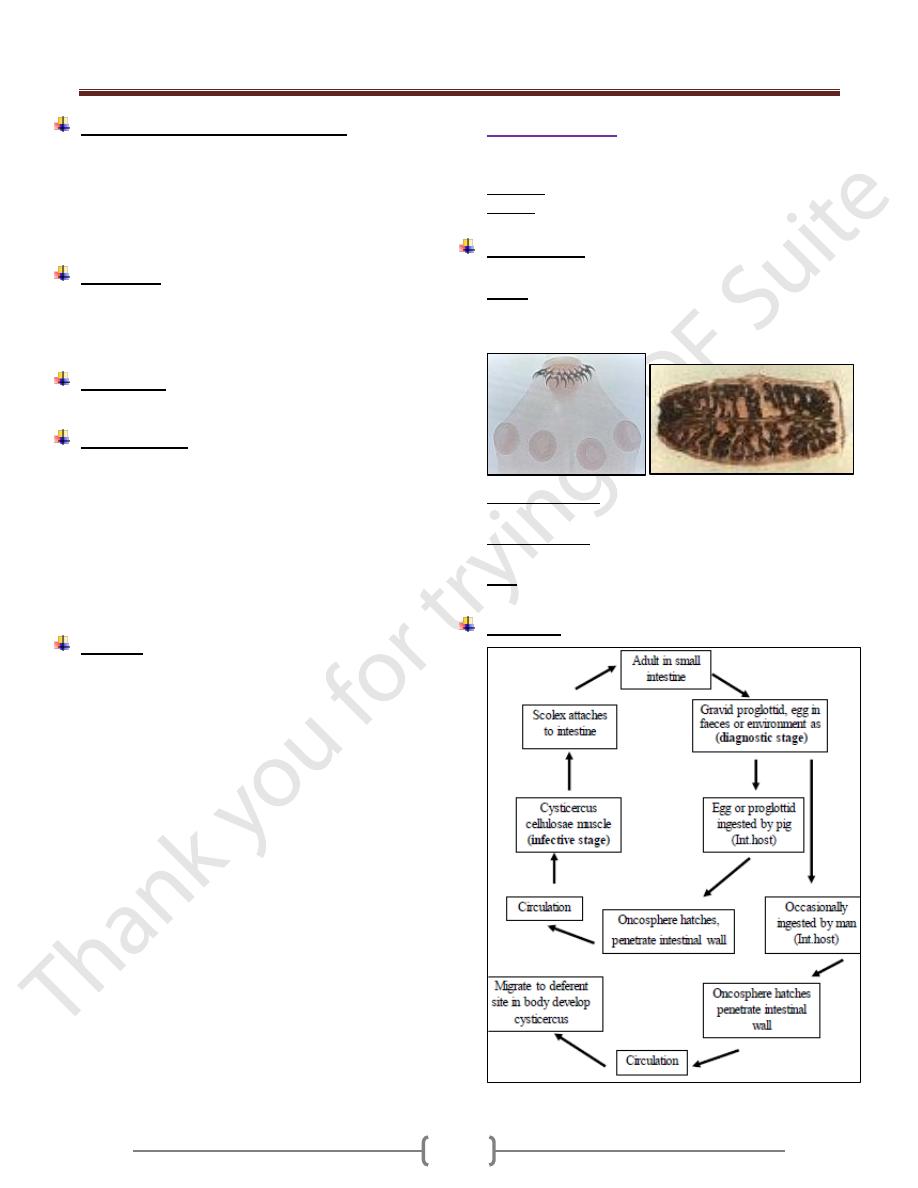
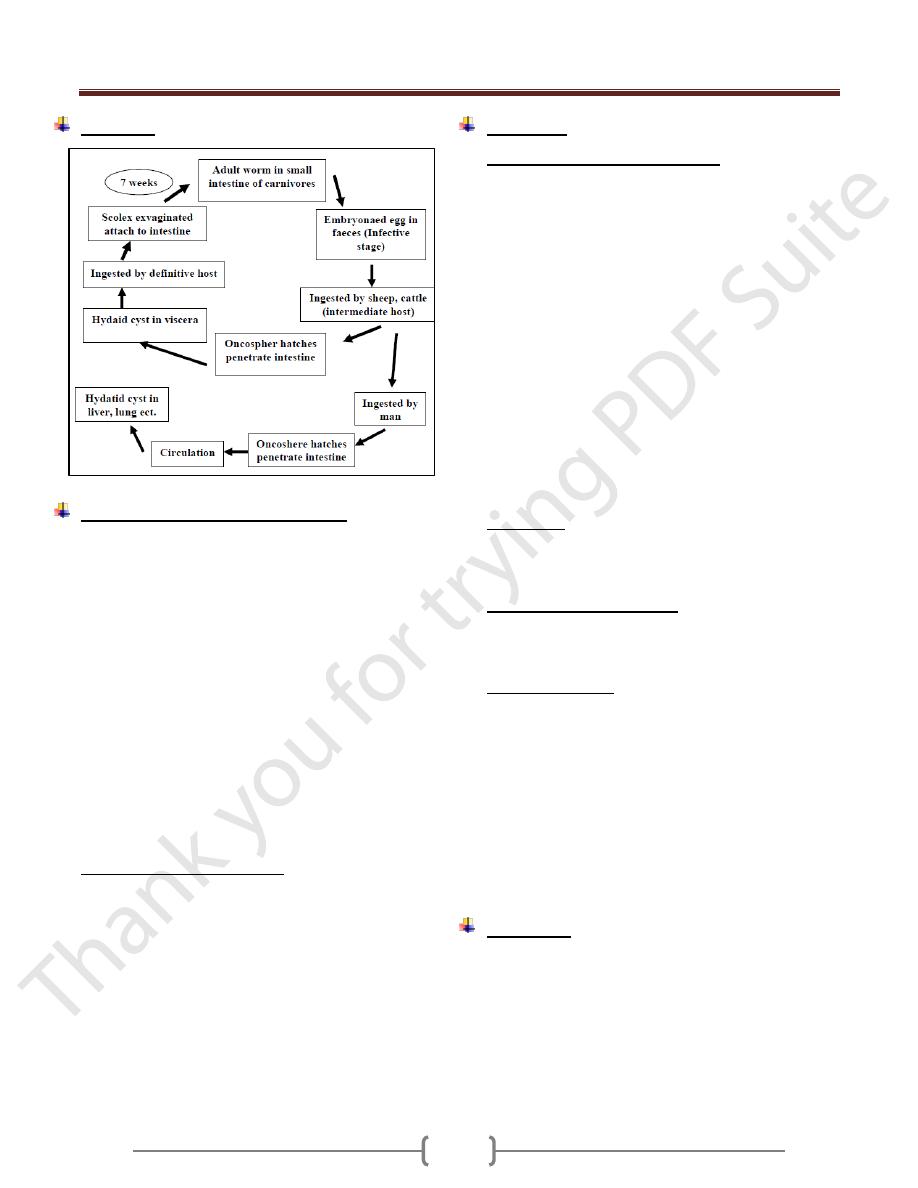
Life Cycle
Cysticercus bovis: Oval, elliptical in shape which
measures 5 by 10 mm and head likes the adult worm,
invaginated into fluid filled bladder. ,
Measly beef: meat that contain cysticercus bovis
Unit 3: Helminthes (Cestodes)
58
Pathogenesis and symptomatology:
Infection with adult T.saginata is without symptoms
Abdominal discomfort
Diarrhea alternate with constipation.
Anorexia, hunger pain.
Intestinal obstruction (rarely)
Diagnosis:
Demonstration of proglottid or egg in faeces.
Serodiagnosis: IHA, IFA, ElISA.
Adhesive cellophane tape technique.
Treatment:
Niclosamide- praziquantel quinacrine hydrochloride
Epidemiology:
Cattle acquire the larval stage of T.saginata by grazing on
moist pasture contaminated with faeces or sewage
containing egg
EGG remains viable for 2 months in natural condition and
for 6 months under optimal condition of moisture & temp.
Man is the only natural definitive host of saginata. Man
acquires the infection by eating uncooked or under
cooked beef containing cysticerci.
Control:
1) Proper disposal of human faeces
2) Workers at cattle feed lots examined periodically for sign
of infection.
3) Thorough cooking of beef before consumption, heating
the meat to 65 degree centigrates is a safe guard.
4) Freezing the beef at -20 degree centigrates for 24 hours
or longer kill the cysticerci.
Taenia Solium
Pork tape worm, armed tape worm,
Disease
: Taeniasis solium , pork , tapewarm infection .
Habitat: small intestine of man.
Morphology:
2-3 meters in length, fewer than 1000 proglottid.
Scolex: Globular in shape, 4 suckers, of alternating large
and small hooks 22 to36 in number and measuring 140 to
200 µm and 100 to 150-µm long.
Mature proglottids: are wider than long and nearly
identical to those of T.saginata, Testes 150-200 follicles.
Gravid Segments: longer than wide, have a uterus, the
medial stem with 9 to 10 lateral branches.
Eggs: are morphologically similar to that of T.saginata
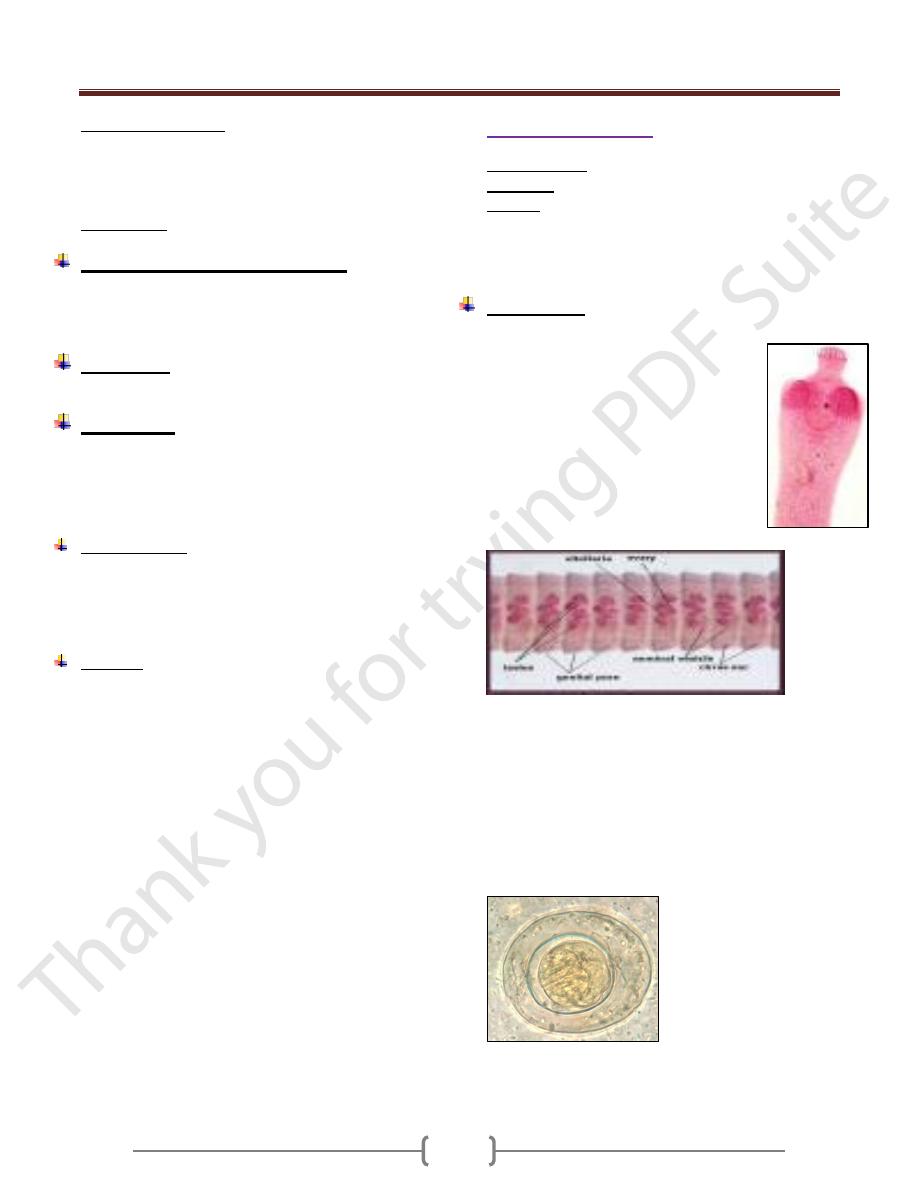
Life cycle
Unit 3: Helminthes (Cestodes)
59
Cysticercus cellulosae: Pearly white, measuring 5 mm
by 8 to 10 mm, the scolex deeply invaginated into fluid
filled bladder is provided with 4 suckers and a rostellr as
in adult is provided with 4 suckers and a rostellum as in
adult worm.
Measley pork: pork containing cysticercus cellulosae.
Pathogenesis and symptomatology:
Infectin with the adult T.solium produce the same clinical
manifestations as infection with T.saginata.
However , no intestinual obstruction.
Diagnosis:
Similar to that of T.saginata
Treatment:
Niclosamide , Praziquantel are the drug of choice
However Niclosamide is not recommended causes the
proglottids to disintegrate releasing the eggs to the bowel
lumen.
Epidemiology:
Human infection with adult T. solium results from
eating raw pork containing Cysticercus cellulosae.
Man is the only natural host of the adult worm. Man is
also a suitable host for the cysticercus.
Control:
Sanitary disposal of human faeces , Treatment of
infected person , Thorough cooking of pork or held in
a deep freeze for at least 24 hrs .
Hymenolepis nana
Common name: Dwarf tape worm
Synonyms: Vampirolepis nana
Disease: Hymenolepiasis nana, Dwarf tape worm
infection. Hymenolepiasis nana is an infection by adult
and larval stage of H. nana. It is found warld wide,
primarily limited to children in warm climate.
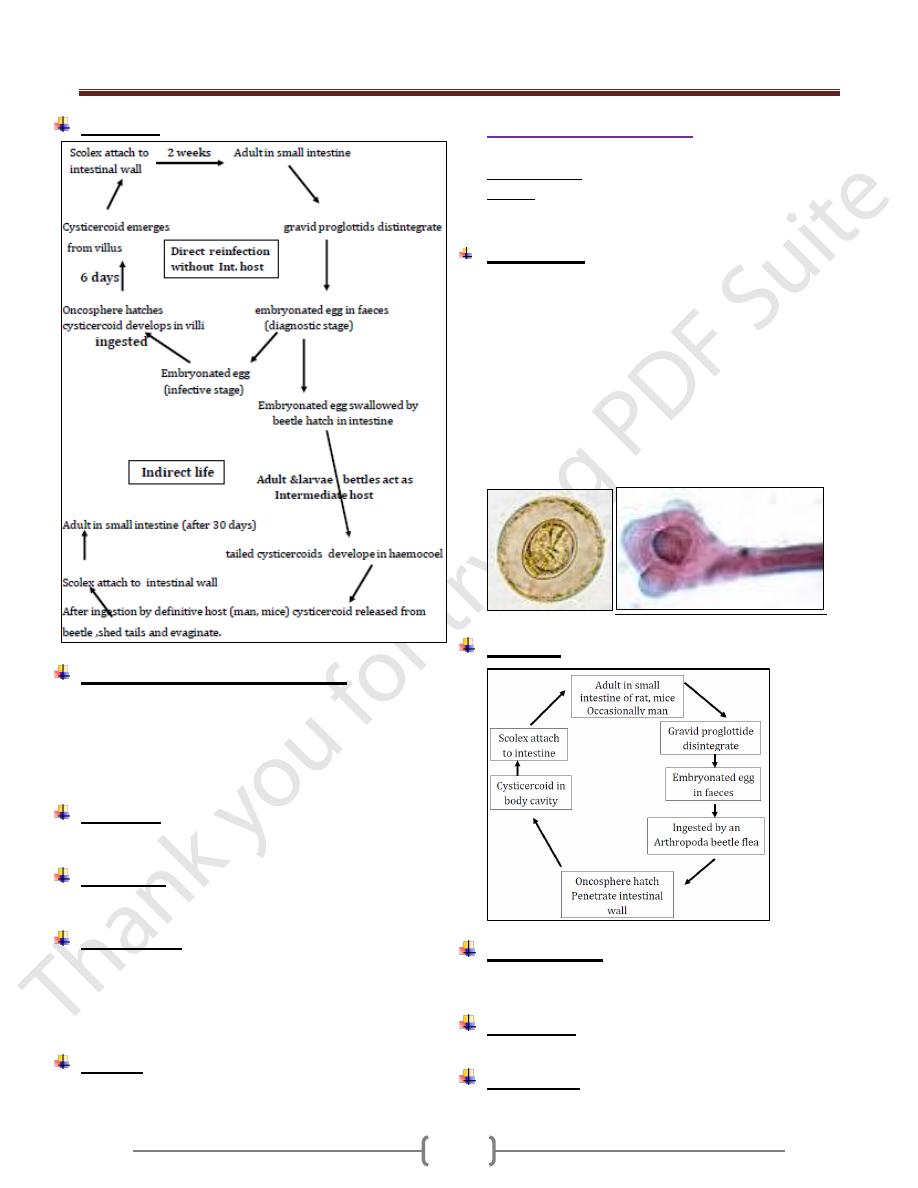
Morphology:
Small 25 to 4o mm in length, 1 mm in breadth
Scolex: Small, globular with short rectactile
rostellum, 4 sucker s and a single ring of 2o
to 3o minute hooklets
Strobila: 2oo segments, broader than long
Mature proglottids: single genital pore on
one side of segment
There are 3 round testes lie in the posterior
part of each segment, Bilobed ovary lie
posteriorly between the testes with compact
vitelline gland behind.
Gravid uterus forms a sac filled with eggs. Gravid
segment destroyed in the intestine releasing the eggs
which are found in faeces.
Egg: nearly spherical 3o _ 47 µ m in diameter. with two
thin membranous shell s . The inner one with 2 polar
thickenings, each provided with 4 to 8 long thread like
filaments extending into the space between the inner and
outer shells. The centrally located hexacanth embryo is
equipped with 3 pairs of hooklets
Unit 3: Helminthes (Cestodes)
60
Life Cycle
Pathogenesis and symptomatology:
Infection with H. nana produces No symptoms in light
infection or may be diarrhea, anorexia, vomiting, loss of
weight, pruritus of the nose and anus, urticaria.
Heavy infection causes diarrhea, abdominal pain,
anorexia and nervous disorders.
Diagnosis:
By demonstration of the egg in the stool.
Treatment:
Niclosamide is the drug of choice in a course of 5-7 days
Epidemiology:
Infection iscommonly acquired by anus to mouth
transmission of eggs. (Hand, food) is more common in
children.
Occasional infection may occur from rodent source.
Control:
a) Good personal hygiene and sanitation
b) Treatment of infected person.
Hymenolepis dimenuta
Common name: Rat tape worm infection
Habitat: in the small intestine of Rat and mice and
rarely in Human.
Morphology:
2o-6O Cm in length by 3.5 to 4.o mm in width, with
1,ooo proglottids
Scolex: o.4 mm wide with 4 suckers and retractable and
un armed rostellum.
Proglottids as in H.Nana.
Egg: Ovoid to sub spherical 72 to 86 µm by 6o to 79
µm with a space between the outer tanned egg
membrane and the hyaline inner membrane which
provided with a pair of pollar thickenings but lack the
polar filaments.
Life cycle
Pathogenesis:
Nonpathogenic but may produce mild diarrhea and
abdominal pain.
Diagnosis:
By demonstration of eggs in stool.
Treatment:
Similar to that for H. nana
Unit 3: Helminthes (Cestodes)
61
Epidemiology:
H. diminuta is worldwide in distribution. Human infection
is associated with the contamination of cereals, grains by
infected grain beetles. Infected fleas may transferred to
the mouth by dirty hands.
Control:
1) Eradication of rat around the home.
2) Protection of food such as grain and cereals from rat
dropping and from insect.
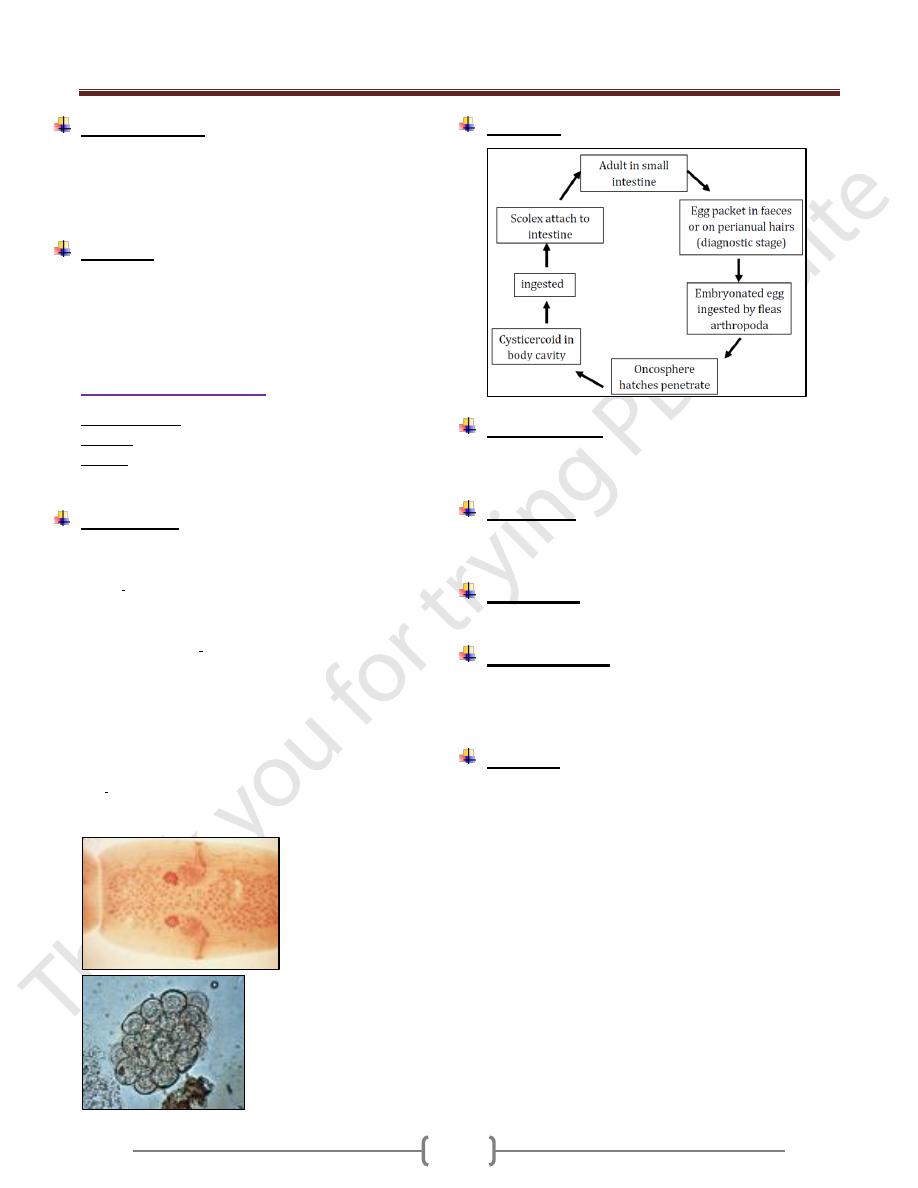
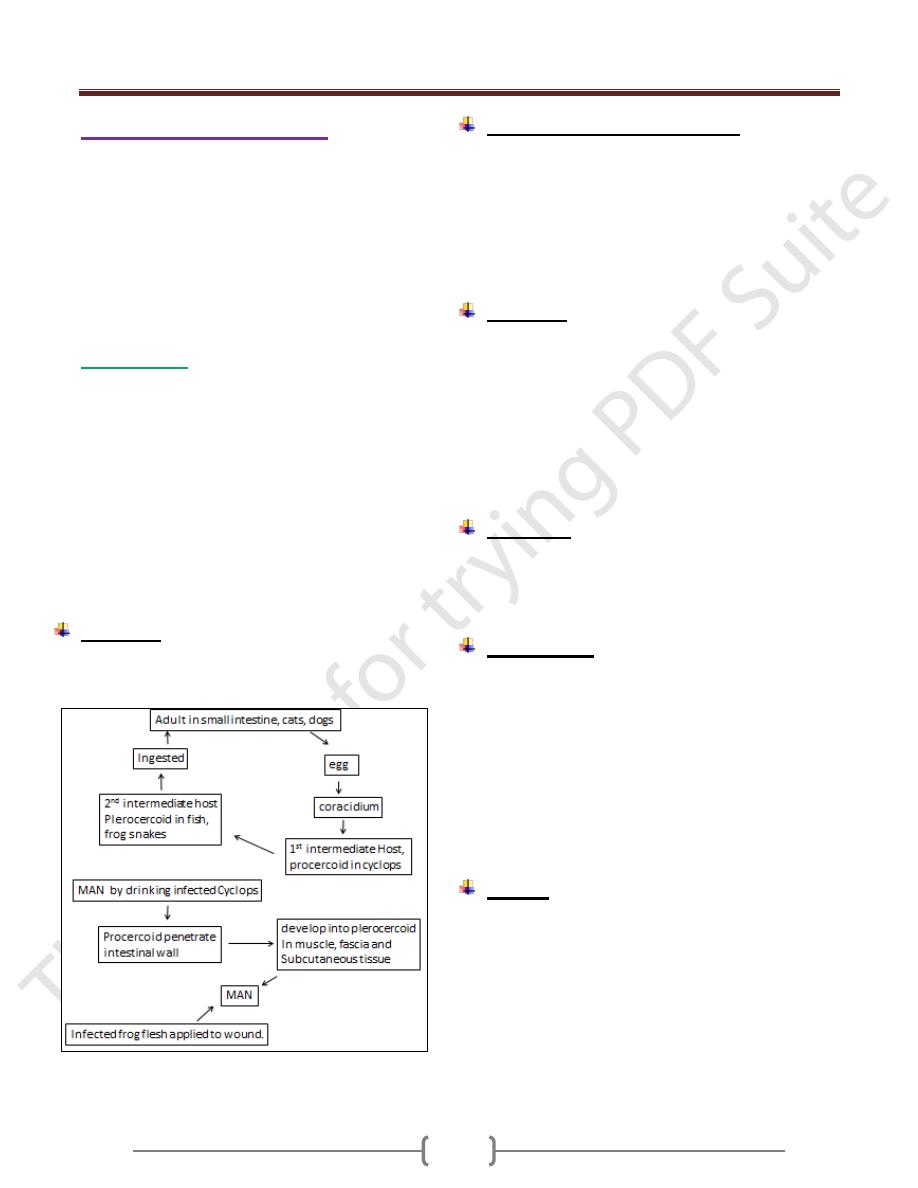
Dipylidium caninum
Common name: Dog / cat tape worm
Disease: Dipylidiasis, dog tape worm infection
Habitat: Adult in the small intestine of dogs and cats.
Occasionally in human mostly in children, infants.
Morphology:
Adult median size 1o _ 7o cm in length, 6o_17o
proglottids.
Scolex: rhomboidal in shape, o.3_ o.5 mm in diameter, 4
suckers, introversible apical club _shape proboscis with 6
rows of minute hooklets.
Mature proglottids: Contain paired reproductive organs
with a genital pore at each lateral margin.
Gravid proglottids:
Resemble cucumber seeds in shape, size. Uterus
disappear early in development and replaced by hyaline ,
non-cellular masses of egg capsules, each egg capsule
filled with 1 to 2 o fully embryonated eggs.
Egg: 3o_ 6o µm in diameter consist of typical 6 hooked
oncosphere .
Life cycle
Pathogenesis:
In a child may produce diarrhea, unrest, sometimes
urticaria, fever, eosinophilia and rarely convulsion.
Diagnosis:
Based on recovery of egg packets or gravid segment in
stool.
Treatment:
Niclosamide, praziquantel, quanacrine hydrochloride.
Epidemiology:
Human infection especially children occur upon ingestion
of the fleas intermediate host, by licking of an infected
dog or cat or by hand to mouth contamination
Control:
1) Infected dogs and cats should be treated.
2) Children should be taught not to let dogs or cats lick
them in their mouth.
Unit 3: Helminthes (Cestodes)
62
Larval tape worm infection
The majority of adult tape worm parasitize the small
intestine of human .The larval stage (meta cestode) and
several spp.of tape worm develop in the extra intestinal
tissue of human (somatic tape worm) namely cysticercus
of T.solium ,coenurus of T.multiceps ,hydatid cyst of
Echinococcus granulosus and sparganum (plerocercoid)
of spirometra spp .
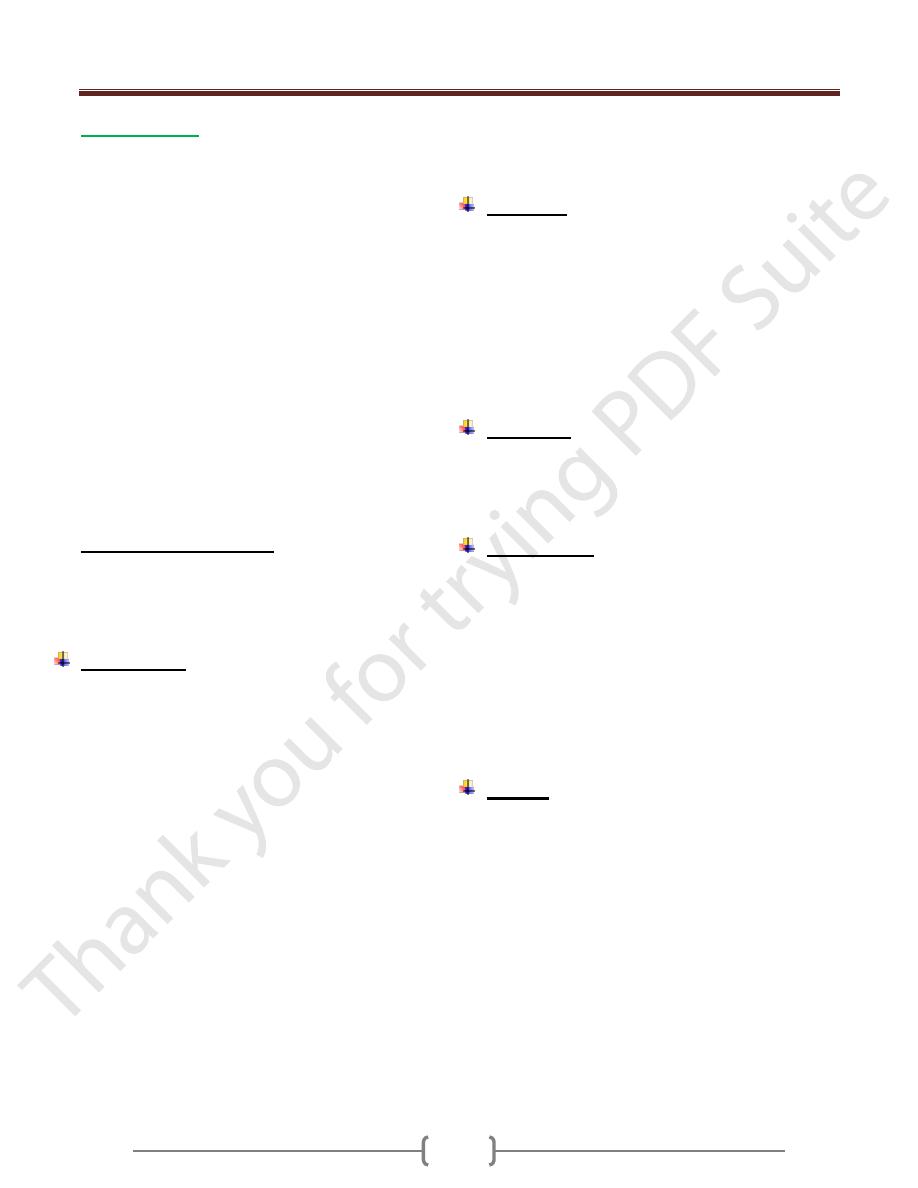
Sparganosis:
The plerocercoid larvae or spargana of spieces of
pseudophyllidea .tape worm may infect human & cause
sparganosis.
Most of spargana reported in human are believed to be "
spirometra mansoni " and other spieces.
Cats ,dogs and related wild animals are definitive host
Copepods Cyclops being the 1
st
intermediate host
Several spp.of vertebrates, fish, frog &snakes as 2
nd
intermediate host.
Human infection occurs by swallowing a procercoid in a
copepod or a plerocercoid in 2
nd
int.host.
Life cycle:
the life cycle of Spirometra species follows the same
pattern as that of Diphyllobothrium sp.
Pathogenesis & Symptomatology:
Little host tissue reaction occurs in the early stages later
in the infection, the area around the worm become
edematous & painful to the touch.
Death of the parasite result in marked inflammation with
local eosinophilia and charcot leyden crystal.
Ocular sparganosis: intense pain, irritation, excessive
lacrymation & edema.
Diagnosis:
1) Biopsy: typical worm structure can be seen by biopsy
(subcutaneous cyst).
2) Speices.diagnosis: can be made by feading a living
sparganum to cat or dog and subsequentelly examinating
the adult worm.
3) Serodiagnosis:
a. Indirect IF Ab test.
b. agar gel diffusion
c. Indirect haemagglutination test
Treatment:
Consist of surgical removal of the sparganum from the
tissue.
Infection about the eye treated with injection of 2-4 ml of
4% ethyl alcohol with procaine (epinephrine –free).
Epidemiology:
Man becomes infected by:
1) Swallowing infected Cyclops in drinking water from
pond, stream, lake).
2) Eating raw infected frog, snakes, small mammals.
3) Applying plerocercoid infected flesh of frog or snakes for
treatment of inflamed eye or finger
In such case, larvae migrate into human tissue and
encysted in various parts of the body.
4) human infection is also acquired from eating raw pork as
sparganum develop also in pigs
Control:
1) drinking only safe waer
2) Eating only well-cooked flesh of animals.
Unit 3: Helminthes (Cestodes)
63
Cysticercosis:
Is an infection by the larval stage of T.solium, the pork
tape worm refered to as cysticercous cellulosae
Man is the definitive host.
Pig is the intermediate host in which the hexacanth
embryo hatch from egg and develop into cysticercus
cellulosae or bladder worm.
Man is also satisfactory host for development of this
larvae .So man may serve as intermediate host when egg
is ingested by mouth, hatch in the small intestine,
liberated oncosphere burrow into the mucosal circulation
& carried to different organs & tissues producing (human
cysticercosis)
The fully developed cysticercus is a small ovoid ,smooth
bladder or cyst filled with fluid & measure 5 mm x 10
mm in size ,developed from the inner wall is single
invaginated scolex with 4 sucker & a double circular
crown of hooks (9-10weeks to develops)
Dead cysicercus possess a cloudy fluid and yellowish
color scolex.
Racemose Cysticercus:
This type is unencapsulated larva with numerous branches
reaching length of 15cm .It is only seen in CNS mainly in
the ventricular and subarachnoid spaces at the base of the
brain.
Pathogenesis:
The most common location of cysticerci inhuman body is
the CNS followed by muscle, subcutaneous tissues, eye,
lung, heart, liver and other visceral location.
Cysticerci survive in man for 4 to 5 years
The clinical feature depends on their location and the
number. Except in the brain and eye, live cysticerci are
surrounded by a tough adventitious.
Cysticerci in human are surrounded by a tough
adventitious capsule which allow them to be detached
easily from the surrounding tissue.
Cysticerci that develop in the subcutaneous and muscle
tissue cause no pain.
Symptom result from the death of larvae in the visceral
organs .With the death of the parasite cyst capsule
distended with fluid ,increase in size replaced by fibrous
tissue or undergo calcification and surrounded by capsule
of Connective tissues.
Cysticerci in brain cause:
Epileptic, seizures, hydrocephalus, stroke also severe
headaches, nausea, vomiting, dizziness, diplopia and
psychic changes.
Living cysticerci (race mose type) in the eye cause
damage to any tissue of the eye ball resulting in uveitis,
iritis, detachment of the retina, atrophy of the choroid.
Diagnosis:
1) Biopsy: surgical removal of the nodule and doing
histopathological examination.
2) Radiology: calcified larvae on x-ray film of muscle.
ocular cyst can be detached by ophthalmoscopy.
computed tomography of the brain for neurocysticercus .
3) Serological test: CFT (Complement Fixation Test), IHA
haemaglutination test, ELISA, immune electrophoresis
are used. using purified Ag and crude Ag ( extract of pig
cysticerci)
Treatment:
Syrgical removal of the cyst is useful in treating some
ocular or cerebral cases.
Chemotherapy: praziquantel following or accompanying
administration of corticosteroid is effective.
Epidemiology:
Human acquired infection of cysticercus by:
1) Accidental ingestion of eggs of T.solium in contaminated
food or drink (heteroinfection) .It is the usual mode of
transfer.
2) Anus to finger to mouth contact & that called external
autoinfection.
3) Internal autoinfection: gravid proglottids. in infected
person with T.solium detached from strobila and
regurgitated into stomach as a result of reverse peristalsis
then return to the duodenum.
Control:
1) Early detection & treatment of case of T .solium.
2) Improvement in sanitation.
3) Good personal hygiene.
4) Adequate cooking as prior freezing of pork to prevent
infection with the adult worm.
Unit 3: Helminthes (Cestodes)
64
Hydrated disease (hydatidosis),
Echinococcosis
The larval stage of species of the tape worm
Echinococcus is known as the hydatid cyst , several
species occur in human
Echinococcus granulosus
Common name: dog tape worm, hydatid tape worm.
Disease: unilocular hydatid disease.
Geographic distribution: Echinococcus granulosus
widely distributed throughout temperate and subtropical
regions ,commonly in sheep and cattle raising countries.
Human infection is common in south America ,parts of
Africa and Europe ,the middle east ,southern Australia,
New Zealand ,extensive area of Asia , south western
united states , Canada.
Habitat :
Man harbours the larval form (hydatid cyst ) specially in
liver and lungs
Adult worm is found in the small intestine of dog and
other canines.
Morphology:
Adult worms are small in size up to 6 mm long,
Scolex: pyriform in shape, has a rostellum with 28 to 50
hooks in 2 rows and 4 suckers.
Strobila: with neck ,one immature ,one mature and one or
two gravid proglottids
Mature segment: with male and female genital organ,
male with 45-65 testes.
Gravid segment: measures more than half the total length
of the whole tape worm with sac like uterus.
Eggs: spherical , 31-40 –m in diameter ,morphologically
similar to those of either taeniid species of dog
Outer shell surround ---- with radially striated
embryophore (inner shell) Hexacanth embryo
Morphology of larval stage (Hydatid cyst):
Larval stage found in organs and tissues of herbivorous
host such as sheep, cattle, hogs.
These animals act as Intermediate host
Man also becomes accidentally infected and act as
intermediate host.
The most common site for development of the cyst in man
is liver followed by lungs (about 70% in liver and 25%in
lungs)
Less frequently the spleen, kidneys, heart, bones,
peritoneum and CNS
These are 2 morphologic types in human tissue
1-Unilocular cyst 2-Osseous
1- Unilocular hydatid cyst:
Is a fluid –filled cyst that is spherical in shape
Cross-section of the cyst wall reveals .an external ,milky
white laminated membrane about 1 mm thick without
nuclei and an inner germinal layer
About 10-15 –m in thickness with nuclei. An outer layer
of fibrous connective tissue is formed as a result of host
reaction to the presence and growing of the cyst.
From the inner germinative layer small secondary cysts
develop ,They are known as broad capsules and as they
grow protoscolices develop from their inner wall (A
protoscolex is ovoid scolex with typical 4 sucker ,
rostellum , a double crown of hooklets deeply with drawn
into the post sucker region )
The brood capsules may detach to form daughter cysts,
which with free scoleces, form hydatid sand within the
cyst cavity.
The majority of human hydatids are unilocular ,with a
size depends on the site and on its age
After 12-20 years it may be 15 cm in diameter or more.
(Slowly growing) containing a liter or more of clear
sterile hydatid fluid.
Some cyst fail to develop broad capsules they become
sterile cyst
Multiple cysts in the liver may be the result of multiple
egg infections or the formation of exogenous daughter
cysts as a result of herniation of the germinative layer
before the host response has resulted in a fibrous
connective tissue wall.
2- Osseous hydatid:
This type of hydatid cyst form in bone of man particularly
the long bone—and pelvic arch.
Larval growth in bones is atypical the outer membranes
are not produced and the organism proceeds to grow as a
protoplasmic stream that erodies the cancellous tissues.
Unit 3: Helminthes (Cestodes)
65
Life cycle
Pathogenesis and symptomatology:
Most of the hydatid cysts of the unilocular type, develop
in the liver, infection of the lung is next in prevalence, the
other organs also invaded occasionally
An inflammatory reaction by the host results in the
enveloping of the cyst by a fibrous connective tissue wall.
After years .may die, shrink, calcify
As the cyst grows, pressure and necrosis may result in
the destruction of the normal liver tissue and impaired
liver function.
Leakage or rupture of the cyst causing the liberation of
hydatid sand into the pleural ,peritoneal or pericardial
cavities and the associated dissemination of scoleces
result in multiple secondary hydatid cyst formation .
The antigenic stimulus from the leakage may result in
anaphylactic shock marked allergic reactions with high
eosinophilia.
Rupture of pulmonary cyst cause chest pain, dyspnea,
cough.
Hydatid cyst in the brain produce increasing symptomatic
evidence of an intracranial tumor.
Osseous hydatid: there is minimal response on the part of
the tissue ,so fibrous outer layer is not produce .and there
is extensive bone erosion to a stage at which fracture or
crumbling suddenly occur
Most infection in human begins in childhood and
discovered in adult life.
Diagnosis:
1) Casoni ُ s test (Intradermal test)
Based on the principle of immediate hypersensitivity.
The antigen used is hydatid fluid collected from animal or
human cysts and sterilized by (seitz filter).
0.2 ml of the antigen injected intradermally on one arm---
--and 0.2 ml saline as a control on the other hand.
In positive cases a large wheal about 5 cm in diameter
with multiple pseudopodia appear within 1/2 hr at the test
side and fades away in an hour.
A delayed reaction appears after 18 to 48 hours -----------
Characterized by Oedema and indurations 5-6 cm
surrounding the site of injection .Anegative reaction does
not exclude echinococcal infection.
The test usually becomes positive 8-12 weeks after
infection and remains positive after surgical removal of
cyst from the patients .It is sensitive but not specific as
false +ve reaction occur in many other infection like
cysticercosis
2)
Radiology:
X-ray film demonstrate hydatid cyst in lung, bone, detect
uncalcified cysts.
Ultra sound, CT scan .Magnetic Resonance Imaging (MRI)
3)
Exploratory cyst puncture
:
Needle aspiration of cysts is dangerous because of
possible spillage of the contents causing secondary spread
or anaphylaxis.
4) Serological Tests:
Based on detection of antibodies and antigen in the patient
serum. .useful tests include ELISA , indirect
haemagglutination ,latex agglutination FIA -
immunoelectrophorensis test , the first 3 are highly
sensitive for initial screening of serum .
Specific confirmation of reactive serum can be obtained
with immunoelectrophoresis to detect the diagnostic (arc 5)
Cysticercosis gives cross reacting antibodies to
Echinococcus antigen 5
5)
Histological examination
of removed specimen.
Treatment:
Surgical removal of the cyst .is the most effective
treatment.
If surgical removed is not possible.
Oral therapy with mebendazole is useful ,in a dose of 400-
600 mg 3 times a day for a period of 21 to 30 days.
Unit 3: Helminthes (Cestodes)
66
Epidemiology:
Human infection with hydatid cyst occur in sheep or
(other herbivores) raising area.
Dogs harbor the adult worms,
Sheep or hogs serve as common reservoirs of the larval
stage
Hydatid in cattle is sterile,
Exposure commonly occur in childhood among boys
playing with infected dogs
Hydatid may grow for 5 to 20 years before diagnoses is
made.
Control:
To break the E.granulosus life cycle and subsequently
halt the spread of human disease several preventive
measure are essential.
All infected viscera should be buried or incinerated.
Stray dogs should be destroyed.
Domestic dogs should be periodically dewarmed
Personal hygiene to avoid ingestion of the eggs.
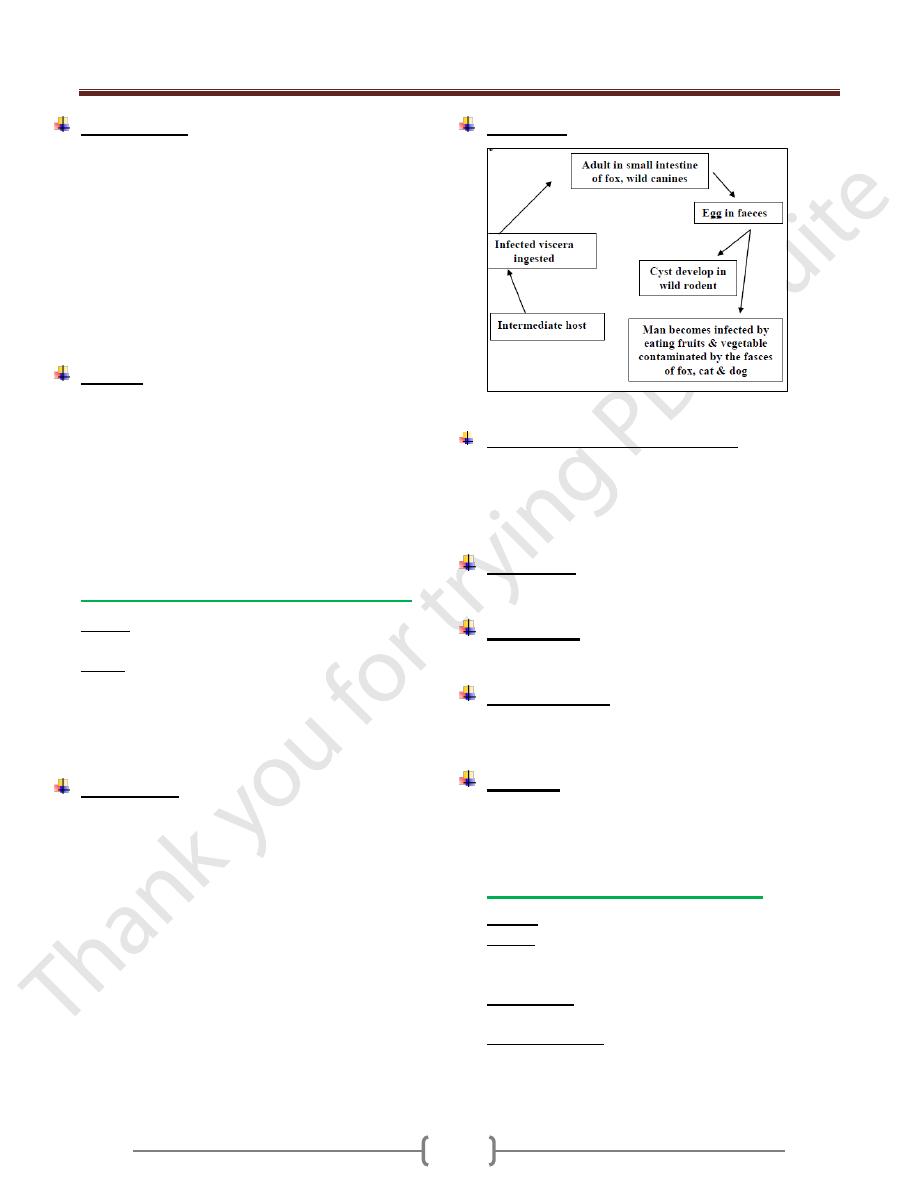
Hydatid of Echinococcus multilocularis
Disease: Alveolar hydatid diseases as multiloculae
hydatid disease.
Habitat: Adult worm E.multilocularis occur in small
intestine of foxes and other wild canines (definitive host)
Natural intermediate host wild mice, in which larval form
recoverd.
Alveolar hydatid in man occur in USSP, Jappan and -------
Morphology:
Adult: smaller than E.granulosus 1.2 to 3.3 mm long and
differ in the position of the genital pore with respect to the
genital organs also in the number of tests 16-29.
Egg: are like other taeniid egg but more resistant to cold
and other environment condition.
Larval form: Alveolar cyst or multiloculares cyst.
The cyst grow by exogenous budding into small irregular
cavities, each within a hyaline membrane, frequently
without fibrous encapsulation, thus there are resultant
metastases through the lymphaties and circulation.
Brood capsule scattered in the cyst
Scolices in the alveolar hydatid in man are few or none.
Most alveolar cyst occur in the liver.
Life cycle:
In general life cycle is similar to that of E.granulosus.
Pathogenesis and symptomatology:
Liver is the most common site to be affected in the
alveolar hydatid cyst .Rarely in lung.
It is a lethal disease.
In human .Intra hepatic portal hypertension results in
Jaundice, ascites, splenomegaly.
Diagnosis:
Biopsy. Ct scan, ultrasound helpful in ascertain the site &
shape. -Immunological test.
Treatment:
Alveolar cyst is not amenable to surgical removal.
Chemotherapy with mebendazole is useful.
Epidemiology:
Infection acquired from eating raw fruits and vegetable
picked off the ground and contaminated with the faeces
of infected foxes and other caniidae .
Control:
Personal hygiene
Good sanitation
Sacrifice of infected animals
Hydatid cyst of Echinococcus vogeli
Disease: Polycystic hydatid disease .
Habitat: in the small intestine of bush dog (definitive
host) in latin America. Rodent, paca (natural intermediate
host).
Morphology: Adult differs from E. granulosus in greater
length 3.9- 5.6 mm and more slender proglottids
Polycystic hydatid: is alveolar in characters but less so
than that of E. multilocularis, so it is intermediate between
cystic and alveolar hydatid disease, present like a mass of
tumor in the liver