Basic Anatomy
renal
contains the upper expanded end of the ureter, the
The renal sinus, which is the space within the hilum,
medullary rays.
striations known as
ing from the bases of the renal pyramids into the cortex are
Extend
renal columns.
between adjacent pyramids as the
medially (Fig. 5.64). The cortex extends into the medulla
projecting
renal papilla,
toward the cortex and its apex, the
each having its base oriented
renal pyramids,
a dozen
The medulla is composed of about
medulla.
brown inner
and a light
cortex
Each kidney has a dark brown outer
Renal Structure
inal wall.
kidneys and hold them in position on the posterior abdom
The perirenal fat, renal fascia, and pararenal fat support the
toneal fat.
is often in large quantity. It forms part of the retroperi
This lies external to the renal fascia and
Pararenal fat:
with the fascia transversalis.
kidneys and suprarenal glands; it is continuous laterally
sue that lies outside the perirenal fat and encloses the
This is a condensation of connective tis
Renal fascia:
This covers the fibrous capsule.
Perirenal fat:
closely applied to its outer surface.
This surrounds the kidney and is
Fibrous capsule:
The kidneys have the following coverings (Fig. 5.64):
Coverings
pathetic fibers also pass through the hilum.
branch of the renal artery (VAUA). Lymph vessels and sym
207
-
■
■
■
■
■
■
-
■
■
-
-
-
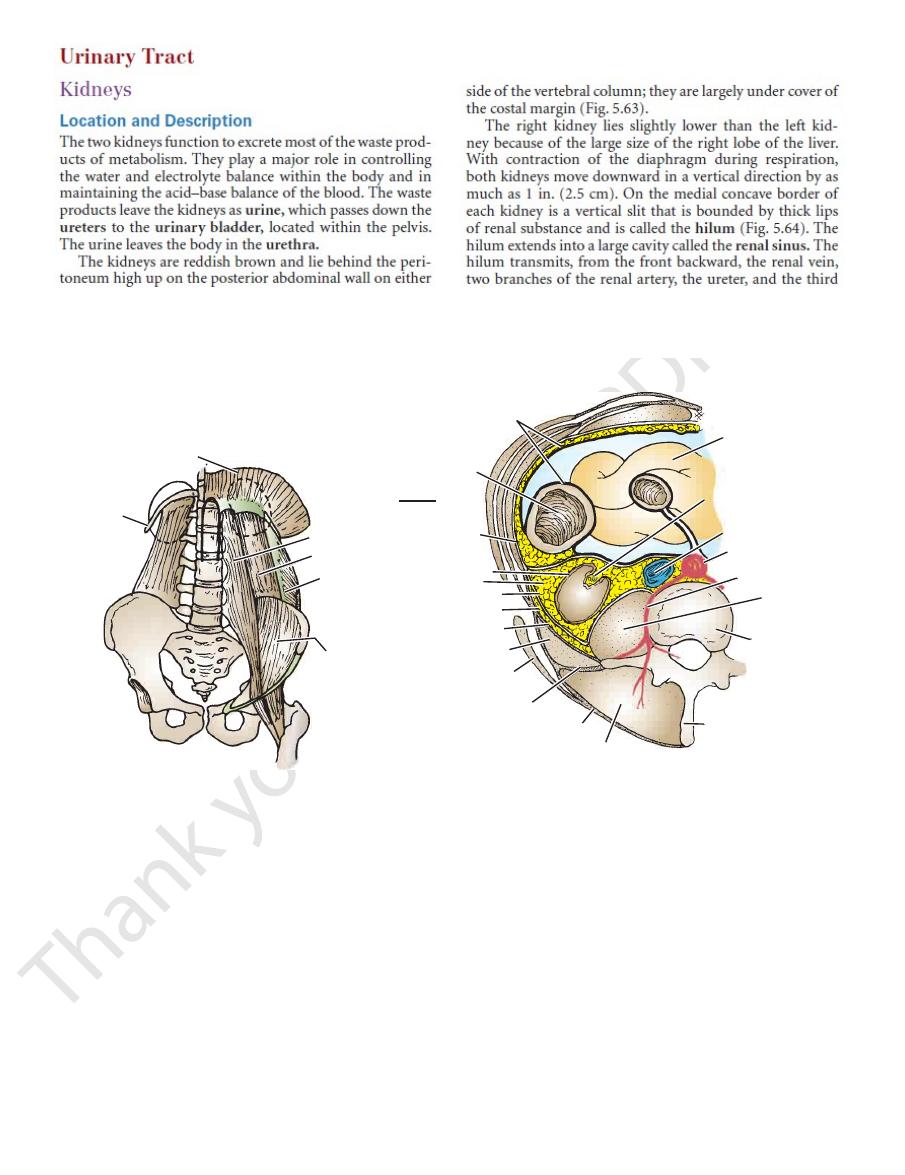
diaphragm
rib 12
iliacus
transversus
abdominis
quadratus
lumborum
psoas
peritoneum
ascending colon
fascia
transversalis
capsule of kidney
perirenal fat
renal fascia
pararenal fat
anterior layer of lumbar fascia
quadratus lumborum
latissimus dorsi
middle layer of lumbar fascia
posterior layer of
lumbar fascia
erector spinae
muscle
spinous process
body of second
lumbar vertebra
psoas
lumbar artery
aorta
inferior vena cava
hilum of right kidney
coils of small
intestine
A
B
RIGHT
FIGURE 5.62
Retroperitoneal space.
verse section of the posterior abdominal wall showing structures in the retroperitoneal space as seen from below.
Trans
Structures present on the posterior abdominal wall behind the peritoneum.
A.
B.
-
Trauma to Organs in the Retroperitoneal Space
(the peritoneum forms the anterior boundary of the space; Fig.
Palpation of the anterior abdominal wall in the lumbar and iliac
regions may give rise to signs indicative of peritoneal irritation
5.62). In other words, tenderness and muscle spasm (rigidity)
may be present. Palpation of the back in the interval between the
12th rib and the vertebral column may reveal tenderness sugges-
tive of kidney disease.
Abdominal radiographs may reveal air in the extraperito-
neal tissues, indicating perforation of a viscus (e.g., ascending
or descending colon). CT scans can often accurately define the
extent of the injury to the extraperitoneal organs.
Abscess Formation
Infection originating in retroperitoneal organs, such as the kid-
neys, lymph nodes, and retrocecal appendix, may extend widely
into the retroperitoneal space.
Leaking Aortic Aneurysm
The blood may first be confined to the retroperitoneal space
before rupturing into the peritoneal cavity.
C L I N I C A L N O T E S
208
CHAPTER 5
artery and drains into the inferior vena cava.
The renal vein emerges from the hilum in front of the renal
Veins
lobular arteries.
arise as branches of the inter
ent glomerular arterioles
affer
that ascend in the cortex. The
interlobular arteries
pyramids (Fig. 5.65). The arcuate arteries give off several
which arch over the bases of the
arcuate arteries,
off the
of the cortex and the medulla, the interlobar arteries give
cortex on each side of the renal pyramid. At the junction
(Fig. 5.64). The interlobar arteries run toward the
arteries
interlobar
stance, each lobar artery gives off two or three
one for each renal pyramid. Before entering the renal sub
arise from each segmental artery,
Lobar arteries
kidney.
They are distributed to different segments or areas of the
that enter the hilum of the kidney.
segmental arteries
five
2nd lumbar vertebra. Each renal artery usually divides into
The renal artery arises from the aorta at the level of the
Arteries
layers of peritoneum. For details, see Figure 5.65.
with the kidneys, whereas others are separated by visceral
Note that many of the structures are directly in contact
ward and laterally (Fig. 5.34).
iliohypogastric, and ilioinguinal nerves (L1) run down
transversus abdominis muscles. The subcostal (T12),
and 12th ribs; and the psoas, quadratus lumborum, and
recess of the pleura; the 11th (the left kidney is higher)
The diaphragm; the costodiaphragmatic
Posteriorly:
num (Figs. 5.4 and 5.65)
ach, the pancreas, the left colic flexure, and coils of jeju
The suprarenal gland, the spleen, the stom
Anteriorly:
Important Relations, Left Kidney
(L1) run downward and laterally (Fig. 5.34).
subcostal (T12), iliohypogastric, and ilioinguinal nerves
tus lumborum, and transversus abdominis muscles. The
recess of the pleura; the 12th rib; and the psoas, quadra
The diaphragm; the costodiaphragmatic
Posteriorly:
part of the duodenum, and the right colic flexure (Figs.
The suprarenal gland, the liver, the second
Anteriorly:
Important Relations, Right Kidney
renal papilla.
mid, the
Each minor calyx is indented by the apex of the renal pyra
(Fig. 5.64).
minor calyces
which divides into two or three
each of
major calyces,
This divides into two or three
pelvis.
The Abdomen: Part II—The Abdominal Cavity
-
■
■
5.4 and 5.65).
■
■
-
■
■
-
-
■
■
-
Blood Supply
-
-
-
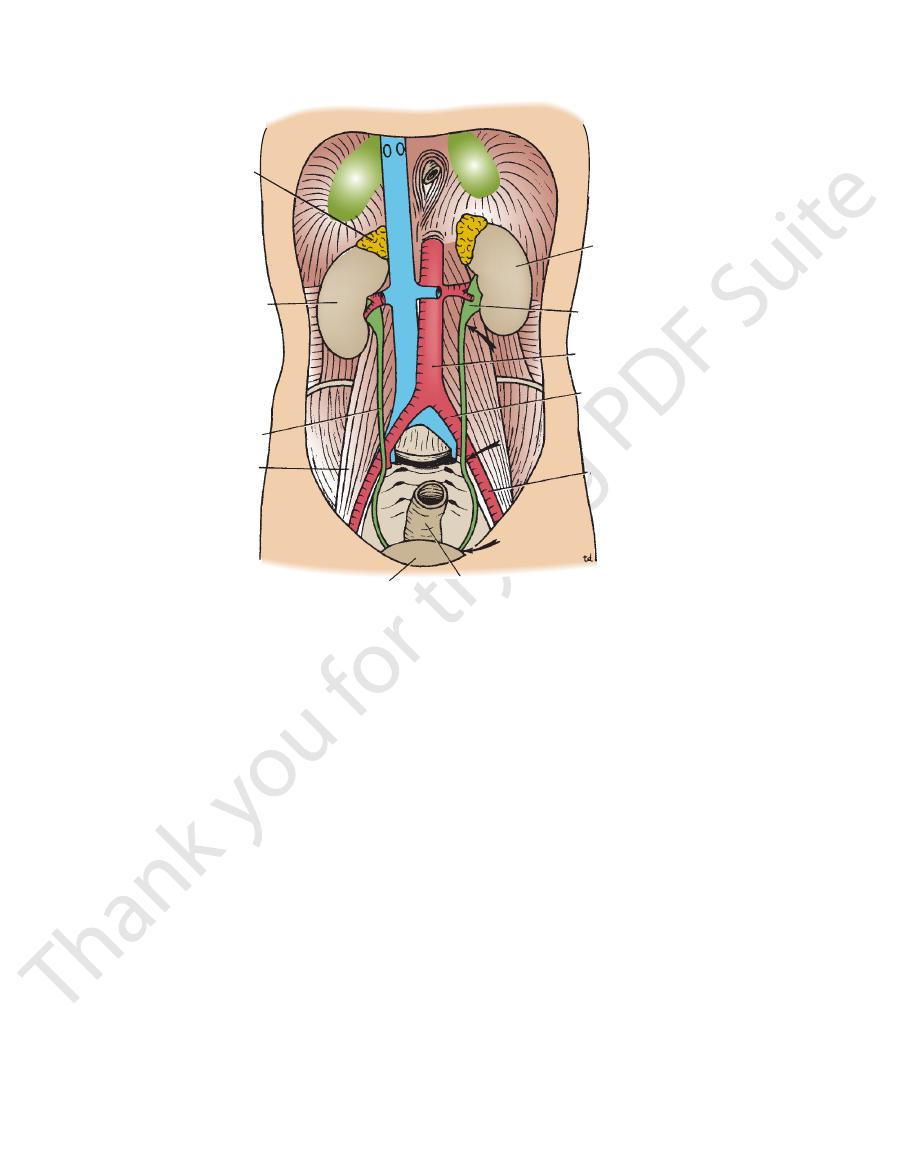
right kidney
right ureter
psoas
rectum
external iliac artery
common iliac artery
aorta
renal pelvis
left kidney
suprarenal
gland
urinary bladder
FIGURE 5.63
Posterior abdominal wall showing the kidneys and the ureters in situ.
ureter is narrowed.
Arrows indicate three sites where the
Basic Anatomy
pressure of the glomeruli.
contractions of the muscle coat, assisted by the filtration
5.63). The urine is propelled along the ureter by peristaltic
kidneys to the posterior surface of the urinary bladder (Fig.
The two ureters are muscular tubes that extend from the
Location and Description
nal cord in the 10th, 11th, and 12th thoracic nerves.
ent fibers that travel through the renal plexus enter the spi
The nerve supply is the renal sympathetic plexus. The affer
Nerve Supply
origin of the renal artery.
Lymph drains to the lateral aortic lymph nodes around the
Lymph Drainage
209
-
-
Ureter
perirenal fat
renal fascia
pararenal fat
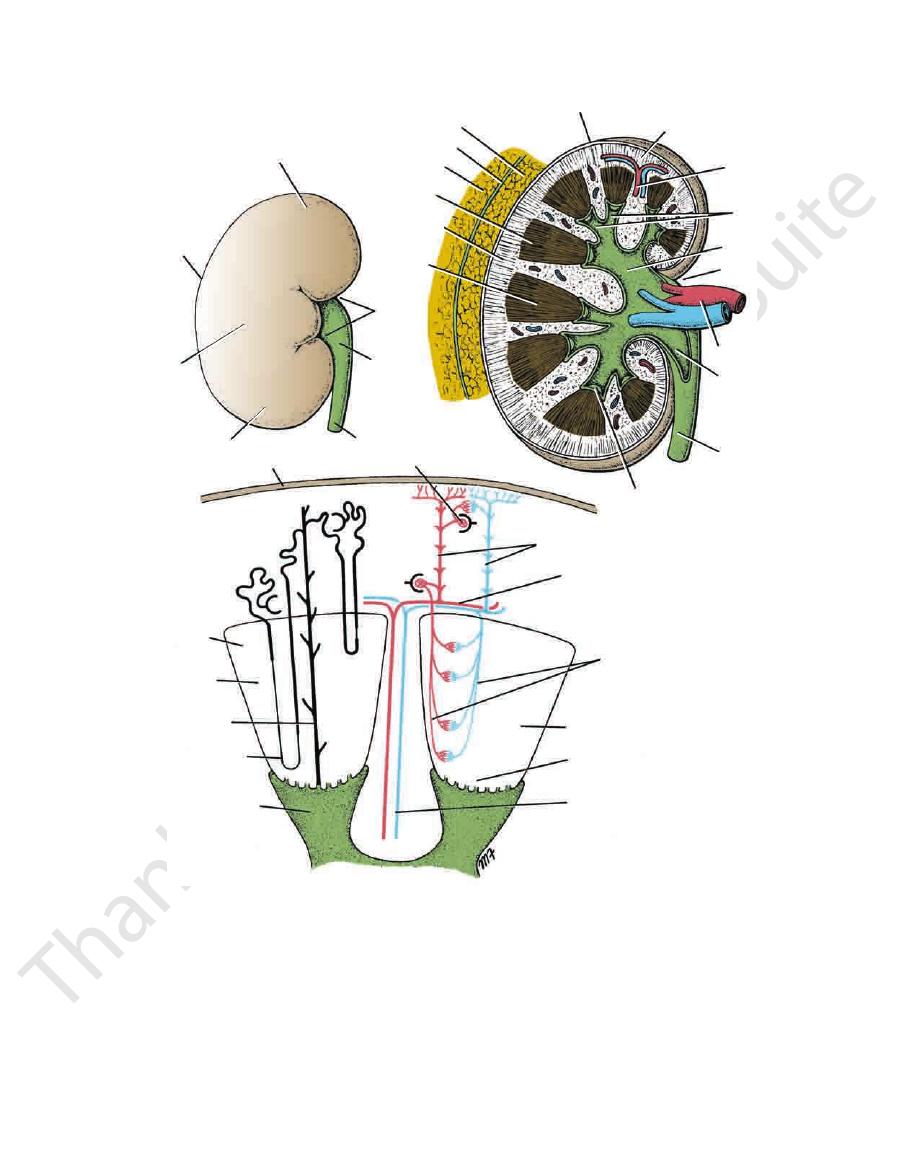
medulla
medullary rays
pyramid
renal papilla
ureter
pelvis
of kidney
renal vessels
hilum
major calyx
minor
calyces
interlobar
artery
and vein
cortex
capsule
superior pole
lateral
border
anterior
surface
inferior pole
ureter
pelvis
of kidney
hilum
cortex
pyramid
collecting
tubule
loop of Henle
interlobular artery and vein
acuate artery and vein
vasa recta
pyramid
renal papilla
major calyx
A
B
C
capsule
glomerulus
interlobar artery and vein
minor calyx
medulla
FIGURE 5.64
sels within the kidney.
Section of the kidney showing the position of the nephrons and the arrangement of the blood ves
papillae, and calyces.
Right kidney, coronal section showing the cortex, medulla, pyramids, renal
Right kidney, anterior surface.
A.
B.
C.
-
210
CHAPTER 5
The Abdomen: Part II—The Abdominal Cavity
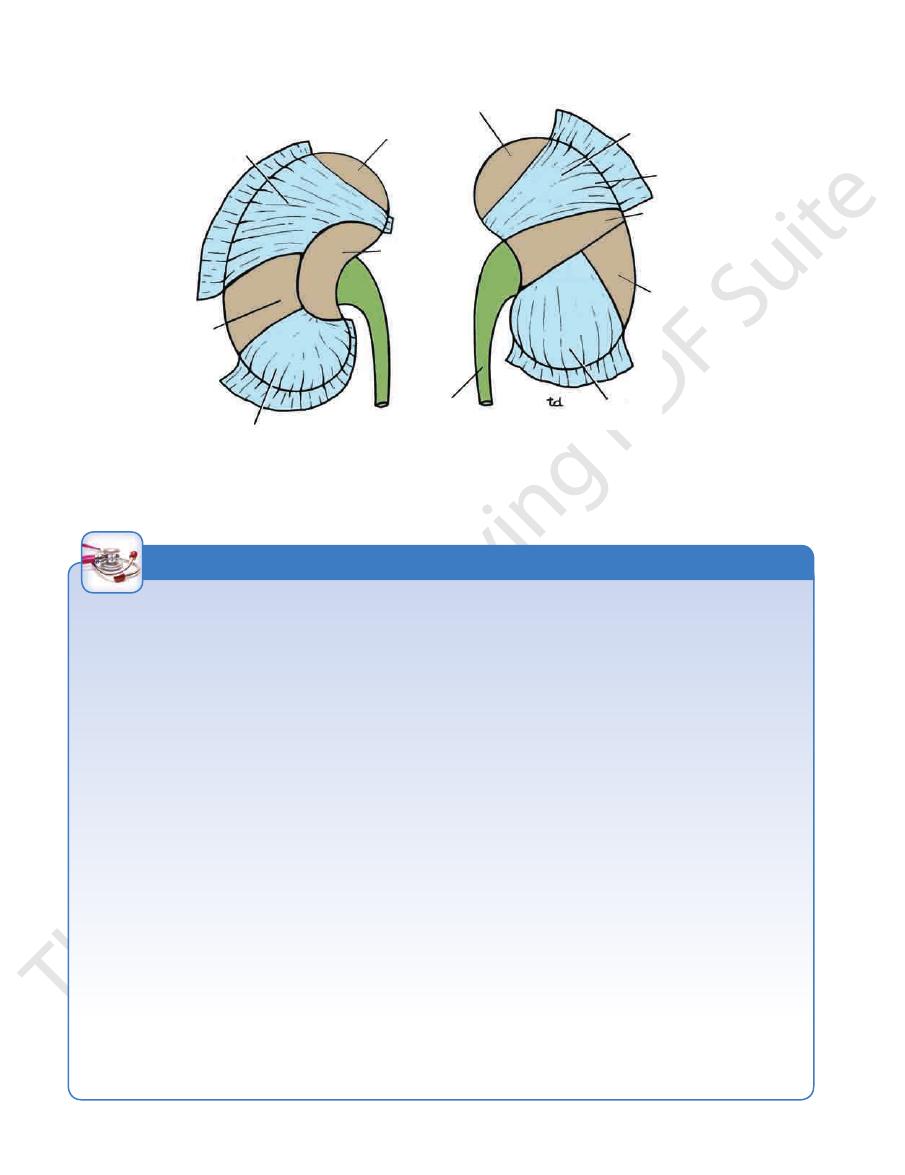
right suprarenal gland
liver
colon
duodenum
left suprarenal gland
stomach
colon
small intestine
ureter
pancreas
spleen
small intestine
FIGURE 5.65
isceral peritoneum covering the kidneys has been left in position. Brown
Anterior relations of both kidneys. V
areas indicate where the kidney is in direct contact with the adjacent viscera.
Renal Mobility
Anastomosis of the branches of the internal iliac arteries on the
is anastomosed end to side to the external iliac vein (Fig. 5.67).
the distribution of the subcostal nerve (T12) to the flank and the
spinal cord at the level of T12. Pain is commonly referred along
nerve in the thorax and the sympathetic trunk. They enter the
and ascend to the spinal cord through the lowest splanchnic
fibers pass through the renal plexus around the renal artery
of the smooth muscle in the renal pelvis. The afferent nerve
pain can result from stretching of the kidney capsule or spasm
that may radiate downward into the lower abdomen. Renal
Renal pain varies from a dull ache to a severe pain in the flank
stab wounds or gunshot wounds and often involve other viscera.
eration of the organ. Penetrating injuries are usually caused by
undisturbed because the latter occupies a separate compart
abdominal musculature. Should the amount of perirenal fat be
and the lower pole may be palpated in the right lumbar region
abdominal pressure and by their connections with the perirenal
The kidneys are maintained in their normal position by intra-
fat and renal fascia. Each kidney moves slightly with respiration.
The right kidney lies at a slightly lower level than the left kidney,
at the end of deep inspiration in a person with poorly developed
reduced, the mobility of the kidney may become excessive and
produce symptoms of renal colic caused by kinking of the ure-
ter. Excessive mobility of the kidney leaves the suprarenal gland
-
ment in the renal fascia.
Kidney Trauma
The kidneys are well protected by the lower ribs, the lumbar
muscles, and the vertebral column. However, a severe blunt
injury applied to the abdomen may crush the kidney against the
last rib and the vertebral column. Depending on the severity of
the blow, the injury varies from a mild bruising to a complete lac-
Because 25% of the cardiac outflow passes through the kidneys,
renal injury can result in rapid blood loss. A summary of the inju-
ries to the kidneys is shown in Figure 5.66.
Kidney Tumors
Malignant tumors of the kidney have a strong tendency to spread
along the renal vein. The left renal vein receives the left testicular
vein in the male, and this may rarely become blocked, producing
left-sided varicocele (see page 132).
Renal Pain
anterior abdominal wall.
Transplanted Kidneys
The iliac fossa on the posterior abdominal wall is the usual site
chosen for transplantation of the kidney. The fossa is exposed
through an incision in the anterior abdominal wall just above the
inguinal ligament. The iliac fossa in front of the iliacus muscle is
approached retroperitoneally. The kidney is positioned and the
vascular anastomosis constructed. The renal artery is anasto-
mosed end to end to the internal iliac artery and the renal vein
two sides is sufficient so that the pelvic viscera on the side of
the renal arterial anastomosis are not at risk. Ureterocystostomy
is then performed by opening the bladder and providing a wide
entrance of the ureter through the bladder wall.
C L I N I C A L N O T E S
Basic Anatomy
of the small intestine (Fig. 5.27)
ticular or ovarian vessels, and the root of the mesentery
ileum, the right colic and ileocolic vessels, the right tes
The duodenum, the terminal part of the
Anteriorly:
Relations, Right Ureter
detail on pages 269 and 278.
the bladder. The pelvic course of the ureter is described in
ischial spine and turns forward to enter the lateral angle of
runs down the lateral wall of the pelvis to the region of the
in front of the sacroiliac joint (Fig. 5.63). The ureter then
vis by crossing the bifurcation of the common iliac artery
verse processes of the lumbar vertebrae. It enters the pel
psoas muscle, which separates it from the tips of the trans
behind the parietal peritoneum (adherent to it) on the
from the hilum of the kidney and runs vertically downward
receives the major calyces (Fig. 5.64). The ureter emerges
end of the ureter. It lies within the hilum of the kidney and
The renal pelvis is the funnel-shaped expanded upper
and where it pierces the bladder wall (Fig. 5.63).
the ureter, where it is kinked as it crosses the pelvic brim,
constrictions along its course: where the renal pelvis joins
resembles the esophagus (also 10 in. long) in having three
Each ureter measures about 10 in. (25 cm) long and
211
-
-
■
■
-
A
B
C
D
E
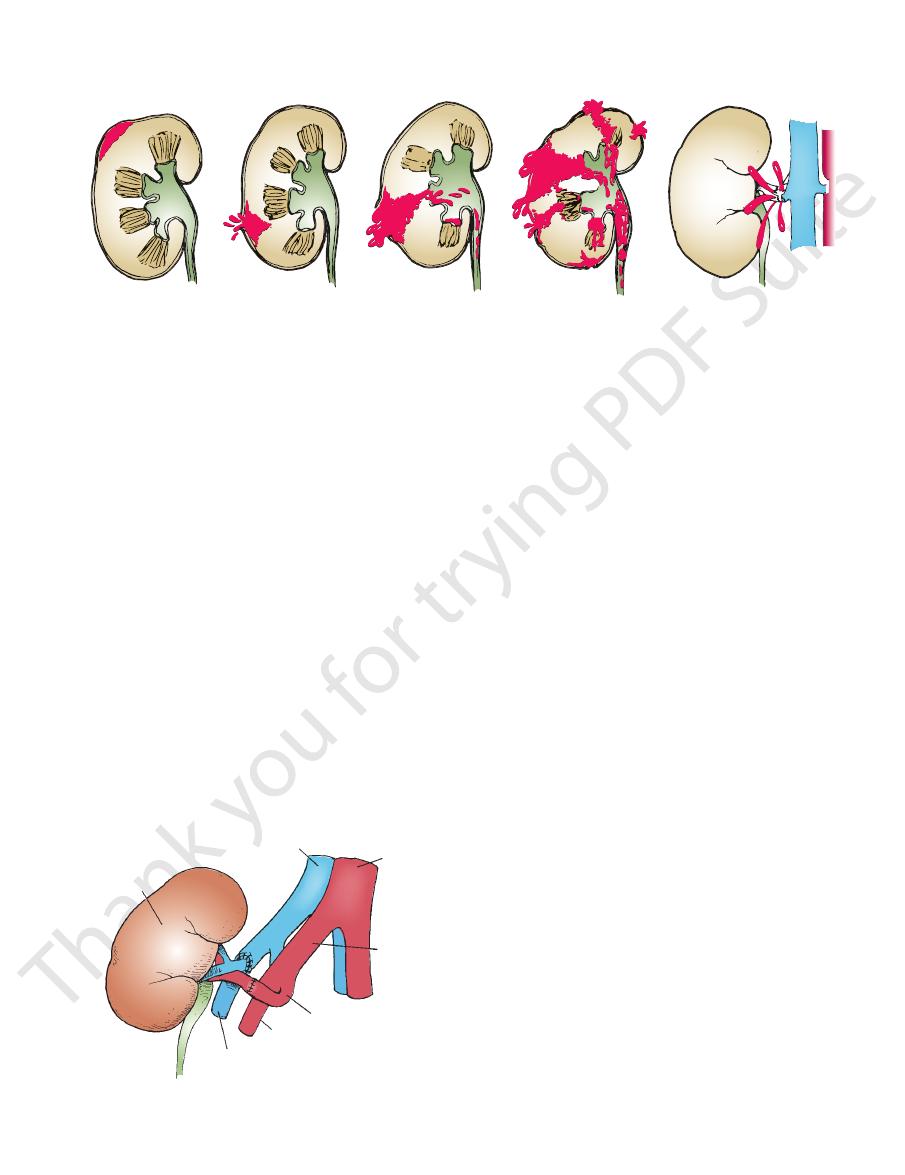
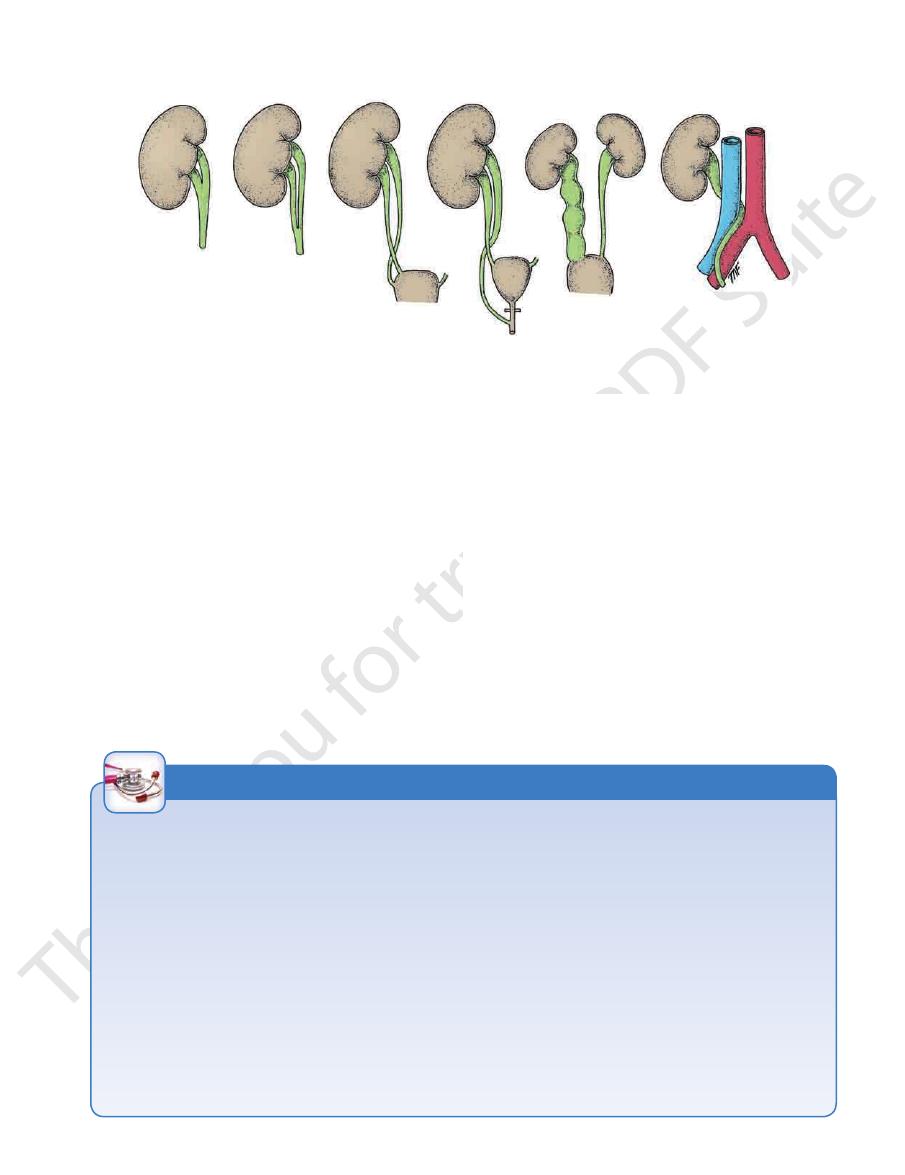
FIGURE 5.66
Injuries to the kidney.
the renal pedicle involving the renal vessels and possibly the renal pelvis.
Injury to
tion of blood and urine into the perirenal and pararenal fat; blood also enters the calyces and appears in the urine.
Shattered kidney with extensive hemorrhage and extravasa
the perirenal and pararenal fat and into the peritoneal cavity.
the medulla. Note the escape of blood into the calyces and therefore the urine. Urine as well as blood may extravasate into
Tearing of the capsule, the cortex, and
Tearing of the capsule and cortex with bleeding occurring into the perirenal fat.
Contusion, with hemorrhage confined to the cortex beneath the intact fibrous capsule.
A.
B.
C.
D.
-
E.
inferior vena cava
abdominal
aorta
common iliac
artery
internal iliac artery
external iliac artery
external iliac vein
transplanted
kidney
FIGURE 5.67
The transplanted kidney.
are surrounded by renal fascia (but are separated from the
organs that lie on the upper poles of the kidneys. They
The two suprarenal glands are yellowish retroperitoneal
1st and 2nd lumbar segments.
with the sympathetic nerves and enter the spinal cord in the
hypogastric plexuses (in the pelvis). Afferent fibers travel
The nerve supply is the renal, testicular (or ovarian), and
Nerve Supply
nodes.
The lymph drains to the lateral aortic nodes and the iliac
Lymph Drainage
arteries.
Venous blood drains into veins that correspond to the
Veins
artery; and in the pelvis, the superior vesical artery.
the renal artery; middle portion, the testicular or ovarian
The arterial supply to the ureter is as follows: upper end,
Arteries
the left ureter (Fig. 5.27).
The inferior mesenteric vein lies along the medial side of
tion of the left common iliac artery (Fig. 5.63)
from the lumbar transverse processes, and the bifurca
The left psoas muscle, which separates it
Posteriorly:
sels (Figs. 5.13 and 5.27)
the left colic vessels, and the left testicular or ovarian ves
The sigmoid colon and sigmoid mesocolon,
Anteriorly:
Relations, Left Ureter
tion of the right common iliac artery (Fig. 5.63)
from the lumbar transverse processes, and the bifurca
The right psoas muscle, which separates it
Posteriorly:
■
■
-
■
■
-
■
■
-
Blood Supply
Suprarenal Glands
Location and Description
212
CHAPTER 5
The Abdomen: Part II—The Abdominal Cavity
Traumatic Ureteral Injuries
at a lower level and is often referred to the testis or the tip of the
strong peristaltic waves of contraction pass down the ureter in
spinal cord at segments T11 and 12 and L1 and 2. In renal colic,
processes of the lumbar vertebrae, crosses the region of the
essary. The ureter runs down in front of the tips of the transverse
stones may be arrested, namely, the pelviureteral junction,
into the retroperitoneal tissues on the posterior abdominal
the ureters are retroperitoneal in position, urine may escape
and, in a few individuals, penetrating stab wounds. Because
ureter are rare. Most injuries are caused by gunshot wounds
Because of its protected position and small size, injuries to the
wall.
Ureteric Stones
There are three sites of anatomic narrowing of the ureter where
the pelvic brim, and where the ureter enters the bladder. Most
stones, although radiopaque, are small enough to be impossible
to see definitely along the course of the ureter on plain radio-
graphic examination. An intravenous pyelogram is usually nec-
sacroiliac joint, swings out to the ischial spine, and then turns
medially to the bladder.
Renal Colic
The renal pelvis and the ureter send their afferent nerves into the
an attempt to pass the stone onward. The spasm of the smooth
muscle causes an agonizing colicky pain, which is referred to
the skin areas that are supplied by these segments of the spinal
cord, namely, the flank, loin, and groin.
When a stone enters the low part of the ureter, the pain is felt
penis in the male and the labium majus in the female. Sometimes,
ureteral pain is referred along the femoral branch of the genito-
femoral nerve (L1 and 2) so that pain is experienced in the front of
the thigh. The pain is often so severe that afferent pain impulses
spread within the central nervous system, giving rise to nausea.
C L I N I C A L N O T E S
Development of the Kidneys and Ureters
urinary stasis, which may result in infection and stone formation.
come to rest in the low lumbar region. Both ureters are kinked
trapped behind the inferior mesenteric artery so that the kidneys
ascend from the pelvis, but the interconnecting bridge becomes
mal ascent; it usually is found at the brim of the pelvis (Fig. 5.70).
aorta. The kidneys reach their final position opposite the 2nd
its blood supply from the pelvic continuation of the aorta, the
The developing kidney is initially a pelvic organ and receives
The metanephrogenic cap condenses around the ureteric bud
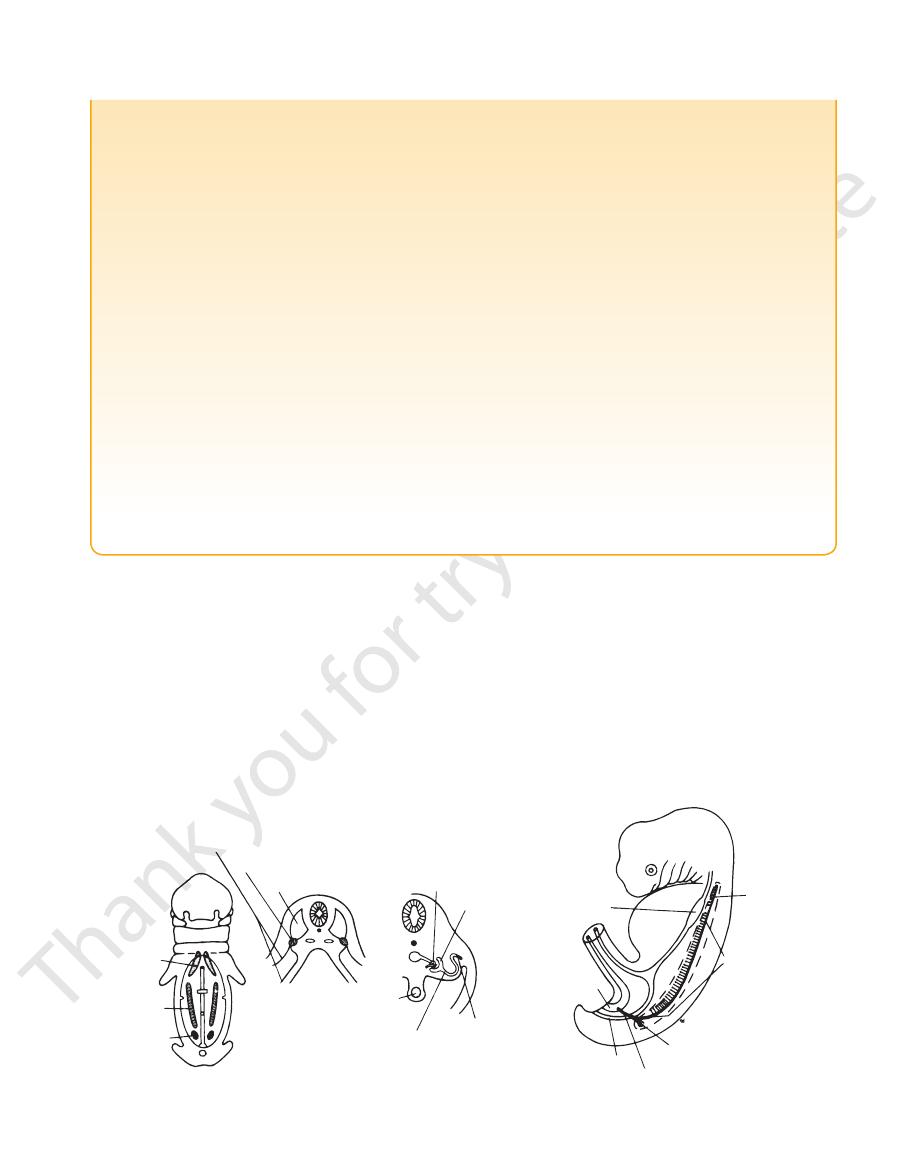
Three sets of structures in the urinary system appear, called
the pronephros, mesonephros, and metanephros. In the human,
the metanephros is responsible for the permanent kidney. The
metanephros develops from two sources: the ureteric bud from
the mesonephric duct and the metanephrogenic cap from the
intermediate cell mass of mesenchyme of the lower lumbar and
sacral regions.
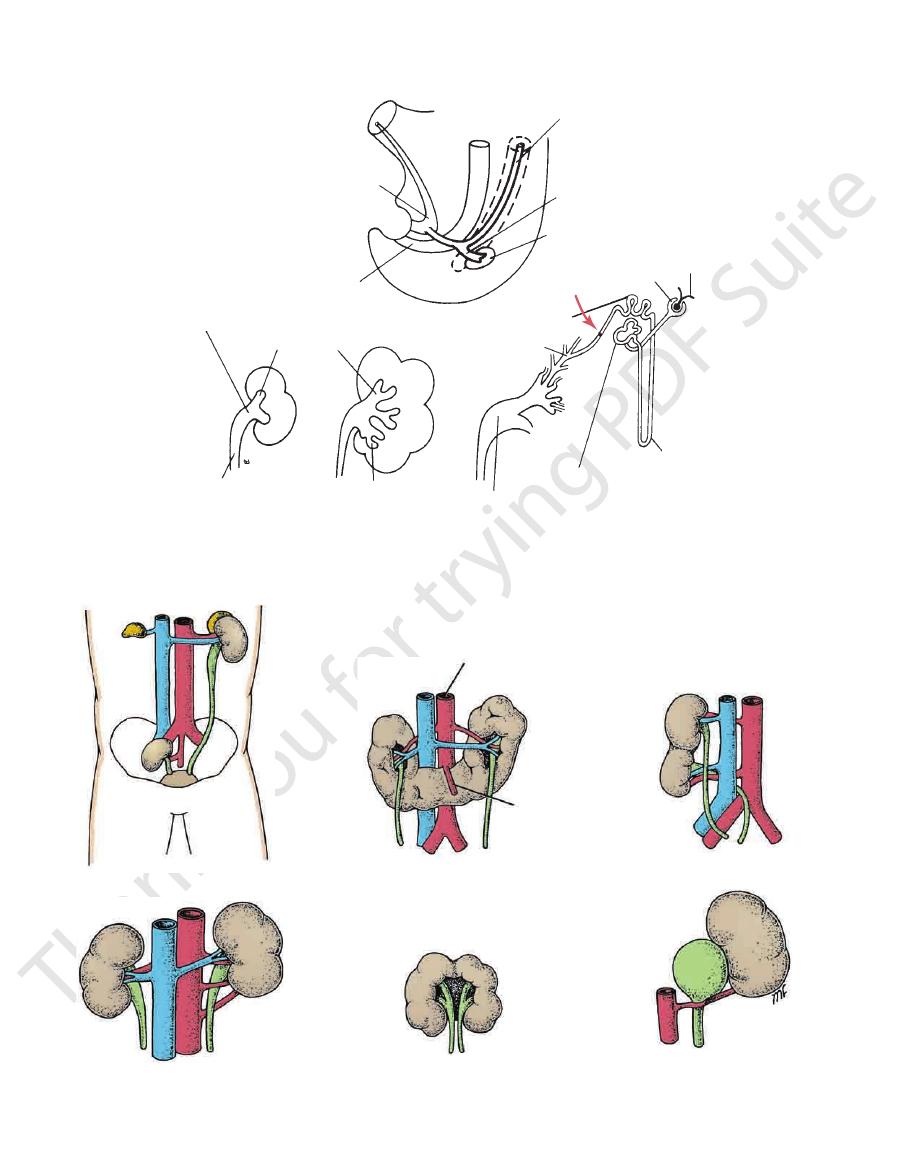
Ureteric Bud
The ureteric bud arises as an outgrowth of the mesonephric duct
(Figs. 5.68 and 5.69). It forms the ureter, which dilates at its upper
end to form the pelvis of the ureter. The pelvis later gives off
branches that form the major calyces, and these in turn divide
and branch to form the minor calyces and the collecting tubules.
Metanephrogenic Cap
(Fig. 5.69) and forms the glomerular capsules, the proximal and
distal convoluted tubules, and the loops of Henle. The glomeru-
lar capsule becomes invaginated by a cluster of capillaries that
form the glomerulus. Each distal convoluted tubule formed from
the metanephrogenic cap tissue becomes joined to a collecting
tubule derived from the ureteric bud. The surface of the kidney
is lobulated at first, but after birth, this lobulation usually soon
disappears.
middle sacral artery. Later, the kidneys “ascend” up the poste-
rior abdominal wall. This so-called ascent is caused mainly by
the growth of the body in the lumbar and sacral regions and by
the straightening of its curvature. The ureter elongates as the
ascent continues.
The kidney is vascularized at successively higher levels by
successively higher lateral splanchnic arteries, branches of the
lumbar vertebra. Because of the large size of the right lobe of
the liver, the right kidney lies at a slightly lower level than the
left kidney.
Polycystic Kidney
A hereditary disease, polycystic kidneys can be transmitted by
either parent. It may be associated with congenital cysts of the
liver, pancreas, and lung. Both kidneys are enormously enlarged
and riddled with cysts. Polycystic kidney is thought to be caused
by a failure of union between the developing convoluted tubules
and collecting tubules. The accumulation of urine in the proximal
tubules results in the formation of retention cysts.
Pelvic Kidney
In pelvic kidney, the kidney is arrested in some part of its nor-
Such a kidney may present with no signs or symptoms and may
function normally. However, should an ectopic kidney become
inflamed, it may—because of its unusual position—give rise to
a mistaken diagnosis.
Horseshoe Kidney
When the caudal ends of both kidneys fuse as they develop, the
result is horseshoe kidney (Fig. 5.70). Both kidneys commence to
as they pass inferiorly over the bridge of renal tissue, producing
Surgical division of the bridge corrects the condition.
E M B R Y O L O G I C N O T E S
(continued)
Basic Anatomy
213
Unilateral Double Kidney
the urinary stasis, the ureter is prone to infection. Plastic surgery
absence of motility (Fig. 5.71). The cause is unknown. Because of
more liable to become infected or to be the seat of calculus for
chance on radiologic investigation of the urinary tract. They are
ureter crosses its fellow and may produce urinary obstruction. The
independently into the bladder (Fig. 5.71). In the latter case, one
may open through a common orifice into the bladder, or may open
In bifid ureter, the ureters may join in the lower third of their course,
outflow of urine, producing dilatation of the calyces and pelvis, a
Both kidneys may fuse together at their hila, and they usually
fuses with the lower pole of the normally placed kidney (Fig.
blood vessels. In unilateral double kidney, the ureteric bud on
The kidney on one side may be double, with separate ureters and
one side crosses the midline as it ascends, and its upper pole
5.70). Here again, angulation of the ureter may result in stasis of
the urine and may require surgical treatment.
Rosette Kidney
remain in the pelvis. The two kidneys together form a rosette
(Fig. 5.70). This is the result of the early fusion of the two ureteric
buds in the pelvis.
Supernumerary Renal Arteries
Supernumerary renal arteries are relatively common. They rep-
resent persistent fetal renal arteries, which grow in sequence
from the aorta to supply the kidney as it ascends from the pelvis.
Their occurrence is clinically important because a supernumer-
ary artery may cross the pelviureteral junction and obstruct the
condition known as hydronephrosis (Fig. 5.70).
Double Pelvis
Double pelvis of the ureter is usually unilateral (Fig. 5.71). The
upper pelvis is small and drains the upper group of calyces;
the larger lower pelvis drains the middle and lower groups of
calyces. The cause is a premature division of the ureteric bud
near its termination.
Bifid Ureter
cause of bifid ureter is a premature division of the ureteric bud.
Cases of double pelvis and double ureters may be found by
-
mation than a normal ureter.
Megaloureter
Megaloureter may be unilateral or bilateral and shows complete
is required to improve the rate of drainage.
Postcaval Ureter
The right ureter may ascend posterior to the inferior vena cava
and may be obstructed by it (Fig. 5.71). Surgical rerouting of the
ureter with reimplantation of the distal end into the bladder is the
treatment of choice.
pronephros
mesonephros
metanephros
lateral cell mass
intermediate cell mass
paraxial cell mass
glomerular
capsule
glomerulus
mesonephric
duct
gut
mesonephric tubule
stomach
pronephros
mesonephros
metanephros
mesonephric duct
rectum
anterior part of
the cloaca
FIGURE 5.68
The origins and positions of the pronephros, mesonephros, and metanephros.
on the diaphragm.
creas, the lesser sac, and the stomach and rests posteriorly
upper pole to the hilus (Fig. 5.4). It lies behind the pan
extends along the medial border of the left kidney from the
is crescentic in shape and
left suprarenal gland
The
diaphragm.
behind the inferior vena cava. It rests posteriorly on the
behind the right lobe of the liver and extends medially
caps the upper pole of the right kidney (Fig. 5.4). It lies
is pyramid shaped and
right suprarenal gland
The
norepinephrine.
epinephrine
the catecholamines
the sex organs. The medulla of the suprarenal glands secretes
which probably play a role in the prepubertal development of
sex hormones,
drates, fats, and proteins; and small amounts of
are concerned with the control of the metabolism of carbohy
which
glucocorticoids,
trol of fluid and electrolyte balance;
which are concerned with the con
mineral corticoids,
include
The cortex of the suprarenal glands secretes hormones that
medulla.
and a dark brown
cortex
kidneys by the perirenal fat). Each gland has a yellow
-
-
and
-
214
CHAPTER 5
The Abdomen: Part II—The Abdominal Cavity
anterior part of cloaca
rectum
mesonephric duct
ureteric bud
metanephrogenic cap
glomerulus
glomerular capsule
distal convoluted tubule
collecting tubules
Henle's loop
proximal convoluted tubule
pelvis of ureter
pelvis of ureter
major calyx
ureter
minor calyx
FIGURE 5.69
The origin of the ureteric bud from the mesonephric duct and the formation of the major and minor calyces and
indicates the point of union between the collecting tubules and the convoluted tubules.
Arrow
the collecting tubules.
pelvic kidney
unilateral double kidney
rosette kidney (cake kidney)
aorta
horseshoe kidney
aberrant renal arteries
aberrant renal artery causing
urinary obstruction
inferior
mesenteric
FIGURE 5.70
Some common congenital anomalies of the kidney.
Basic Anatomy
medulla of the gland.
nic nerves supply the glands. Most of the nerves end in the
Preganglionic sympathetic fibers derived from the splanch
The lymph drains into the lateral aortic nodes.
Lymph Drainage
renal vein on the left.
drains into the inferior vena cava on the right and into the
A single vein emerges from the hilum of each gland and
Veins
inferior phrenic artery, aorta, and renal artery.
The arteries supplying each gland are three in number:
Arteries
215
Blood Supply
Nerve Supply
-
postcaval ureter
double pelvis
bifid ureter
bifid ureter
ectopic ureteric orifice
megaloureter
FIGURE 5.71
Some common congenital anomalies of the ureter.
rior mesenteric artery, and inferior mesenteric artery
Three anterior visceral branches: the celiac artery, supe
Branches
Figure 5.73.
The surface markings of the aorta are shown in
azygos vein. On its left side lies the left sympathetic trunk.
rior vena cava, the cisterna chyli, and the beginning of the
mon iliac arteries (Fig. 5.72). On its right side lie the infe
of the 4th lumbar vertebra, it divides into the two com
surface of the bodies of the lumbar vertebrae. At the level
5.72). It descends behind the peritoneum on the anterior
of the diaphragm in front of the 12th thoracic vertebra (Fig.
The aorta enters the abdomen through the aortic opening
Location and Description
Wall
Arteries on the Posterior Abdominal
Aorta
-
-
■
■
-
Cushing’s Syndrome
The suprarenal glands, together with the kidneys, are enclosed
close relationship of the suprarenal glands to the crura of the
ment; however, when interpreting CT scans, remember the
wall, few tumors of the suprarenal glands can be palpated.
Because of their position on the posterior abdominal
Adrenocortical insufficiency (Addison’s disease), which is
ism), and hypertension; if the syndrome occurs later in life, it may
Suprarenal cortical hyperplasia is the most common cause of
Cushing’s syndrome, the clinical manifestations of which include
moon-shaped face, truncal obesity, abnormal hairiness (hirsut-
result from an adenoma or carcinoma of the cortex.
Addison’s Disease
characterized clinically by increased pigmentation, muscular
weakness, weight loss, and hypotension, may be caused by
tuberculous destruction or bilateral atrophy of both cortices.
Pheochromocytoma
Pheochromocytoma, a tumor of the medulla, produces a parox-
ysmal or sustained hypertension. The symptoms and signs result
from the production of a large amount of catecholamines, which
are then poured into the bloodstream.
CT scans can be used to visualize the glandular enlarge-
diaphragm.
Surgical Significance of the Renal Fascia
within the renal fascia; the suprarenal glands, however, lie in a
separate compartment, which allows the two organs to be sepa-
rated easily at operation.
C L I N I C A L N O T E S