Unit 3: Helminthes (Trematodes)
89
Lecture 5+6+7 - Blood Fluke
Schistosoma haematobium:
Schistosomes are digenetic trematodes that inhabit the
blood stream of vertebrate host. So referred as blood
flukes .Schistosome so called because of the (split body)
on the ventral side of the male in which the female is held
during insemination & egg laying.
Disease: Shistosomiasis haemotobia (urinary schistosomiasis
Natural habitat: vesical venules.
Geographical distribution: In Africa ,middle east
Biology:
Sexes are separated .adult worm are delicate & cylindrical
Male: about 10-15 mm in length &1 mm in diameter ,the
tegument is provided with fine tubercle .There is 4-5
small sub globose (testes) behind the acetabulum .There is
a gynecophoric canal on the ventral side of the body .The
muscular male is attached by its sucker to the wall of the
vessels holding the thread-like female in its sex canal.
Female: about 20mm in length &0.25 mm in width .The
genital organ exclusive of the vitellaria occupy the
median longitudinal field.
ovary in the posterior .half of the body.
Uterus –long containing 20-30 eggs
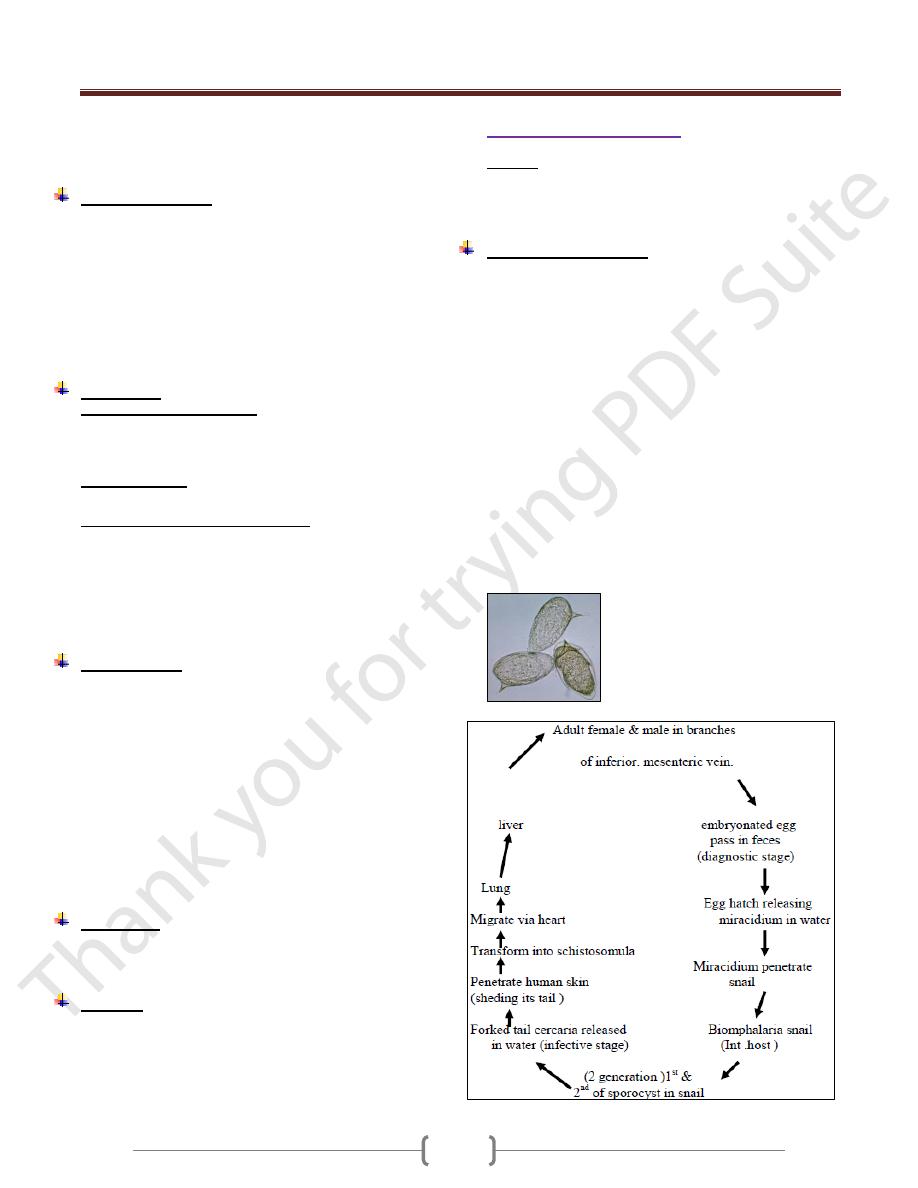
Egg: the mature egg is rounded at one pole &
has a terminal spine at the other .It measure
upto 170-µ--m in length by 70—µm in width
.Straw coloured & relatively transparent.
Holding the female in the sex canal of the
male enable the female to extend its anterior
.extremity into the smaller venules to deposite it ُs eggs.
obstruction of the venules
pressure exerted by the worm
Increase in size of the eggs
hypermotility of the parasitized organ cause the blood
vessel .to repture & discharge the egg into the
surrounding tissue .On oviposition ,the eggs are immature
but when shed from the tissue & excreated .they become
fully embryonated .(maturation takes about one week)
Then the egg is sloughed into the lumen of the bladder &
excreated in the urine.
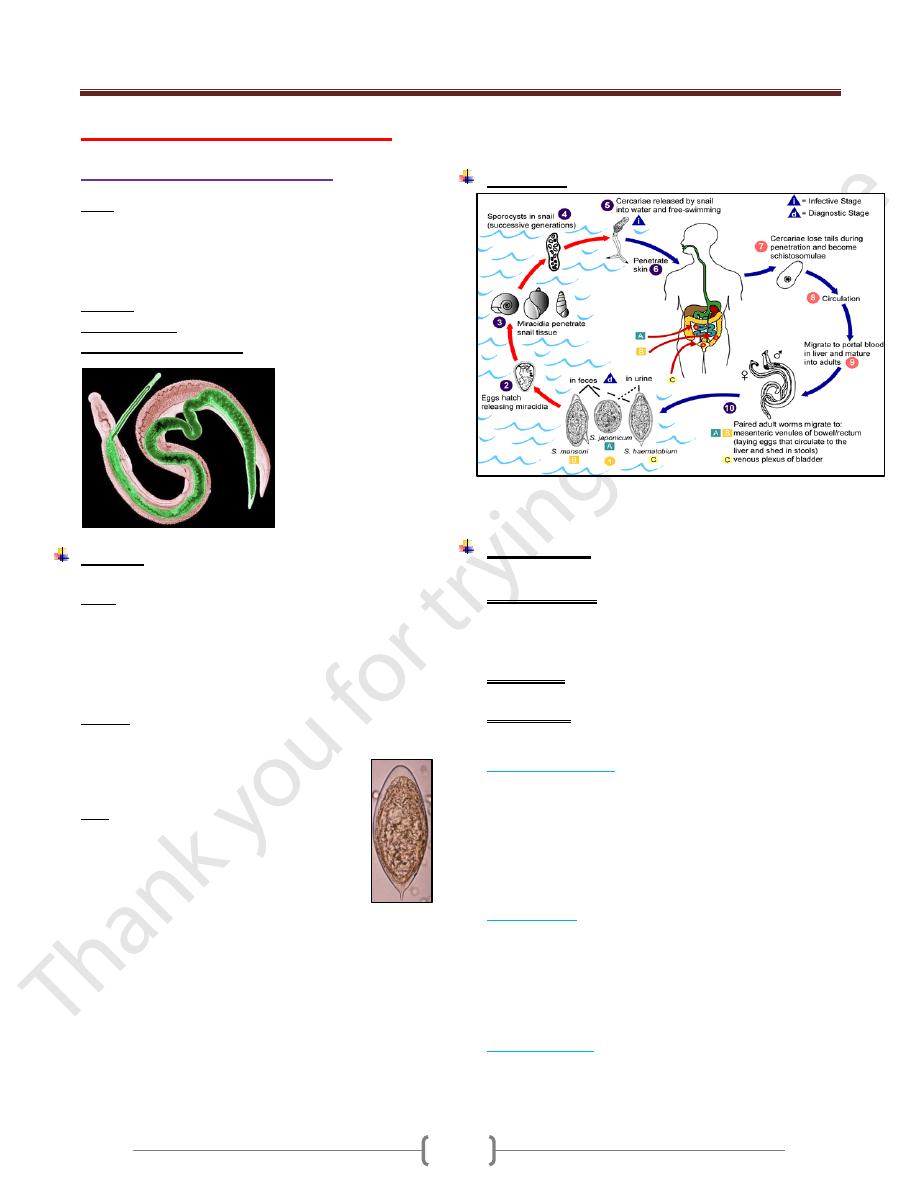
Life cycle:
Egg appears in urine 10-12 weeks after skin penetration.
Sch.haematobium may live 20-30 years
Pathogenesis:
The pathologic changes are divided into 3 consecutive periods
1) Prepatent period: From the skin penetration to the
appearance of eggs in urine .In this period petechial
haemorrhage, popular pruritic rash ,small foci of
eosinophilic & inflammatory changes in the lung & liver
2) Acute stage: when we have active egg deposition &
extrausion
3) chronic stage: which consist of stable egg output, tissue
proliferation & repair
Prepatent period:
Schistosoma dermatitis , resulting from contact with
cercaria of Schistosomes. The lesion composed of initial
Prickling sensation accompanied by erythema and local or
general urticaria then irritation subside leaving a macules ,
but in few hours there is intense itching and papules
formation. The reaction reaches its maximu m between the
2
nd
and 3
rd
day, then gradually decrease.
Acute stage:
Egg deposition and extrusion cause local damage to the
tissue of the rectum or urinary bladder. Ulceration and
irritation of the epithelium of the bladder lead to
formation of Polyps which may undergo malignant
changes. Numerous eggs calcified giving the inner surface
a "sandy appearance" and Calculi may form in the lumen
Chronic stage:
Extensive fibrosis of the bladder wall leads to contraction
of the organ. Fibrosis of the bladder neck obstructs the
Unit 3: Helminthes (Trematodes)
89
flow of urine with the development of hydro ureter and
hydronephrosis which may be associated with bacteriuria.
In Female the vulva is hyper plastic and indurated.
Symptomatology:
During the prepatent period the patients may be
symptomless or may have malaise with late afternoon
fever, moderate hepatic pain or epigastric distress .
If worms mature in the rectal veins there is severe
tenesmus with dysentery.
The first evidence of infection is the painless passage of
blood at the end of micturition, then discharge of pus
cells and necrotic tissue debris , decrease in the interval
between urination and eventually incontinence or Anuria
.
Diagnosis:
1) Urine examination for eggs
* Simple sedimentation (centrifugation)
* Nucleopore filtration method
* Miracidial hatching.
2) Intradermal test:
By using purified extracts of adult worm
3) Serological and Immunological test:
* Indirect immunofluorescence
* Elisa
* Circumoval precipitin
* Cercarien _ hullen reaction
* Radiologic test
* Rectal and Bladder mucosal Biobsy and Cystoscopy.
Epidemiology
Three factors must coincide for transmission to occur:
Presence of the vector snail Bulinus. Man is the only
important definitive host of Sch.
Presence of human infected with the parasite.
Human habit, that lead to urine contamination of fresh
water and to water contact and expos ure to cercaria.
Schistosomiasis haematobia is endemic in Africa, Middle
east,. In Iraq it is distributed in southern parts . After the
extension of irrigation system other areas are included.
Prevalence increase with age peaking at age 15_2o years
then start to decline.
Treatment
Praziquantel (Biltricide) single oral dose 4o mg/ kg.
Side effect: Abdominal discomfort, headache, drowsiness,
backache, fever, sweating, giddiness.
Control:
Effective measures includes
Chemotherapy
Snail control: Biological & chemical
Environmental sanitation.
Health Education
Schistosoma mansoni
Disease: Schistosomiasis mansoni
Manson ُ s blood fluke is a parasite of man occur widely
in Africa, several foci of the Arabian in south America .It
is hyper endemic in the Nile delta (Egypt )
Biology & Life cycle:
Male of S.mansoni measure (6.4-9.9) mm in length &
female (7.2-14)mm
The tegument of the male is provided with numerous
warty excrescences
The number of testes (6-9) form a grape like cluster a
short distance behind the acetabulum.
The most striking internal feature of female is a short
uterus containing very few eggs
The adult worm usually reside in tributaries of the inferior
mesenteric vein adjacent to the lower colon ,they may be
found at higher level of the intestine , in intra hepatic
portal veins ,vesical venules , pulmonary arterioles.
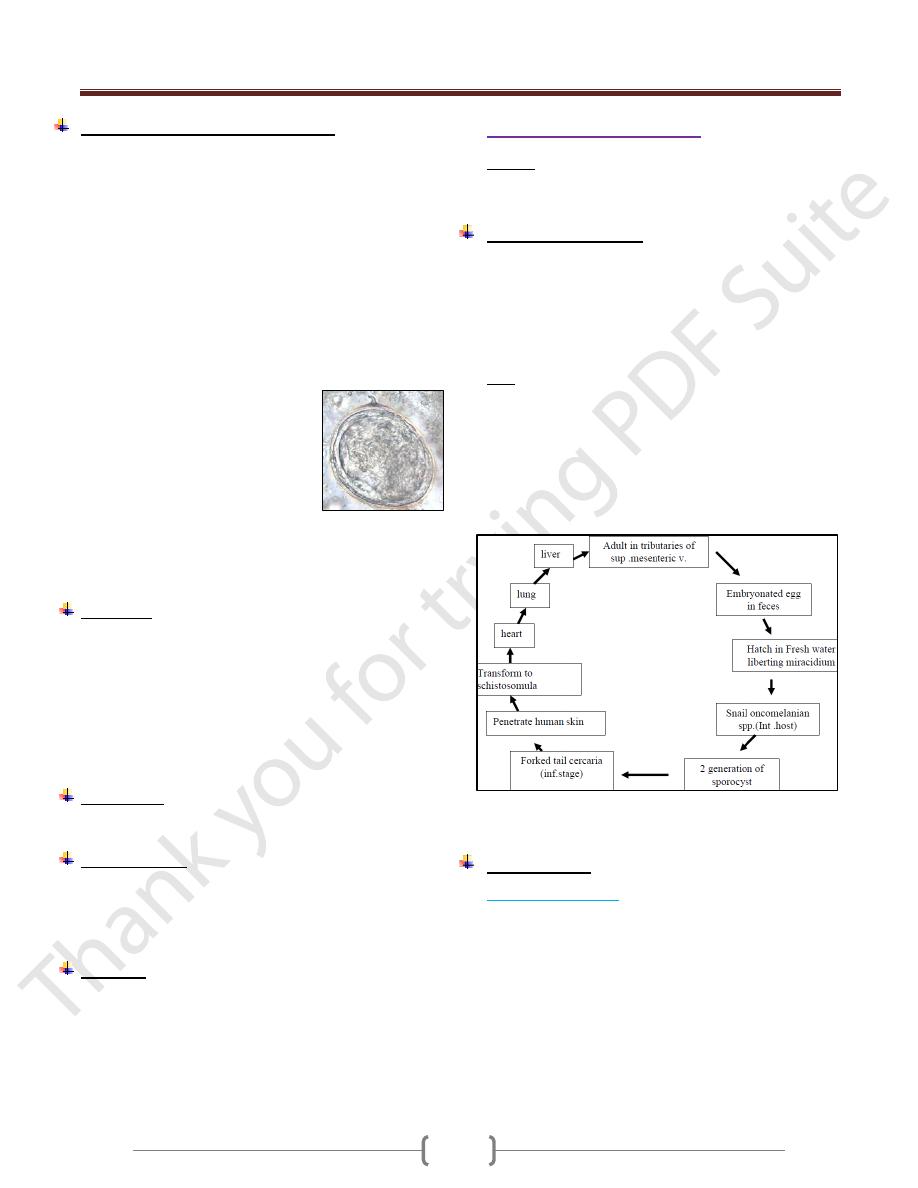
Fully developed egg of Sch. mansoni are large ,rounded
at both ends &provided with a conspicuous lateral spine
near one pole .The egg range in size from (120 x 45)-µ--m
when laid to (170 x 65 )—µm when ready to hatch .
Unit 3: Helminthes (Trematodes)
89
Pathogenesis & Symptomatology:
Humeral & tissue changes caused by S. mansoni resemble
those of infection with other intestinal schistosome spp.but:
1) The incubation period is about 2 weeks longer.
2) The early intestinal lesions typically develop in the
colon rather than the small intestine.
3) The number of eggs produced by each female is less ,
there for fewer eggs extruded from the intestinal
wall& fewer that later become trapped in the
perivascular tissue of the intestine & liver
Thus intestinal & hepatic fibrosis develop more slowly in
Manson ۥs schistosomiasis.
The common manifestation with S. mansoni are:
Fever, chills, weakness, weight loss,
headache, nausea, vomiting, diarrhea
(at times bloody)
There may be evidence suggestive of
peptic ulcer, malabsorption
syndrome, gastrointestinal bleeding,
marked eosinophilia, rectal polyps,
thrombophlebitis . hepatic fibrosis
which may lead to portal hypertension & splenomegaly.
Frank ascitis is less frequent.
pulmonary lesion & symptoms are relatively common
Diagnosis
1) Fecal examination.
2) Rectal biopsy.
3) Immuno diagnostic test.
a) circumoval precipitin test
b) cercarien-Hüllen reaction
c) Immuno diffusion
d) Immuno electrophoresis.
e) Fluorescent antibody test.
Treatment:
-Praziquantel (drug of choice) 40 mg/kg .once
-Oxamniquine.15mg/kg .once
Epidemiology:
S. mansoni is also a parasite of several spp. of mammals.
Ex: Rodent, monkey in Africa & brazil
Man is only definitive host.
Exposure result from contact with cercaria- infected water.
Control :
1) Chemotherapy
2) Snail control.
a) chemical (Niclosamide)
b) Biology Predators (Thiara spp)
Competitor (Marisa spp.)
3) Enviromental sanitation
4) Health education.
Schistosoma japonicum
Disease: Schistosomiasis japonicum
It occurs in the Far East mainly in china, Japan &
Philippines.
Biology &Life cycle:
adult male measure 12-20 mm by 0,5 mm
The tegument is smooth
Oral & ventral sucker are subequal.
There are 7 relatively large testes behind the ventral sucker
Female are delicate with a length (15-30) mm &width
(0.1-0.3)mm
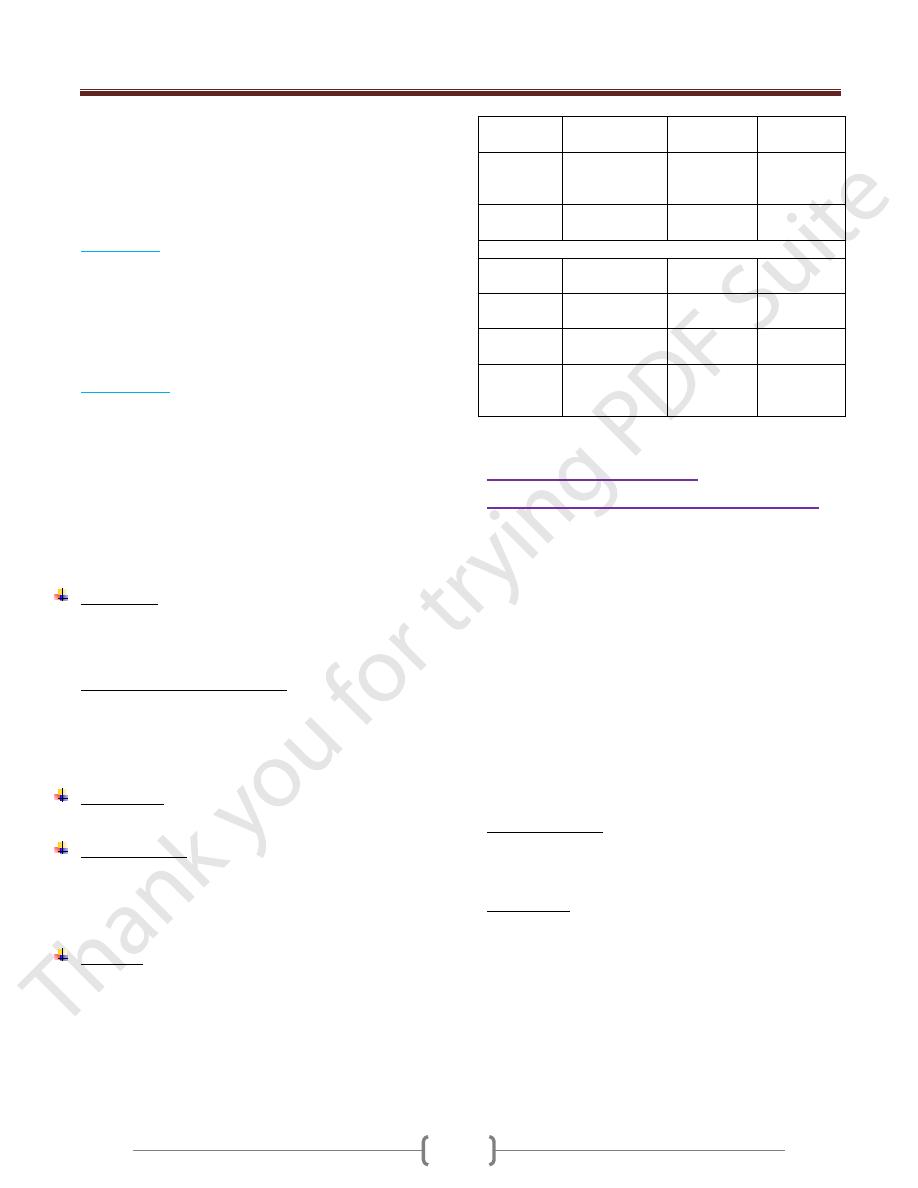
Egg: are round measuring 70-100—m each contains
ciliated miracidium. Aminute blunt projection may be
seen on the outer surface.
The earliest habitat of the young adult is tributaries of the
superior .mesenteric vein. of small Intestine.
Later some worm migrate into the inferior. mesenteric vein.
In these location, female continue to lay eggs daily over a
period of years.
Intramolluscan phase 6-7 weeks. -4-5 weeks from
cercaria penetration & adult maturation & laying eggs.
Pathogenesis:
The prepatent period
is short 4-5 weeks
Female Schistosoma japanicum produce large
number.of eggs.
most of damage is born by the small intestine & liver
Damage is produced as each egg escape from the
venule, filter through the tissue & extruded into the
lumen of the intestine through the ruptured mucosa
with accompanying hemorrhage.
The worm metabolites causes systemic sensitization,
resulting in eosinophilic leukocytosis .over a period of
5 years in heavy infection there is evidence of fibrosis,
Unit 3: Helminthes (Trematodes)
89
papillomas, stenosis of small intestine, hepatic fibrosis
with ascitis, splenomegaly &pulmonary fibrosis.
Towards the end of prepatent period: late
afternoon,fever ,night sweat &diarrhea ,enlarged
tender ,liver ,epigastric distress , pain in the back, groin
or legs .also sometime urticaria develop.
Acute stage:
characterized by :
Diarrhea, eggs in feces, fever, epigastric pain,
enlargement of liver, loses of appetite & weight.
After few weeks ,he may feel better & return to work,
but symptoms return on physical exertion
the blood picture is one of anemia ,increase in serum
globulin level with high eosinophilia
Chronic stage
:
Liver become increasingly fibrosed with multiple minute
granulomas in the parenchyma &on the surface.
The mesentery & omentum may be thickened so as to
bind down the colon & separate the abdomen into an
upper & lower portion .Then increasing ascitis &
emaciation develop dyspnea on slight exertion ,dilatation
of the superficial abdominal veins ,myocarditis due to
infiltaration of eggs into the cardiac wall .The patient
gradually goes into a decline & may die of exhaustion or
supervening infection.
Diagnosis:
Is similar to that of Sch .mansoni
Sedimentation & Kato-thick smear technique may be
required to discover the eggs.
Notes about human blood fluke:
Schistosomiasis japonicum :
most pathogenic - least responsive to treatment.
Schistosomiasis haematobia
Least pathogenic - most responsive to treatment.
Treatment:
Praziquantel 30 mg/kg in one day.
Epidemiology:
Most mammals are susceptible to infection .Exposure
occur when cercariae come in contact with the skin during
washing .The principal source of infection in the snail is
faecal contamination by man.
Control:
Is very difficult because other mammals is susceptible to
infection but it is similar to the control of Sch.haematobium
S.
haematobium
S. mansoni
S.
japonicum
length
10-15 mm
20 mm/adult
6.1-9.9 mm
7.2-14 mm
12-20 mm
15-30 mm
Male
tegument
Slightly
tuberculated
Warty
exerescence
smooth
Reproducti ve system
In male /
testes
4-5
6-9 grape
like cluster
7
Location
of uterus
Anterior two
third
Anterior
half
Anterior
half
Position of
ovary
Posterior half
Anterior
half
Middle half
Location
of caecal
junction
middle
Anterior
half
Posterior
fourth
Schistosoma.dermatitis
Cercarial dermatitis (swimmerۥs itch)
Is the skin reaction that produced by the cutaneous
penetration of cercaria of non-human schistosoma.
They are cercaria of schistosome of aquatic birds
&mammals & may affects person exposing skin to fresh
or salt water, all over the world.
Avian schistosomes that are responsible for Cercarial
dermatitis belong to the genera Trichobilharzia,
ornithobilharzia, Gegantobilharizia, Microbilharzia,
Austrobilharzia
When human are attacked by bird or non-human
mammalian schistosome cercaria, the parasite become
trapped in the skin & fail to complete their circulatory
migration, initiate cercarial dermatitis & then die in
several day.
Clinical Aspect:
Consist of prickling sensation, erythema, urticaria &
macules & papules .The reaction reached into maximu m
within 48-72 hr after exposure then gradually decreases .
Treatment:
Application of palliative (calamine lotion), antihistamine
cream or orally to relieve itching or trimeprazine