Basic Anatomy
uncinate process.
sels and is called the
head extends to the left behind the superior mesenteric ves
the concavity of the duodenum (Fig. 5.58). A part of the
of the pancreas is disc shaped and lies within
head
The
creas is divided into a head, neck, body, and tail (Fig. 5.58).
the peritoneum. It crosses the transpyloric plane. The pan
lated and situated on the posterior abdominal wall behind
epigastrium and the left upper quadrant. It is soft and lobu
The pancreas is an elongated structure that lies in the
carbohydrate metabolism.
which play a key role in
glucagon,
insulin
hormones
produces the
pancreatic islets (islets of Langerhans),
and carbohydrates. The endocrine portion of the gland,
contains enzymes capable of hydrolyzing proteins, fats,
exocrine portion of the gland produces a secretion that
The pancreas is both an exocrine and endocrine gland. The
Location and Description
the lumen constantly open.
the “spiral valve.” The function of the spiral valve is to keep
the neck of the gallbladder. The fold is commonly known as
201
Pancreas
the
and
-
-
-
lumen of gallbladder
FIGURE 5.54
Longitudinal sonogram of the upper part of the
of Dr. M.C. Hill.)
abdomen showing the lumen of the gallbladder. (Courtesy
Development of the Liver and Bile Ducts
may not be recognized when performing a cholecystectomy, and
The gallbladder drains directly into the bile duct. The condition
leave the narrow stem that would normally form the cystic duct.
from the hepatic bud develops into the gallbladder and fails to
In the absence of the cystic duct, the entire outgrowth of cells
Rarely, the outgrowth of cells from the hepatic bud bifurcates so
Occasionally, the outgrowth of cells from the hepatic bud fails
atresia should be attempted when possible. If the atresia cannot
Jaundice appears soon after birth; clay-colored stools and very
comes to occupy the greater part of the abdominal cavity; the
and the
common hepatic duct
now become canalized to form the
a point halfway along the second part of the fully formed duode
entodermal cells (Figs. 5.41 and 5.55). The site of origin lies at the
Liver
The liver arises from the distal end of the foregut as a solid bud of
apex of the loop of the developing duodenum and corresponds to
-
num. The hepatic bud grows anteriorly into the mass of splanch-
nic mesoderm called the septum transversum. The end of the
bud now divides into right and left branches, from which col-
umns of entodermal cells grow into the vascular mesoderm. The
paired vitelline veins and umbilical veins that course through the
septum transversum become broken up by the invading columns
of liver cells and form the liver sinusoids. The columns of ento-
dermal cells form the liver cords. The connective tissue of the
liver is formed from the mesenchyme of the septum transversum.
The main hepatic bud and its right and left terminal branches
right and left hepatic ducts. The liver grows rapidly in size and
right lobe becomes much larger than the left lobe.
Gallbladder and Cystic Duct
The gallbladder develops from the hepatic bud as a solid out-
growth of cells (Fig. 5.41). The end of the outgrowth expands
to form the gallbladder, while the narrow stem remains as the
cystic duct. Later, the gallbladder and cystic duct become cana-
lized. The cystic duct now opens into the common hepatic duct
to form the bile duct.
Biliary Atresia
Failure of the bile ducts to canalize during development causes
atresia. The various forms of atresia are shown in Figure 5.56.
dark-colored urine are also present. Surgical correction of the
be corrected, the child will die of liver failure.
Absence of the Gallbladder
to develop. In these cases, there is no gallbladder and no cystic
duct (Fig. 5.57).
Double Gallbladder
that two gallbladders are formed (Fig. 5.57).
Absence of the Cystic Duct
the bile duct may be seriously damaged by the surgeon (Fig. 5.57).
Accessory Bile Duct
A small accessory bile duct may open directly from the liver into
the gallbladder, which may cause leakage of bile into the peri-
toneal cavity after cholecystectomy if it is not recognized at the
time of surgery (Fig. 5.57).
Congenital Choledochal Cyst
Rarely, a choledochal cyst develops because of an area of
weakness in the wall of the bile duct. A cyst can contain 1 to 2 L
of bile. The anomaly is important in that it may press on the bile
duct and cause obstructive jaundice (Fig. 5.57).
E M B R Y O L O G I C N O T E S
202
CHAPTER 5
The Abdomen: Part II—The Abdominal Cavity
stomach
ventral mesentery
first part of
duodenum
second part of
duodenum
dorsal
mesentery
hepatic bud
gallbladder
ventral
pancreatic bud
third part
of duodenum
stomach
dorsal pancreatic bud
fourth part of duodenum
gallbladder
dorsal
mesentery
dorsal
mesentery
ventral
mesentery
ventral
pancreatic bud
dorsal
pancreatic bud
liver
remains of
ventral
mesentery
gallbladder
ventral pancreatic bud
dorsal pancreatic bud
peritoneum will fuse here
and then disappear
first part of duodenum
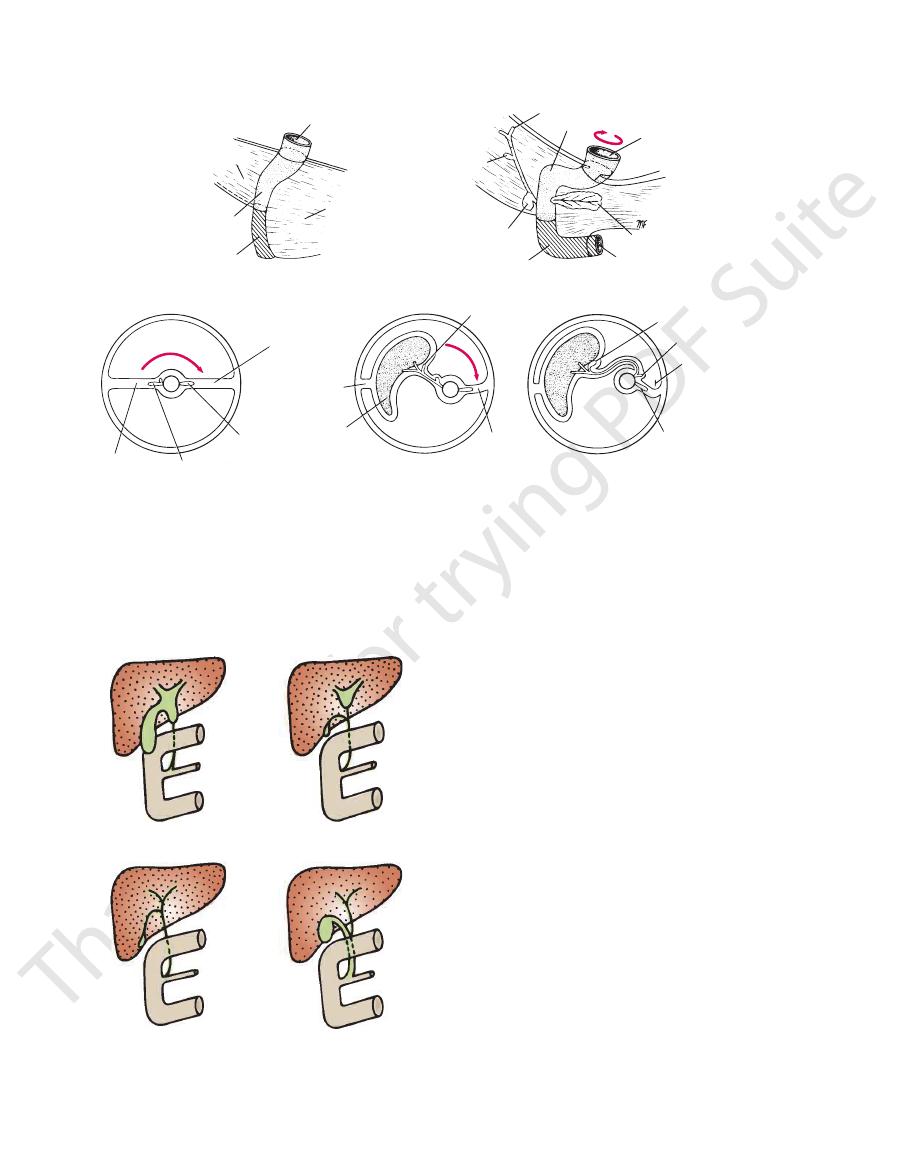
FIGURE 5.55
Development of the duodenum in relation to the ventral and dorsal mesenteries. Stippled area, foregut; cross
hatched area, midgut.
-
atresia of bile duct
atresia of hepatic duct
atresia of entire
extrahepatic apparatus
atresia of hepatic ducts
FIGURE 5.56
Some common congenital anomalies of the
denal arteries (Fig. 5.26) supply the pancreas.
The splenic and the superior and inferior pancreaticoduo
Arteries
frequently communicates with the main duct.
(Figs. 5.51 and 5.58). The accessory duct
duodenal papilla
minor
num a short distance above the main duct on the
the upper part of the head and then opens into the duode
of the pancreas, when present, drains
accessory duct
The
duct drains separately into the duodenum.
(Fig. 5.51). Sometimes, the main
major duodenal papilla
duodenum at about its middle with the bile duct on the
the way (Fig. 5.58). It opens into the second part of the
the length of the gland, receiving numerous tributaries on
begins in the tail and runs
main duct of the pancreas
The
Pancreatic Ducts
hilum of the spleen (Figs. 5.4 and 5.27)
muscle, the left suprarenal gland, the left kidney, and the
origin of the superior mesenteric artery, the left psoas
and splenic veins, the inferior vena cava, the aorta, the
From right to left: the bile duct, the portal
Posteriorly:
sac, and the stomach (Figs. 5.4 and 5.6)
the attachment of the transverse mesocolon, the lesser
From right to left: the transverse colon and
Anteriorly:
and comes in contact with the hilum of the spleen (Fig. 5.4).
passes forward in the splenicorenal ligament
The
(Fig. 5.4). It is somewhat triangular in cross section.
runs upward and to the left across the midline
body
The
enteric artery from the aorta (Fig. 5.26).
ning of the portal vein and the origin of the superior mes
connects the head to the body. It lies in front of the begin
is the constricted portion of the pancreas and
neck
The
biliary ducts.
-
-
tail
Relations
■
■
■
■
-
Blood Supply
-
Basic Anatomy
(Figs. 5.4 and 5.11).
colic flexure. The left kidney lies along its medial border
The stomach, tail of the pancreas, and left
Anteriorly:
tail of the pancreas).
splenicorenal ligament (carrying the splenic vessels and the
sels). The peritoneum also passes to the left kidney as the
ach (carrying the short gastric and left gastroepiploic ves
omentum (ligament) to the greater curvature of the stom
5.61), which passes from it at the hilum as the gastrosplenic
The spleen is surrounded by peritoneum (Figs. 5.5 and
cannot be palpated on clinical examination (Fig. 5.61).
pole extends forward only as far as the midaxillary line and
long axis lies along the shaft of the 10th rib, and its lower
the diaphragm close to the 9th, 10th, and 11th ribs. The
notched anterior border. It lies just beneath the left half of
lymphoid tissue in the body. It is oval shaped and has a
The spleen is reddish and is the largest single mass of
Location and Description
ply the area.
Sympathetic and parasympathetic (vagal) nerve fibers sup
Nerve Supply
and superior mesenteric lymph nodes.
gland. The efferent vessels ultimately drain into the celiac
Lymph nodes are situated along the arteries that supply the
Lymph Drainage
The corresponding veins drain into the portal system.
Veins
203
-
Spleen
-
-
Relations
■
■
body
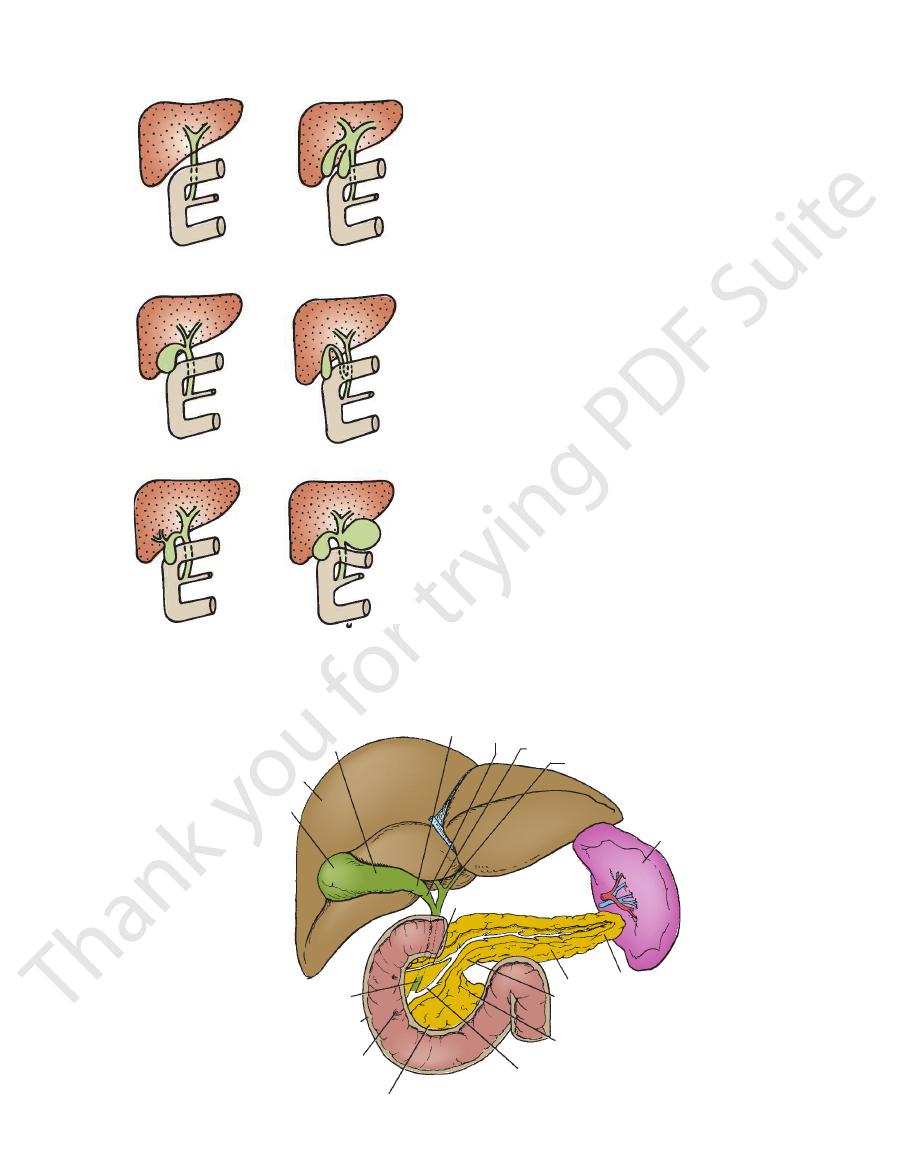
right lobe
of liver
bile duct
second part
of duodenum
major duodenal
papilla
head of pancreas
main pancreatic duct
uncinate process
neck
tail
spleen
left hepatic duct
right hepatic duct
neck
accessory pancreatic duct
fundus of
gallbladder
body
cystic duct
FIGURE 5.58
Different parts of the pancreas dissected to reveal the duct system.
absence of cystic duct
abnormally long cystic duct
congenital absence
of gallbladder
double gallbladder
accessory bile duct
choledochal cyst
FIGURE 5.57
Some common congenital anomalies of the
gallbladder.
204
CHAPTER 5
The Abdomen: Part II—The Abdominal Cavity
Diagnosis of Pancreatic Disease
atic enzymes that produce the signs and symptoms of acute
Because the pancreas lies behind the stomach and trans
The deep location of the pancreas sometimes gives rise to prob-
lems of diagnosis for the following reasons:
■
■
Pain from the pancreas is commonly referred to the back.
■
■
-
verse colon, disease of the gland can be confused with that
of the stomach or transverse colon.
■
■
Inflammation of the pancreas can spread to the peritoneum
forming the posterior wall of the lesser sac. This in turn can
lead to adhesions and the closing off of the lesser sac to form
a pseudocyst.
Trauma of the Pancreas
The pancreas is deeply placed within the abdomen and is well
protected by the costal margin and the anterior abdominal wall.
However, blunt trauma, such as in a sports injury when a sudden
blow to the abdomen occurs, can compress and tear the pan-
creas against the vertebral column. The pancreas is most com-
monly damaged by gunshot or stab wounds.
Damaged pancreatic tissue releases activated pancre-
peritonitis.
Cancer of the Head of the Pancreas and the Bile Duct
Because of the close relation of the head of the pancreas to
the bile duct, cancer of the head of the pancreas often causes
obstructive jaundice.
The Pancreatic Tail and Splenectomy
The presence of the tail of the pancreas in the splenicorenal
ligament sometimes results in its damage during splenectomy.
The damaged pancreas releases enzymes that start to digest
surrounding tissues, with serious consequences.
C L I N I C A L N O T E S
Development of the Pancreas
Basically, congenital fibrocystic disease in the pancreas is
Ectopic pancreatic tissue may be found in the submucosa of the
This opens on the summit
als, the two ducts join and form a common dilatation, the
through the duodenal wall, although in close contact, and open
(Fig. 5.52). In some individuals, they pass separately
wall of the second part of the duodenum to open on the summit of
duct are joined to one another. They pass obliquely through the
As seen from development, the bile duct and the main pancreatic
The inferior part of the head and the uncinate process of the
Continued growth of the entodermal cells of the now-fused
num. The proximal part of the dorsal pancreatic duct may persist
the distal part of the dorsal pancreatic duct. The main pancreatic
is derived from the entire ventral pancreatic duct and
main pan
Fusion also occurs between the ducts, so that the
the left side of the duodenum, results in the ventral bud’s coming
of the stomach and duodenum, together with the rapid growth of
A canalized duct system now develops in each bud. The rotation
bud, close to the junction of the foregut with the midgut (Fig. 5.41).
mesentery. The ventral bud arises in common with the hepatic
short distance above the ventral bud and grows into the dorsal
mal cells that arise from the foregut. The dorsal bud originates a
The pancreas develops from a dorsal and ventral bud of entoder-
into contact with the dorsal bud, and fusion occurs (Fig. 5.59).
-
creatic duct
duct joins the bile duct and enters the second part of the duode-
as an accessory duct, which may or may not open into the duo-
denum about 0.75 in. (2 cm) above the opening of the main duct.
ventral and dorsal pancreatic buds extends into the surround-
ing mesenchyme as columns of cells. These columns give off
side branches, which later become canalized to form collecting
ducts. Secretory acini appear at the ends of the ducts.
The pancreatic islets arise as small buds from the develop-
ing ducts. Later, these cells sever their connection with the duct
system and form isolated groups of cells that start to secrete
insulin and glucagon at about the 5th month.
pancreas are formed from the ventral pancreatic bud; the supe-
rior part of the head, the neck, the body, and the tail of the pan-
creas are formed from the dorsal pancreatic bud (Fig. 5.59).
Entrance of the Bile Duct and Pancreatic Duct
into the Duodenum
the major duodenal papilla, which is surrounded by the sphinc-
ter of Oddi
separately on the summit of the duodenal papilla. In other individu-
hepato-
pancreatic ampulla (ampulla of Vater).
of the duodenal papilla.
Anular Pancreas
In anular pancreas, the ventral pancreatic bud becomes fixed so
that, when the stomach and duodenum rotate, the ventral bud
is pulled around the right side of the duodenum to fuse with the
dorsal bud of the pancreas, thus encircling the duodenum (Fig.
5.60). This may cause obstruction of the duodenum, and vomit-
ing may start a few hours after birth. Early surgical relief of the
obstruction is necessary.
Ectopic Pancreas
stomach, duodenum, small intestine (including Meckel’s diver-
ticulum), and gallbladder, and in the spleen. It is important in that
it may protrude into the lumen of the gut and be responsible for
causing intussusception.
Congenital Fibrocystic Disease
caused by an abnormality in the secretion of mucus. The mucus
produced is excessively viscid and obstructs the pancreatic
duct, which leads to pancreatitis with subsequent fibrosis. The
condition also involves the lungs, kidneys, and liver.
E M B R Y O L O G I C N O T E S

Basic Anatomy
205
dorsal bud
region of rapid growth
ventral bud
bile duct
bile duct
forms main pancreatic duct
forms accessory pancreatic duct
duodenum
duodenum
FIGURE 5.59
The rotation of the duodenum and the unequal growth of the duodenal wall lead to the fusing of the ventral and
dorsal pancreatic buds.
narrowed lumen of duodenum
fixed ventral pancreatic bud
dorsal bud
dorsal pancreatic bud
duodenum
ventral pancreatic bud
FIGURE 5.60
Formation of the anular pancreas, producing duodenal obstruction. Note the narrowing of the duodenum.
9
10
11
splenic
vessels
splenicorenal
ligament
gastrosplenic
omentum
costodiaphragmatic
recess
diaphragm
liver
stomach
transverse colon
left lung
spleen
notched anterior
border
A
B
FIGURE 5.61
Spleen.
Shows relation of spleen to adjacent structures.
It is oval shaped and has a notched anterior border.
A.
B.

206
CHAPTER 5
from the celiac plexus.
The nerves accompany the splenic artery and are derived
Nerve Supply
and then drain into the celiac nodes.
a few lymph nodes along the course of the splenic artery
The lymph vessels emerge from the hilum and pass through
Lymph Drainage
form the portal vein.
creas, the splenic vein joins the superior mesenteric vein to
and the body of the pancreas. Behind the neck of the pan
The splenic vein leaves the hilum and runs behind the tail
Veins
about six branches, which enter the spleen at the hilum.
border of the pancreas. The splenic artery then divides into
artery. It has a tortuous course as it runs along the upper
The large splenic artery is the largest branch of the celiac
Arteries
ribs (Figs. 5.11 and 5.61).
phragmatic recess); left lung; and 9th, 10th, and 11th
The diaphragm; left pleura (left costodia
Posteriorly:
The Abdomen: Part II—The Abdominal Cavity
■
■
-
Blood Supply
-
ment prevent a direct downward enlargement of the organ.
Splenic Enlargement
A pathologically enlarged spleen extends downward and
medially. The left colic flexure and the phrenicocolic liga-
As the enlarged spleen projects below the left costal margin,
its notched anterior border can be recognized by palpation
through the anterior abdominal wall.
The spleen is situated at the beginning of the splenic vein,
and in cases of portal hypertension it often enlarges from
venous congestion.
Trauma to the Spleen
Although anatomically the spleen gives the appearance of
being well protected, automobile accidents of the crushing
or run-over type commonly produce laceration of the spleen.
Penetrating wounds of the lower left thorax can also damage
the spleen.
C L I N I C A L N O T E S
Retroperitoneal Space
two branches of the renal artery, the ureter, and the third
hilum transmits, from the front backward, the renal vein,
The
renal sinus.
hilum extends into a large cavity called the
(Fig. 5.64). The
hilum
of renal substance and is called the
each kidney is a vertical slit that is bounded by thick lips
much as 1 in. (2.5 cm). On the medial concave border of
both kidneys move downward in a vertical direction by as
With contraction of the diaphragm during respiration,
ney because of the large size of the right lobe of the liver.
The right kidney lies slightly lower than the left kid
the costal margin (Fig. 5.63).
side of the vertebral column; they are largely under cover of
toneum high up on the posterior abdominal wall on either
The kidneys are reddish brown and lie behind the peri
urethra.
The urine leaves the body in the
located within the pelvis.
urinary bladder,
to the
ureters
which passes down the
urine,
products leave the kidneys as
maintaining the acid–base balance of the blood. The waste
the water and electrolyte balance within the body and in
ucts of metabolism. They play a major role in controlling
The two kidneys function to excrete most of the waste prod
Location and Description
Urinary Tract
and gonadal blood vessels.
roperitoneal space also contains the ureters and the renal
descending parts of the colon, and the duodenum. The ret
for the suprarenal glands, the kidneys, the ascending and
variable amount of fatty connective tissue that forms a bed
a definite layer of fascia. In front of the fascial layers is a
Each of these muscles is covered on the anterior surface by
muscles and the origin of the transversus abdominis muscle.
medial to lateral by the psoas and quadratus lumborum
The floor or posterior wall of the space is formed from
the iliac crests below (Fig. 5.62).
12th thoracic vertebra and the 12th rib to the sacrum and
wall behind the parietal peritoneum. It extends from the
The retroperitoneal space lies on the posterior abdominal
-
Kidneys
-
-
-
Development of the Spleen
dorsal mesentery (Fig. 5.46). In the earliest stages, the spleen
The spleen develops as a thickening of the mesenchyme in the
consists of a number of mesenchymal masses that later fuse.
The notches along its anterior border are permanent and indi-
cate that the mesenchymal masses never completely fuse.
E M B R Y O L O G I C N O T E S
(continued)
The part of the dorsal mesentery that extends between
hypertrophy after removal of the major spleen and be respon
icorenal ligament. Their clinical importance is that they may
the hilum of the spleen and the greater curvature of the
stomach is called the gastrosplenic omentum; the part that
extends between the spleen and the left kidney on the poste-
rior abdominal wall is called the splenicorenal ligament. The
spleen is supplied by a branch of the foregut artery (celiac
artery), the splenic artery.
Supernumerary Spleen
In 10% of people, one or more supernumerary spleens may be
present, either in the gastrosplenic omentum or in the splen-
-
sible for a recurrence of symptoms of the disease for which
splenectomy was initially performed.