
Basic Anatomy
639
superior, middle, and inferior constrictor muscles. Some of
(Fig. 11.90). The capsule is separated from the supe
capsule
fibrous
The tonsil is covered on its lateral surface by a
tonsillar crypts.
openings that lead into the
into the pharynx. The surface is pitted by numerous small
by mucous membrane, and its free medial surface projects
palatopharyngeal arches (Fig. 11.90). Each tonsil is covered
oral part of the pharynx between the palatoglossal and
each located in the depression on the lateral wall of the
The palatine tonsils are two masses of lymphoid tissue,
Palatine Tonsils
geus muscle) relaxes and the bolus enters the esophagus.
Finally, the lower part of the pharyngeal wall (the cricopharyn
piriform fossae.
into the larynx, that is, down through the
the food slides down the groove on either side of the entrance
-
-
rior constrictor muscle by loose areolar tissue (Fig. 11.90),
the respiratory and digestive systems forms a ring. The
The lymphoid tissue that surrounds the opening into
Waldeyer’s Ring of Lymphoid Tissue
behind the angle of the mandible.
The upper deep cervical lymph nodes, just below and
Lymph Drainage of the Tonsil
tine, the pharyngeal, or the facial veins.
the superior constrictor muscle and join the external pala
The tonsillar branch of the facial artery. The veins pierce
hood, but after puberty it diminishes considerably in size.
The tonsil reaches its maximum size during early child
the loop of the facial artery, and the internal carotid artery.
the superior constrictor muscle lie the styloglossus muscle,
in this tissue to join the pharyngeal venous plexus. Lateral to
and the external palatine vein descends from the soft palate
-
Blood Supply
-
lateral part of the ring is formed by the palatine tonsils
and tubal tonsils (lymphoid tissue around the opening
of the auditory tube in the lateral wall of the nasopharynx).
Posteriorly:
chea and the esophagus (Fig. 11.49).
ascend one on each side, in the groove between the tra
The trachea; the recurrent laryngeal nerves
Anteriorly:
rax is described on page 100.
neck, it inclines to the left side. Its further course in the tho
commences in the midline, but as it descends through the
tilage, opposite the body of the sixth cervical vertebra. It
11.13 and 11.88). It begins at the level of the cricoid car
long, extending from the pharynx to the stomach (Figs.
The esophagus is a muscular tube about 10 in. (25 cm)
of the tongue forms the lower part.
the upper part, and the lingual tonsil on the posterior third
The pharyngeal tonsil in the roof of the nasopharynx forms
The Esophagus
-
-
Relations in the Neck
■
■
-
■
■
The prevertebral layer of deep
ical
cerv
fascia, the longus colli, and the vertebral column
(Fig. 11.49)
is the area of the nasal cavity lying just inside the nostril
nasal vestibule
nose opens into the nasopharynx. The
behind, where the
choanae
or
posterior nasal apertures
The nasal cavity extends from the nostrils in front to the
Nasal Cavity
maxillary nerve (CN V) (see page 608).
thalmic nerve (CN V) and the infraorbital branch of the
The infratrochlear and external nasal branches of the oph
plied by branches from the facial artery.
skin of the ala and the lower part of the septum are sup
ophthalmic and the maxillary arteries (see page 598). The
The skin of the external nose is supplied by branches of the
formed of plates of hyaline cartilage (Fig. 11.92).
the nasal part of the frontal bone. Below, the framework is
the nasal bones, the frontal processes of the maxillae, and
The framework of the external nose is made up above by
rounded and mobile.
(Fig. 11.92). The lateral margin, the
septum
which are separated from each other by the
trils,
The external nose has two elliptical orifices called the
External Nose
halves.
both of which are divided by a septum into right and left
The nose consists of the external nose and the nasal cavity,
and from the sympathetic trunks.
The nerves are derived from the recurrent laryngeal nerves
The lymph vessels drain into the deep cervical lymph nodes.
Lymph Drainage in the Neck
rior thyroid veins.
drain into the infe
veins
the inferior thyroid arteries. The
of the esophagus in the neck are derived from
arteries
The
and the carotid sheath (Fig. 11.49)
On each side lie the lobe of the thyroid gland
Laterally:
■
■
Blood Supply in the Neck
-
Nerve Supply in the Neck
The Respiratory System in the Head
and Neck
The Nose
nos-
nasal
ala nasi, is
Blood Supply of the External Nose
-
Nerve Supply of the External Nose
-
(Fig. 11.93). The nasal cavity is divided into right and left
and a medial or septal wall.
Each half of the nasal cavity has a floor, a roof, a lateral wall,
Walls of the Nasal Cavity
vomer.
ethmoid,
vertical plate of the
septal cartilage,
made up of the
(Fig. 11.92). The septum is
nasal septum
halves by the
the
and the
640
CHAPTER 11
The Head and Neck
frontal bone
frontal bone
A
C
B
nasal bone
nasal
bone
nasal bone frontal process
of maxilla
maxilla
incisive canal
vomer
sphenoid sinus
horizontal plate
of palatine
palatine process of maxilla
vertical plate
of ethmoid bone
frontal
sinus
upper lateral
nasal cartilage
upper lateral
nasal cartilage
septal cartilage
septal
cartilage
lesser alar cartilages
nostril
lower lateral
nasal cartilage
lower lateral
nasal cartilage
accessory cartilage
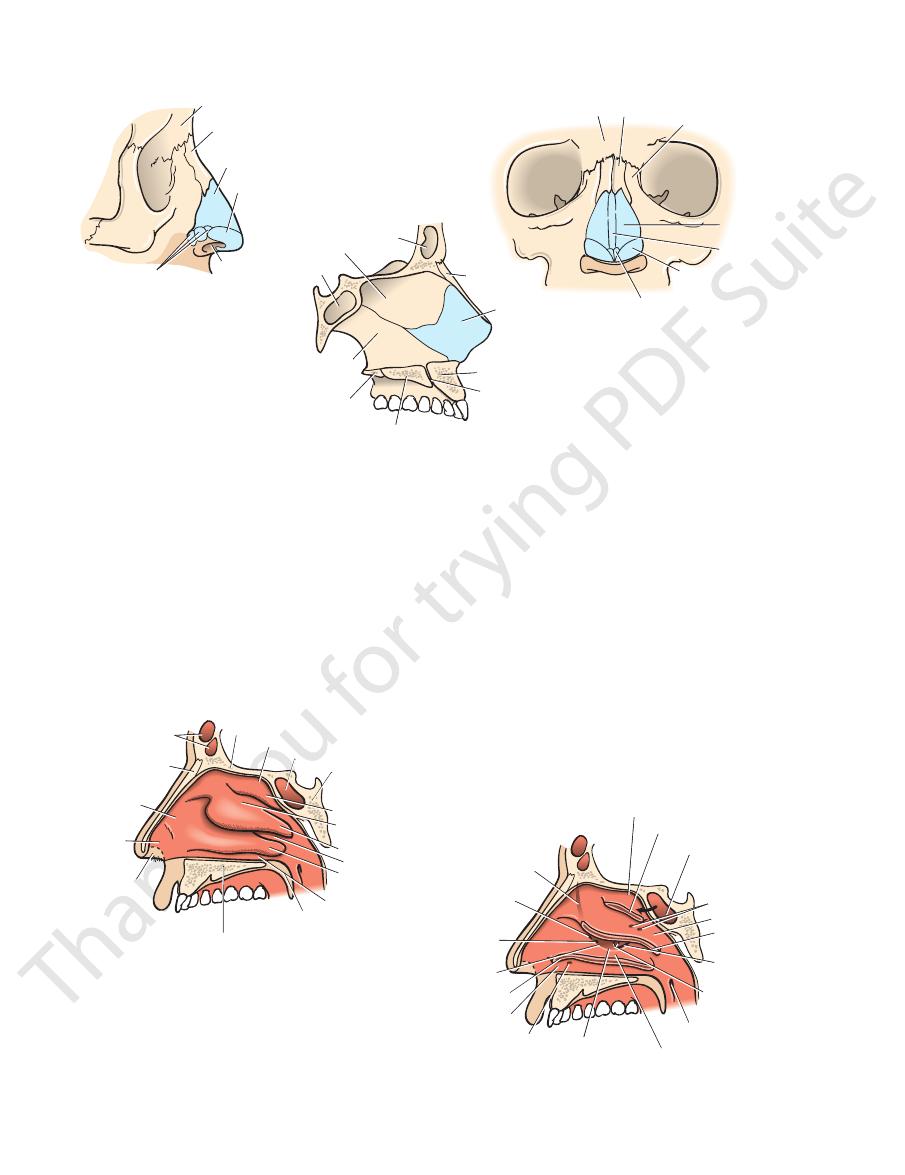
FIGURE 11.92
External nose and nasal septum.
Bony and cartilaginous skeleton of nasal septum.
rior view of bony and cartilaginous skeleton of external nose.
Lateral view of bony and cartilaginous skeleton of external nose.
A.
B. Ante-
C.
frontal
sinus
A
B
cribriform plate of ethmoid
sphenoethmoidal recess
sphenoethmoidal recess
sphenoidal sinus
sphenoidal air sinus
openings of
posterior
ethmoidal
sinuses
openings of middle
ethmoidal sinuses
openings of auditory
tube
openings of
maxillary sinus
body of sphenoid bone
superior nasal concha
superior nasal concha
middle nasal concha
middle nasal
concha
inferior nasa
concha
inferior nasal concha
inferior meatus
inferior meatus
opening of
nasolacrimal duct
soft palate
hard palate formed by
palatine process of maxilla and
horizontal plate of palatine bone
middle meatus
middle meatus
hiatus semilunaris
superior meatus
superior meatus
nasal bone
atrium of
middle
meatus
vestibule
nostril
bony channel by
which frontal
sinus opens into
infundibulum
opening of frontal
sinus into
infundibulum
opening of anterior
ethmoidal sinuses
bulla ethmoidalis
FIGURE 11.93
A.
posterior ethmoid sinuses.
superior concha (Fig. 11.93). It receives the openings of the
The superior meatus lies below the
Superior Meatus
(Fig. 11.93).
sphenoid air sinus
opening of the
is a small area above the superior concha. It receives the
The sphenoethmoidal recess
Sphenoethmoidal Recess
meatus.
The space below each concha is called a
(Fig. 11.93).
inferior nasal conchae
superior, middle,
The lateral wall has three projections of bone called the
Lateral Wall
downward sloping body of the sphenoid (Fig. 11.93).
beneath the anterior cranial fossa, and posteriorly by the
middle by the cribriform plate of the ethmoid, located
bridge of the nose by the nasal and frontal bones, in the
The roof is narrow and is formed anteriorly beneath the
Roof
of the palatine bone (Fig. 11.92)
The palatine process of the maxilla and the horizontal plate
conchae have been partially removed to show openings of the paranasal sinuses and the nasolacrimal duct into the meati.
Lateral wall of the right nasal cavity; the superior, middle, and inferior
Lateral wall of the right nasal cavity. B.
Floor
and

Basic Anatomy
The paranasal sinuses are cavities found in the interior of the
by vessels that pass to the upper deep cervical nodes.
dibular nodes. The remainder of the nasal cavity is drained
The lymph vessels draining the vestibule end in the subman
Lymph Drainage of the Nasal Cavity
accompany the arteries.
bule. The submucous venous plexus is drained by veins that
labial branch of the facial artery in the region of the vesti
artery anastomoses with the septal branch of the superior
sphenopalatine artery (Fig. 11.95). The sphenopalatine
external carotid artery. The most important branch is the
the maxillary artery, one of the terminal branches of the
The arterial supply to the nasal cavity is from branches of
Blood Supply to the Nasal Cavity
(Fig. 11.94).
and the maxillary division (V2) of the trigeminal nerve
sensation are branches of the ophthalmic division (V1)
to the olfactory bulbs (Fig. 11.94). The nerves of ordinary
ascend through the cribriform plate of the ethmoid bone
The olfactory nerves from the olfactory mucous membrane
Nerve Supply of the Nasal Cavity
which are then swallowed and destroyed by gastric acid.
traps foreign particles and organisms in the inspired air,
tem. The presence of mucus on the surfaces of the conchae
to heat up the inspired air as it enters the respiratory sys
The presence of warm blood in the venous plexuses serves
Function of Warm Blood and Mucus of Mucous
present in the respiratory region.
large plexus of veins in the submucous connective tissue is
nasal cavity is lined with respiratory mucous membrane. A
sensitive to the reception of smell. The lower part of the
olfactory mucous membrane and contains nerve endings
hairs. The area above the superior concha is lined with
The vestibule is lined with modified skin and has coarse
Mucous Membrane of the Nasal Cavity
decreasing the size of the other.
thus increasing the size of one half of the nasal cavity and
the septal cartilage. The septum rarely lies in the midline,
the vomer (Fig. 11.92). The anterior part is formed by
part is formed by the vertical plate of the ethmoid and
The medial wall is formed by the nasal septum. The upper
Medial Wall
membrane (Fig. 11.93).
which is guarded by a fold of mucous
nasolacrimal duct,
rior concha and receives the opening of the lower end of the
The inferior meatus lies below the infe
Inferior Meatus
hiatus semilunaris.
meatus through the
opens into the middle
maxillary sinus
The
frontal sinus.
which is continuous with the
infundibulum,
nel called the
anterior end of the hiatus leads into a funnel-shaped chan
lies just below the bulla (Fig. 11.93). The
tus semilunaris,
which open on its upper border. A curved opening, the
middle ethmoidal air sinuses,
that is formed by the
bulla ethmoi
concha. It has a rounded swelling called the
The middle meatus lies below the middle
Middle Meatus
641
-
dalis
hia-
-
-
Membrane
-
-
-
The Paranasal Sinuses
maxilla, frontal, sphenoid, and ethmoid bones (Fig. 11.97).
the voice is markedly changed.
are blocked or they become filled with fluid, the quality of
the weight of the skull. When the apertures of the sinuses
sinuses is to act as resonators to the voice; they also reduce
ated during the blowing of the nose. The function of the
age of the mucus is also achieved by the siphon action cre
into the nose by ciliary action of the columnar cells. Drain
The mucus produced by the mucous membrane is moved
Drainage of Mucus and Function of Paranasal
adolescence.
ciably after the eighth year and become fully formed in
present in a rudimentary form at birth; they enlarge appre
small apertures. The maxillary and sphenoidal sinuses are
they communicate with the nasal cavity through relatively
They are lined with mucoperiosteum and filled with air;
-
Sinuses
-
-
A
B
olfactory
nerves
olfactory
nerves
medial posterior
superior nasal
nerves (V2)
nasopalatine
nerve (V2)
olfactory bulb
olfactory
bulb
olfactory tract
lateral posterior
superior nasal
nerves (V2)
lateral posterior
inferior nasal
nerves (V2)
lesser palatine
nerve (V2)
greater palatine nerve (V2)
pharyngeal
nerve (V2)
anterior
ethmoidal
nerve (V1)
internal nasal
nerve from
anterior
ethmoidal
nerve (V1)
external nasal
nerve (V1)
internal
nasal
nerve
(V1)
FIGURE 11.94
A.
sensory innervation of mucous membrane.
Nasal septum showing
Lateral wall of nasal cavity showing sensory innervation of mucous membrane. B.
642
CHAPTER 11
The Head and Neck
A
B
anterior ethmoidal
artery (ophthalmic)
anterior ethmoidal
artery (ophthalmic)
Kiesselbach’s
area
septal branch
from facial
artery
posterior ethmoidal
artery (ophthalmic)
sphenopalatine
artery
(maxillary)
septal branches of
sphenopalatine artery
(maxillary)
lesser palatine
artery (maxillary)
lesser palatine
artery (maxillary)
greater palatine
artery (maxillary)
greater palatine
artery (maxillary)
branches
from
facial
artery
posterior ethmoidal
artery (ophthalmic)
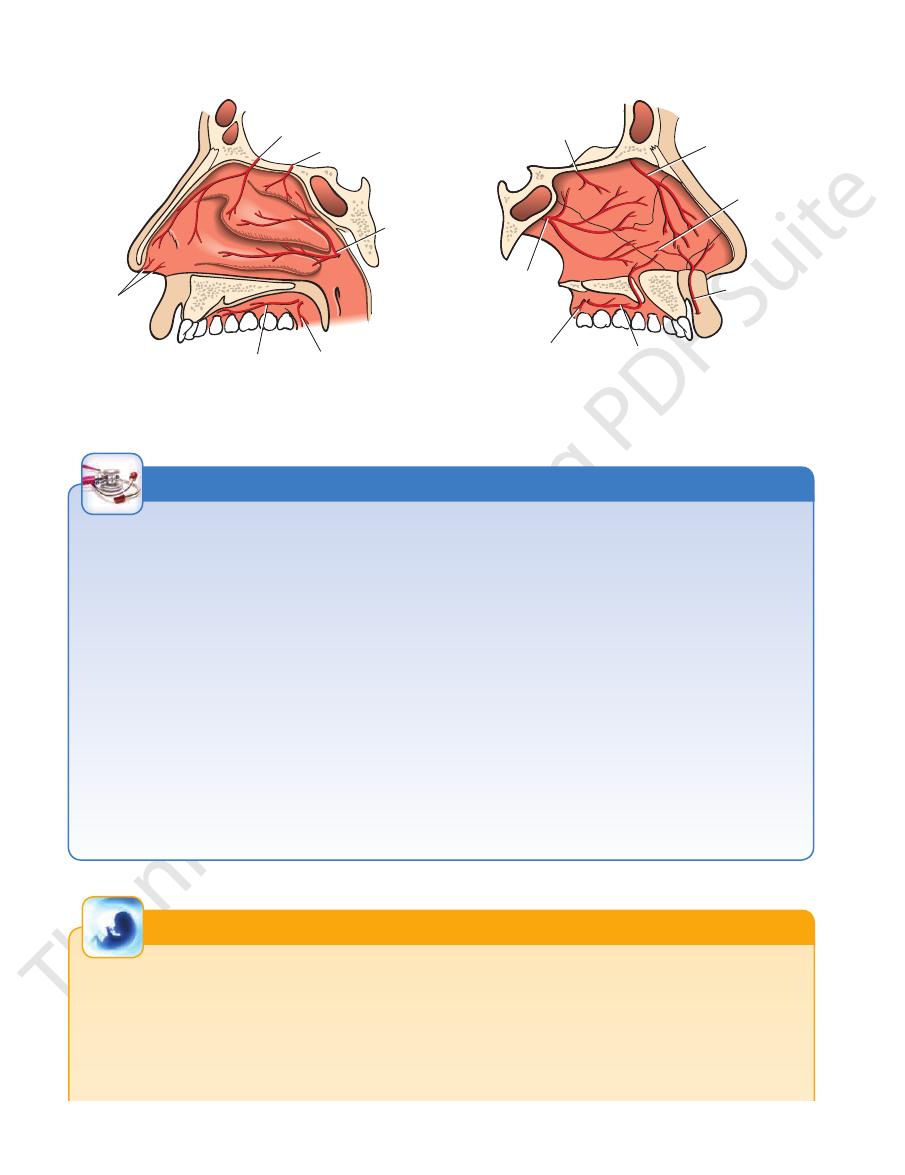
FIGURE 11.95
A.
Nasal septum showing
Lateral wall of nasal cavity showing the arterial supply of the mucous membrane. B.
the arterial supply of the mucous membrane.
Examination of the Nasal Cavity
The most common cause is nose picking. The bleeding may be
like conchae make impaction and retention of balloons, peas,
placed downward and inward. Lateral fractures also occur in
Examination of the nasal cavity may be carried out by inserting
a speculum through the external nares or by means of a mirror
in the pharynx. In the latter case, the choanae and the posterior
border of the septum can be visualized (Fig. 11.91).
It should be remembered that the nasal septum is rarely situ-
ated in the midline. A severely deviated septum may interfere
with drainage of the nose and the paranasal sinuses.
Trauma to the Nose
Fractures involving the nasal bones are common. Blows directed
from the front may cause one or both nasal bones to be dis-
which one nasal bone is driven inward and the other outward;
the nasal septum is usually involved.
Infection of the Nasal Cavity
Infection of the nasal cavity can spread in a variety of direc-
tions. The paranasal sinuses are especially prone to infection.
Organisms may spread via the nasal part of the pharynx and the
auditory tube to the middle ear. It is possible for organisms to
ascend to the meninges of the anterior cranial fossa, along the
sheaths of the olfactory nerves through the cribriform plate, and
produce meningitis.
Foreign Bodies in the Nose
Foreign bodies in the nose are common in children. The pres-
ence of the nasal septum and the existence of the folded, shelf-
and small toys relatively easy.
Nose Bleeding
Epistaxis, or bleeding from the nose, is a frequent condition.
arterial or venous, and most episodes occur on the anteroinfe-
rior portion of the septum and involve the septal branches of the
sphenopalatine and facial vessels.
C L I N I C A L N O T E S
Development of the Nose
process on each side. At this stage, the floors of the olfactory
the medial nasal process and the anterior part of the maxillary
lary process. As these processes fuse, the olfactory pits become
The roof of the nose is formed from the lateral nasal processes,
from which the lateral walls also are formed, with the assistance
of the maxillary processes (Fig. 11.43). The anterior openings of
the nose begin as olfactory pits in the frontonasal process. Each
olfactory pit is bounded medially by the medial nasal process,
laterally by the lateral nasal process, and inferiorly by the maxil-
deeper and form well-defined blind sacs, the opening into each
of which is the nostril.
The floor of the nose at first is very short and consists of
pits rupture so that the nasal cavities communicate with the
E M B R Y O L O G I C N O T E S
(continued)
Basic Anatomy
643
developing mouth (Fig. 11.82). Meanwhile, the nasal septum is
tened structure and gains its recognizable form only after the
11.82). Later, the palatal processes of the maxilla grow medially
forming as a downgrowth from the medial nasal process (Fig.
and fuse with each other and with the nasal septum, thus com-
pleting the floor of the nose. Each nasal cavity therefore com-
municates anteriorly with the exterior through the nostril and
posteriorly through the choana with the nasopharynx.
In the early stages of development, the nose is a much-flat-
facial development is complete.
Median Nasal Furrow
In median nasal furrow, the nasal septum is split, separating the
two halves of the nose (Fig. 11.96A).
Lateral Proboscis
In lateral proboscis, a skin-covered process develops, usually
with a dimple at its lower end (Fig. 11.96B).
A
B
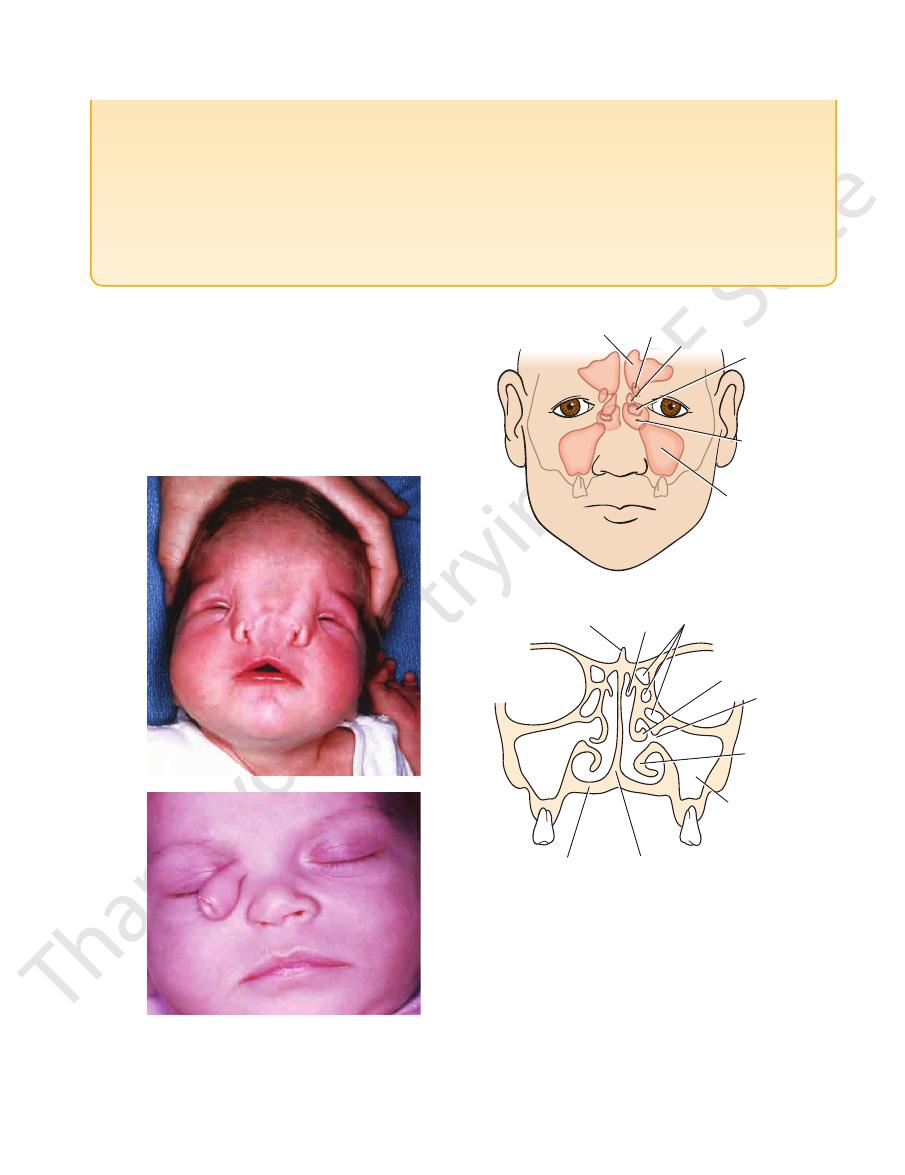
FIGURE 11.96
A.
nose through the infundibulum (Fig. 11.93).
Each frontal sinus opens into the middle meatus of the
into the medial part of the roof of the orbit.
upward above the medial end of the eyebrow and backward
a bony septum. Each sinus is roughly triangular, extending
bone (Fig. 11.97). They are separated from each other by
The two frontal sinuses are contained within the frontal
Frontal Sinuses
the nose through the hiatus semilunaris (Fig. 11.97).
teeth. The maxillary sinus opens into the middle meatus of
the floor is related to the roots of the premolars and molar
(Fig. 11.97). The roof is formed by the floor of the orbit, and
within the body of the maxilla behind the skin of the cheek
The maxillary sinus is pyramidal in shape and located
wide furrow. (Courtesy of L. Thompson.)
the nose. Note that the external nares are separated by a
septum has completely split, separating the two halves of
Median nasal furrow in which the nasal
B. Lateral probos-
cis. (Courtesy of R. Chase.)
Maxillary Sinus
frontal sinus
anterior ethmoidal sinuses
A
B
ethmoidal sinuses
orbit
middle ethmoidal sinuses
posterior
ethmoidal
sinuses
sphenoid
sinuses
maxillary
sinuses
crista galli
superior
concha
inferior
concha
maxillary
sinus
nasal septum
hard palate
middle concha
hiatus
semilunaris
FIGURE 11.97
A.
cavity showing the ethmoidal and the maxillary sinuses.
relation to the face.
The position of the paranasal sinuses in
B. Coronal section through the nasal
644
CHAPTER 11
summarized in Table 11.11.
The various sinuses and their openings into the nose are
the posterior sinuses open into the superior meatus.
the middle meatus, on or above the bulla ethmoidalis; and
open into the infundibulum; the middle sinuses open into
spread from the sinuses into the orbit. The anterior sinuses
the latter by a thin plate of bone so that infection can readily
the nose and the orbit (Fig. 11.97). They are separated from
and they are contained within the ethmoid bone, between
The ethmoidal sinuses are anterior, middle, and posterior
noethmoidal recess above the superior concha.
noid bone (Fig. 11.97). Each sinus opens into the sphe
The two sphenoidal sinuses lie within the body of the sphe
The Head and Neck
Sphenoidal Sinuses
-
-
Ethmoid Sinuses
Paranasal Sinuses and Their
Site of Drainage into the Nose
*
T A B L E 1 1 . 1 1
Sinusitis and the Examination of the Paranasal
by pressing the finger upward beneath the medial end of the
Sinuses
Infection of the paranasal sinuses is a common complica-
tion of nasal infections. Rarely, the cause of maxillary sinus-
itis is extension from an apical dental abscess. The frontal,
ethmoidal, and maxillary sinuses can be palpated clinically
for areas of tenderness. The frontal sinus can be examined
superior orbital margin. Here, the floor of the frontal sinus is
closest to the surface.
The ethmoidal sinuses can be palpated by pressing the
finger medially against the medial wall of the orbit. The maxil-
lary sinus can be examined for tenderness by pressing the fin-
ger against the anterior wall of the maxilla below the inferior
orbital margin; pressure over the infraorbital nerve may reveal
increased sensitivity.
C L I N I C A L N O T E S
(continued)
Directing the beam of a flashlight either through the roof of
Crossing of Air and Food Pathways in the
because its drainage orifice through the hiatus semilunaris is
the mouth or through the cheek in a darkened room will often
enable a physician to determine whether the maxillary sinus is
full of inflammatory fluid rather than air. This method of transil-
lumination is simple and effective. Radiologic examination of
the sinuses is also most helpful in making a diagnosis. One
should always compare the clinical findings of each sinus on
the two sides of the body.
The frontal sinus is innervated by the supraorbital nerve,
which also supplies the skin of the forehead and scalp as far
back as the vertex. It is, therefore, not surprising that patients
with frontal sinusitis have pain referred over this area. The
maxillary sinus is innervated by the infraorbital nerve and, in
this case, pain is referred to the upper jaw, including the teeth.
The frontal sinus drains into the hiatus semilunaris, via the
infundibulum, close to the orifice of the maxillary sinus on the
lateral wall of the nose. It is thus not unexpected to find that
a patient with frontal sinusitis nearly always has a maxillary
sinusitis. The maxillary sinus is particularly prone to infection
badly placed near the roof of the sinus. In other words, the
sinus has to fill up with fluid before it can effectively drain with
the person in the upright position. The relation of the apices of
the roots of the teeth in the maxilla to the floor of the maxillary
sinus was already emphasized.
Pharynx
muscles, and lined by mucous membrane.
are held together by ligaments and membranes, moved by
The framework of the larynx is formed of cartilages that
and at the sides by the thyroid gland.
larynx is covered in front by the infrahyoid strap muscles
pharynx, and below is continuous with the trachea. The
(Fig. 11.87). It opens above into the laryngeal part of the
at the level of the fourth, fifth, and sixth cervical vertebrae
and between the great blood vessels of the neck and lies
production. It is situated below the tongue and hyoid bone
at the inlet of the air passages and is responsible for voice
The larynx is an organ that provides a protective sphincter
use of wind instruments such as the trumpet.
maximum expiration of air through the mouth as in the
the respiratory system through the mouth. It also allows the
an arrangement permits the expectoration of mucus from
the mouth rather than the narrow cavities of the nose. Such
of the larynx, the soft palate is raised to direct air through
desirable to direct the maximum amount of air in and out
the nasopharynx in swallowing (see page XXX). When it is
ynx from the oropharynx, thus preventing food entering
The completely raised soft palate can shut off the nasophar
chewing food so that breathing may continue unaffected.
from the oropharynx, for example, during the process of
which serves as a flap valve. This flap shuts off the mouth
This is made possible by the presence of the soft palate,
It is in the pharynx that the air and food pathways cross.
-
The Larynx
Sinus
Site of Drainage
Maxillary sinus
Middle meatus through hiatus semi-
lunaris
Frontal sinuses
Middle meatus via infundibulum
Sphenoidal sinuses
Sphenoethmoidal recess
Ethmoidal sinuses
Anterior group
Infundibulum and into middle meatus
Middle group
Middle meatus on or above bulla
ethmoidalis
Posterior group
birth, enlarge appreciably after the eighth year, and are fully formed in adolescence.
*Note that maxillary and sphenoidal sinuses are present in rudimentary form at
Superior meatus
Basic Anatomy
lation with the inferior cornu of the thyroid cartilage.
on each side of the lateral surface is a facet for articu
cricoid cartilage lies below the thyroid cartilage, and
behind and a shallow arch in front (Fig. 11.98). The
lage and shaped like a signet ring, having a broad plate
This cartilage is formed of hyaline carti
Cricoid cartilage:
lamina is an oblique line for the attachment of muscles.
On the outer surface of each
inferior cornu.
into an
and downward
superior cornu
extends upward into a
angle (the so-called Adam’s apple). The posterior border
cartilage that meet in the midline in the prominent V
ynx (Fig. 11.98) and consists of two laminae of hyaline
This is the largest cartilage of the lar
Thyroid cartilage:
Cartilages of the Larynx
645
-
-
-
Posteriorly, the lamina has on its upper border on each
ytenoid muscles.
ally gives attachment to the posterior and lateral cricoar
that projects later
muscular process
vocal ligament. A
that projects forward and gives attachment to the
cess
vocal pro
with the lamina of the cricoid cartilage, and a
below that articulates
small corniculate cartilage, a
above that articulates with the
apex
cartilage has an
upper border of the lamina of the cricoid cartilage. Each
back of the larynx (Fig. 11.98). They articulate with the
which are small and pyramid shaped and located at the
There are two arytenoid cartilages,
Arytenoid cartilages:
All these joints are synovial.
side a facet for articulation with the arytenoid cartilage.
base
-
-
-
arch of cricoid cartilage
epiglottis
hyoid bone
lateral thyrohyoid
ligament
superior cornu
lamina of thyroid
cartilage
inferior cornu
arch of cricoid
cartilage
cricotracheal ligament
trachea
cricothyroid ligament
oblique line
thyrohyoid membrane
thyrohyoid ligament
lateral thyrohyoid ligament
epiglottis
hyoid bone
thyrohyoid membrane
thyrohyoid ligament
cricothyroid ligament
cricothyroid muscle
lamina of cricoid cartilage
epiglottis
greater cornu of hyoid
bone
thyrohyoid membrane
corniculate
cartilage
arytenoid
cartilage
lamina of thyroid
cartilage
muscular process
trachealis muscle
hyoepiglottic ligament
epiglottis
greater cornu of
hyoid bone
superior cornu of
thyroid cartilage
aryepiglottic fold
cuneiform cartilage
corniculate cartilage
arytenoid cartilage
muscular process
vocal process
lamina of cricoid
cartilage
body of hyoid bone
thyrohyoid membrane
thyroid cartilage
right vestibular fold
right vocal ligament
cricothyroid ligament
arch of cricoid
cartilage
A
B
C
D
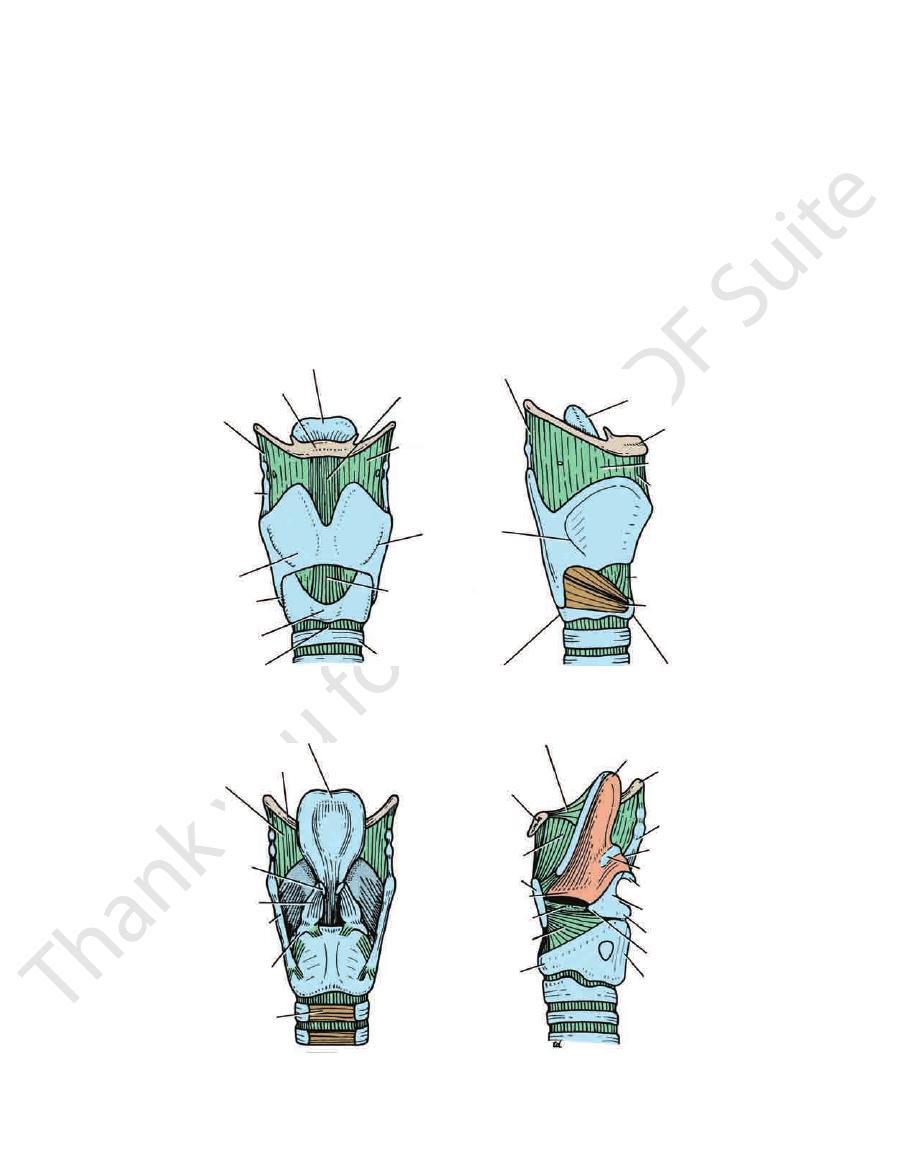
FIGURE 11.98
The larynx and its ligaments from the front
lamina of thyroid cartilage has been removed to display the interior of the larynx.
The left
(A), from the lateral aspect (B), and from behind (C). D.

646
CHAPTER 11
The Head and Neck
greater cornu of hyoid bone
epiglottis
tubercle
of epiglottis
aryepiglottic
muscle
aryepiglottic
muscle
oblique
arytenoid
muscle
transverse
arytenoid
muscle
posterior
cricoarytenoid
muscle
trachea
lamina of cricoid cartilage
thyroid cartilage
arytenoid cartilage
corniculate cartilage
cuneiform cartilage
thyrohyoid membrane
epiglottis
aryepiglottic fold
piriform fossa
quadrangular membrane
saccule
thyroid cartilage
vestibular fold
vestibular ligament
sinus
vocal fold
vocalis
vocal ligament
cricothyroid ligament
cricoid cartilage
rima glottidis
first ring of trachea
vocal fold
vestibular fold
rima glottidis
cuneiform cartilage
corniculate cartilage
thyroid cartilage
rima glottidis
vocal ligament
arytenoid cartilage
thyroid cartilage
rima glottidis
vocal process
arytenoid cartilage
muscular process
vocal ligament
vocalis
lateral cricoarytenoid muscle
posterior cricoarytenoid muscle
transverse arytenoid muscle
oblique arytenoid muscle
A
B
C
D
E
FIGURE 11.99
A.
Corniculate cartilages:
Muscles that move vocal ligaments.
Rima glottidis wide open as in deep breathing.
open as in quiet breathing.
Rima glottidis partially
Coronal section through the larynx.
Muscles of the larynx seen from behind. B.
C.
D.
E.
Two small conical-shaped cartilages
(Fig. 11.90). Laterally, the mucous
vallecula
called the
the depression on each side of the fold is
glottic fold;
median glossoepi
terior surface of the tongue as the
of mucous membrane passes forward onto the pos
The upper edge of the epiglottis is free. The covering
lages by the aryepiglottic folds of mucous membrane.
of the epiglottis are attached to the arytenoid carti
attached to the back of the thyroid cartilage. The sides
behind the root of the tongue (Fig. 11.98). Its stalk is
This leaf-shaped lamina of elastic cartilage lies
Epiglottis:
strengthen them (Fig. 11.99).
lages are found in the aryepiglottic folds and serve to
These two small rod-shaped carti
Cuneiform cartilages:
give attachment to the aryepiglottic folds.
articulate with the arytenoid cartilages (Fig. 11.99). They
-
-
-
-
membrane passes onto the wall of the pharynx as the
lateral glossoepiglottic fold.
epiglottis and the arytenoid cartilages (Fig. 11.99).
This extends between the
Quadrangular membrane:
to the first ring of the trachea (Fig. 11.98).
This connects the cricoid cartilage
Cricotracheal ligament:
a branch of the superior laryngeal nerve (Fig. 11.80).
superior laryngeal vessels and the internal laryngeal nerve,
The membrane is pierced on each side by the
ligament.
median thyrohyoid
midline, it is thickened to form the
the thyroid cartilage to the hyoid bone (Fig. 11.98). In the
This connects the upper margin of
Thyrohyoid membrane:
Membranes and Ligaments of the Larynx
Basic Anatomy
lowing. Note that many of these muscles are attached to
These muscles move the larynx up and down during swal
extrinsic and intrinsic.
The muscles of the larynx may be divided into two groups:
mucous secretion lubricates the vocal cords.
membrane that ascends from the sinus (Fig. 11.99). The
The saccule of the larynx is a diverticulum of mucous
Saccule of the Larynx
lined with mucous membrane (Fig. 11.99).
larynx situated between the vestibular and vocal folds. It is
The sinus of the larynx is a small recess on each side of the
above and the lower border of the cricoid cartilage below
which is situated between the vocal folds
lower region,
The
lar folds above and the vocal folds below
which is situated between the vestibu
middle region,
The
vestibular folds
which is situated between the inlet and the
vestibule,
The
the cavity of the trachea. It is divided into three regions:
border of the cricoid cartilage, where it is continuous with
The cavity of the larynx extends from the inlet to the lower
Cavity of the Larynx
the larynx within the cricoid cartilage is the narrowest part.
adult and less in the female. In children, the lower part of
and measures about 2.5 cm from front to back in the male
noid cartilages. The glottis is the narrowest part of the larynx
the vocal folds and behind by the medial surface of the aryte
(Fig. 11.99). The glottis is bounded in front by
glottis
or
rima glotti
The gap between the vocal folds is called the
(Fig. 11.99).
with a laryngoscope
respiration and its white color is easily seen when viewed
The vocal fold moves with
in color.
white
avascular and
by mucous membrane covering the vocal ligament and is
ynx and is concerned with voice production. It is formed
fold on each side of the lar
mobile
The vocal fold is a
Vocal Fold (Vocal Cord)
in color.
the vestibular ligament and is vascular and
(Fig. 11.98). It is formed by mucous membrane covering
fold on each side of the larynx
fixed
The vestibular fold is a
Vestibular Fold
Laryngeal Folds
hyoid membrane.
tic fold and laterally by the thyroid cartilage and the thyro
inlet (Fig. 11.99). It is bounded medially by the aryepiglot
The piriform fossa is a recess on either side of the fold and
The Piriform Fossa
a small elevation on the upper border.
within and strengthens the aryepiglottic fold and produces
with the corniculate cartilages. The cuneiform cartilage lies
membrane, and posteriorly by the arytenoid cartilages
the epiglottis, laterally by the aryepiglottic fold of mucous
is wider in front than behind and is bounded in front by
the laryngeal part of the pharynx (Fig. 11.88). The opening
The inlet of the larynx looks backward and upward into
arytenoid cartilage.
posterior end is attached to the vocal process of the
ligament is attached to the thyroid cartilage, and the
(Fig. 11.99). The anterior end of each vocal
cords)
vocal folds (vocal
ligaments form the interior of the
on each side. The vocal
vocal ligament
important
composed almost entirely of elastic tissue, forms the
surface of the thyroid cartilage. Its upper free margin,
attached to the thyroid cartilage, ascends on the medial
The superior margin of the ligament, instead of being
the upper border of the cricoid cartilage (Fig. 11.99).
The lower margin is attached to
Cricothyroid ligament:
(Fig. 11.99).
vestibular folds
and the vestibular ligaments form the interior of
ment,
vestibular liga
Its thickened inferior margin forms the
647
-
the
Inlet of the Larynx
-
-
pink
-
-
dis
-
-
Sinus of the Larynx
Muscles of the Larynx
Extrinsic Muscles
-
the hyoid bone, which is attached to the thyroid cartilage by
cartilages apart so that the posterior part of the glottis is open.
the capsules of the cricoarytenoid joints keeps the arytenoid
and abducts the vocal process (Fig. 11.99). The elastic tissue in
terior cricoarytenoid, which rotates the arytenoid cartilage
The rima glottidis is opened by the contraction of the pos
of the cricoid cartilage.
and down on the sloping shoulder of the superior border
ments of the arytenoid cartilages, which rotate and slide up
The movements of the vocal folds depend on the move
Movements of the Vocal Folds (Cords)
Table 11.12.
action of the intrinsic muscles of the larynx are given in
The details of the origins, insertions, nerve supply, and
arytenoid muscle
The transverse
Approximates the arytenoid cartilages:
enoid muscle
The posterior cricoaryt
Abducting the vocal cords:
muscle
The lateral cricoarytenoid
Adducting the vocal cords:
muscle
The thyroarytenoid (vocalis)
Relaxing the vocal cords:
The cricothyroid muscle
Tensing the vocal cords:
Five muscles move the vocal folds (cords) (Fig. 11.99):
The thyroepiglottic muscle
Widening the inlet:
The oblique arytenoid muscle
Narrowing the inlet:
Two muscles modify the laryngeal inlet (Fig. 11.99):
omohyoid muscles
The sternothyroid, the sternohyoid, and the
Depression:
geus, and the palatopharyngeus muscles
geniohyoid, the stylopharyngeus, the salpingopharyn
The digastric, the stylohyoid, the mylohyoid, the
Elevation:
hyoid bone are accompanied by movements of the larynx.
the thyrohyoid membrane. It follows that movements of the
-
Intrinsic Muscles
■
■
■
■
■
■
■
■
■
■
■
■
-
■
■
-
-
648
CHAPTER 11
The Head and Neck
Intrinsic Muscles of the Larynx
T A B L E 1 1 . 1 2
Muscle
Origin
Insertion
Nerve Supply
Action
Muscles Controlling the Laryngeal Inlet
Oblique arytenoid
Muscular process of
arytenoid cartilage
Voice Production in the Larynx
producing a grunting sound.
some of the air by momentarily opening the rima glottidis,
tract. After a prolonged effort, the person often releases
by the presence of compressed air within the respiratory
and the upward movement of the diaphragm is prevented
The muscles of the anterior abdominal wall now contract,
glottidis. After deep inspiration, the rima glottidis is closed.
held temporarily in the respiratory tract by closing the rima
with micturition, defecation, and parturition, air is often
against a closed glottis. In abdominal straining associated
In the Valsalva maneuver, forced expiration takes place
where the material is either swallowed or expectorated.
respiratory tract and carry the material up into the pharynx,
air will often dislodge foreign particles or mucus from the
suddenly abducted. The sudden release of the compressed
result, the intrathoracic pressure rises, and the vocal folds are
the muscles of expiration are made to contract strongly. As a
sphincter. After inspiration, the vocal folds are adducted, and
In coughing or sneezing, the rima glottidis serves as a
the laryngeal inlet, the piriform fossae.
the epiglottis or moving down the grooves on either side of
food, or fluids, then enters the esophagus by passing over
and serves as a cap over the laryngeal inlet. The bolus of
muscles. The epiglottis is pulled backward by the tongue
by the action of the oblique arytenoid and aryepiglottic
the back of the tongue. The inlet of the larynx is narrowed
tongue and the hard palate, the larynx is pulled up beneath
ing. As the bolus of food is passed backward between the
The sphincter at the inlet is used only during swallow
rima glottidis.
sphincters in the larynx: one at the inlet and another at the
There are two
Sphincteric Function of the Larynx
the arytenoid cartilages (Fig. 11.99).
diamond shape because of the maximal lateral rotation of
abducted and the triangular shape of the glottis becomes a
On deep inspiration, the vocal folds are maximally
a small gap between them (Fig. 11.99).
11.99). On expiration, the vocal folds are adducted, leaving
glottidis is triangular in shape with the apex in front (Fig.
inspiration, the vocal folds are abducted and the rima
On quiet
Movements of the Vocal Folds with Respiration
muscle (Fig. 11.99).
by contraction of the vocalis, a part of the thyroarytenoid
thyroid muscle (Fig. 11.100). The vocal folds are slackened
The vocal folds are stretched by contraction of the crico
by contraction of the transverse arytenoid muscles.
is narrowed when the arytenoid cartilages are drawn together
the vocal process (Fig. 11.99). The posterior part of the glottis
coarytenoid, which rotates the arytenoid cartilage and adducts
The rima glottidis is closed by contraction of the lateral cri
Transverse
Tenses vocal cords
Muscles Controlling the Movements of the Vocal Folds (Cords)
Apex of opposite
arytenoid cartilage
Recurrent
laryngeal nerve
Narrows the inlet by bring-
ing the aryepiglottic folds
together
Thyroepiglottic
Medial surface of thyroid
cartilage
Lateral margin of
epiglottis and arye-
piglottic fold
Recurrent
laryngeal nerve
Widens the inlet by pulling the
aryepiglottic folds apart
Cricothyroid
Side of cricoid cartilage
Lower border and
inferior cornu of
thyroid cartilage
External
laryngeal nerve
Thyroarytenoid
(vocalis)
Inner surface of thyroid
cartilage
Arytenoid cartilage
Recurrent
laryngeal nerve
Relaxes vocal cords
Lateral
cricoarytenoid
Upper border of cricoid
cartilage
Muscular process of
arytenoid cartilage
Recurrent
laryngeal nerve
Adducts the vocal cords by
rotating arytenoid cartilage
Posterior
cricoarytenoid
Back of cricoid cartilage
Muscular process of
arytenoid cartilage
Recurrent
laryngeal nerve
Abducts the vocal cords by
rotating arytenoid cartilage
arytenoid
Back and medial surface of
arytenoid cartilage
Back and medial
surface of opposite
arytenoid cartilage
Recurrent
laryngeal nerve
Closes posterior part of rima
glottidis by approximating
arytenoid cartilages
-
-
-
tongue, teeth, and lips. Vowel sounds are usually purely
into recognizable consonants and vowels by the use of the
Normal speech depends on the modification of the sound
plate, tongue, floor of the mouth, cheeks, lips, and jaws.
quality of the voice is controlled by the muscles of the soft
namely, the pharynx, mouth, and paranasal sinuses. The
of the voice depends on the resonators above the larynx,
quality
the length and tension of the vocal ligaments. The
of the sound is determined by changes in
pitch,
or
quency,
fre
their vibration and in the production of sound. The
of expired air between the adducted vocal folds results in
The intermittent release
-
Basic Anatomy
649
relaxed
right vocal
ligament (cord)
external view of
right lamina of
thyroid cartilage
cricothyroid
muscle
cricoid
cartilage
A
B
internal view of
right lamina of
thyroid cartilage
vocal process
right arytenoid
cartilage
lamina of
cricoid cartilage
C
stretched
right vocal
ligament (cord)
relaxed
right vocal
ligament (cord)
cri
mu
cri
ca
A
B
internal v
right lami
thyroid ca
vocal
righ
cart
lamin
cricoid
C
stretched
right vocal
ligament (cord)
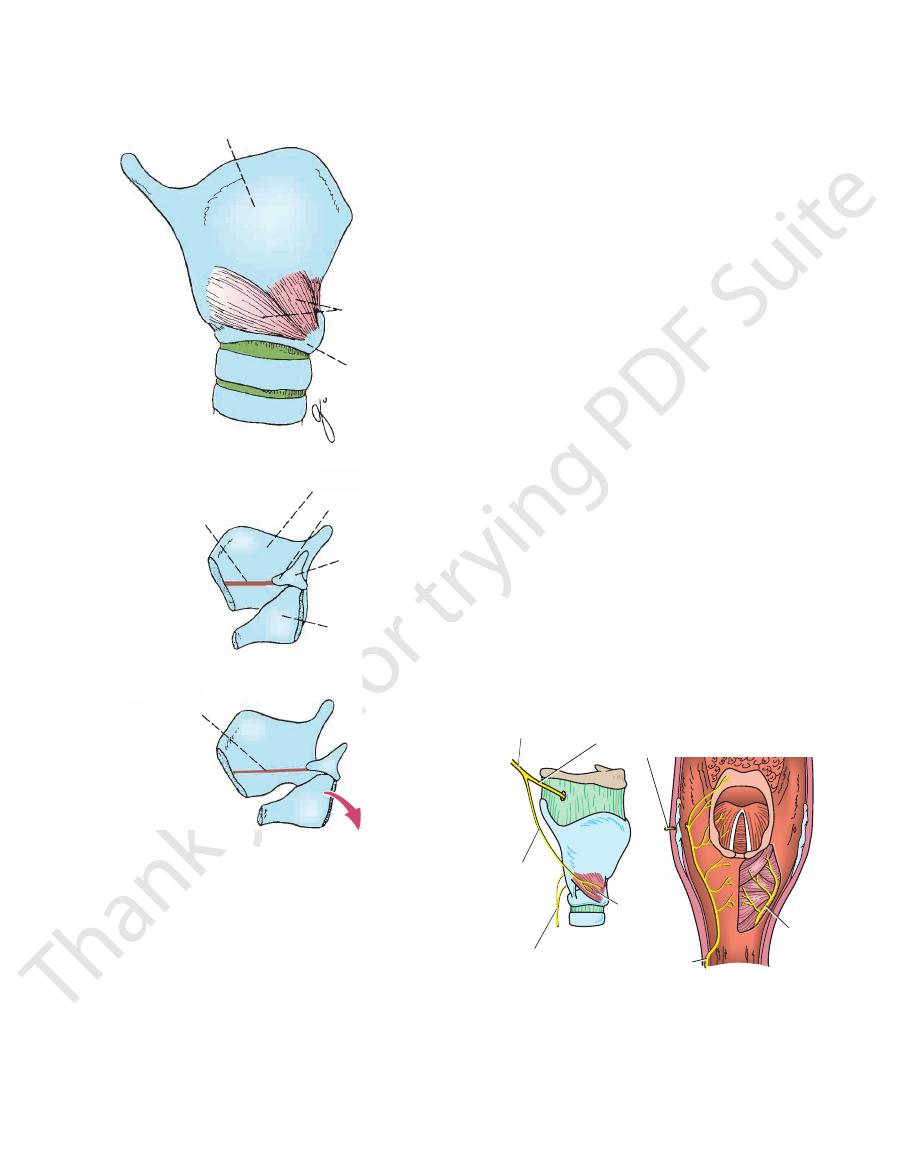
FIGURE 11.100
hments and
Diagrams showing the attac
nodes.
The lymph vessels drain into the deep cervical group of
Lymph Drainage of the Larynx
of the inferior thyroid artery
The inferior laryngeal branch
Lower half of the larynx:
of the superior thyroid artery
The superior laryngeal branch
Upper half of the larynx:
of the vagus.
external laryngeal branch of the superior laryngeal branch
laryngeal nerve. The cricothyroid muscle is supplied by the
the cricothyroid muscle are supplied by the recurrent
All the intrinsic muscles of the larynx except
Motor Nerves
geal nerve (Fig. 11.101)
The recurrent laryn
Below the level of the vocal cords:
the superior laryngeal branch of the vagus
The internal laryngeal branch of
Above the vocal cords:
Sensory Nerves
Nerve Supply of the Larynx
is covered with stratified squamous epithelium.
repeated trauma during phonation, the mucous membrane
cords, however, where the mucous membrane is subject to
is covered with ciliated columnar epithelium. On the vocal
The mucous membrane of the larynx lines the cavity and
Mucous Membrane of the Larynx
glottidis.
air that passes through the posterior part of the rima
the vibrations are given to a constant stream of expired
tilting backward by contraction of the cricothyroid muscles.
stretched as a result of the cricoid and arytenoid cartilages
Interior view of the larynx showing the right vocal ligament
larynx showing the relaxed right vocal ligament.
Interior view of the
the larynx and the cricothyroid muscle.
Right lateral view of
actions of the cricothyroid muscle. A.
B.
C.
■
■
■
■
-
Blood Supply of the Larynx
■
■
■
■
internal laryngeal
nerve
superior
laryngeal
branch of
vagus nerve
exterior
laryngeal
nerve
recurrent
laryngeal
nerve
recurrent
laryngeal
nerve
recurrent
laryngeal
nerve
(mucous
membrane
removed)
cricothyroid
muscle
A
B
FIGURE 11.101
A.
adducted, but the arytenoid cartilages are separated;
adducted vocal folds. In whispering, the vocal folds are
a more prolonged release of the expired air between the
a note requires
Singing
between the adducted vocal folds.
involves the intermittent release of expired air
Speech
through the mouth rather than the nose.
oral with the soft palate raised so that the air is channeled
The larynx is viewed from above and posteriorly.
nal branches of the internal and recurrent laryngeal nerves.
The distribution of the termi
branch of the vagus nerve.
and external laryngeal branches of the superior laryngeal
Lateral view of larynx showing the internal
B.
-
650
CHAPTER 11
The Head and Neck
Lesions of the Laryngeal Nerves
the blade tip has left the esophagus, it is in the laryngeal part
and is, therefore, distal to the level of the vocal cords. Once
Remember that the tip of the blade is at first in the esophagus
all times and is permitted to rise up out of the esophagus.
drawn. The tip of the blade is kept under direct vision at
is anatomically). The blade should by now have moved toward
fully inserted into the esophagus (so that you know where it
and down into the esophagus. The tip of the blade must be
molar teeth. The blade can then be passed over the tongue
the blade is correctly placed alongside the right mandibular
The laryngoscope is inserted into the patient’s mouth, and
lished and the patient has assumed the “sniffing” position.
The patient’s head and neck are correctly positioned so that
If the patient is asked to breathe deeply, the vocal folds become
clearly seen. The two elevations produced by the corniculate
a pillow and the head is fully extended at the atlanto-occipital
tidis to swell and encroach on the airway. In severe cases, a cri
The mucous membrane of the larynx is loosely attached to the
drawing together of the vocal folds (Fig. 11.102). Acute breath
results in bilateral paralysis of the abductor muscles and the
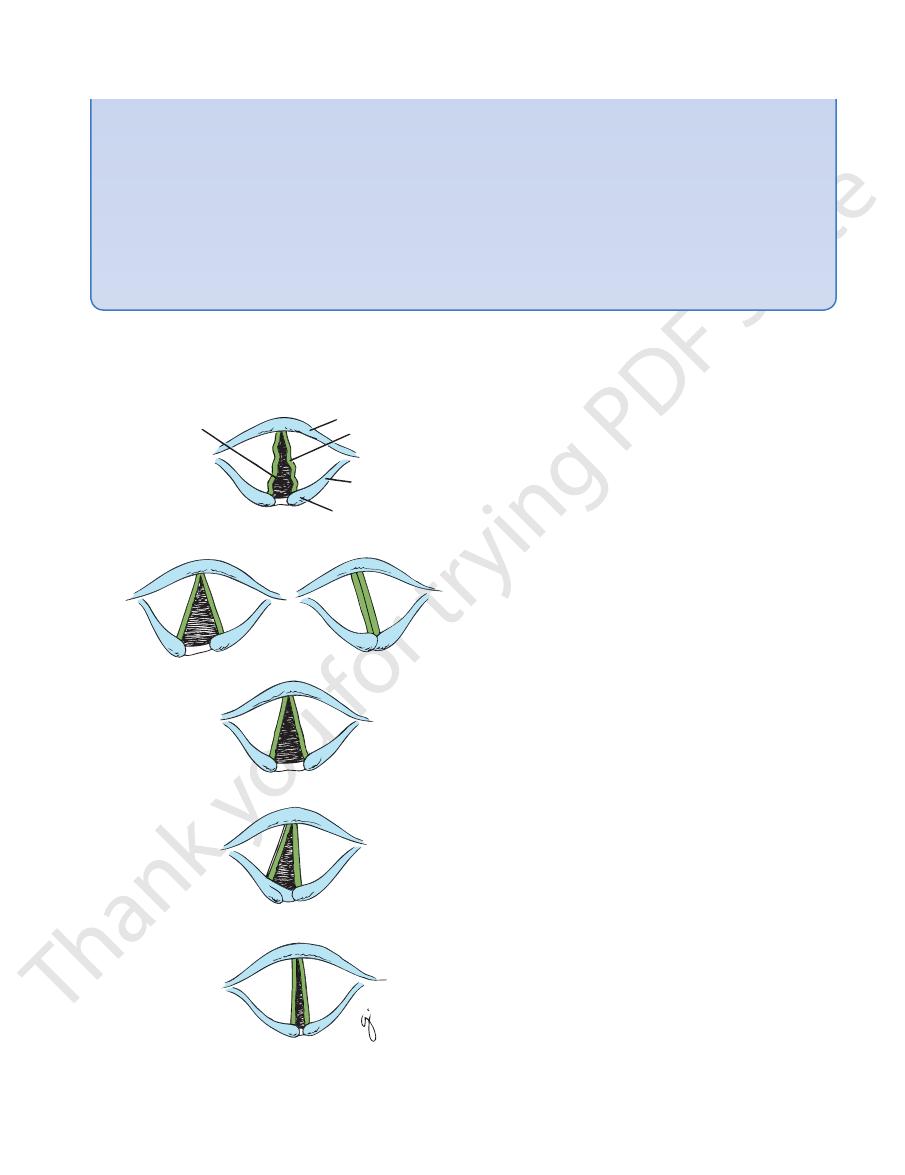
Bilateral partial section of the recurrent laryngeal nerve
than of the adductor muscles. The affected vocal fold assumes
vocal fold compensates to some extent and moves toward the
of the voice because the vocal fold cannot be tensed. The crico
rent laryngeal nerves may be damaged by malignant involve
deposits in the mediastinal lymph nodes. The right and left recur
geal nerves, with the exception of the cricothyroid muscle, which
The muscles of the larynx are innervated by the recurrent laryn-
is supplied by the external laryngeal nerve. Both these nerves
are vulnerable during operations on the thyroid gland because
of the close relationship between them and the arteries of the
gland. The left recurrent laryngeal nerve may be involved in a
bronchial or esophageal carcinoma or in secondary metastatic
-
-
ment of the deep cervical lymph nodes.
Section of the external laryngeal nerve produces weakness
-
thyroid muscle is paralyzed (Fig. 11.102).
Unilateral complete section of the recurrent laryngeal nerve
results in the vocal fold on the affected side assuming the posi-
tion midway between abduction and adduction. It lies just lateral
to the midline. Speech is not greatly affected because the other
affected vocal fold (Fig. 11.102).
Bilateral complete section of the recurrent laryngeal nerve
results in both vocal folds assuming the position midway between
abduction and adduction. Breathing is impaired because the
rima glottidis is partially closed, and speech is lost (Fig. 11.102).
Unilateral partial section of the recurrent laryngeal nerve
results in a greater degree of paralysis of the abductor muscles
the adducted midline position (Fig. 11.102). This phenomenon
has not been explained satisfactorily. It must be assumed that
the abductor muscles receive a greater number of nerves than
the adductor muscles, and thus partial damage of the recurrent
laryngeal nerve results in damage to relatively more nerve fibers
to the abductor muscles. Another possibility is that the nerve
fibers to the abductor muscles are traveling in a more exposed
position in the recurrent laryngeal nerve and are therefore more
prone to be damaged.
-
lessness (dyspnea) and stridor follow, and cricothyroidotomy or
tracheostomy is necessary.
Edema of the Laryngeal Mucous Membrane
underlying structures by submucous connective tissue. In the
region of the vocal folds, however, the mucous membrane is
firmly attached to the vocal ligaments. This fact is of clinical
importance in cases of edema of the larynx. The accumulation of
tissue fluid causes the mucous membrane above the rima glot-
-
cothyroidotomy or tracheostomy may be necessary.
Laryngeal Mirror and Laryngoscope
The interior of the larynx can be inspected indirectly through a
laryngeal mirror passed through the open mouth into the oral
pharynx (Fig. 11.103). A more satisfactory method is the direct
method using the laryngoscope. The neck is brought forward on
joints. The illuminated instrument can then be introduced into the
larynx over the back of the tongue (Fig. 11.103). The valleculae,
the piriform fossae, the epiglottis, and the aryepiglottic folds are
and cuneiform cartilages can be recognized. Within the larynx,
the vestibular folds and the vocal folds can be seen. The former
are fixed, widely separated, and reddish in color; the latter move
with respiration and are white in color. With quiet breathing,
the rima glottidis is triangular, with the apex in front. With deep
inspiration, the rima glottidis assumes a diamond shape because
of the lateral rotation of the arytenoid cartilages.
widely abducted, and the inside of the trachea can be seen.
Important Anatomic Axes for Endotracheal Intubation
The upper airway has three axes that have to be brought into
alignment if the glottis is to be viewed adequately through a
laryngoscope—the axis of the mouth, the axis of the pharynx,
and the axis of the trachea (Fig. 11.104).
The following procedures are necessary: First, the head is
extended at the atlanto-occipital joints. This brings the axis of
the mouth into the correct position. Then, the neck is flexed at
cervical vertebrae C4 to C7 by elevating the back of the head off
the table, often with the help of a pillow. This brings the axes of
the pharynx and the trachea in line with the axis of the mouth.
Anatomy of the Visualization of the Vocal Cords with the
Laryngoscope
■
■
The pear-shaped epiglottis is attached by its stalk at its lower
end to the interior of the thyroid cartilage (Fig. 11.98).
■
■
The vocal cords (ligaments) are attached at their anterior
ends to the thyroid cartilage just below the attachment of the
epiglottis (Fig. 11.98).
■
■
Because of the above two facts, it follows that manipulation
of the epiglottis and possibly the thyroid cartilage will greatly
assist the operator in visualizing the cords and the glottis.
the three axes of the airway (noted above) have been estab-
the midline and followed the anatomic curvature on the poste-
rior surface of the tongue.
The laryngoscopic blade is then gently and slowly with-
C L I N I C A L N O T E S
(continued)
Basic Anatomy
651
of the pharynx (Figs. 11.88 and 11.91), and a view of the glottis
changes are largely mediated through the branches of the
lar changes such as bradycardia and hypertension. These
during the process of intubation may produce cardiovascu
Stimulation of the mucous membrane of the upper airway
Again use your knowledge of anatomy. With the right
epiglottis to expose the glottis. If the glottis is still not in view,
Now use your anatomic
the glottis is not visualized, then the operator is viewing the
should immediately be apparent. This is the critical stage. If
posterior surface of the epiglottis.
knowledge.
With the tip of the blade of the laryngoscope applied to the
posterior surface of the epiglottis, gently lift up and elevate the
do
not panic!
free hand, grasp the thyroid cartilage (to which the cords and the
epiglottis are attached) between finger and thumb and apply firm
backward, upward, rightward pressure (BURP). This maneuver
realigns the box of the larynx relative to the laryngoscopic blade,
and the visual axis of the operator and the glottis should imme-
diately be seen.
Reflex Activity Secondary to Endotracheal Intubation
-
vagus nerves.
rima
glottidis
epiglottis
right vocal
fold (cord)
aryepiglottic fold
corniculate cartilage
inspiration
phonation
inspiration
inspiration
inspiration
inspiration
A.
Bilateral
external laryngeal
nerve palsy
Unilateral
complete section
of right recurrent
laryngeal nerve
Unilateral partial section
of right recurrent
laryngeal nerve
Bilateral
complete section
of recurrent laryngeal
nerves
Bilateral partial section
of recurrent laryngeal
nerves
B.
C.
D.
E.
deep cervical nodes
Into the pretracheal and paratracheal lymph nodes and the
Lymph Drainage of the Trachea
arteries.
arteries and the lower third is supplied by the bronchial
The upper two thirds is supplied by the inferior thyroid
Blood Supply of the Trachea
laryngeal nerves.
The sensory nerve supply is from the vagi and the recurrent
Nerve Supply of the Trachea
the thorax are described on page 63.
The relations of the trachea in the superior mediastinum of
sheath and contents (Fig. 11.49)
Lobes of the thyroid gland and the carotid
Laterally:
and the esophagus
Right and left recurrent laryngeal nerves
Posteriorly:
lapped by the sternothyroid and sternohyoid muscles
sent), and the left brachiocephalic vein in children, over
thyroid vein, jugular arch, thyroidea ima artery (if pre
(in front of the second, third, and fourth rings), inferior
Skin, fascia, isthmus of the thyroid gland
Anteriorly:
Relations of the Trachea in the Neck
many goblet cells and tubular mucous glands.
pseudostratified ciliated columnar epithelium and contains
The mucous membrane of the trachea is lined with
muscle.
trachealis
tilage are connected by smooth muscle, the
embedded in its wall. The posterior free ends of the car
U-shaped cartilaginous bar (rings) of hyaline cartilage
The fibroelastic tube is kept patent by the presence of
thoracic vertebrae).
the sternal angle (opposite the disc between the 4th and 5th
into right and left principal (main) bronchi at the level of
by dividing
carina
In the thorax, the trachea ends at the
6th cervical vertebra. It descends in the midline of the neck.
at the lower border of the cricoid cartilage at the level of the
tube (Fig. 11.105). It begins as a continuation of the larynx
The trachea is a mobile cartilaginous and membranous
Description
The Trachea
-
■
■
-
-
■
■
■
■
FIGURE 11.102
The position of the vocal folds (cords) after
damage to the external and recurrent laryngeal nerves.