556
CHAPTER 11
The Head and Neck
pterygoid venous plexus. Both veins pass
ough
backward thr
the superior orbital fissure and drain into the
nous sinus.
caver
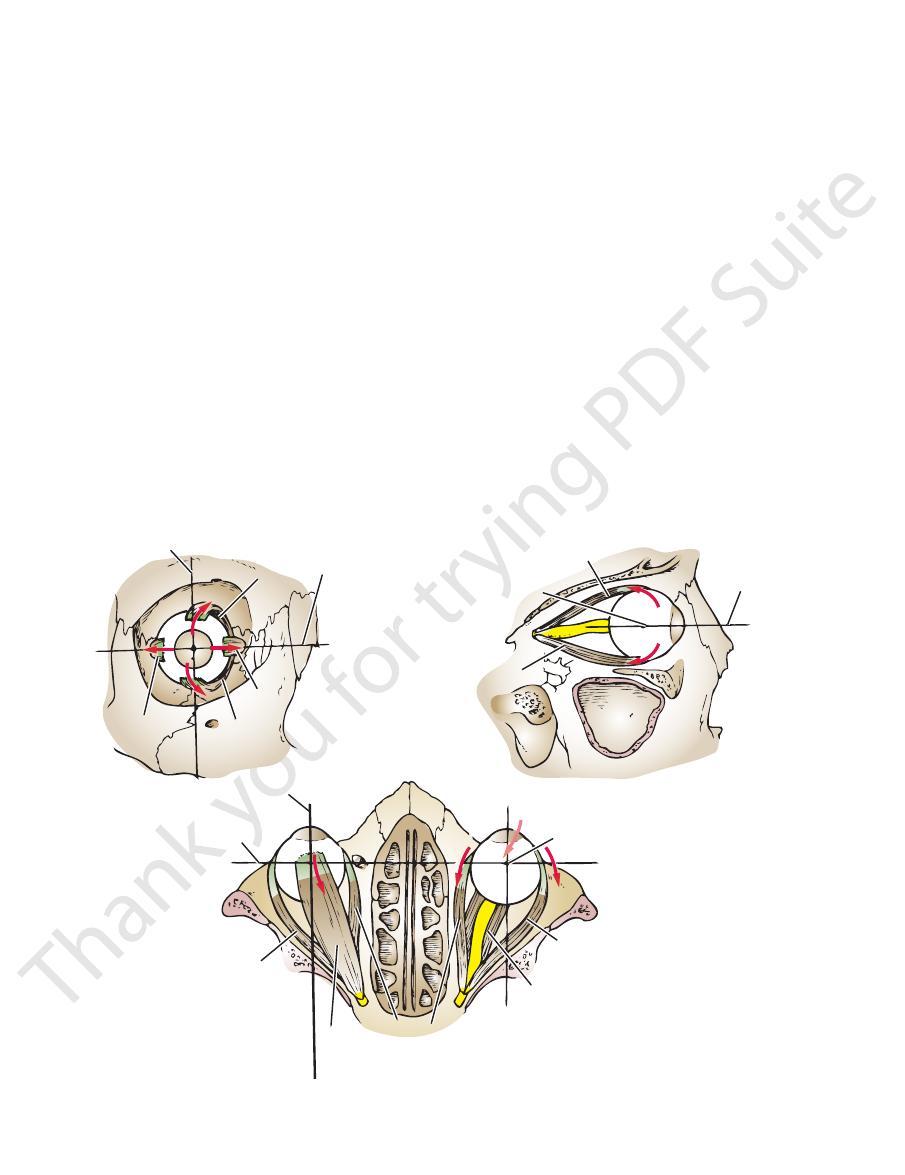
(Fig. 11.21). For the superior
rotate it medially
but also
they not only raise and depress the cornea, respectively,
on the medial side of the vertical axis of the eyeball,
Because the superior and the inferior recti are inserted
oblique muscles.
inferior
superior
lateral rectus,
rectus,
medial
inferior rectus,
superior rectus,
are the
wall of the orbital cavity to the eyeball (Fig. 11.18). These
There are six voluntary muscles that run from the posterior
Eye
Extrinsic Muscles Producing Movement of the
marker. The eye rotates either medially or laterally.
the eyeball use the upper rim of the cornea (or pupil) as the
is the rotation of the eye medially. Rotatory movements of
adduction
is the rotation of the eye laterally, and
abduction
is the rotation of the eye downward,
depression
upward,
is the rotation of the eye
Elevation
becomes as follows:
(horizontal, vertical, and sagittal). The terminology then
of the anterior pole as it rotates on any one of the three axes
of the eye are then related to the direction of the movement
as the anatomic “anterior pole” of the eye. All movements
The center of the cornea or the center of the pupil is used
Terms Used in Describing Eye Movements
or nodes are present in the orbital cavity.
No lymph vessels
Lymph Vessels
The Eye
Movements of the Eyeball
the
the
the
and the
and
rectus muscle to raise the cornea directly upward, the
inferior oblique muscle must assist; for the inferior
us
rect
carefully Figure 11.24.
muscles of the eyeball are summarized in Table 11.2. Study
The origins, insertions, nerve supply, and actions of the
rectus muscle.
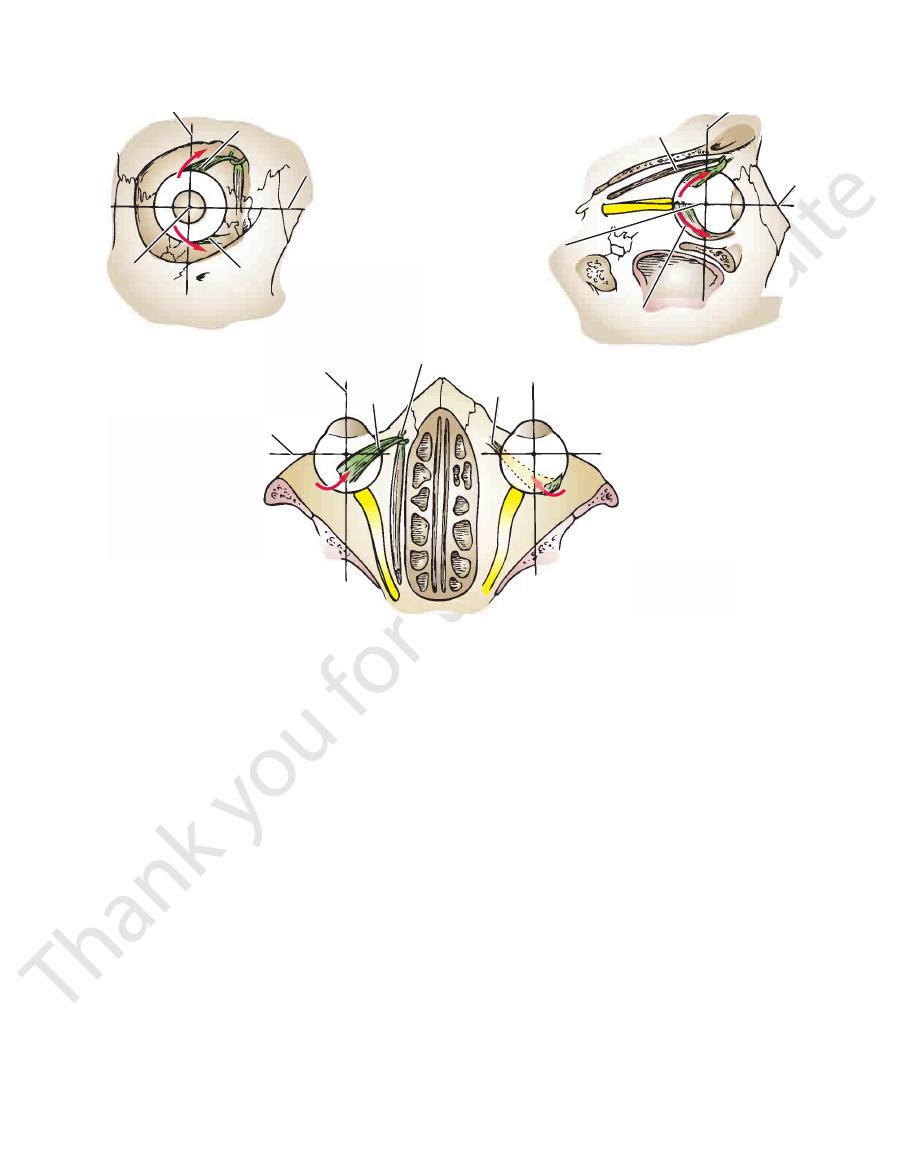
erally and is inserted into the sclera beneath the superior
the frontal bone. The tendon now turns backward and lat
through a fibrocartilaginous pulley (trochlea) attached to
that the tendon of the superior oblique muscle passes
oblique muscle must assist (Figs. 11.21 and 11.22). Note
to depress the cornea directly downward, the superior
-
vertical axis
superior
rectus
transverse axis
medial
rectus
inferior
rectus
lateral
rectus
superior rectus
transverse axis
inferior rectus
sagittal axis
sagittal axis
transverse axis
lateral rectus
superior
rectus
medial
recti
inferior rectus
lateral rectus
vertical axis
A
B
C
FIGURE 11.21
The actions of the four recti muscles in producing movements of the eyeball.
Basic Anatomy
you are testing the inferior oblique at its best position.
versely, by asking the patient to look medially and upward,
are testing the superior oblique at its best position. Con
medially and downward at the tip of his or her nose, you
the cornea. In other words, when you ask a patient to look
tion to lower (superior oblique) or raise (inferior oblique)
medially, thus placing these muscles in the optimum posi
the action of these muscles by asking the patient first to look
medial and anterior to their insertions. The physician tests
oblique and the origin of the inferior oblique muscles lie
oblique muscles can be tested. The pulley of the superior
Using the same rationale, the superior and inferior
rectus) or lower (inferior rectus) the cornea.
cles are placed in the optimum position to raise (superior
the patient is asked to turn the cornea laterally, these mus
about 23° medial to their insertions, and, therefore, when
The origins of the superior and inferior recti are situated
single action of each muscle predominates (Fig. 11.23).
downward, the physician tests the eye movements where the
a patient is asked to look vertically upward or vertically
superior and inferior oblique muscles are complicated when
Because the actions of the superior and inferior recti and the
and Inferior Recti and the Superior and Inferior
Clinical Testing for the Actions of the Superior
557
Oblique Muscles
-
-
-
rtical axis
ve
superior oblique
oblique
inferior
transverse axis
superior oblique
sagittal
axis
rtical axis
ve
transverse axis
oblique
inferior
oblique
superior
transverse axis
inferior oblique
sagittal axis
sagittal axis
trochlea
A
B
C
FIGURE 11.22
The actions of the superior and inferior oblique muscles in producing movements of the eyeball.
and
medial
of the orbit by triangular ligaments called the
and lateral recti are attached to the medial and lateral walls
tubular sheath. The sheaths for the tendons of the medial
the orbital muscles and is reflected onto each of them as a
socket for free movement. It is perforated by the tendons of
rates the eyeball from the orbital fat and provides it with a
nerve to the corneoscleral junction (Fig. 11.25). It sepa
The fascial sheath surrounds the eyeball from the optic
Fascial Sheath of the Eyeball
cussed later.
take no part in the movement of the eyeball and are dis
dilator pupillae of the iris
constrictor,
ciliary muscle
The involuntary intrinsic muscles are the
Intrinsic Muscles
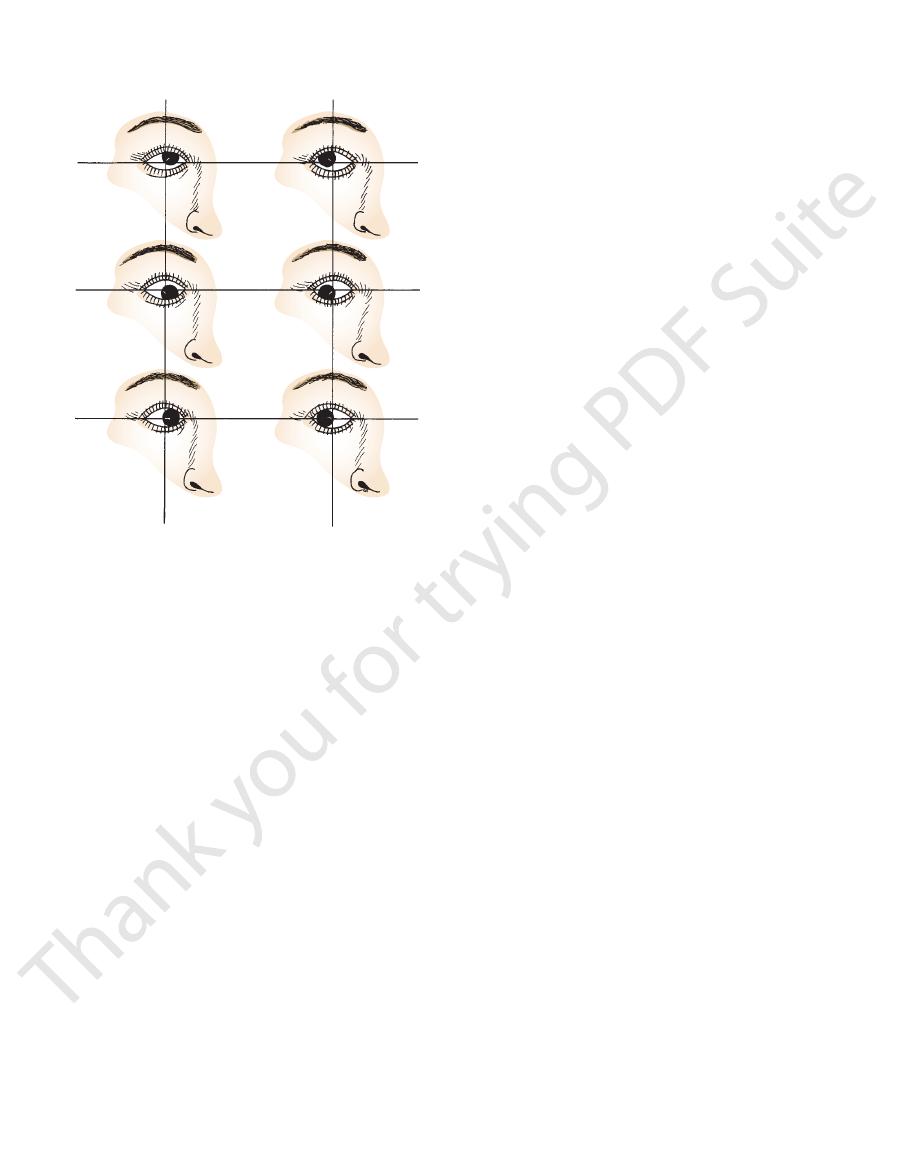
recti and oblique muscles are shown in Figure 11.24.
The cardinal positions of the eyes and the actions of the
rectus.
turning the cornea directly medially tests the medial
her cornea directly laterally tests the lateral rectus and
relative to the eyeball, asking the patient to turn his or
Because the lateral and medial recti are simply placed
and the
and the
-
-
The lower part of the fascial sheath,
lateral check ligaments.
which passes beneath the eyeball and
ts the check
connec
558
CHAPTER 11
central aperture, the pupil (Fig. 11.25). It is suspended in
The iris is a thin, contractile, pigmented diaphragm with a
The Iris and Pupil
refractive power of the lens.
elastic lens becomes more convex. This increases the
relieves the tension in the suspensory ligament, and the
meridianal fibers, pulls the ciliary body forward. This
Contraction of the ciliary muscle, especially the
Action:
ers pass forward to the eyeball in the short ciliary nerves.
synapsing in the ciliary ganglion, the postganglionic fib
asympathetic fibers from the oculomotor nerve. After
is supplied by the par
ciliary muscle
The
Nerve supply:
fewer in number and lie internal to the meridianal fibers.
junction to the ciliary processes. The circular fibers are
fibers run backward from the region of the corneoscleral
anal and circular fibers of smooth muscle. The meridianal
(Fig. 11.25) is composed of meridi
ciliary muscle
The
suspensory ligaments of the lens.
ridges, to the posterior surfaces of which are connected the
are radially arranged folds, or
ciliary processes
The
ciliary striae.
surface has shallow grooves, the
is the posterior part of the body, and its
ciliary ring
The
ciliary processes, and the ciliary muscle.
the iris (Fig. 11.25). It is composed of the ciliary ring, the
roid, and anteriorly it lies behind the peripheral margin of
is continuous posteriorly with the cho
ciliary body
The
an inner, highly vascular layer.
The choroid is composed of an outer pigmented layer and
ward, of the choroid, the ciliary body, and the iris.
The vascular pigmented coat consists, from behind for
Vascular Pigmented Coat
corneal epithelial cells should be stressed.
tear film in maintaining the normal environment for the
differs greatly from that of the air. The importance of the
the cornea, where the refractive index of the cornea (1.38)
eye. This refractive power occurs on the anterior surface of
The cornea is the most important refractive medium of the
Function of the Cornea
division of the trigeminal nerve
Long ciliary nerves from the ophthalmic
Nerve Supply
ous humor and from the capillaries at its edge.
phatic drainage. It is nourished by diffusion from the aque
The cornea is avascular and devoid of lym
Blood Supply
posteriorly with the aqueous humor.
tion of the light entering the eye (Fig. 11.25). It is in contact
is largely responsible for the refrac
cornea
The transparent
corneoscleral junction, or limbus.
sclera is directly continuous in front with the cornea at the
nerves and their associated veins, the venae vorticosae. The
The sclera is also pierced by the ciliary arteries and
the nerve fibers of the optic nerve.
is the area of the sclera that is pierced by
lamina cribrosa
The Head and Neck
The Cornea
-
-
-
-
The Choroid
The Ciliary Body
-
-
■
■
-
-
■
■
superior rectus
inferior oblique
inferior rectus
superior oblique
medial rectus
lateral rectus
FIGURE 11.23
Actions of the four recti and two oblique mus
suspensory ligament of the eye
it is called the
ligaments, is thickened and serves to suspend the eyeball;
page 557.
in the living intact eye are tested clinically, as described on
of the superior and inferior recti and the oblique muscles
horizontal planes should be noted in each case. The actions
alone. The position of the pupil in relation to the vertical and
cles of the right orbit, assuming that each muscle is acting
-
(Fig. 11.25).
fused with the dural sheath of that nerve (Fig. 11.25). The
is white. Posteriorly, it is pierced by the optic nerve and is
The opaque sclera is composed of dense fibrous tissue and
The Sclera
sclera, and an anterior transparent part, the cornea (Fig.
The fibrous coat is made up of a posterior opaque part, the
Fibrous Coat
nervous coat.
are the fibrous coat, the vascular pigmented coat, and the
eyeball consists of three coats, which, from without inward,
separated from it by the fascial sheath of the eyeball. The
The eyeball (Fig. 11.25) is embedded in orbital fat but is
lateral walls of the orbit, as if in a hammock.
By this means, the eye is suspended from the medial and
Structure of the Eye
Coats of the Eyeball
11.25).
Basic Anatomy
559
A
B
C
D
E
F
G
H
I
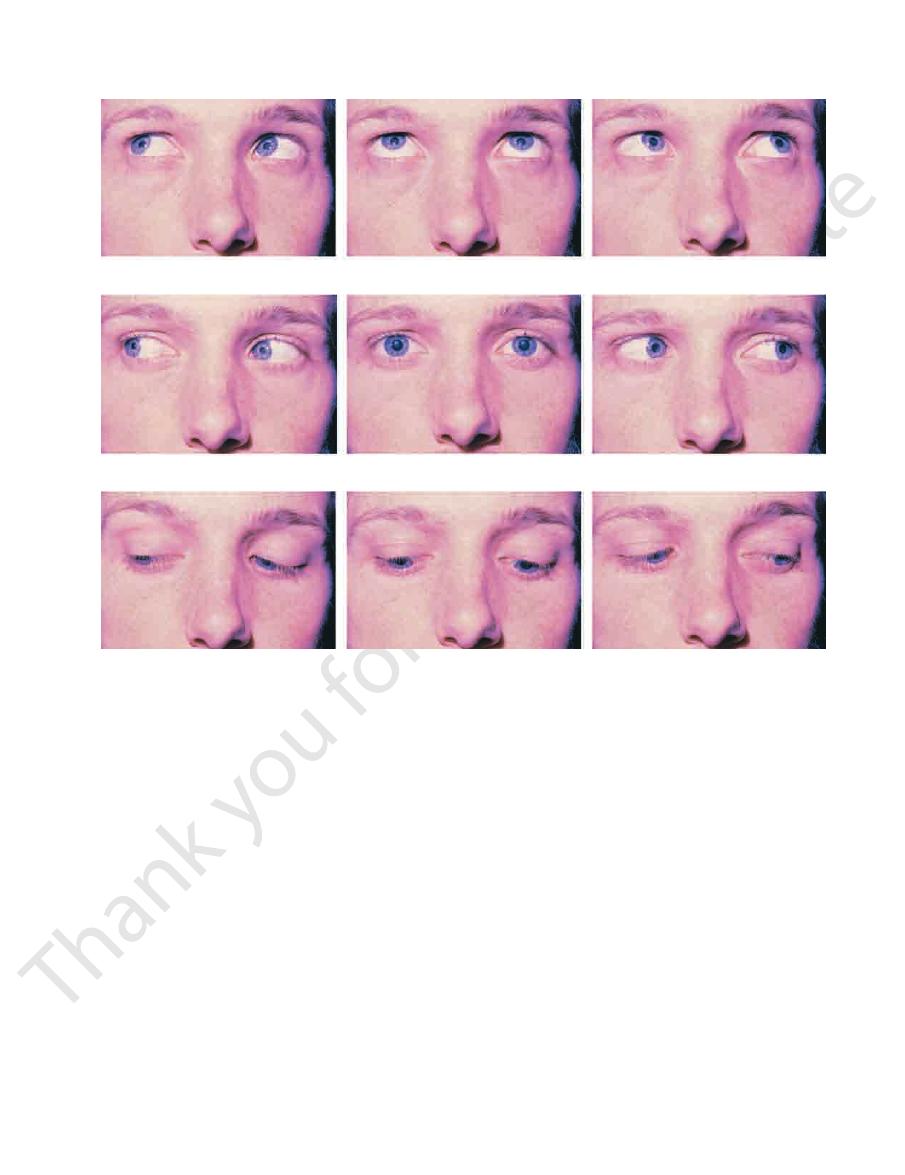
FIGURE 11.24
The cardinal positions of the right and left eyes and the actions of the recti and the oblique muscles principally
of light of low intensity or in the presence of excessive
The dilator pupillae dilates the pupil in the presence
the presence of bright light and during accommodation.
The sphincter pupillae constricts the pupil in
Action:
pass forward to the eyeball in the long ciliary nerves.
is supplied by sympathetic fibers, which
dilator pupillae
pass forward to the eyeball in the short ciliary nerves. The
synapsing in the ciliary ganglion, the postganglionic fibers
parasympathetic fibers from the oculomotor nerve. After
is supplied by
sphincter pupillae
The
Nerve supply:
posterior surface.
consist of a thin sheet of radial fibers that lie close to the
dilator pupillae
the pupil. The radial fibers form the
and are arranged around the margin of
sphincter pupillae
of circular and radiating fibers. The circular fibers form the
The muscle fibers of the iris are involuntary and consist
posterior chamber.
anterior
the cornea into an
the ciliary body. It divides the space between the lens and
periphery of the iris is attached to the anterior surface of
the aqueous humor between the cornea and the lens. The
eye, inferior rectus muscle.
Right eye, superior oblique muscle; left
Both eyes, inferior recti and superior oblique muscles.
Right eye, inferior rectus muscle; left eye,
Right eye, medial rectus muscle; left eye, lateral rectus muscle.
Primary position, with the eyes fixed on a distant fixa
Right eye, lateral rectus muscle; left eye, medial rectus muscle.
Right eye, inferior oblique muscle; left eye, superior rectus muscle.
eyes, superior recti and inferior oblique muscles.
Both
Right eye, superior rectus muscle; left eye, inferior oblique muscle.
responsible for the movements of the eyes. A.
B.
C.
D.
E.
-
tion point. F.
G.
superior oblique muscle. H.
I.
and a
and
■
■
■
■
sympathetic activity such as occurs in fright.
and the back of the iris.
This anterior part of the retina covers the ciliary processes
pigment cells, with a deeper layer of columnar epithelium.
rior part of the retina is nonreceptive and consists merely of
and the nervous tissues end here. The ante
ora serrata,
is the receptor organ. Its anterior edge forms a wavy ring,
body (Fig. 11.25). The posterior three quarters of the retina
choroid, and its inner surface is in contact with the vitreous
Its outer surface is in contact with the
inner nervous layer.
outer pigmented layer
The retina consists of an
Nervous Coat: The Retina
and an
the
-
560
CHAPTER 11
The Head and Neck
venous sinus
conjunctiva
ora serrata
medial check ligament
medial rectus
retinal
arteries
sclera
choroid
retina
optic disc
dura mater
arachnoid mater
subarachnoid space
pia mater
optic nerve
central artery and vein of retina
lateral check ligament
suspensory ligament
medial check ligament
cerebrospinal fluid
short ciliary nerve
long ciliary nerve
fovea centralis
hyaloid canal
vitreous body
orbital fat
fascial
sheath
vitreous
membrane
lateral rectus
lateral check
ligament
suspensory ligament
ciliary muscle
posterior chamber
iris
pupil
anterior chamber
cornea
lens
A
B
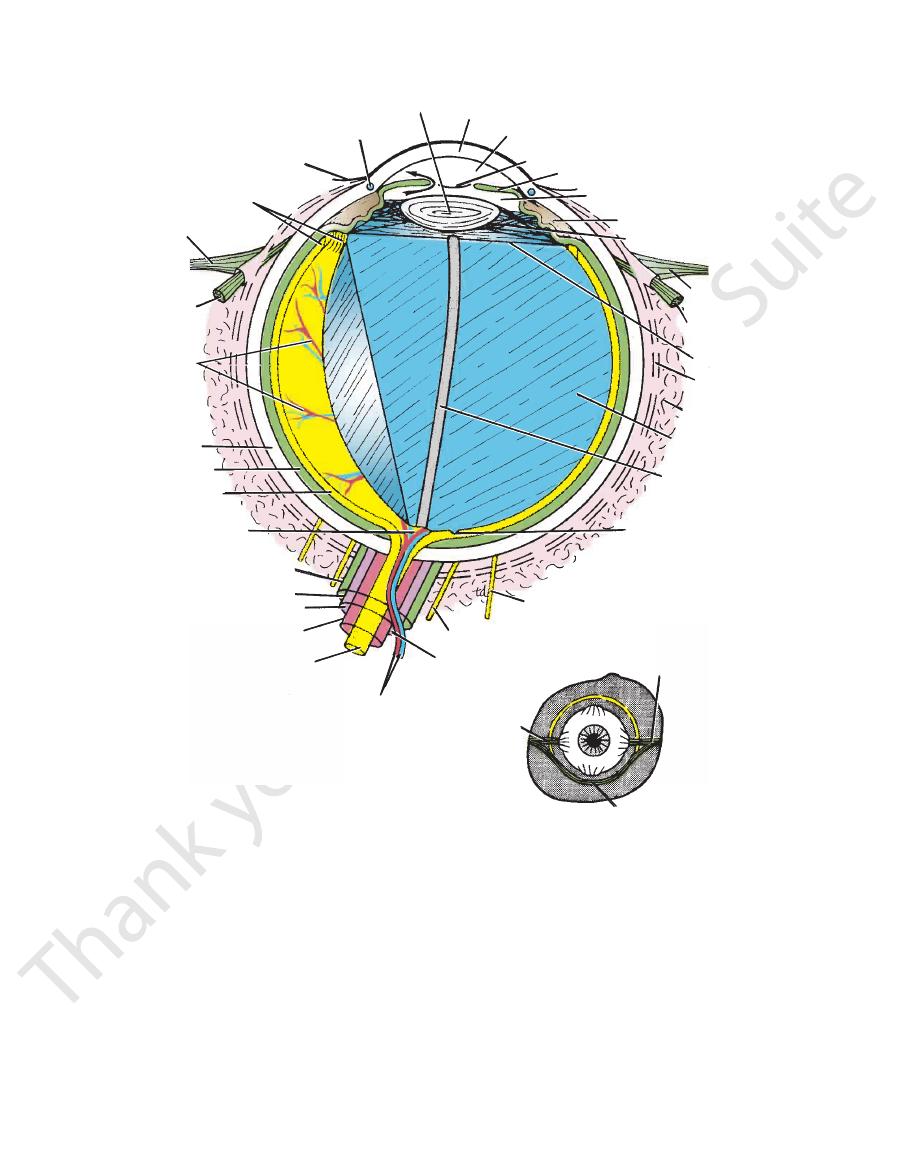
FIGURE 11.25
A.
away through the spaces at the iridocorneal angle into the
the anterior chamber through the pupil and is drained
which it enters the posterior chamber. It then flows into
believed to be a secretion from the ciliary processes, from
and posterior chambers of the eyeball (Fig. 11.25). It is
The aqueous humor is a clear fluid that fills the anterior
Aqueous Humor
the aqueous humor, the vitreous body, and the lens.
The contents of the eyeball consist of the refractive media,
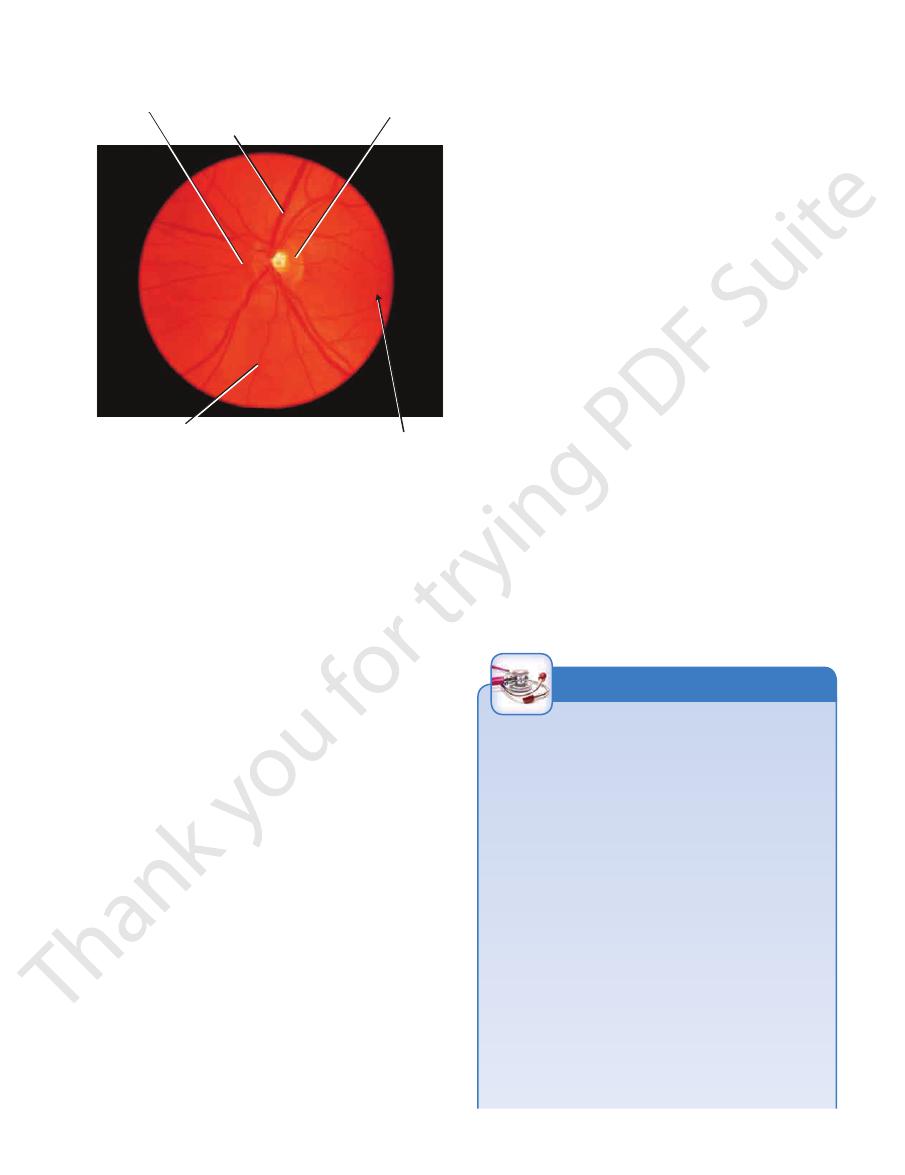
color, much paler than the surrounding retina.
scopic examination, the optic disc is seen to be pale pink in
On ophthalmo
“blind spot.”
light and is referred to as the
so that it is insensitive to
cones
rods
plete absence of
At the optic disc is a com
central artery of the retina.
is slightly depressed at its center, where it is pierced by
optic
medial side of the macula lutea by the optic disc. The
The optic nerve leaves the retina about 3 mm to the
(Figs. 11.25 and 11.26).
fovea centralis
sion, the
retina for the most distinct vision. It has a central depres
which is the area of the
macula lutea,
yellowish area, the
At the center of the posterior part of the retina is an oval,
Check ligaments and suspensory ligament of the eyeball.
cross the subarachnoid space to reach the optic nerve.
Horizontal section through the eyeball and the optic nerve. Note that the central artery and vein of the retina
B.
-
disc
the
-
and
-
Contents of the Eyeball
Basic Anatomy
561
pigmentation of retina
branch of central artery of retina
optic disc
tributary of central vein of retina
site of fovea
centralis
FIGURE 11.26
The left ocular fundus as seen with an oph
rectus muscles.
eyes results from the coordinated contraction of the medial
that a single object, not two, is seen. Convergence of the
from a distance toward an individual, the eyes converge so
of objects (single binocular vision). When an object moves
In humans, the retinae of both eyes focus on only one set
of the Lens
Convergence of the Eyes during Accommodation
muscle contracts so the pupil becomes smaller.
accommodation for near objects, the sphincter pupillae
of the lens so spherical aberration is diminished during
To ensure that the light rays pass through the central part
Constriction of the Pupil during Accommodation
eye in focusing on nearby objects.
use of an additional lens in the form of glasses to assist the
ened (presbyopia). This disability can be overcome by the
elastic, and, as a result, the ability to accommodate is less
With advancing age, the lens becomes denser and less
lar shape.
relaxed. This allows the elastic lens to assume a more globu
so that the radiating fibers of the suspensory ligament are
cle contracts and pulls the ciliary body forward and inward
To accommodate the eye for close objects, the ciliary mus
Accommodation of the Eye
flattened so that the eye can be focused on distant objects.
ers of the suspensory ligament tends to keep the elastic lens
The pull of the radiating fib
suspensory ligament.
by the
lens is attached to the ciliary processes of the ciliary body
disc shape. The equatorial region, or circumference, of the
constantly to endeavor to assume a globular rather than a
The elastic lens capsule is under tension, causing the lens
lens. The lens fibers make up the bulk of the lens.
formed from the cuboidal epithelium at the equator of the
which are
lens fibers,
the anterior surface of the lens; and
which is confined to
cuboidal epithelium,
the structure; a
which envelops
capsule,
The lens consists of an elastic
ciliary processes.
iris and in front of the vitreous body and is encircled by the
enclosed in a transparent capsule. It is situated behind the
The lens (Fig. 11.25) is a transparent, biconvex structure
of the retina against the pigmented part of the retina.
rior surface of the lens and assists in holding the neural part
to the magnifying power of the eye. It supports the poste
The function of the vitreous body is to contribute slightly
is filled by the hyaloid artery, which disappears before birth.
optic disc to the posterior surface of the lens; in the fetus, it
row channel that runs through the vitreous body from the
hyaloid canal
11.25) and is a transparent gel. The
The vitreous body fills the eyeball behind the lens (Fig.
Vitreous Body
lens do not possess a blood supply.
these functions are important because the cornea and the
and the lens and removes the products of metabolism;
maintaining its optical shape. It also nourishes the cornea
wall of the eyeball by exerting internal pressure and thus
The function of the aqueous humor is to support the
the retina, with consequent blindness.
This can produce degenerative changes in
glaucoma.
called
aqueous humor results in a rise in intraocular pressure
Obstruction to the draining of the
canal of Schlemm.
-
thalmoscope.
is a nar-
-
The Lens
-
-
-
-
of the Eye
Eye Trauma
ing loss of sensation of the skin of the cheek and the gum on
such as golf balls, which can cause severe damage to the eye.
globe. The bony orbit provides no protection from small objects,
tennis balls, which tend to strike the orbital margin but not the
orbit, it is protected anteriorly only from large objects, such as
Although the eyeball is well protected by the surrounding bony
Careful examination of the eyeball relative to the orbital mar-
gins shows that it is least protected from the lateral side.
Blowout fractures of the orbital floor involving the maxil-
lary sinus commonly occur as a result of blunt force to the
face. If the force is applied to the eye, the orbital fat explodes
inferiorly into the maxillary sinus, fracturing the orbital floor.
Not only can blowout fractures cause displacement of the
eyeball, with resulting symptoms of double vision (diplopia),
but also the fracture can injure the infraorbital nerve, produc-
that side. Entrapment of the inferior rectus muscle in the frac-
ture may limit upward gaze.
Strabismus
Many cases of strabismus are nonparalytic and are caused
by an imbalance in the action of opposing muscles. This type
C L I N I C A L N O T E S
(continued)