170
CHAPTER 5
The Abdomen: Part II—The Abdominal Cavity
C L I N I C A L N O T E S
The Esophagus
glucagon.
reduced in response to secretin, cholecystokinin, and
and this can be augmented by the hormone gastrin and
The closure of the sphincter is under vagal control,
ing into the esophagus.
sphincter prevents the stomach contents from regurgitat
the food enters the stomach. The tonic contraction of this
at the lower end occurs ahead of the peristaltic wave so that
descends through the esophagus, relaxation of the muscle
in this region serves as a physiologic sphincter. As the food
esophagus. However, the circular layer of smooth muscle
No anatomic sphincter exists at the lower end of the
propel the food onward.
peristalsis,
stomach. Wavelike contractions of the muscular coat, called
The esophagus conducts food from the pharynx into the
Function
sympathetic trunk.
(vagi) and sympathetic branches of the thoracic part of the
The nerve supply is the anterior and posterior gastric nerves
Nerve Supply
The lymph vessels follow the arteries into the left gastric nodes.
Lymph Drainage
portal vein (see portal–systemic anastomosis, page 195).
The veins drain into the left gastric vein, a tributary of the
Veins
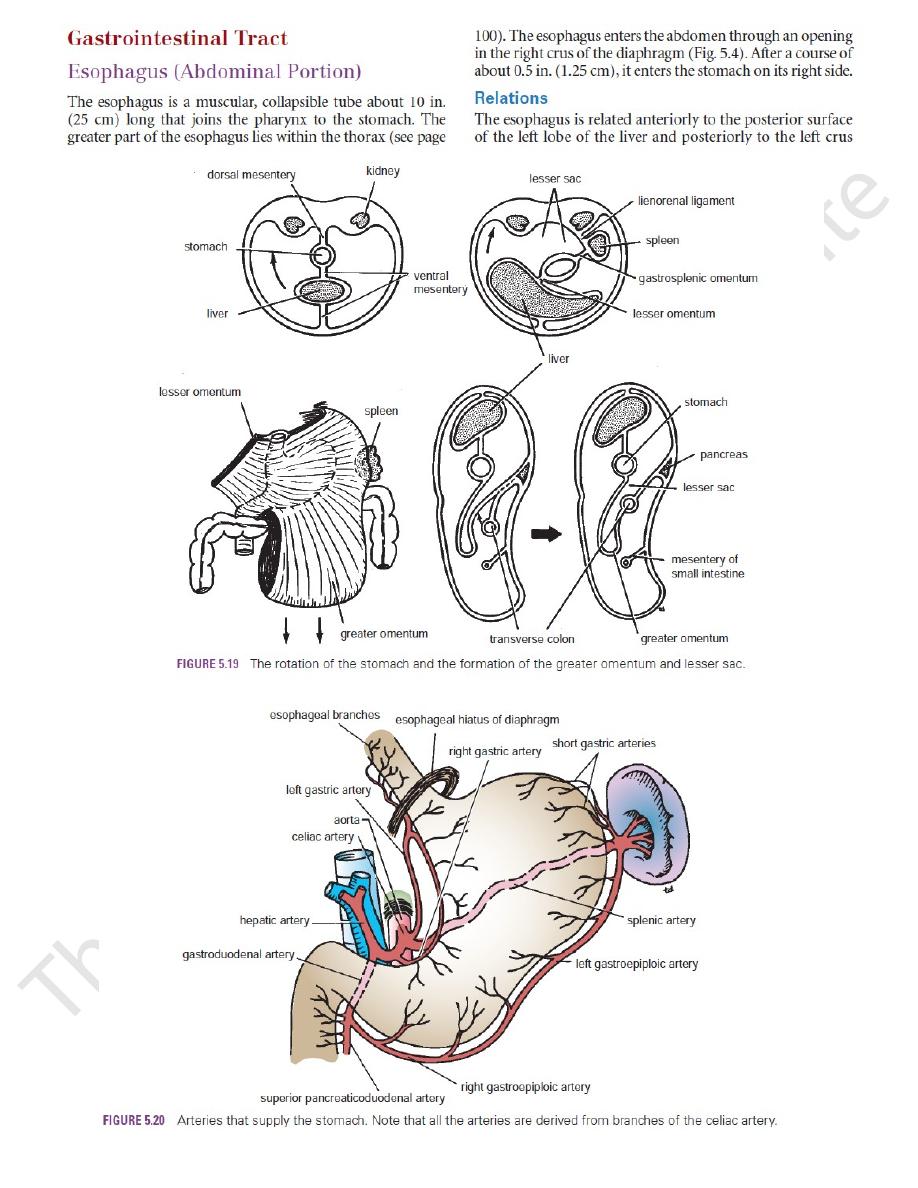
(Fig. 5.20).
The arteries are branches from the left gastric artery
Arteries
and posterior surfaces, respectively.
of the diaphragm. The left and right vagi lie on its anterior
Persistent hiccups caused by irritation of the diaphragm by the
Damage to the esophagus from overinflation of the esopha
hypertension develops, resulting in dilatation and varicosity of
At the lower third of the esophagus is an important
The causes of this disease include failure of the lower esopha
week. If the reflux continues, the esophageal mucous mem
accompanied by proximal dilatation and distal narrowing of the
lowing) and regurgitation are common symptoms that are later
disorder may be in the innervation of the cardioesophageal
plexus) in the wall of the esophagus. The primary site of the
a degeneration of the parasympathetic plexus (Auerbach’s
The cause of achalasia is unknown, but it is associated with
The esophagus is narrowed at three sites: at the beginning,
Narrow Areas of the Esophageal Lumen
behind the cricoid cartilage of the larynx; where the left bron-
chus and the arch of the aorta cross the front of the esophagus;
and where the esophagus enters the stomach. These three sites
may offer resistance to the passage of a tube down the esopha-
gus into the stomach (see Fig. 3.44).
Achalasia of the Cardia (Esophagogastric Junction)
sphincter by the vagus nerves. Dysphagia (difficulty in swal-
esophagus.
Gastroesophageal Reflux Disease
Gastroesophageal reflux disease is the most common gas-
trointestinal disorder seen in outpatient clinics. It consists of
a reflux of acid stomach contents into the esophagus produc-
ing the symptoms of heartburn on at least two occasions per
-
brane becomes inflammed. Later, if the condition persists, the
lining of the esophagus changes from squamous epithelium
to columnar epitheliuim, and there is a risk of the develop-
ment of adenocarcinoma at the lower end of the esophagus.
-
geal sphincter, hiatus hernia of the diaphragm, and abdominal
obesity.
Bleeding Esophageal Varices
portal–
systemic venous anastomosis (see page 195). Here, the esopha-
geal tributaries of the left gastric vein (which drains into the
portal vein) anastomose with the esophageal tributaries of the
azygos veins (systemic veins). Should the portal vein become
obstructed, as, for example, in cirrhosis of the liver, portal
the portal–systemic anastomoses. Varicosed esophageal veins
may rupture, causing severe vomiting of blood (hematemesis).
Anatomy of the Insertion of the Sengstaken–
Blakemore Balloon for Esophageal Hemorrhage
The Sengstaken–Blakemore balloon is used for the control
of massive esophageal hemorrhage from esophageal varices.
A gastric balloon anchors the tube against the esophageal–gas-
tric junction. An esophageal balloon occludes the esophageal
varices by counterpressure. The tube is inserted through the
nose or by using the oral route.
The lubricated tube is passed down into the stomach, and
the gastric balloon is inflated. In the average adult, the distance
between the external orifices of the nose and the stomach is 17.2 in.
(44 cm), and the distance between the incisor teeth and the
stomach is 16 in. (41 cm).
Anatomy of the Complications
■
■
Difficulty in passing the tube through the nose
■
■
-
geal tube
■
■
Pressure on neighboring mediastinal structures as the
esophagus is expanded by the balloon within its lumen
■
■
distended esophagus and irritation of the stomach by the blood
Blood Supply
Gastroesophageal Sphincter
-