Lecture 8 – Nutrition in special diseases
37
1- Diabetes mellitus
Diabetes is present when the fasting plasma glucose is
126 mg/dl {7 mmol/L} or greater on two occasions.
Diabetes is a major source of disability. It is the most
common cause of blindness among Americans. It is
responsible for one third to one half of all cases of chronic
renal failure requiring dialysis. Undiagnosed diabetes can
be a life-threatening disease in children.
Causes of diabetes:
The two types of diabetes are
Type 1, or insulin - dependent diabetes {IDDM}, and
type 2, or non-insulin-dependent diabetes {NIDDM}.
1) Type 1 diabetes, which accounts for approximately 10%
of cases, is believed to be the result of an autoimmune
process in which a progressive destruction of pancreatic
beta cells results in insulin deficiency. Its onset is
typically in childhood. This form of diabetes was
uniformly fatal until insulin was discovered in the 1920s.
2) Type 2 diabetes represents the remaining 90% of cases. It
is also known as adult-onset diabetes. Obesity is present
in 80-90% of individuals with type 2 diabetes and
contributes to the insulin resistance, which is thought to
be a key element in the pathogenesis of this condition.
Impairment in insulin secretion is also a factor in the
development of type 2 diabetes.
The effect of weight loss on type 2 diabetes:
Weight loss has been shown to lower plasma glucose,
triglycerides and very low-density lipoprotein {VLDL}
concentrations in a high proportion of individuals with
type 2 diabetes. Weight loss also reduces blood pressure.
Because elevated blood pressure, triglycerides, and VLDL
are common in type 2 diabetes and because they are
important risk indicators in this condition {which is
accompanied by increased cardiovascular risk}.
How can weight loss be achieved in individuals with
type 2 diabetes?
Although a reduction in energy intake is, in theory, the
ideal treatment for type 2 diabetes, this is extremely
difficult to achieve for long-term management, in part
because of the accessibility of highly palatable, energy-
dense foods in modern culture. Also, most studies show
that weights regain occurs in the majority of people who
have lost weight, usually over a 1-2 year interval.
Therefore, there has been considerable interest in formal,
aerobic exercise as an adjunct to dietary measures for the
purpose of losing weight, studies done over a period of 2-
3 years show that regular exercise, combined with a low-
fat diet, can result in sustained weight loss.
Diabetes and low-fat diet:
A low-fat diet is still strongly recommended for the
prevention and treatment of coronary artery disease.
Several studies have shown that when an isocaloric high-
carbohydrate, low-fat diet is compared with a diet higher
in fat and lower in carbohydrate, the high-carbohydrate
diet tends to result in hypertriglyceridemia. Therefore it is
probably still best to recommend a high-carbohydrate
{50-60% of calories}, low-fat {20-30% of calories} diet
for people with type 2 diabetes.
Dietary protein requirements in diabetes:
Diabetic patients should strive for a moderate protein
intake. When diabetes is controlled, protein metabolism
becomes normal. Studies have shown that restricting
protein in patients with diabetic nephropathy reduces
protienuria. It is, therefore, prudent for diabetic patients to
avoid high-protein diets. The diabetic diet should contain
moderate amounts of protein, usually 15-20% of total
energy.
Micronutrient supplementation in diabetes:
Supplementation of micronutrients not recommended in
diabetes. Physicians are often asked about chromium
picolinate, a preparation found in health food stores,
which has been touted as a treatment for diabetes.
Chromium is a cofactor of insulin. Chromium
supplementation is not currently recommended.
Magnesium and zinc have been suggested as
supplements but are also not generally indicated. A
patient with poorly controlled diabetes, especially one
who is taking diuretics, may become deficient in
magnesium, but no benefit has been shown from
magnesium therapy. It has been suggested that zinc
supplementation might aid in the healing of leg ulcers, but
zinc deficiency is extremely rare.
General advice to patients with diabetes:
Diet and exercise recommendations for diabetic patients.
A diet high in complex carbohydrate {with emphasis on
fiber} and low in fat with some limitations on simple
sugar and alcohol content is recommended for everyone
but especially for diabetics. Consistency of food intake is
also important, to avoid episodes of hyperglycemia.
Exercise, which is important for everyone, is especially
important for the diabetic patient. Sadly,
Lecture 8 – Nutrition in special diseases
38
recommendations for weight loss and exercise too often
fall upon deaf ears in the adult-onset diabetic.
2- Hypertension
Dietary management of hypertension:
Hypertension is one of the most common diseases of
adults.. Nutritional factors are as important as
pharmacologic therapy in the management of
hypertension. Up until the past three decades, patients
with hypertension generally died early, but, with modern
pharmacologic, nutritional, and lifestyle management,
patients with hypertension can live a normal life span.
Dietary measures in prevention of hypertension:
The incidence of hypertension can be reduced by
modifying four predisposing factors, three of which are
nutritional. These four factors are overweight, high salt
intake, excess alcohol consumption, and lack of physical
activity.
The optimum weight for the management of
hypertension:
The weight should be normal. Using the BMI and RW
indices to measure that. A reasonable definition is 20%
above the upper limit of the normal range.
Sodium restriction and hypertension:
Prevention of HT is associated with moderate salt
restriction, defined as 6 grams of salt/ day[ 2400 mg of
sodium]. More severe degrees of salt restriction are not
usually necessary for hypertension in the absence of heart
failure, but, with heart failure it is necessary to have more
restrictive sodium intake.
Potassium intake with hypertension:
There is an association between high potassium intake
and lower blood pressure. An increased potassium intake
is associated with reduced mortality from stroke. The
mechanisms include
lowering of the peripheral resistance
suppression of the rennin- angiotensin
mechanism
Useful substitute for sodium in achieving a low-
sodium diet.
Patients with hypertension are often treated with diuretics,
these drugs especially the hypochlorthiazides, are
associated with potassium loss therefore potassium should
be supplemented to prevent negative potassium balance.
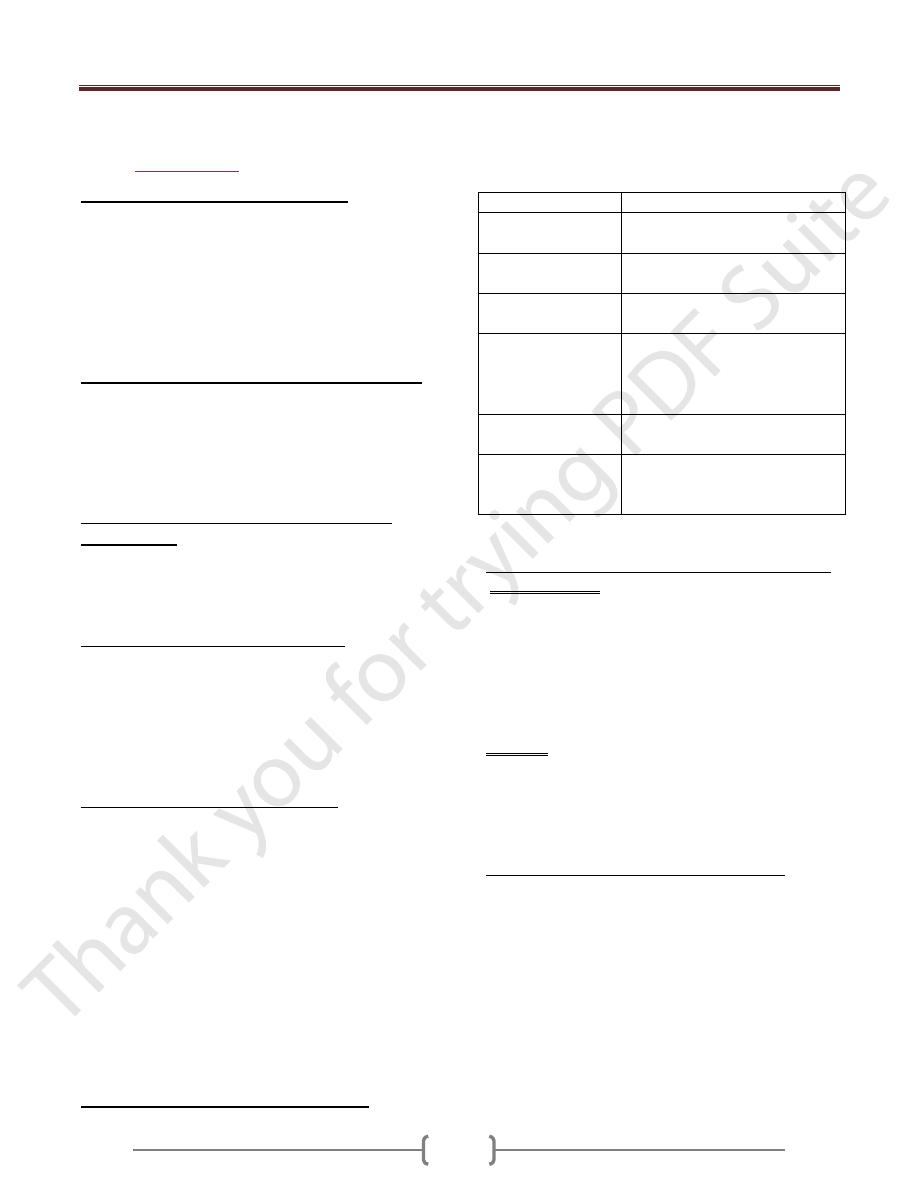
Major drug- nutrient interactions in Hb:
Most of the drugs used to control blood pressure either
interact with nutrients or have gastrointestinal side effects,
or both:
Drugs
Side-effect
B – blockers
[propanalol]
Anorexia, dry mouth
nausea, diarrhea, abdominal pain
& and B- blockers [
labetalol]
Dry mouth, taste change, nausea
diarrhea.
&
1
recepter
blockers[prazocin]
Dry mouth, nausea, diarrhea,
constipation
ACE inhibitors
[enalapril]
Anorexia Dry mouth, nausea,
diarrhea, constipation, taste
change, glossitis and stomatitis,
abdominal pain.
Calcium channel
blockers [vepramil]
nausea, constipation
Vasodilator
[hydralazin]
Anorexia Dry mouth, nausea,
diarrhea, constipation, taste
change,
Modification in lifestyle of hypertensive patients:
Physical activity:
Exercise is the first major change, only 30minutes
scheduled exercise three times a week can have a
beneficial effect and the exercise need to be no more
elaborate than brisk walking.exersice have three benefits:
Lower blood pressure by 6 or 7 mmhg...
Useful to the weight loss program.
It helps to break the cycle of physical activity,
Smoking:
Many people think that smoking primarily damages the
lung. but the excess cardiovascular mortality related to
smoking is three times as large as the excess mortality
related to lung cancer.
Management of Hb in the elderly patients:
The systolic blood pressure rises as people age.
Management is as for younger patients. Weight reduction,
sodium restriction, alcohol limitation, and exercise are all
important components in the overall management.