Basic Anatomy
93
arterial end
venous end
dorsal mesocardium
loss of dorsal mesocardium
serous
pericardium
visceral
layers of serous
pericardium
fibrous
pericardium
pericardial cavity
transverse sinus
superior vena cava
pulmonary veins
pulmonary trunk
aorta
inferior vena
cava
fibrous pericardium
transverse sinus
oblique sinus
endocardial tube
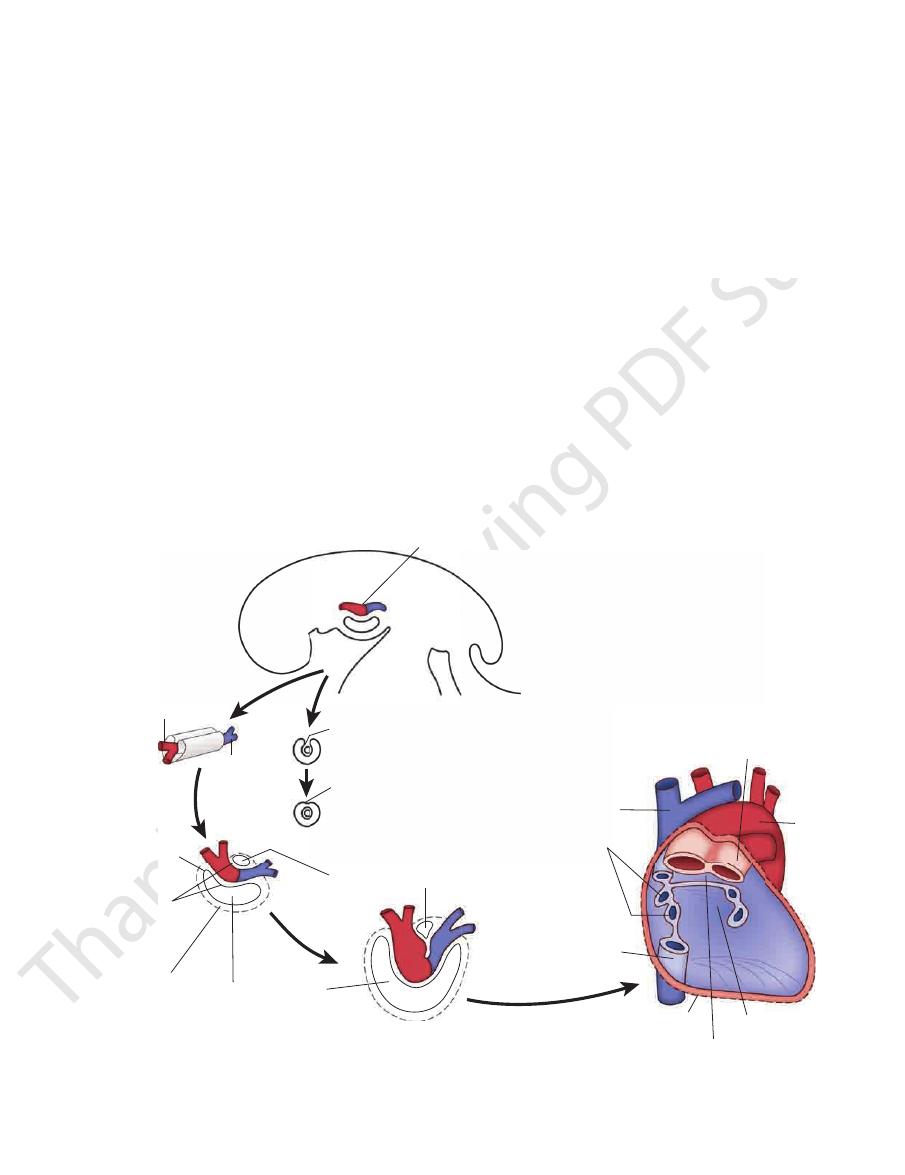
FIGURE 3.43
The development of the endocardial tube in relation to the pericardial cavity.
heart (Fig. 3.36). The vena azygos joins the posterior aspect
3.48). It passes downward to end in the right atrium of the
the union of the two brachiocephalic veins (Figs. 3.32 and
the head and neck and both upper limbs and is formed by
The superior vena cava contains all the venous blood from
Superior Vena Cava
the superior vena cava (Fig. 3.48).
aortic arch. It joins the right brachiocephalic vein to form
manubrium sterni and in front of the large branches of the
It passes obliquely downward and to the right behind the
has a similar origin (Figs. 3.30 and 3.32).
chiocephalic vein
left bra
internal jugular veins (Figs. 3.15 and 3.48). The
the neck by the union of the right subclavian and the right
is formed at the root of
right brachiocephalic vein
The
Brachiocephalic Veins
Large Veins of the Thorax
-
include large ventricular septal defect; stenosis of the pulmonary
the abdominal veins and increasing the systemic arterial resis
severe untreated abnormalities die. Once the diagnosis has been
congenital cyanosis and considerably limit activity; patients with
the high blood pressure in the right ventricle. The defects cause
ity only); and severe hypertrophy of the right ventricle, because of
ventricular septal defect (instead of from the left ventricular cav
or at the pulmonary valve; exit of the aorta immediately above the
trunk, which can occur at the infundibulum of the right ventricle
-
made, most children can be successfully treated surgically.
Most children find that assuming the squatting position after
physical activity relieves their breathlessness. This happens
because squatting reduces the venous return by compressing
-
tance by kinking the femoral and popliteal arteries in the legs;
both these mechanisms tend to decrease the right-to-left shunt
through the ventricular septal defect and improve the pulmonary
circulation.
94
CHAPTER 3
The Thorax: Part II—The Thoracic Cavity
arteries of
pharyngeal arches
pericardial
cavity
serous
pericardium
fibrous
pericardium
umbilical vein
vitelline vein
common cardinal vein
aortic sac
truncus arteriosus
(distal part of
bulbus cordis)
bulbus cordis
ventricle
atrium
sinus venosus
horn of sinus venosus
FIGURE 3.44
The parts of the endocardial heart tube within
the pericardium.
aortic sac
atrium
sinus venosus
ventricle
aortic sac
bulbus cordis
horns of sinus
venosus
atrium
aortic sac
truncus
arteriosus
lower part of
bulbus cordis
atrium
sinus venosus
ventricle
aortic sac
aortic
sac
bulbus cordis
bulbus cordis
truncus arteriosus
ventricle
right atrium
right atrium
left atrium
left atrium
right ventricle
ventricular septum
left ventricle
atrioventricular canal
FIGURE 3.45
The bending of the heart tube within the pericardial cavity. The interior of the developing ventricles is shown at
Figs. 3.15, 3.36, and 3.48).
immediately enters the lowest part of the right atrium (see
phragm opposite the eighth thoracic vertebra and almost
The inferior vena cava pierces the central tendon of the dia
Inferior Vena Cava
at the level of the seventh thoracic vertebra (see Fig. 2.11).
fourth to the eighth intercostal veins. It joins the azygos vein
The superior hemiazygos vein is formed by the union of the
Superior Hemiazygos Vein
tinal veins.
medias
lower left intercostal veins
tributaries some
right and joins the azygos vein (see Fig. 2.11). It receives as
about the level of the eighth thoracic vertebra, turns to the
It ascends through the left crus of the diaphragm and, at
of the left ascending lumbar vein and the left subcostal vein.
The inferior hemiazygos vein is often formed by the union
Inferior Hemiazygos Vein
mediastinal veins.
and numerous
veins,
inferior hemiazygos
superior
intercostal vein,
right superior
eight lower right intercostal veins,
The azygos vein has numerous tributaries, including
cava (Fig. 3.15).
to empty into the posterior surface of the superior vena
Here it arches forward above the root of the right lung
aorta to the level of the fifth thoracic vertebra (Fig. 3.48).
tic opening in the diaphragm on the right side of the
It ascends through the aor
right subcostal vein.
right ascending lumbar vein
formed by the union of the
The origin of the azygos vein is variable. It is often
Azygos Vein
the diaphragm, the bronchi, and the esophagus (Fig. 3.48).
tal spaces, the posterior abdominal wall, the pericardium,
They drain blood from the posterior parts of the intercos
rior hemiazygos vein, and the superior hemiazygos vein.
The azygos veins consist of the main azygos vein, the infe
Azygos Veins
dium (Figs. 3.15 and 3.48).
of the superior vena cava just before it enters the pericar
the bottom right.
-
-
-
and the
-
the
the
the
and
and
-
-
Basic Anatomy
95
septum primum
endocardial
cushion
sinuatrial
orifice
foramen
primum
atrioventricular
canal
septum secundum
right atrium
interventricular
foramen
septum
primum
foramen
secundum
septum
intermedium
septum primum
breaking down
left atrium
septum
intermedium
septum secundum
septum primum
foramen ovale
membranous part of
ventricular septum
muscular part of
ventricular septum
ventricular septum
septum secundum
septum primum
foramen ovale
crista terminalis
formed from
septum spurium
valve of inferior
vena cava
valve of
coronary sinus
A
B
C
D
E
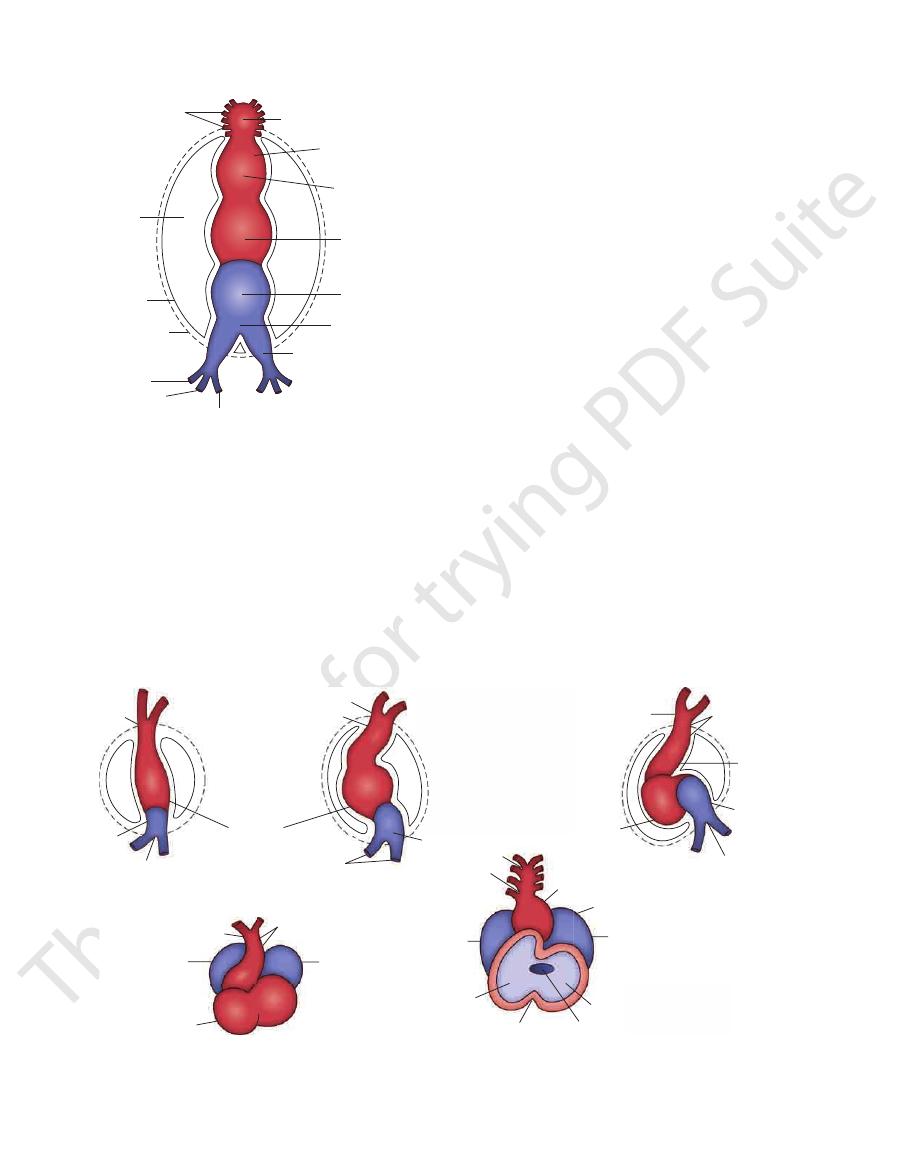
FIGURE 3.46
The division of the primitive atrium into the right and left atria by the appearance of the septa. The sinuatrial
orifice and the fate of the venous valves are shown, as is the appearance of the ventricular septum.
Azygos Veins and Caval Obstruction
In obstruction of the superior or inferior venae cavae, the
azygos veins provide an alternative pathway for the return of
venous blood to the right atrium of the heart. This is possible
because these veins and their tributaries connect the superior
and inferior venae cavae.
C L I N I C A L N O T E S
Pulmonary Veins
ated blood to the left atrium of the heart (Figs. 3.15, 3.35,
Two pulmonary veins leave each lung carrying oxygen-
and 3.39).
arches over the apex of the left lung.
the esophagus to enter the root of the neck (Fig. 3.15). It
3.49). It runs upward along the left side of the trachea and
behind the left common carotid artery (Figs. 3.34, 3.35, and
arises from the aortic arch
left subclavian artery
The
sternoclavicular joint.
the left of the trachea and enters the neck behind the left
phalic artery (Figs. 3.34 and 3.49). It runs upward and to
surface of the aortic arch on the left side of the brachioce
arises from the convex
left common carotid artery
The
right sternoclavicular joint.
subclavian and right common carotid arteries behind the
and to the right of the trachea and divides into the right
of the aortic arch (Figs. 3.34 and 3.49). It passes upward
arises from the convex surface
brachiocephalic artery
The
Branches
descending aorta.
level of the sternal angle, becomes continuous with the
passes downward to the left of the trachea and, at the
of the trachea (its main direction is backward). It then
and arches upward, backward, and to the left in front
aorta (Fig. 3.34). It lies behind the manubrium sterni
The arch of the aorta is a continuation of the ascending
Arch of the Aorta
of these important arteries is described on pages 86 to 87.
terior aortic sinus (Figs. 3.34 and 3.41). The further course
arises from the left pos
left coronary artery
sinus, and the
arises from the anterior aortic
right coronary artery
The
Branches
each aortic valve cusp.
one behind
sinuses of the aorta,
possesses three bulges, the
nary trunk in a sheath of serous pericardium. At its root, it
pericardium (Fig. 3.32) and is enclosed with the pulmo
(Fig. 3.34). The ascending aorta lies within the fibrous
where it becomes continuous with the arch of the aorta
right half of the sternum at the level of the sternal angle,
and runs upward and forward to come to lie behind the
The ascending aorta begins at the base of the left ventricle
Ascending Aorta
descending thoracic aorta, and abdominal aorta.
into the following parts: ascending aorta, arch of the aorta,
sues of the body. It is divided for purposes of description
ated blood from the left ventricle of the heart to the tis
The aorta is the main arterial trunk that delivers oxygen
Large Arteries of the Thorax
Aorta
-
-
-
-
-
96
CHAPTER 3
The Thorax: Part II—The Thoracic Cavity
Upper Part of Bulbus Cordis
Lower Part of Bulbus Cordis
blood in
pulmonary trunk
aorta
pulmonary trunk
right bulbar ridge
septum
intermedium
(endocardial
cushions)
left bulbar
ridge
interventricular
foramen
ventricular septum
(muscular part)
spiral
aorticopulmonary
septum
blood entering
aorta
right
bulbar
ridge
right
atrioventricular
opening
left
bulbar
ridge
septum
intermedium
(endocardial
cushions)
right
ventricle
A
B
C
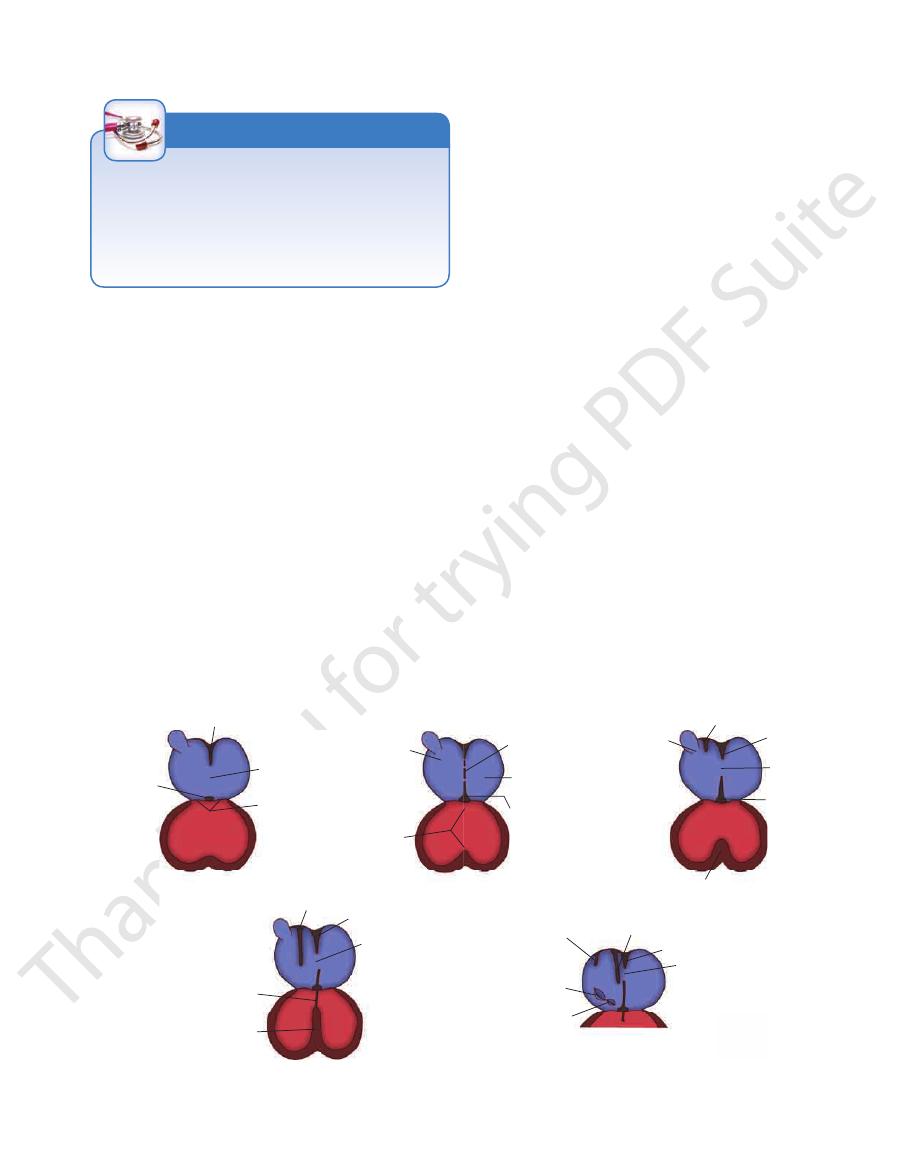
FIGURE 3.47
The division of the bulbus cordis by the spiral aorticopulmonary septum into the aorta and pulmonary trunk.
) is called the membranous part of the ventricular septum.
) and the septum intermedium (
The area of the ventricular septum that is formed from the
) and the muscular part of the ventricular septum.
), which then grow down and join the septum interme
the formation of the spiral septum by fusion of the bulbar ridges (
The lower part of the bulbus cordis showing
The spiral septum in the truncus arteriosus (upper part of the bulbus cordis).
A.
B.
red
-
dium (blue
C.
fused bulbar ridges (red
blue
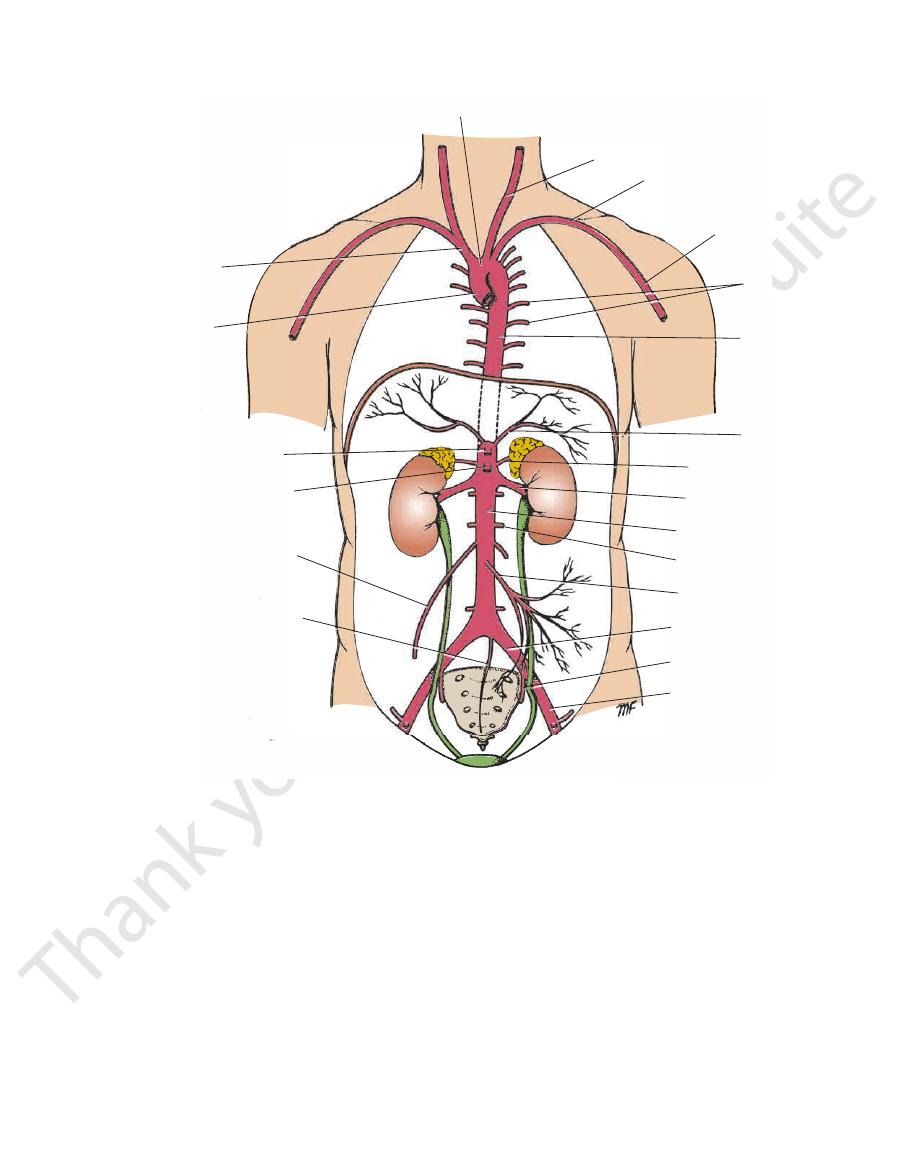
inferior thyroid vein
left internal jugular vein
left subclavian vein
left brachiocephalic vein
left internal thoracic vein
left pulmonary veins
great cardiac vein
inferior vena cava
branches of
anterior cardiac vein
superior vena cava
right
brachiocephalic vein
left internal jugular vein
left subclavian vein
left brachiocephalic vein
posterior intercostal veins
hemiazygos veins
hepatic veins
left suprarenal vein
left testicular (ovarian) vein
inferior vena cava
median sacral vein
right brachiocephalic vein
superior vena cava
azygos vein
inferior phrenic vein
right suprarenal vein
right renal vein
right testicular (ovarian) vein
right lumbar veins
right common iliac vein
right internal iliac vein
right external iliac vein
A
B
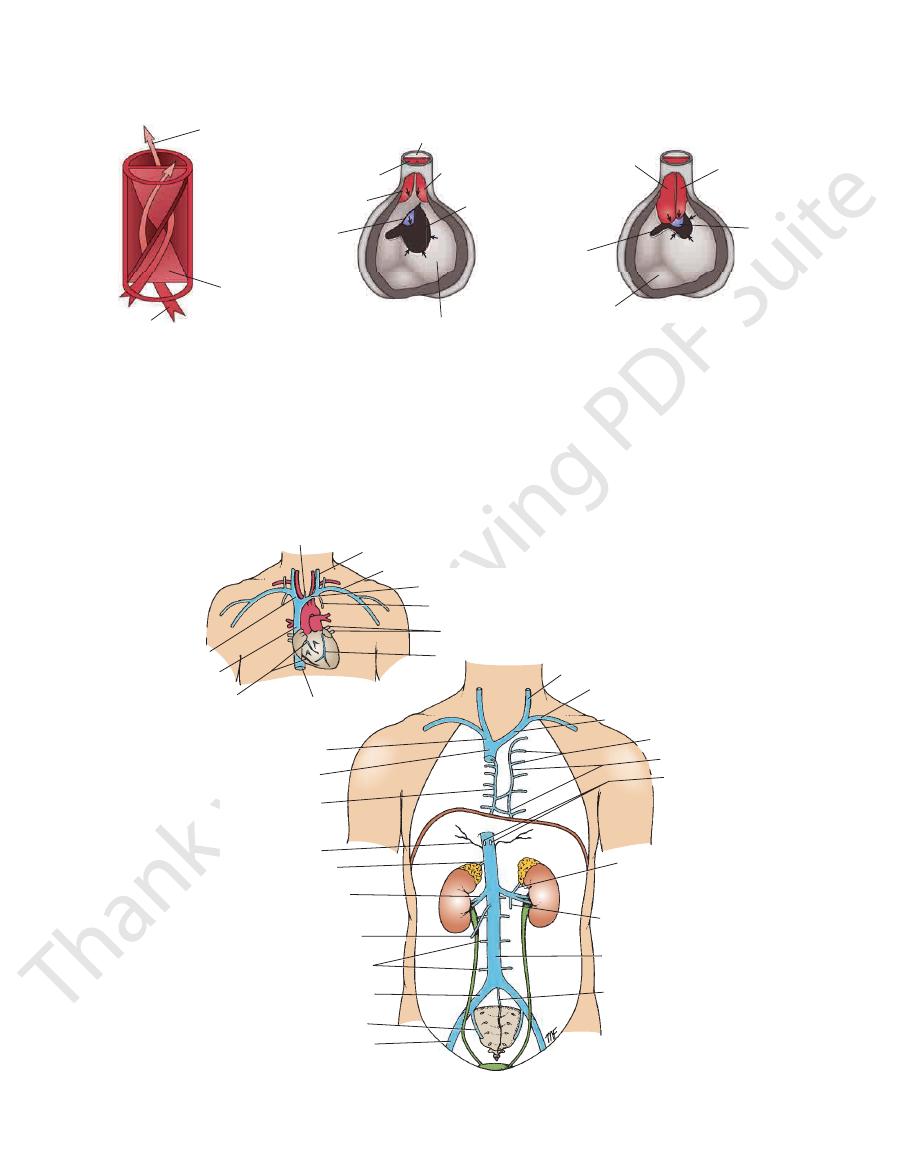
FIGURE 3.48
Major veins draining into the superior and inferior venae cavae.
Major veins entering the heart.
A.
B.
Basic Anatomy
97
arch of aorta
brachiocephalic
artery
ascending
aorta
celiac artery
superior
mesenteric artery
testicular
(ovarian) artery
median
sacral artery
left common carotid artery
left subclavian
artery
axillary artery
posterior
intercostal
arteries
descending
thoracic
aorta
inferior
phrenic artery
suprarenal artery
renal artery
abdominal aorta
lumbar artery
inferior
mesenteric artery
common iliac artery
internal iliac artery
external iliac artery
FIGURE 3.49
Major branches of the aorta.
(Fig. 3.32).
fibrous pericardium and a sheath of serous pericardium
Together with the ascending aorta, it is enclosed in the
dividing into right and left pulmonary arteries (Fig. 3.11).
long and terminates in the concavity of the aortic arch by
ward, and to the left (Fig. 3.34). It is about 2 in. (5 cm)
upper part of the right ventricle and runs upward, back
the right ventricle of the heart to the lungs. It leaves the
The pulmonary trunk conveys deoxygenated blood from
Pulmonary Trunk
small branches that are distributed to these organs.
are
bronchial arteries
Pericardial, esophageal,
border of the 12th rib to enter the abdominal wall.
are given off on each side and run along the lower
arteries
Subcostal
nine intercostal spaces on each side (Fig. 3.49).
are given off to the lower
Posterior intercostal arteries
Branches
continuous with the abdominal aorta.
(through the aortic opening) in the midline and becomes
the 12th thoracic vertebra, it passes behind the diaphragm
the vertebral column (Figs. 3.15 and 3.49). At the level of
ing forward and medially to reach the anterior surface of
It runs downward in the posterior mediastinum, inclin
the 4th thoracic vertebra (i.e., opposite the sternal angle).
aorta on the left side of the lower border of the body of
astinum and begins as a continuation of the arch of the
The descending thoracic aorta lies in the posterior medi
Descending Thoracic Aorta
-
-
and
-
98
CHAPTER 3
necessary.
ventricle (Fig. 3.37). Surgical ligation of the ductus is then
pulmonary hypertension and hypertrophy of the right
blood will enter the pulmonary circulation, producing
birth, the ductus closes. Should it remain patent, aortic
lower border of this structure (Figs. 3.15 and 3.35). After
lungs. The left recurrent laryngeal nerve hooks around the
the pulmonary trunk to the aorta, thus bypassing the
ductus arteriosus, which in the fetus conducts blood from
3.35). The ligamentum arteriosum is the remains of the
lower concave surface of the aortic arch (Figs. 3.15 and
connects the bifurcation of the pulmonary trunk to the
is a fibrous band that
ligamentum arteriosum
The
(Figs. 3.11, 3.15, and 3.34).
of the descending aorta to enter the root of the left lung
runs to the left in front
left pulmonary artery
The
the right lung (Figs. 3.11, 3.15, and 3.34).
ascending aorta and superior vena cava to enter the root of
runs to the right behind the
right pulmonary artery
The
Branches
The Thorax: Part II—The Thoracic Cavity
Patent Ductus Arteriosus
The ductus arteriosus represents the distal portion of the sixth
left aortic arch and connects the left pulmonary artery to the
beginning of the descending aorta (Fig. 3.37D). During fetal
life, blood passes through it from the pulmonary artery to the
aorta, thus bypassing the lungs. After birth, it normally con-
stricts, later closes, and becomes the ligamentum arteriosum.
Failure of the ductus arteriosus to close may occur as an
isolated congenital abnormality or may be associated with
congenital heart disease. A persistent patent ductus arte-
riosus results in high-pressure aortic blood passing into the
pulmonary artery, which raises the pressure in the pulmonary
circulation. A patent ductus arteriosus is life threatening and
should be ligated and divided surgically.
C L I N I C A L N O T E S
Aneurysm and Coarctation of the Aorta
the lower borders of the ribs, producing characteristic notch
terior intercostal arteries. The dilated intercostal arteries erode
To compensate for the diminished volume of blood reaching the
lumen becomes narrowed. Later, when fibrosis takes place, the
from an unusual quantity of ductus arteriosus muscle tissue in
of the ligamentum arteriosum. This condition is believed to result
The arch of the aorta lies behind the manubrium sterni. A gross
dilatation of the aorta (aneurysm) may show itself as a pulsatile
swelling in the suprasternal notch.
Coarctation of the aorta is a congenital narrowing of the
aorta just proximal, opposite, or distal to the site of attachment
the wall of the aorta. When the ductus arteriosus contracts, the
ductal muscle in the aortic wall also contracts, and the aortic
aortic wall also is involved, and permanent narrowing occurs.
Clinically, the cardinal sign of aortic coarctation is absent
or diminished pulses in the femoral arteries of both lower limbs.
lower part of the body, an enormous collateral circulation devel-
ops, with dilatation of the internal thoracic, subclavian, and pos-
-
ing, which is seen on radiographic examination. The condition
should be treated surgically.
C L I N I C A L N O T E S
Lymph Nodes and Vessels of the
the left edge of the esophagus to enter the root of the neck
racic vertebra (sternal angle). It then runs upward along
the level of the lower border of the body of the 4th tho
and reaches the left border of the esophagus (Fig. 3.6B) at
It gradually crosses the median plane behind the esophagus
in the diaphragm, on the right side of the descending aorta.
It ascends through the aortic opening
cisterna chyli.
sac, the
The thoracic duct begins below in the abdomen as a dilated
chea and superior vena cava.
tant neighboring mediastinal structures, such as the tra
enlargement of these nodes may exert pressure on impor
bronchomediastinal trunks and thoracic duct. Disease and
lymph from mediastinal structures and empty into the
are found scattered through the mediastinum. They drain
In addition to the nodes draining the lungs, other nodes
lymph enters the thoracic duct.
lying near the heads of the ribs. From here, the
costal nodes
posterior inter
intercostal spaces drain backward to the
side. The deep lymph vessels of the posterior parts of the
left side and the bronchomediastinal trunk on the right
From here, the lymph passes to the thoracic duct on the
along the internal thoracic blood vessels.
thoracic nodes
internal
parts of the intercostal spaces drain forward to the
The deep lymph vessels of the anterior
rior axillary nodes.
poste
the skin of the posterior thoracic wall drain to the
The lymph vessels of
anterior axillary nodes.
drain to the
The lymph vessels of the skin of the anterior thoracic wall
Thoracic Wall
Thorax
-
-
Mediastinum
-
-
Thoracic Duct
-
(Fig. 3.6B). Here, it bends laterally behind the carotid sheath
artery to enter the beginning of the left brachiocephalic vein.
front of the left phrenic nerve and crosses the subclavian
and in front of the vertebral vessels. It turns downward in