Basic Anatomy
529
natomy
asic
B
a
The head and neck region of the body contains many
and abdomen.
except the 10th, which also supplies structures in the chest
nerves are distributed to structures in the head and neck,
through foramina and fissures in the skull. All the cranial
12 pairs of cranial nerves, which leave the brain and pass
or in the cavities bounded by them. The brain gives rise to
special senses, the eye and the ear, lie within the skull bones
its covering meninges enclosed in the cranial cavity. The
The head is formed mainly by the skull with the brain and
area.
important structures compressed into a relatively small
The Head
Bones of the Skull
ered on the outer and inner surfaces with periosteum.
and more brittle than the external table. The bones are cov
(Fig. 11.2). The internal table is thinner
called the
of compact bone separated by a layer of spongy bone
tables
internal
external
The skull bones are made up of
of the cranium (Fig. 11.1).
is the lowest part
base of the skull
of the cranium, and the
is the upper part
vault
cranium and those of the face. The
The bones of the skull can be divided into those of the
by the mobile temporomandibular joint (see page 571).
dible is an exception to this rule, for it is united to the skull
The man
sutural ligament.
between the bones is called a
The connective tissue
sutures.
at immobile joints called
The skull is composed of several separate bones united
Composition
-
and
diploë
-
optic canal
lacrimal
frontal
zygomaticomaxillar
y
superciliary arch
nasal
frontal process
of maxilla
supraorbital notch
parietal
greater wing
of sphenoid
zygomatic process
of frontal
squamous temporal
zygomatic
infraorbital foramen
mastoid process
ramus of mandible
body of mandible
symphysis menti
mental foramen
maxilla
inferior concha
middle concha
suture
inferior orbital
fissure
superior orbital
fissure
zygomatic
frontozygomatic
suture
coronal suture
orbital plate of frontal
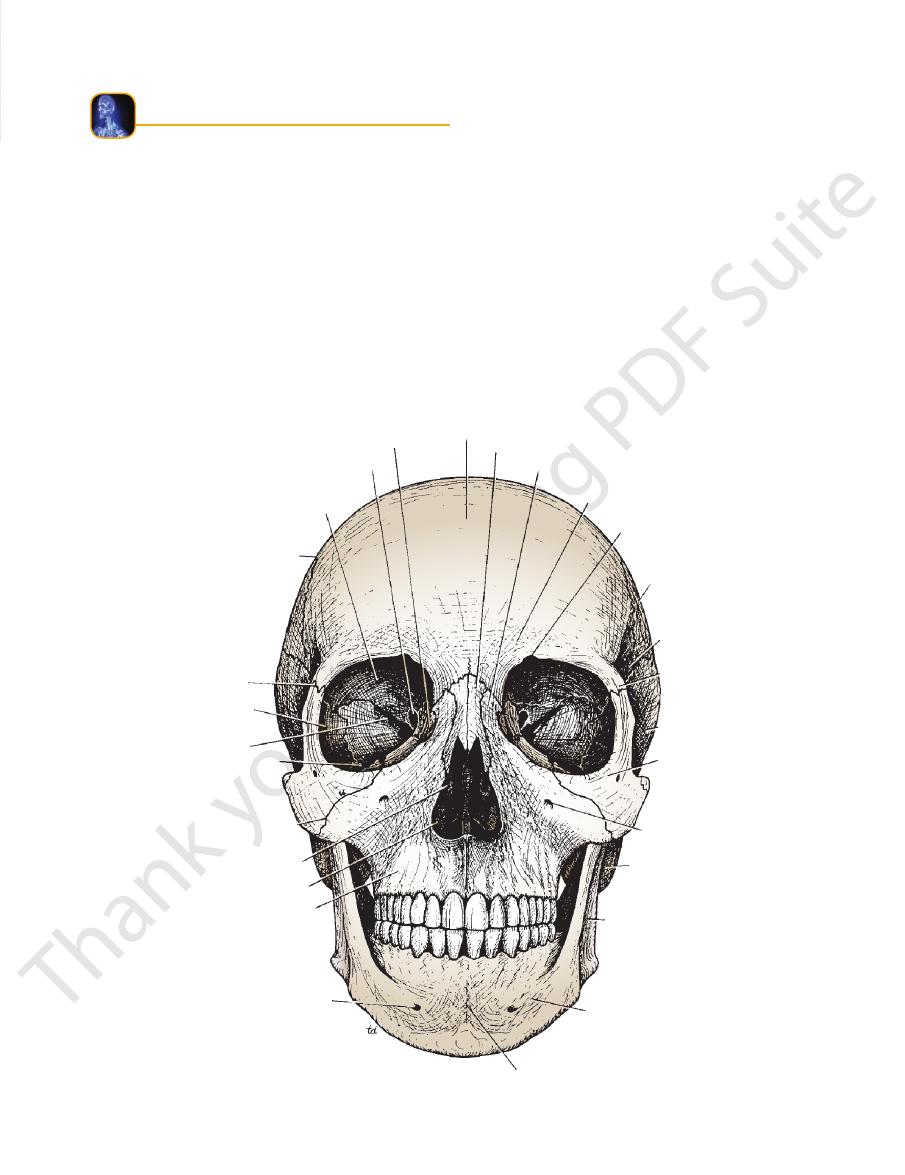
FIGURE 11.1
Bones of the anterior aspect of the skull.

530
CHAPTER 11
The Head and Neck
superficial vein of scalp
emissary vein
cerebral artery in
skin
connective tissue
aponeurosis
loose connective
tissue
pericranium
(periosteum)
outer table of
parietal bone
diploe
inner table of
parietal bone
cerebral vein in
subarachnoid space
cerebral cortex
pia mater
subarachnoid space
arachnoid
meningeal layer
of dura mater
endosteal layer
of dura mater
arachnoid granulation
superior sagittal sinus
diploic vein
sagittal suture
¨
falx cerebri
inferior sagittal sinus
FIGURE 11.2
tal suture of the skull,
Coronal section of the upper part of the head showing the layers of the scalp, the sagit
and serves as a voice resonator.
This communicates with the nasal cavity
maxillary sinus.
mid-shaped cavity lined with mucous membrane called the
carries the upper teeth. Within each maxilla is a large, pyra
which
alveolar arch,
fellow of the opposite side, forms the
projects downward and, together with the
alveolar process
The
infraorbital foramen.
the maxilla is perforated by the
the lower margin of the nasal aperture. Below the orbit,
and form
intermaxillary suture
meet in the midline at the
and part of the floors of the orbital cavities. The two bones
the hard palate, part of the lateral walls of the nasal cavities,
form the upper jaw, the anterior part of
maxillae
The two
are separate bones.
inferior conchae
on each side; the
ethmoid
ject into the nasal cavity from the
are shelves of bone that pro
middle conchae
superior
The
vomer.
nasal septum, which is largely formed by the
The nasal cavity is divided into two by the bony
aperture.
anterior nasal
lower borders, with the maxillae, make the
form the bridge of the nose. Their
two nasal bones
The
and serve as voice resonators.
These communicate with the nose
frontal air sinuses.
are two hollow spaces lined with mucous membrane called
just above the orbital margins,
frontal bone,
Within the
medially.
riorly, and the processes of the maxilla and frontal bone
superiorly, the zygomatic bone laterally, the maxilla infe
are bounded by the frontal bone
orbital margins
The
tal bone articulates with the zygomatic bone.
of the maxillae and with the nasal bones. Laterally, the fron
ally, the frontal bone articulates with the frontal processes
can be recognized. Medi
foramen,
or
supraorbital notch,
can be seen on either side, and the
superciliary arches
The
to make the upper margins of the orbits (Fig. 11.1).
or forehead bone, curves downward
frontal bone,
The
Anterior View of the Skull
External Views of the Skull
the following description.
should have a dried skull available for reference as they read
students should be familiar with the skull as a whole and
detailed structure of each individual skull bone. However,
It is unnecessary for students of medicine to know the
Mandible: 1
Inferior conchae: 2
Palatine bones: 2
Vomer: 1
Lacrimal bones: 2
Nasal bones: 2
Maxillae: 2
Zygomatic bones: 2
single:
consist of the following, two of which are
facial bones
The
Ethmoid bone: 1
Sphenoid bone: 1
Temporal bones: 2
Occipital bone: 1
Parietal bones: 2
Frontal bone: 1
which are paired (Figs. 11.3 and 11.4):
consists of the following bones, two of
cranium
The
relation of cerebral blood vessels to the subarachnoid space.
the falx cerebri, the superior and inferior sagittal venous sinuses, the arachnoid granulations, the emissary veins, and the
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
-
-
-
the
and
-
-
Basic Anatomy
531
external auditory meatus
squamous temporal
zygoma
pterion
coronal suture
temporal lines
frontal
greater wing
of sphenoid
zygomatic process
of frontal
nasion
frontal process
of zygomatic
lacrimal
zygomatic
zygomaticofacial
foramen
infraorbital foramen
coronoid process
maxilla
alveolar part
mental foramen
body of mandible
ramus
angle
neck of mandible
head of mandible
styloid process
mastoid process
tympanic plate
suprameatal spine
suprameatal triangle
superior nuchal line
external occipital
protuberance (inion)
occipital
lambdoid
suture
supramastoid crest
parietal
nasal
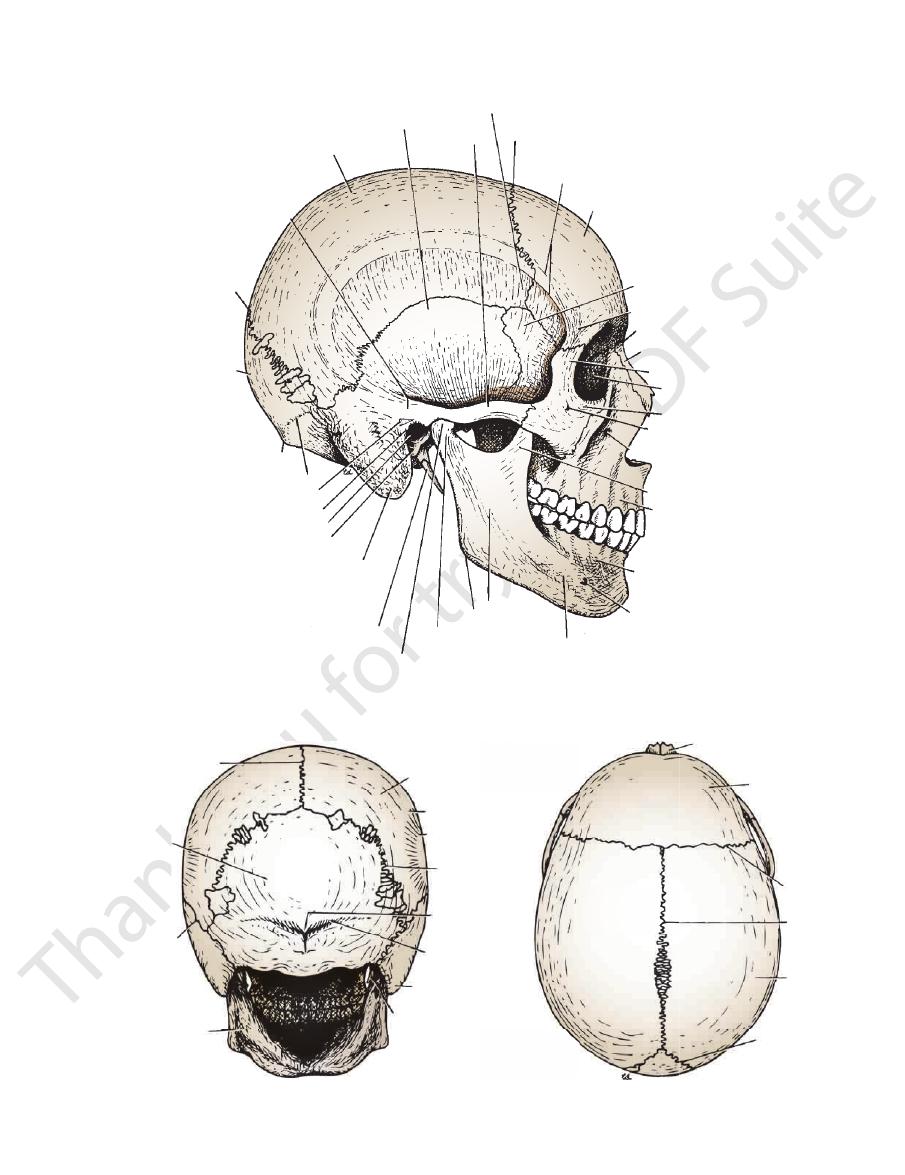
FIGURE 11.3
Bones of the lateral aspect of the skull.
sagittal suture
occipital
parietomastoid
suture
mandible
styloid process
mastoid process
superior nuchal
line
external occipital
protuberance
lambdoid suture
inferior temporal
line
superior temporal
line
parietal
nasal
frontal
coronal
suture
sagittal
suture
parietal
lambdoid
suture
A
B
FIGURE 11.4
Bones of the skull viewed from the posterior (A) and superior (B) aspects.
532
CHAPTER 11
infratemporal fossa through the pterygomaxillary fissure,
below the orbital cavity. It communicates laterally with the
is a small space behind and
pterygopalatine fossa
The
maxilla. It leads forward into the orbit.
between the greater wing of the sphenoid bone and the
is a horizontal fissure
inferior orbital fissure
The
palatine fossa.
pterygo
and back of the maxilla. It leads medially into the
fossa between the pterygoid process of the sphenoid bone
is a vertical fissure that lies within the
gomaxillary fissure
ptery
on the greater wing of the sphenoid. The
ral crest
infratempo
lies below the
infratemporal fossa
The
rior temporal line.
lies below the infe
temporal fossa
they arch backward. The
the zygomatic process of the frontal bone and diverge as
which begin as a single line from the posterior margin of
inferior temporal lines,
superior
Identify the
vein.
artery
middle meningeal
it overlies the anterior division of the
Clinically, the pterion is an important area because
pterion.
is referred to as the
articulates with the greater wing of the sphenoid; this point
skull is where the anteroinferior corner of the parietal bone
Note that the thinnest part of the lateral wall of the
tus. The ramus and body of the mandible lie inferiorly.
Note the position of the external auditory mea
sphenoid.
greater wing of the
zygomatic process;
cess,
squamous, tympanic, mastoid process, styloid pro
namely,
temporal bone,
parts of the
occipital bone;
of the
The skull is completed at the side by the squamous part
lambdoid suture.
behind, at the
They articulate with the occipital bone
sagittal suture.
nium and articulate with each other in the midline at the
form the sides and roof of the cra
parietal bones
The
suture (Fig. 11.3).
skull and articulates with the parietal bone at the coronal
forms the anterior part of the side of the
frontal bone
The
Lateral View of the Skull
body and two vertical rami (for details, see page 569).
or lower jaw, consists of a horizontal
mandible,
The
otemporal nerves.
by two foramina for the zygomaticofacial and zygomatic
form the zygomatic arch. The zygomatic bone is perforated
ulates with the zygomatic process of the temporal bone to
Medially, it articulates with the maxilla and laterally it artic
and part of the lateral wall and floor of the orbital cavity.
forms the prominence of the cheek
zygomatic bone
The
The Head and Neck
-
-
-
the
-
and
and the
-
and
and
-
-
-
-
medially with the nasal cavity through the
rotundum, and anteriorly with the orbit through the
superiorly with the skull through the foramen
foramen,
sphenopalatine
Above the posterior edge of the hard palate are the
foramina.
lesser palatine
greater
Posterolaterally are the
men.
fora
incisive fossa
In the midline anteriorly is the
can be identified.
zontal plates of the palatine bones
hori
palatal processes of the maxillae
The
(Fig. 11.5).
hard palate
the skull is seen to be formed by the
If the mandible is discarded, the anterior part of this aspect of
Inferior View of the Skull
sagittal suture.
in the midline at the
Behind, the two parietal bones articulate
metopic suture.
two halves of the frontal bone fail to fuse, leaving a midline
Occasionally, the
coronal suture.
two parietal bones at the
Anteriorly, the frontal bone (Fig. 11.4) articulates with the
Superior View of the Skull
extend laterally toward the temporal bone.
superior nuchal lines
either side of the protuberance the
attachment to muscles and the ligamentum nuchae. On
which gives
external occipital protuberance,
called the
the midline of the occipital bone is a roughened elevation
the occipital bone articulates with the temporal bone. In
On each side
lambdoid suture.
the occipital bone at the
the parietal bones articulate with the squamous part of
are seen above. Below,
sagittal suture
with the intervening
The posterior parts of the two parietal bones (Fig. 11.4)
Posterior View of the Skull
inferior orbital fissure.
and the
-
and
-
and
on the lateral surface of
suprameatal crest
identify the
While examining this region,
external auditory meatus.
bone, is C shaped on section and forms the bony part of the
which forms part of the temporal
tympanic plate,
The
this foramen from the cavity of the skull to the exterior.
with fibrous tissue, and only a few small vessels pass through
During life, the foramen lacerum is closed
men lacerum.
fora
bone and the greater wing of the sphenoid, forms the
is irregular and, together with the basilar part of the occipital
The medial end of the petrous part of the temporal bone
of the petrous part of the temporal bone.
can be seen on the inferior surface
carotid canal
ing of the
downward and forward from its inferior aspect. The open
of the temporal bone projects
styloid process
The
tympani nerve exits from the tympanic cavity.
through the medial end of which the chorda
panic fissure,
squamotym
from the tympanic plate posteriorly is the
temporomandibular joint. Separating the mandibular fossa
form the upper articular surfaces for the
articular tubercle
of the temporal bone and the
mandibular fossa
The
can be identified.
The opening of the bony part of the tube
auditory tube.
temporal bone, is a groove for the cartilaginous part of the
the greater wing of the sphenoid and the petrous part of the
Behind the spine of the sphenoid, in the interval between
spine of the sphenoid.
foramen spinosum is the
Posterolateral to the
foramen spinosum.
and the small
foramen ovale
wing of the sphenoid is pierced by the large
the greater
lateral pterygoid plate,
Posterolateral to the
hamulus.
pterygoid
is prolonged as a curved spike of bone, the
plate
medial pterygoid
sphenoid bone. The inferior end of the
of the
medial pterygoid plates
are bounded laterally by the
and
vomer
from each other by the posterior margin of the
(posterior nasal apertures). These are separated
choanae
-
-
-
Basic Anatomy
533
incisive foramen
palatal process of palatine
inferior orbital fissure
greater palatine foramen
lesser palatine foramen
vomer
lateral pterygoid
plate
medial pterygoid
plate
foramen ovale
foramen spinosum
spine of sphenoid
petrous part of
temporal bone
tympanic part of
temporal bone
carotid canal
jugular foramen
condyle
external occipital protuberance
occipital bone
superior nuchal line
foramen magnum
pharyngeal tubercle
mastoid process
stylomastoid
foramen
squamous part of
temporal bone
styloid process
articular tubercle
mandibular fossa
scaphoid fossa
infratemporal crest
hamulus
tubercle of maxilla
zygomatic arch
palatal process of maxilla
hypoglossal canal
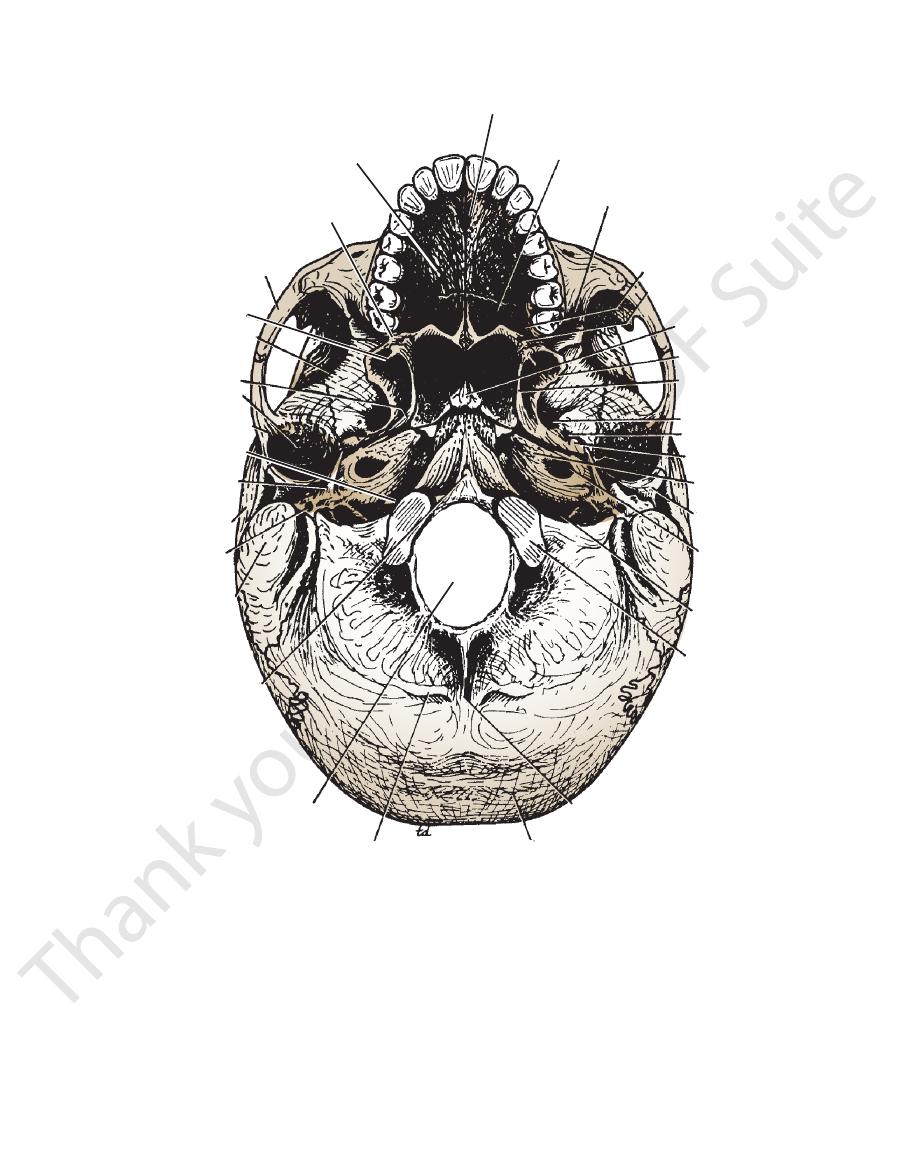
FIGURE 11.5
Inferior surface of the base of the skull.
suprameatal
the squamous part of the temporal bone, the
triangle,
In the interval between the styloid and mastoid
suprameatal spine.
and the
processes, the
a shallower notch on the occipital bone, forms the
temporal bone has a deep notch, which, together with
Medial to the styloid process, the petrous part of the
can be seen.
stylomastoid foramen
side.
lines should be identified as they curve laterally on each
the external occipital protuberance. The superior nuchal
Posterior to the foramen magnum in the midline is
sal nerve (Fig. 11.6).
for transmission of the hypoglos
hypoglossal canal
cervical vertebra, the atlas. Superior to the occipital condyle
late with the superior aspect of the lateral mass of the first
should be identified; they articu
occipital condyles
The
part of the occipital bone in the midline.
is a small prominence on the undersurface of the basilar
pharyngeal tubercle
basilar part of the occipital bone. The
of the foramen magnum are the sphenoid bone and the
Behind the posterior apertures of the nose and in front
jugular foramen.
-
is the
-
534
CHAPTER 11
The Head and Neck
crista galli
foramen cecum
cribriform plate
orbital plate of frontal
optic canal
anterior clinoid process
foramen rotundum
foramen lacerum
foramen ovale
groove for middle
meningeal artery
foramen spinosum
squamous part
of temporal
internal acoustic
meatus
groove for
sigmoid sinus
groove for transverse sinus
hypoglossal canal
internal occipital protuberance
internal occipital crest
foramen magnum
basilar part of occipital
jugular foramen
groove for superior
petrosal sinus
arcuate eminence
hiatus for
greater
petrosal nerve
dorsum sellae
posterior
clinoid process
sella turcica
tuberculum sellae
lesser wing of sphenoid
petrous part
of temporal
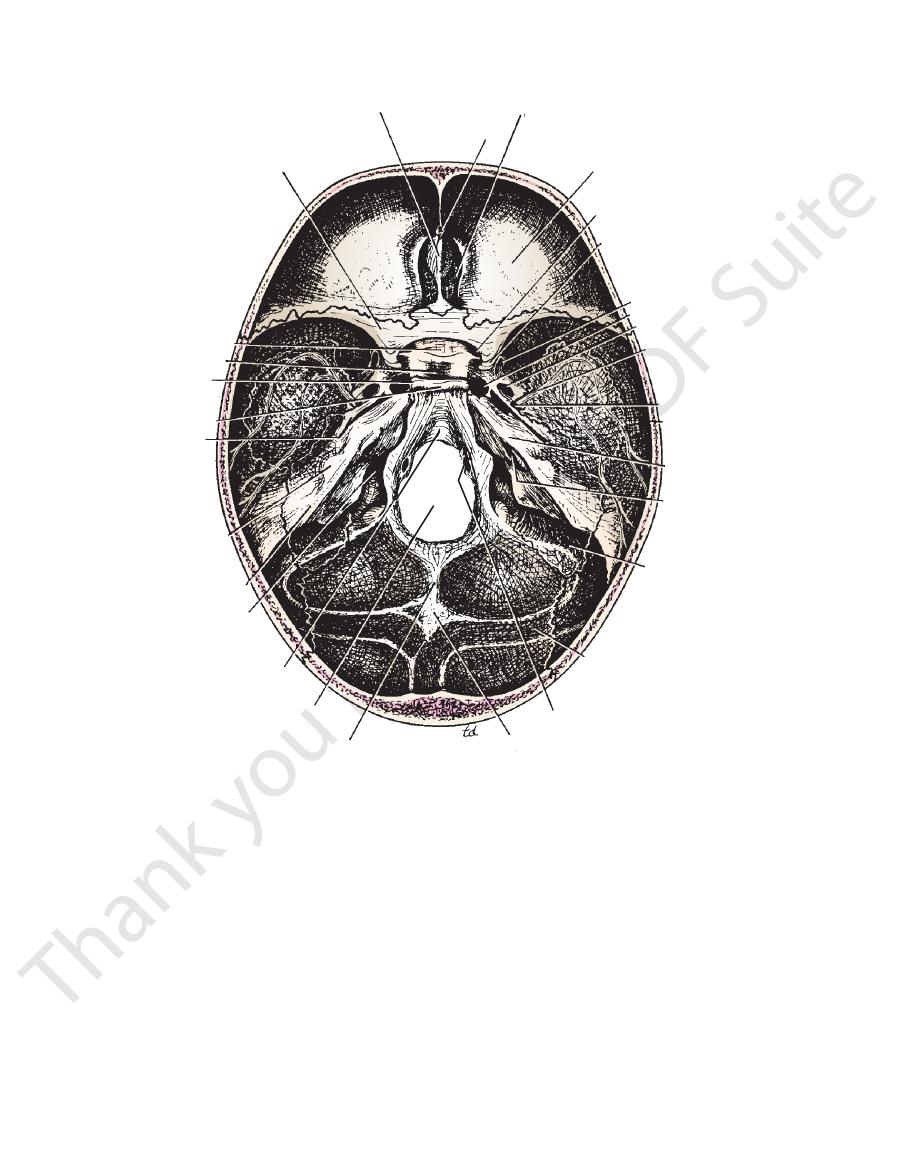
FIGURE 11.6
Internal surface of the base of the skull.
cerebral hemispheres. It is bounded anteriorly by the inner
The anterior cranial fossa lodges the frontal lobes of the
Anterior Cranial Fossa
the petrous part of the temporal bone.
cranial fossa is separated from the posterior cranial fossa by
nial fossa by the lesser wing of the sphenoid, and the middle
The anterior cranial fossa is separated from the middle cra
into three cranial fossae: anterior, middle, and posterior.
The interior of the base of the skull (Fig. 11.6) is divided
the vault.
as they pass up the side of the skull to
meningeal vessels
middle
sent for the anterior and posterior divisions of the
(see page 543). Several narrow grooves are pre
ulations
arachnoid gran
lateral lacunae
which lodge the
granular
side of the groove are several small pits, called
On each
superior sagittal sinus.
tal groove that lodges the
tal, and lambdoid sutures. In the midline is a shallow sagit
The internal surface of the vault shows the coronal, sagit
Vault of the Skull
and venous sinuses.
meninges, portions of the cranial nerves, arteries, veins,
The cranial cavity contains the brain and its surrounding
The Cranial Cavity
-
-
pits,
and
-
-
Base of the Skull
-
surface of the frontal bone, and in the midline is a crest for
angle of the parietal bone, or the pterion. The medial end of
laterally with the frontal bone and meets the anteroinferior
is the sharp lesser wing of the sphenoid, which articulates
Its posterior boundary
falx cerebri.
the attachment of the
Basic Anatomy
the apex of the petrous part of the temporal bone for the
Lateral to the foramen lacerum is an impression on
cess, and emerges from the cavernous sinus (see page 598).
cally upward, medial (Fig. 11.20) to the anterior clinoid pro
process. At this point, the internal carotid artery turns verti
cavernous sinus to reach the region of the anterior clinoid
of the sphenoid bone. Here, the artery turns forward in the
and immediately turns upward to reach the side of the body
carotid artery enters the foramen through the carotid canal
lacerum above the closed inferior opening. The internal
opens into the side of the foramen
carotid canal
The
from the cranial cavity to the neck.
tissue, and only small blood vessels pass through this tissue
the foramen lacerum in life is filled by cartilage and fibrous
and the sphenoid bone (Fig. 11.6). The inferior opening of
between the apex of the petrous part of the temporal bone
foramen lacerum
The large and irregularly shaped
mous part of the temporal bone to reach the parietal bone.
terior branch passes backward and upward across the squa
may be damaged after a blow to the side of the head. The pos
upward on the parietal bone. It is at this site that the artery
by the artery for a short distance before it runs backward and
(Fig. 11.131A). Here, the bone is deeply grooved or tunneled
and upward to the anteroinferior angle of the parietal bone
and posterior branches. The anterior branch passes forward
11.20). After a short distance, the artery divides into anterior
temporal bone and the greater wing of the sphenoid (Fig.
a groove on the upper surface of the squamous part of the
cranial cavity. The artery then runs forward and laterally in
artery from the infratemporal fossa (see page 598) into the
sphenoid. The foramen transmits the middle meningeal
foramen ovale and also perforates the greater wing of the
lies posterolateral to the
foramen spinosum
The small
fossa; the lesser petrosal nerve also passes through it.
motor root of the mandibular nerve to the infratemporal
sphenoid and transmits the large sensory root and small
rotundum (Fig. 11.6). It perforates the greater wing of the
lies posterolateral to the foramen
foramen ovale
The
the trigeminal ganglion to the pterygopalatine fossa.
wing of the sphenoid and transmits the maxillary nerve from
medial end of the superior orbital fissure, perforates the greater
which is situated behind the
foramen rotundum,
The
wing of the sphenoid and drains into the cavernous sinus.
sinus runs medially along the posterior border of the lesser
the superior ophthalmic vein. The sphenoparietal venous
lomotor, nasociliary, and abducent nerves, together with
the sphenoid, transmits the lacrimal, frontal, trochlear, ocu
slitlike opening between the lesser and the greater wings of
which is a
superior orbital fissure,
artery, to the orbit. The
and the ophthalmic artery, a branch of the internal carotid
transmits the optic nerve
optic canal
Anteriorly, the
serve as voice resonators.
membrane and communicate with the nasal cavity; they
which are lined with mucous
sphenoid air sinuses,
stretched on each side. The body of the sphenoid contains
that are out
lesser wings
and
greater
with
body
placed
The sphenoid bone resembles a bat having a centrally
mous and petrous parts of the temporal bone.
is formed by the greater wing of the sphenoid and the squa
The floor of each lateral part of the middle cranial fossa
noid, and the parietal bones.
parts of the temporal bones, the greater wings of the sphe
parts of the temporal bones. Laterally lie the squamous
noid and posteriorly by the superior borders of the petrous
It is bounded anteriorly by the lesser wings of the sphe
cerebral hemispheres.
of the
temporal lobes
lateral parts form concavities on either side, which lodge
is formed by the body of the sphenoid, and the expanded
expanded lateral parts (Fig. 11.6). The median raised part
The middle cranial fossa consists of a small median part and
Middle Cranial Fossa
olfactory nerves.
cribriform plate are for the
ports the olfactory bulbs, and the small perforations in the
cavity. The upper surface of the cribriform plate sup
into the nasal
anterior ethmoidal nerve
the passage of the
the crista galli is a narrow slit in the cribriform plate for
midline for the attachment of the falx cerebri. Alongside
is a sharp upward projection of the ethmoid bone in the
crista galli
of the ethmoid medially (Fig. 11.6). The
plate
cribriform
plates of the frontal bone laterally and by the
The floor of the fossa is formed by the ridged orbital
is limited posteriorly by the groove for the optic chiasma.
The median part of the anterior cranial fossa
rium cerebelli.
tento
on each side, which gives attachment to the
process
anterior clinoid
the lesser wing of the sphenoid forms the
535
-
-
the
-
-
-
-
the
-
-
-
lies
-
-
body of the sphenoid (Figs. 11.9 and 11.10). It carries in its
The cavernous sinus is directly related to the side of the
attachment to the fixed margin of the tentorium cerebelli.
which give
posterior clinoid processes,
tubercles, called the
The superior angles of the dorsum sellae have two
sellae.
dorsum
posteriorly by a square plate of bone called the
The sella turcica is bounded
pituitary gland.
lodges the
which
sella turcica,
the elevation is a deep depression, the
Behind
tuberculum sellae.
to the sulcus is an elevation, the
on each side. Posterior
optic canal
and leads laterally to the
which is related to the optic chiasma
sulcus chiasmatis,
by the body of the sphenoid bone (Fig. 11.6). In front is
The median part of the middle cranial fossa is formed
hemisphere (Fig. 11.30).
the tympanic cavity from the temporal lobe of the cerebral
of bone is the only major barrier that separates infection in
the tympanic cavity, and the auditory tube. This thin plate
behind forward, it forms the roof of the mastoid antrum,
adjoins the squamous part of the bone (Fig. 11.6). From
extension of the petrous part of the temporal bone and
a thin plate of bone, is a forward
tegmen tympani,
The
superior semicircular canal.
the underlying
the anterior surface of the petrous bone and is caused by
is a rounded eminence found on
arcuate eminence
The
the cavernous sinus.
glion. Here, it leaves the posterior cranial fossa and enters
apex of the petrous bone, medial to the trigeminal gan
The abducent nerve bends sharply forward across the
ward to the foramen ovale.
The lesser petrosal nerve passes for
the pterygoid canal.
nerve of
around the internal carotid artery), to form the
(sympathetic fibers from
deep petrosal nerve
and joins the
enters the foramen lacerum deep to the trigeminal ganglion
branch of the tympanic plexus. The greater petrosal nerve
lesser petrosal nerve,
the smaller lateral groove is for the
a branch of the facial nerve;
greater petrosal nerve,
for the
bone are two grooves for nerves; the largest medial groove is
On the anterior surface of the petrous
trigeminal ganglion.
a
-
-
the
536
CHAPTER 11
and the large
11th cranial nerves;
and
9th, 10th,
inferior petrosal sinus;
tures from before backward: the
part of the occipital bone. It transmits the following struc
the petrous part of the temporal bone and the condylar
lies between the lower border of
jugular foramen
The
hypoglossal nerve.
transmits the
eral boundary of the foramen magnum (Fig. 11.6) and
is situated above the anterolat
hypoglossal canal
The
sory nerves, and the two vertebral arteries.
rounding meninges, the ascending spinal parts of the acces
floor and transmits the medulla oblongata and its sur
occupies the central area of the
foramen magnum
The
above (Fig. 11.10).
below and the occipital lobes of the cerebral hemispheres
which intervenes between the cerebellum
torium cerebelli,
ten
The roof of the fossa is formed by a fold of dura, the
of the temporal bone.
squamous parts of the occipital bone and the mastoid part
the posterior fossa is formed by the basilar, condylar, and
mous part of the occipital bone (Fig. 11.6). The floor of
teriorly it is bounded by the internal surface of the squa
border of the petrous part of the temporal bone, and pos
Anteriorly, the fossa is bounded by the superior
oblongata.
medulla
cerebellum, pons,
the hindbrain, namely, the
The posterior cranial fossa is deep and lodges the parts of
Posterior Cranial Fossa
nerve pass forward through the sinus.
(Fig. 11.12). The internal carotid artery and the 6th cranial
thalmic and maxillary divisions of the 5th cranial nerve
lateral wall the 3rd and 4th cranial nerves and the oph
The Head and Neck
-
and
-
-
-
-
-
-
-
the
to it is attached the small
nal occipital protuberance;
inter
line posteriorly from the foramen magnum to the
runs upward in the mid
internal occipital crest
The
roots of the facial nerve.
the vestibulocochlear nerve and the motor and sensory
face of the petrous part of the temporal bone. It transmits
pierces the posterior sur
internal acoustic meatus
The
jugular vein.
internal
turns down through the foramen to become the
temporal bone to reach the foramen. The sigmoid sinus
the groove on the lower border of the petrous part of the
The inferior petrosal sinus descends in
sigmoid sinus.
-
-
-
falx
cerebelli
pass through them.
openings in the base of the skull and the structures that
Table 11.1 provides a summary of the more important
rior to the mastoid antrum.
toid part of the temporal bone. Here, it lies directly poste
deeply grooves the back of the petrous bone and the mas
As the sigmoid sinus descends to the jugular foramen, it
bone in a narrow groove and drains into the sigmoid sinus.
runs backward along the upper border of the petrous
sinus
superior petrosal
The
sigmoid sinus.
sinus becomes the
mastoid part of the temporal bone, and here the transverse
corner of the parietal bone. The groove now passes onto the
of the occipital bone, to reach the posteroinferior angle or
groove sweeps around on either side, on the internal surface
(Fig. 11.6). This
transverse sinus
a wide groove for the
On each side of the internal occipital protuberance is
occipital sinus.
over the
-
-
Summary of the More Important Openings in the Base of the Skull and the
Structures That Pass Through Them
T A B L E 1 1 . 1
Vestibulocochlear and facial nerves
Lacrimal, frontal, trochlear, oculomotor, nasociliary,
Structures Transmitted
Opening in Skull
Bone of Skull
Anterior Cranial Fossa
Perforations in cribriform plate
Ethmoid
Olfactory nerves
Middle Cranial Fossa
Optic canal
Lesser wing of sphenoid
Optic nerve, ophthalmic artery
Superior orbital fissure
Between lesser and greater
wings of sphenoid
and abducent nerves; superior ophthalmic vein
Foramen rotundum
Greater wing of sphenoid
Maxillary division of the trigeminal nerve
Foramen ovale
Greater wing of sphenoid
Mandibular division of the trigeminal nerve,
lesser petrosal nerve
Foramen spinosum
Greater wing of sphenoid
Middle meningeal artery
Foramen lacerum
Between petrous part of temporal
and sphenoid
Internal carotid artery
Posterior Cranial Fossa
Foramen magnum
Occipital
Medulla oblongata, spinal part of accessory nerve,
and right and left vertebral arteries
Hypoglossal canal
Occipital
Hypoglossal nerve
Jugular foramen
Between petrous part of temporal
and condylar part of occipital
Glossopharyngeal, vagus, and accessory nerves;
sigmoid sinus becomes internal jugular vein
Internal acoustic m
eatus
Petrous part of temporal
Basic Anatomy
537
Fractures of the Skull
bital nerve with anesthesia or paresthesia of the skin of the cheek
riform plate of the ethmoid bone. Double vision (diplopia) may be
with anterior open bite, and possibly leakage of cerebrospinal
ity of the underlying bone on palpation, malocclusion of the teeth
Maxillofacial fractures usually occur as the result of massive
cartilage); therefore, this part of the skull in children is relatively
facial fractures. Fortunately, the upper part of the skull is devel
biotic therapy.
the presence of well-developed, air-filled sinuses and the muco
adult’s, and fractures may be incomplete or greenstick. In adults,
The developing bones of a child’s face are more pliable than an
nerve from injury.
10th, and 11th cranial nerves may be damaged. The strong bony
days later, it tracks between the muscles and appears in the pos
brospinal fluid may leak into the sphenoidal air sinuses and then
bone. The 3rd, 4th, and 6th cranial nerves may be damaged if
involved as they pass through the petrous part of the temporal
tory meatus is common. The 7th and 8th cranial nerves may be
ina and canals in this region; the cavities of the middle ear and
this is the weakest part of the base of the skull. Anatomically,
Fractures of the middle cranial fossa are common, because
hemorrhage beneath the conjunctiva and into the orbital cavity,
of the overlying meninges and underlying mucoperiosteum. The
ball in that a localized blow produces a depression without splin
to the vault often result in a series of linear fractures, which radi
which it splinters. A severe, localized blow produces a local
brittle. Moreover, the sutural ligaments begin to ossify during
Fractures of the skull are common in the adult but much less so
in the young child. In the infant skull, the bones are more resilient
than in the adult skull, and they are separated by fibrous sutural
ligaments. In the adult, the inner table of the skull is particularly
middle age.
The type of fracture that occurs in the skull depends on the
age of the patient, the severity of the blow, and the area of skull
receiving the trauma. The adult skull may be likened to an egg-
shell in that it possesses a certain limited resilience beyond
indentation, often accompanied by splintering of the bone. Blows
-
ate out through the thin areas of bone. The petrous parts of the
temporal bones and the occipital crests strongly reinforce the
base of the skull and tend to deflect linear fractures.
In the young child, the skull may be likened to a table-tennis
-
tering. This common type of circumscribed lesion is referred to
as a “pond” fracture.
Fractures of the Anterior Cranial Fossa
In fractures of the anterior cranial fossa, the cribriform plate of
the ethmoid bone may be damaged. This usually results in tearing
patient will have bleeding from the nose (epistaxis) and leakage
of cerebrospinal fluid into the nose (cerebrospinal rhinorrhea).
Fractures involving the orbital plate of the frontal bone result in
causing exophthalmos. The frontal air sinus may be involved,
with hemorrhage into the nose.
Fractures of the Middle Cranial Fossa
this weakness is caused by the presence of numerous foram-
the sphenoidal air sinuses are particularly vulnerable. The leak-
age of cerebrospinal fluid and blood from the external audi-
the lateral wall of the cavernous sinus is torn. Blood and cere-
into the nose.
Fractures of the Posterior Cranial Fossa
In fractures of the posterior cranial fossa, blood may escape into
the nape of the neck deep to the postvertebral muscles. Some
-
terior triangle, close to the mastoid process. The mucous mem-
brane of the roof of the nasopharynx may be torn, and blood may
escape there. In fractures involving the jugular foramen, the 9th,
walls of the hypoglossal canal usually protect the hypoglossal
Fractures of Facial Bones
Bone Injuries and Skeletal Development
-
periosteal surfaces of the alveolar parts of the upper and lower
jaws means that most facial fractures should be considered to
be open fractures, susceptible to infection, and requiring anti-
Anatomy of Common Facial Fractures
Automobile accidents, fisticuffs, and falls are common causes of
-
oped from membrane (whereas the remainder is developed from
flexible and can absorb considerable force without resulting in
a fracture.
Signs of fractures of the facial bones include deformity, ocu-
lar displacement, or abnormal movement accompanied by crepi-
tation and malocclusion of the teeth. Anesthesia or paresthesia
of the facial skin will follow fracture of bones through which
branches of the trigeminal nerve pass to the skin.
The muscles of the face are thin and weak and cause little
displacement of the bone fragments. Once a fracture of the
maxilla has been reduced, for example, prolonged fixation is
not needed. However, in the case of the mandible, the strong
muscles of mastication can create considerable displacement,
requiring long periods of fixation.
The most common facial fractures involve the nasal bones,
followed by the zygomatic bone and then the mandible. To frac-
ture the maxillary bones and the supraorbital ridges of the frontal
bones, an enormous force is required.
Nasal Fractures
Fractures of the nasal bones, because of the prominence of the
nose, are the most common facial fractures. Because the bones
are lined with mucoperiosteum, the fracture is considered open;
the overlying skin may also be lacerated. Although most are sim-
ple fractures and are reduced under local anesthesia, some are
associated with severe injuries to the nasal septum and require
careful treatment under general anesthesia.
Maxillofacial Fractures
facial trauma. There is extensive facial swelling, midface mobil-
fluid (cerebrospinal rhinorrhea) secondary to fracture of the crib-
present, owing to orbital wall damage. Involvement of the infraor-
and upper gum may occur in fractures of the body of the maxilla.
C L I N I C A L N O T E S
(continued)
538
CHAPTER 11
The Head and Neck
Nose bleeding may also occur in maxillary fractures. Blood
can no longer be palpated.
the end of the 1st year, the fontanelle is usually closed and
parietal bones in front and the occipital bone behind. By
is triangular and lies between the two
posterior fontanelle
replaced by bone and is closed by 18 months of age. The
membrane forming the floor of the anterior fontanelle is
the two parietal bones behind (Fig. 11.8). The fibrous
between the two halves of the frontal bone in front and
is diamond shaped and lies
anterior fontanelle
The
midline of the vault.
nelles are most important and are easily examined in the
Clinically, the anterior and posterior fonta
fontanelles.
are separated by unossified membranous intervals called
the vault are not closely knit at sutures, as in the adult, but
the bones of the base are ossified in cartilage. The bones of
cartilage. The bones of the vault are ossified in membrane;
mobile on each other, being connected by fibrous tissue or
at birth, but the process is incomplete, and the bones are
being no diploë present. Most of the skull bones are ossified
The bones of the skull are smooth and unilaminar, there
results in a great increase in length of the face.
illary sinuses, and the alveolar processes of the maxillae
face. In childhood, the growth of the mandible, the max
skull, has a disproportionately large cranium relative to the
The newborn skull (Fig. 11.8), compared with the adult
tents of the orbital cavity to explode downward through the floor
enters the maxillary air sinus and then leaks into the nasal cavity.
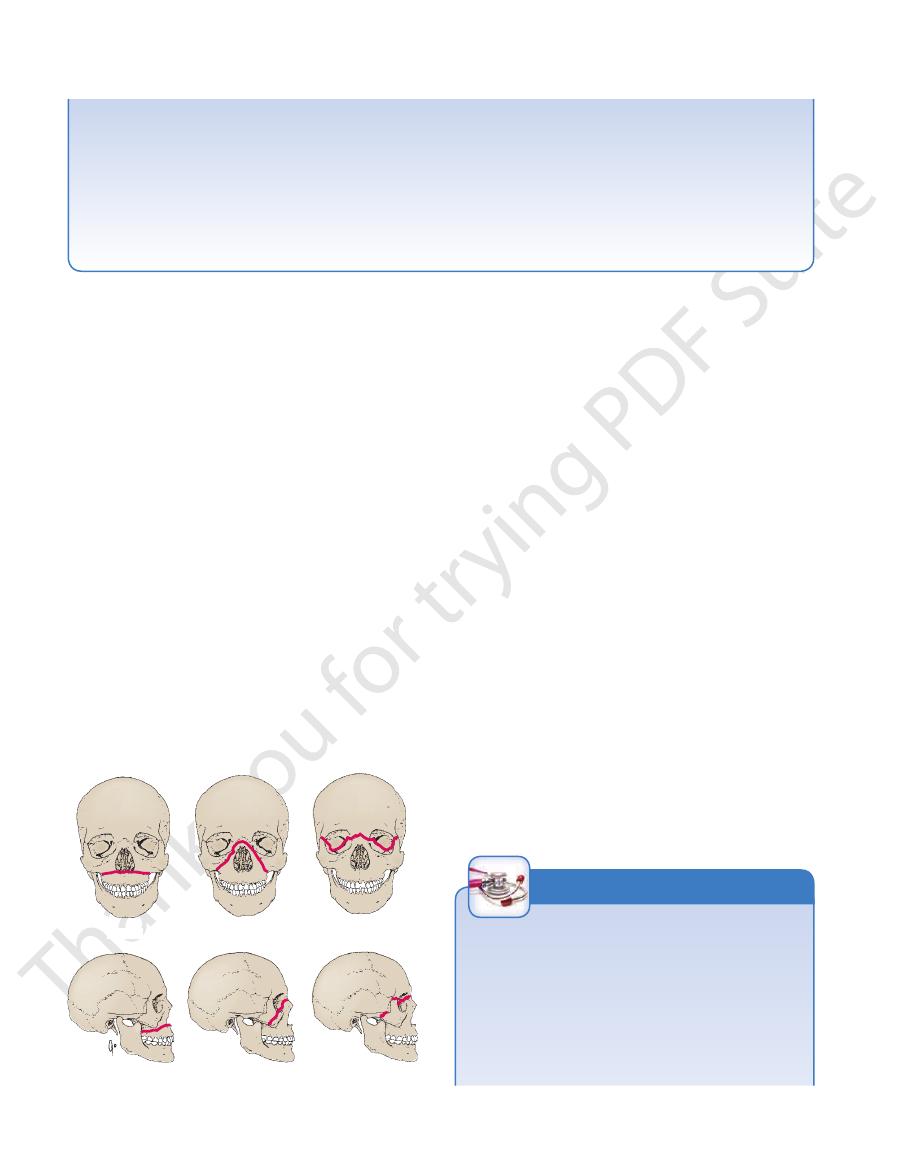
The sites of the fractures were classified by Le Fort as type I,
II, or III; these fractures are summarized in Figure 11.7.
Blowout Fractures of the Maxilla
A severe blow to the orbit (as from a baseball) may cause the con-
of the orbit into the maxillary sinus. Damage to the infraorbital
nerve, resulting in altered sensation to the skin of the cheek,
upper lip, and gum, may occur.
Fractures of the Zygoma or Zygomatic Arch
The zygoma or zygomatic arch can be fractured by a blow to the
side of the face. Although it can occur as an isolated fracture,
as from a blow from a clenched fist, it may be associated with
multiple other fractures of the face, as often seen in automobile
accidents.
Neonatal Skull
-
-
Le Fort I
Le Fort II
Le Fort III
FIGURE 11.7
Le Fort classification of maxillofacial fractures.
head is bent posteriorly.
smaller, the ramus becomes oblique in position so that the
the teeth are lost. As the alveolar part of the bone becomes
In old age, the size of the mandible is reduced when
than the coronoid process.
the head and neck grow so that the head comes to lie higher
that the angle of the mandible assumes the adult shape and
the head. It is only after eruption of the permanent teeth
body and the coronoid process lying at a superior level to
the head being placed level with the upper margin of the
at birth is obtuse (Fig. 11.8),
angle of the mandible
The
by the end of the 1st year.
symphysis menti
the midline with fibrous tissue. The two halves fuse at the
The mandible has right and left halves at birth, united in
surface.
puberty the antrum may lie as much as 15 mm from the
skull continues, the lateral bony wall thickens so that at
As growth of the
suprameatal triangle.
the floor of the
At birth, the mastoid antrum lies about 3 mm deep to
omastoid muscle when the child moves his or her head.
and develops later in response to the pull of the sternocleid
is not present at birth (Fig. 11.8)
mastoid process
The
tympanic membrane comes to face more directly laterally.
grows laterally, forming the bony part of the meatus, and the
faces more inferiorly. During childhood, the tympanic plate
the tympanic membrane is nearly as large as in the adult, it
is nearer the surface. Although
tympanic membrane
meatus is almost entirely cartilaginous in the newborn, and
plate in the adult. This means that the external auditory
C-shaped ring at birth, compared with a C-shaped curved
is merely a
tympanic part of the temporal bone
The
The red line denotes the fracture line.
the
-
Clinical Features of the Neonatal Skull
state of the intracranial pressure (a bulging fontanelle indi
Fontanelles
Palpation of the fontanelles enables the physician to deter-
mine the progress of growth in the surrounding bones, the
degree of hydration of the baby (e.g., if the fontanelles are
depressed below the surface, the baby is dehydrated), and the
-
cates raised intracranial pressure).
C L I N I C A L N O T E S
(continued)
Basic Anatomy
539
Samples of cerebrospinal fluid can be obtained by passing
men, is close to the surface. Thus, it can be damaged by for
and the facial nerve, as it emerges from the stylomastoid fora
fontanelle after 18 months, because the frontal and parietal
a long needle obliquely through the anterior fontanelle into the
subarachnoid space or even into the lateral ventricle.
Clinically, it is usually not possible to palpate the anterior
bones have enlarged to close the gap.
Tympanic Membrane
At birth, the tympanic membrane faces more downward and
less laterally than in maturity; when examined with the oto-
scope, it therefore lies more obliquely in the infant than in the
adult.
Forceps Delivery and the Facial Nerve
In the newborn infant, the mastoid process is not developed,
-
-
ceps in a difficult delivery.
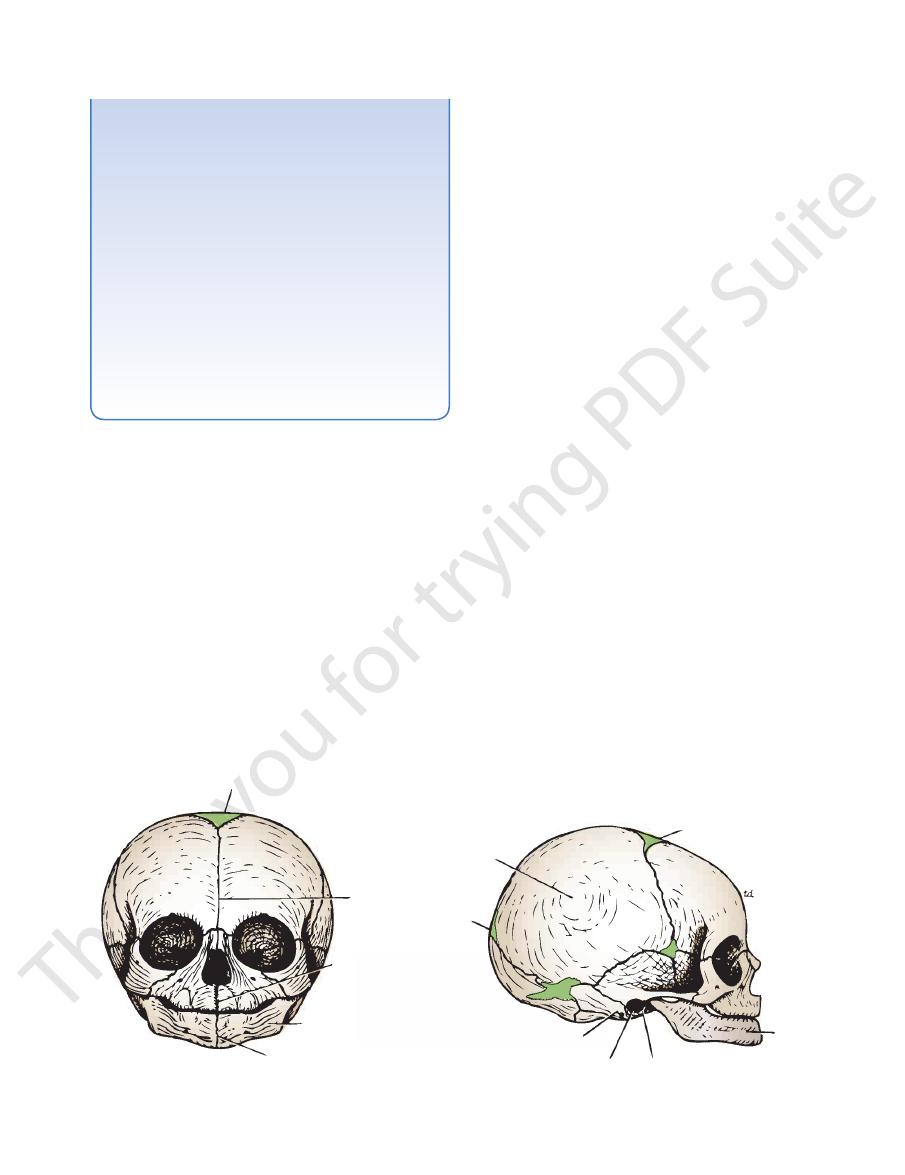
anterior fontanelle
frontal
suture
intermaxillary
suture
mandible
symphysis menti
anterior fontanelle
mandible
tympanic part of temporal bone
tympanic membrane
stylomastoid foramen
posterior
fontanelle
parietal
eminence
A
B
FIGURE 11.8
Neonatal skull as seen from the anterior
The brain in the skull is surrounded by three protective
(A) and lateral (B) aspects.
The Meninges
membranes, or meninges: the dura mater, the arachnoid
mater, and the pia mater. (The spinal cord in the vertebral
column is also surrounded by three meninges. See page 699.)
lateral wall of the cavernous sinus (Figs. 11.11 and 11.12).
the third and fourth cranial nerves pass forward to enter the
cess on each side. At the point where the two borders cross,
the attached border, and is affixed to the anterior clinoid pro
bone. The free border runs forward at its two ends, crosses
of the grooves for the transverse sinuses on the occipital
the superior borders of the petrous bones, and the margins
fixed border is attached to the posterior clinoid processes,
inner free border and an outer attached or fixed border. The
of the midbrain (Figs. 11.11 and 11.12), thus producing an
for the passage
tentorial notch,
spheres. In front is a gap, the
lum and supports the occipital lobes of the cerebral hemi
11.10, and 11.11). It covers the upper surface of the cerebel
mater that roofs over the posterior cranial fossa (Figs. 11.9,
is a crescent-shaped fold of dura
tentorium cerebelli
The
sinus runs along its attachment to the tentorium cerebelli.
sinus runs in its lower concave free margin, and the straight
sinus runs in its upper fixed margin, the inferior sagittal
surface of the tentorium cerebelli. The superior sagittal
broad posterior part blends in the midline with the upper
attached to the internal frontal crest and the crista galli. Its
spheres (Figs. 11.9 and 11.13). Its narrow end in front is
that lies in the midline between the two cerebral hemi
is a sickle-shaped fold of dura mater
falx cerebri
The
to restrict the rotatory displacement of the brain.
the subdivisions of the brain. The function of these septa is
the cranial cavity into freely communicating spaces lodging
The meningeal layer sends inward four septa that divide
rium of the nerves.
skull. Outside the skull, the sheaths fuse with the epineu
cranial nerves as the latter pass through the foramina in the
mater of the spinal cord. It provides tubular sheaths for the
continuous through the foramen magnum with the dura
dense, strong, fibrous membrane covering the brain and is
is the dura mater proper. It is a
meningeal layer
The
base of the skull.
ments. It is most strongly adherent to the bones over the
bones. At the sutures, it is continuous with the sutural liga
continuous with the periosteum on the outside of the skull
the margins of all the foramina in the skull, it becomes
continuous with the dura mater of the spinal cord. Around
through the foramen magnum to become
does not extend
It
periosteum covering the inner surface of the skull bones.
is nothing more than the ordinary
endosteal layer
The
they separate to form venous sinuses.
These are closely united except along certain lines, where
the endosteal layer and the meningeal layer (Fig. 11.2).
The dura mater is conventionally described as two layers:
Dura Mater of the Brain
-
-
-
-
-
-
540
CHAPTER 11
The Head and Neck
superficial vein of scalp
emissary vein
diploic vein
cerebral vein
left transverse sinus
great cerebral vein
falx cerebri
confluence
of sinuses
straight sinus
tentorium cerebelli
right transverse sinus
sigmoid sinus
superior petrosal sinus
facial vein
ophthalmic vein
cavernous sinus
sphenoparietal
sinus
intercavernous sinuses
oculomotor nerve
trochlear nerve
trigeminal nerve
facial and
vestibulocochlear
nerves
diploe
inferior sagittal sinus
superior sagittal sinus
olfactory bulb
¨
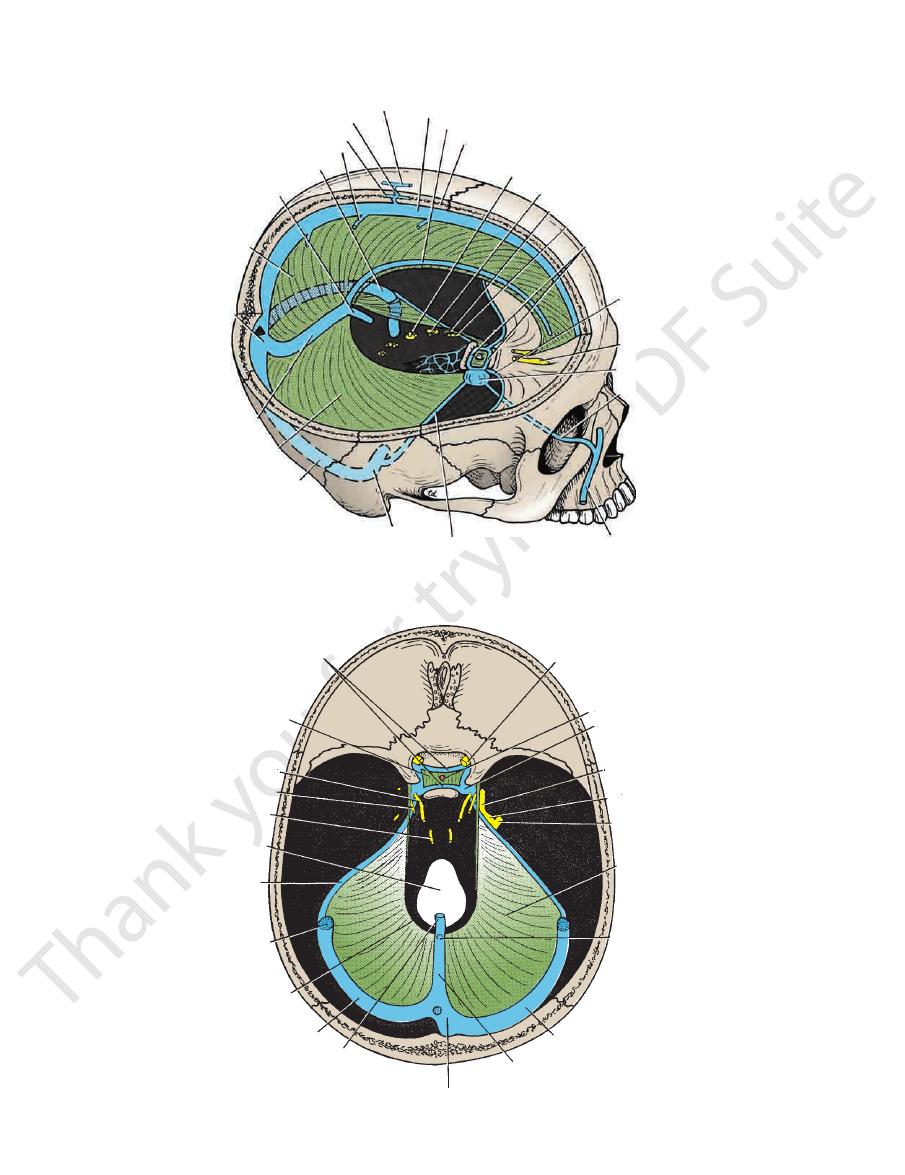
FIGURE 11.9
Interior of the skull showing the dura mater and its contained venous sinuses. Note the connections of the
veins of the scalp and the veins of the face with the venous sinuses.
intercavernous sinuses
diaphragma sellae
oculomotor nerve
trochlear nerve
abducent nerve
foramen magnum
superior
petrosal sinus
sigmoid sinus
tentorial notch
left transverse sinus
great cerebral vein
confluence of sinuses
straight sinus
right transverse sinus
inferior sagittal
sinus
tentorium
cerebelli
mandibular nerve
trigeminal ganglion
maxillary nerve
cavernous sinus
infundibulum
optic nerve
FIGURE 11.10
Diaphragma sellae and tentorium cerebelli. Note the position of the venous sinuses.

Basic Anatomy
541
tentorium cerebelli
midbrain (sectioned)
cerebral aqueduct
trochlear
nerve
internal
carotid
artery
trigeminal
nerve
cut margin of
meningeal layer of
dura
greater superficial
petrosal nerve
mandibular division of
trigeminal nerve
trigeminal
ganglion
maxillary division of
trigeminal nerve
trochlear nerve
internal carotid artery
right optic nerve
olfactory bulb
frontal sinus
optic chiasma
infundibulum
posterior communicating artery
posterior cerebral artery
inferior sagittal sinus (cut open)
falx cerebri
abducent nerve
internal carotid artery
oculomotor nerve
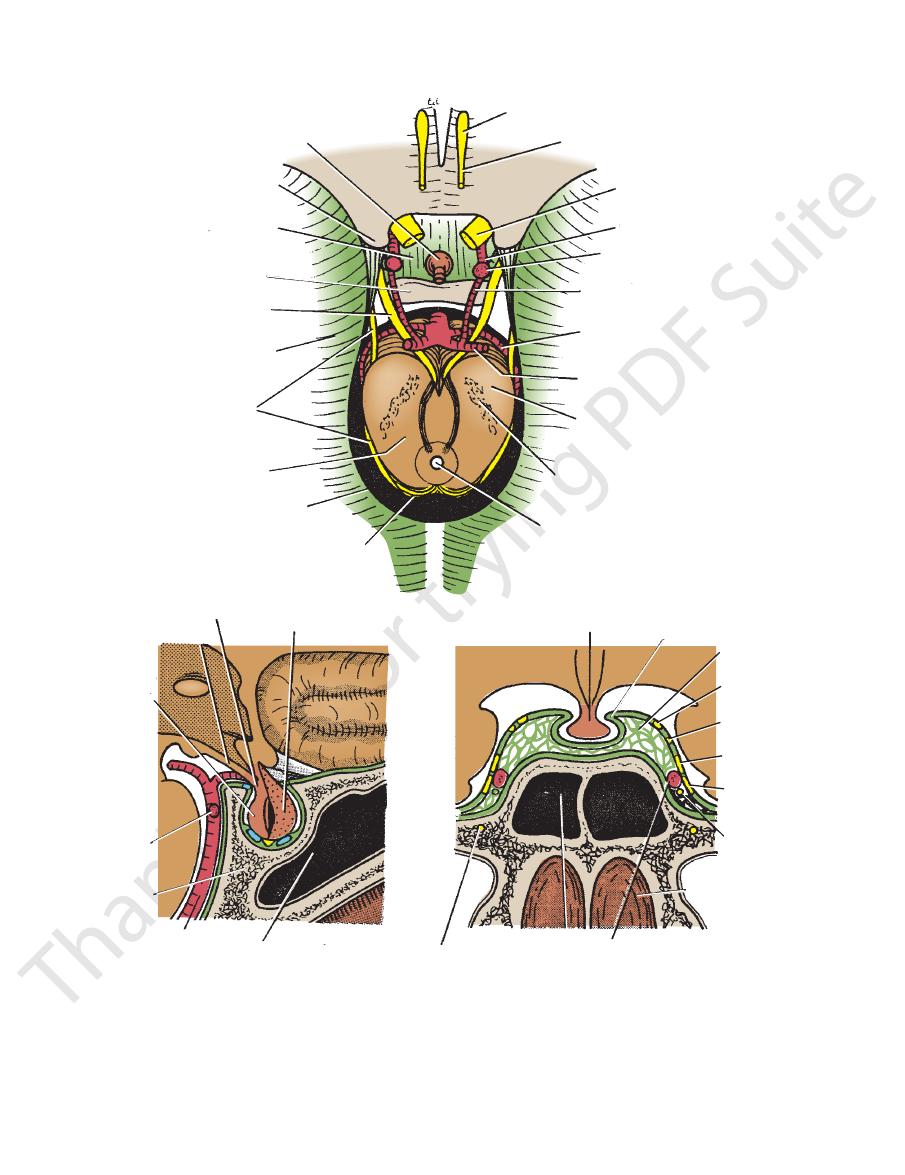
FIGURE 11.11
Lateral view of the skull showing the falx cerebri, tentorium cerebelli, brainstem, and trigeminal ganglion.
supplies the posterior part of the dura mater.
brain. The posterior (parietal) branch curves backward and
roughly to the line of the underlying precentral gyrus of the
rior angle of the parietal bone, and its course corresponds
(frontal) branch deeply grooves or tunnels the anteroinfe
middle cranial fossa is described on page 598. The anterior
Its further course in the
geal and endosteal layers of dura.
lie between the menin
through the foramen spinosum to
ral bone (Fig. 11.20). To enter the cranial cavity, it passes
on the upper surface of the squamous part of the tempo
the cranial cavity and runs forward and laterally in a groove
artery in the infratemporal fossa (see page 598). It enters
arises from the maxillary
middle meningeal artery
The
damaged in head injuries.
tant is the middle meningeal artery, which is commonly
tebral arteries. From a clinical standpoint, the most impor
carotid, maxillary, ascending pharyngeal, occipital, and ver
Numerous arteries supply the dura mater from the internal
Dural Arterial Supply
greater occipital nerve.
the neck and back of the scalp along the distribution of the
level of the tentorium produces referred pain to the back of
of the head. Stimulation of the dural endings below the
produces referred pain to an area of skin on the same side
trigeminal nerve above the level of the tentorium cerebelli
of headache. Stimulation of the sensory endings of the
is sensitive to stretching, which produces the sensation
Numerous sensory endings are in the dura. The dura
the dura.
nerves and branches from the sympathetic system pass to
Branches of the trigeminal, vagus, and first three cervical
pituitary gland (Fig. 11.12).
small opening in its center allows passage of the stalk of the
mater that forms the roof for the sella turcica (Fig. 11.6). A
is a small circular fold of dura
diaphragma sellae
The
Its posterior fixed margin contains the occipital sinus.
projects forward between the two cerebellar hemispheres.
mater that is attached to the internal occipital crest and
is a small, sickle-shaped fold of dura
falx cerebelli
The
to the occipital bone (Fig. 11.10).
petrous bone, and the transverse sinus along its attachment
ebri, the superior petrosal sinus along its attachment to the
The straight sinus runs along its attachment to the falx cer
upper and lower surfaces of the tentorium, respectively.
The falx cerebri and the falx cerebelli are attached to the
trigeminal nerve and the trigeminal ganglion (Fig. 11.11).
beneath the superior petrosal sinus to form a recess for the
bone, the lower layer of the tentorium is pouched forward
Close to the apex of the petrous part of the temporal
-
Dural Nerve Supply
-
-
-
-
-
542
CHAPTER 11
The Head and Neck
hypophysis cerebri
anterior clinoid process
diaphragma sellae
dorsum sellae
oculomotor nerve
tentorium cerebelli
trochlear nerve
tegmentum
tentorial notch
superior colliculus
cerebral aqueduct
substantia nigra
crus cerebri
posterior cerebral artery
superior cerebellar artery
posterior communicating artery
internal carotid artery
ophthalmic artery
optic nerve
olfactory tract
olfactory bulb
infundibulum
tuber cinereum
posterior
lobe
posterior
cerebral
artery
body of
sphenoid
basilar artery
sphenoidal sinus
anterior lobe
hypophysis cerebri
diaphragma sellae
cavernous
sinus
oculomotor
nerve
trochlear
nerve
ophthalmic
nerve
maxillary
nerve
abducent
nerve
cavity of nose
internal carotid artery
sphenoidal sinus
nerve of pterygoid canal
A
B
C
FIGURE 11.12
A.
nial nerves.
through the body of the sphenoid showing the hypophysis cerebri and the cavernous sinuses. Note the position of the cra
Sagittal section through the sella turcica showing the hypophysis cerebri.
The forebrain has been removed, leaving the midbrain, the hypophysis cerebri, and the internal carotid and
basilar arteries in position. B.
C. Coronal section
-
Basic Anatomy
are widely separated to form the
the brain, and in certain situations the arachnoid and pia
The arachnoid bridges over the sulci on the surface of
cerebrospinal fluid.
is filled with
which
subarachnoid space,
and from the pia by the
space,
subdural
separated from the dura by a potential space, the
internally and the dura mater externally (Fig. 11.2). It is
brane covering the brain and lying between the pia mater
The arachnoid mater is a delicate, impermeable mem
Arachnoid Mater of the Brain
the arteries.
plexus or the sphenoparietal sinus. The veins lie lateral to
dle meningeal artery and drains into the pterygoid venous
middle meningeal vein follows the branches of the mid
lie in the endosteal layer of dura. The
meningeal veins
The
Dural Venous Drainage
543
-
-
subarachnoid cisternae.
ies and veins lie in the space, as do the cranial nerves
through the subarachnoid space. All the cerebral arter
and from the brain to the skull or its foramina must pass
It is important to remember that structures passing to
cerebrospinal fluid diffuses into the bloodstream.
(Fig. 11.2). Arachnoid villi serve as sites where the
lations
arachnoid granu
tions of arachnoid villi are referred to as
most numerous along the superior sagittal sinus. Aggrega
The arachnoid villi are
arachnoid villi.
sinuses to form
In certain areas, the arachnoid projects into the venous
-
-
-
(Fig. 11.2). The arachnoid fuses with the epineurium of the
the substance of the brain carry a sheath of pia with them.
fuses with their epineurium. The cerebral arteries entering
est sulci (Fig. 11.2). It extends over the cranial nerves and
the brain, covering the gyri and descending into the deep
The pia mater is a vascular membrane that closely invests
Pia Mater of the Brain
tively protects the brain from trauma.
medium in which the brain floats. This mechanism effec
neuronal activity, the cerebrospinal fluid provides a fluid
In addition to removing waste products associated with
fusing through their walls.
the bloodstream by passing into the arachnoid villi and dif
(see Fig. 12.7). Eventually, the fluid enters
sacral vertebra
second
subarachnoid space extends down as far as the
spheres and downward around the spinal cord. The spinal
culates both upward over the surfaces of the cerebral hemi
ventricle and so enters the subarachnoid space. It now cir
brain through the three foramina in the roof of the fourth
of the brain. It escapes from the ventricular system of the
within the lateral, third, and fourth ventricles
choroid
is produced by the
cerebrospinal fluid
The
as the eyeball (see page 554).
subarachnoid space extends around the optic nerve as far
fuses with the sclera of the eyeball (Fig. 11.25). Thus, the
extends into the orbital cavity through the optic canal and
optic nerve, the arachnoid forms a sheath for the nerve that
nerves at their point of exit from the skull. In the case of the
plexuses
-
-
-
-
-
Intracranial Hemorrhage
ily blood-stained cerebrospinal fluid through a lumbar puncture
from an angioma. The symptoms, which are sudden in onset,
toms. In both forms, the blood clot must be removed through burr
depending on the speed of accumulation of fluid in the subdu
Acute and chronic forms of the clinical condition occur,
to accumulate in the potential space between the dura and the
tal sinus. The cause is usually a blow on the front or the back of
To stop the hemorrhage, the torn artery or vein must be
vascular lesions. Four varieties are considered here: extradural,
Intracranial hemorrhage may result from trauma or cerebral
subdural, subarachnoid, and cerebral.
Extradural hemorrhage results from injuries to the meningeal
arteries or veins. The most common artery to be damaged is the
anterior division of the middle meningeal artery. A comparatively
minor blow to the side of the head, resulting in fracture of the
skull in the region of the anteroinferior portion of the parietal
bone, may sever the artery. The arterial or venous injury is espe-
cially liable to occur if the artery and vein enter a bony canal in
this region. Bleeding occurs and strips up the meningeal layer of
dura from the internal surface of the skull. The intracranial pres-
sure rises, and the enlarging blood clot exerts local pressure on
the underlying motor area in the precentral gyrus. Blood may
also pass outward through the fracture line to form a soft swell-
ing under the temporalis muscle.
ligated or plugged. The burr hole through the skull wall should
be placed about 1 to 1.5 in. (2.5 to 4 cm) above the midpoint of the
zygomatic arch.
Subdural hemorrhage results from tearing of the superior
cerebral veins at their point of entrance into the superior sagit-
the head, causing excessive anteroposterior displacement of the
brain within the skull.
This condition, which is much more common than middle
meningeal hemorrhage, can be produced by a sudden minor
blow. Once the vein is torn, blood under low pressure begins
arachnoid. In about half the cases, the condition is bilateral.
-
ral space. For example, if the patient starts to vomit, the venous
pressure will rise as a result of a rise in the intrathoracic pres-
sure. Under these circumstances, the subdural blood clot will
increase rapidly in size and produce acute symptoms. In the
chronic form, over a course of several months, the small blood
clot will attract fluid by osmosis so that a hemorrhagic cyst is
formed, which gradually expands and produces pressure symp-
holes in the skull.
Subarachnoid hemorrhage results from leakage or rupture of
a congenital aneurysm on the circle of Willis or, less commonly,
include severe headache, stiffness of the neck, and loss of con-
sciousness. The diagnosis is established by withdrawing heav-
(spinal tap).
C L I N I C A L N O T E S
(continued)

544
CHAPTER 11
The Head and Neck
Cerebral hemorrhage
The pituitary gland, which lies medially in the sella
nerve (Fig. 11.12).
the ophthalmic and maxillary divisions of the 5th cranial
In the lateral wall, the 3rd and 4th cranial nerves, and
which travel through it (Fig. 11.12)
The internal carotid artery and the 6th cranial nerve,
the Cavernous Sinuses
Important Structures Associated with
connect the two cavernous sinuses through the sella turcica.
through the superior petrosal sinus. Intercavernous sinuses
ina. The sinus drains posteriorly into the transverse sinus
the inferior ophthalmic vein and the central vein of the ret
the sphenoid bone (Fig. 11.9). Anteriorly, the sinus receives
lies on the lateral side of the body of
cavernous sinus
Each
through the foramen magnum and the transverse sinuses.
falx cerebelli. It communicates with the vertebral veins
lies in the attached margin of the
occipital sinus
The
jugular vein (Fig. 11.30).
skull through the jugular foramen to become the internal
mastoid antrum of the temporal bone and then leaves the
transverse sinuses. Each sinus turns downward behind the
are a direct continuation of the
sigmoid sinuses
The
the sigmoid sinus.
tentorium cerebelli, and they end on each side by becoming
11.10). Each sinus lies in the lateral attached margin of the
usually a continuation of the straight sinus (Figs. 11.9 and
left transverse sinus
of the superior sagittal sinus; the
begins as a continuation
right transverse sinus
The
vein, it drains into the left transverse sinus.
union of the inferior sagittal sinus with the great cerebral
ebri with the tentorium cerebelli (Fig. 11.9). Formed by the
lies at the junction of the falx cer
straight sinus
The
veins from the medial surface of the cerebral hemisphere.
vein to form the straight sinus (Fig. 11.9). It receives cerebral
the falx cerebri. It runs backward and joins the great cerebral
lies in the free lower margin of
inferior sagittal sinus
The
superior cerebral veins.
lacunae (Fig. 11.2). The superior sagittal sinus receives the
Numerous arachnoid villi and granulations project into the
venous lacunae.
sinus communicates on each side with the
becomes continuous with the right transverse sinus. The
der of the falx cerebri (Fig. 11.9). It runs backward and
lies in the upper fixed bor
superior sagittal sinus
The
diploë of the skull, the orbit, and the internal ear.
have no valves. They receive tributaries from the brain, the
of fibrous tissue; they have no muscular tissue. The sinuses
are lined by endothelium. Their walls are thick and composed
situated between the layers of the dura mater (Fig. 11.2); they
The venous sinuses of the cranial cavity are blood-filled spaces
The Venous Blood Sinuses
the
great cerebral veins,
Bleeding then takes place from the
anteroposterior compression of the head often tears the ante
occur from the cerebral veins or the venous sinuses. Excessive
diately loses consciousness, and the paralysis is evident when
is generally caused by rupture of the
thin-walled lenticulostriate artery, a branch of the middle cere-
bral artery. The hemorrhage involves the vital corticobulbar
and corticospinal fibers in the internal capsule and produces
hemiplegia on the opposite side of the body. The patient imme-
consciousness is regained.
Intracranial Hemorrhage in the Infant
Intracranial hemorrhage in the infant may occur during birth and
may result from excessive molding of the head. Bleeding may
-
rior attachment of the falx cerebri from the tentorium cerebelli.
straight sinus, or the inferior sagittal sinus.
-
-
is
-
■
■
■
■
■
■
turcica (Fig.11.12)
The veins of the face, which are connected with
■
■
the cavernous sinus via the facial vein and inferior
ophthalmic vein, are an important route for the spread
of infection from the face (Fig. 11.9)
described.
the following account, only the main parts of the brain are
brain, a textbook of neuroanatomy should be consulted. In
For a detailed description of the gross structure of the
gland is vital to life and is fully described on page 652.
tion in the sella turcica of the sphenoid bone. The pituitary
11.12). The gland is well protected by virtue of its loca
(Fig.
infundibulum
the undersurface of the brain by the
The pituitary gland is a small, oval structure attached to
Pituitary Gland (Hypophysis Cerebri)
the temporal bone (Fig. 11.9)
along the upper and lower borders of the petrous part of
which run
inferior petrosal sinuses,
superior
The
■
■
and
-
Parts of the Brain
Major Parts of the Brain
Cavities of the Brain
Forebrain
Cerebrum
Diencephalon
Right and left lateral
ventricles
Third ventricle
Midbrain
Hindbrain
Pons
Medullaoblongata
Cerebellum
Cerebral aqueduct
Fourth ventricle
and central
canal
bones; above the anterior and middle cranial fossae; and,
Each hemisphere extends from the frontal to the occipital
(Fig. 11.13).
corpus callosum
of white matter called the
connected by a mass
cerebral hemispheres
sists of two
is the largest part of the brain and con
cerebrum
The
cord through the foramen magnum.
lies inside the cranial cavity. It is continuous with the spinal
The brain is that part of the central nervous system that
Cerebrum
-
posteriorly, above the tentorium cerebelli. The hemispheres
(Fig. 11.2). The cerebral
gray matter
and is composed of
cortex
The surface layer of each hemisphere is called the
(Fig. 11.13).
falx cerebri
which projects the
into
longitudinal fissure,
are separated by a deep cleft, the