
the normal human being averages about 25 mm Hg, and the diastolic pressure
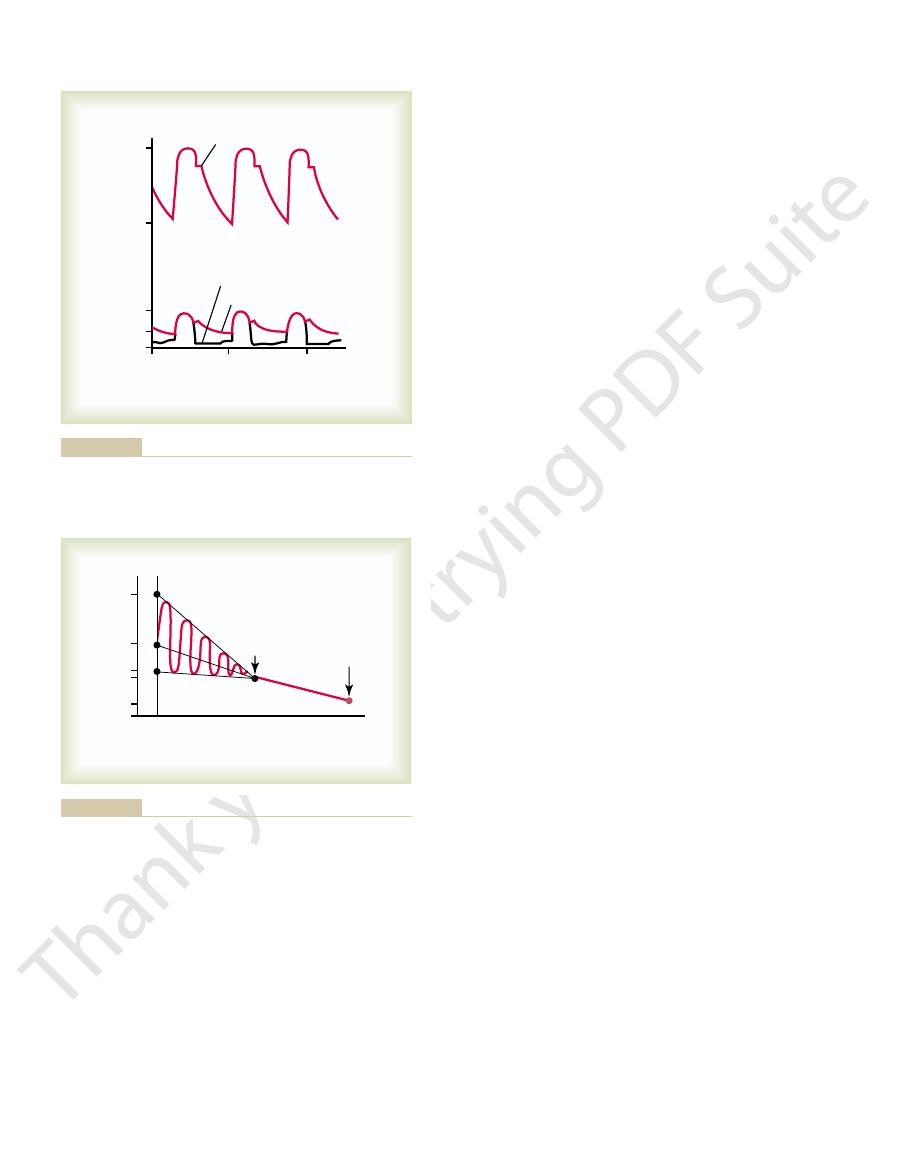
in the upper portion of the figure. The systolic pressure in the right ventricle of
These curves are contrasted with the much higher aortic pressure curve shown
ventricle and pulmonary artery are shown in the lower portion of Figure 38–1.
The pressure pulse curves of the right
Pressure Pulse Curve in the Right Ventricle.
Pressures in the Pulmonary System
tissues, thereby helping to prevent pulmonary edema.
Particulate matter entering the alveoli is partly removed by way of these channels,
right thoracic lymph duct
ing to the hilum of the lung, and thence mainly into the
ning in the connective tissue spaces that surround the terminal bronchioles, cours-
Lymph vessels are present in all the supportive tissues of the lung, begin-
Lymphatics.
than passing back to the right atrium. Therefore, the flow into the left atrium and
porting tissues, it empties into the pulmonary veins and
small bronchi. After this bronchial and arterial blood has passed through the sup-
porting tissues of the lungs, including the connective tissue, septa, and large and
to the partially deoxygenated blood in the pulmonary arteries. It supplies the sup-
blood, in contrast
oxygenated
total cardiac output. This bronchial arterial blood is
originate from the systemic circulation, amounting to about 1 to 2 per cent of the
Bronchial Vessels.
ately empty their effluent blood into the left atrium, to be pumped by the left heart
The pulmonary veins, like the pulmonary arteries, are also short. They immedi-
right ventricle.
which is similar to that of the entire systemic arterial tree. This large compliance
averaging almost 7 ml/mm Hg,
large compliance,
temic arteries. This, combined with the fact that the vessels are thin and distensible,
the smaller arteries and arterioles, have larger diameters than their counterpart sys-
The pulmonary arterial branches are very short, and all the pulmonary arteries, even
The pulmonary artery is thin, with a wall thickness one third that of the aorta.
blood to the two respective lungs.
The pulmonary artery extends only 5 centimeters beyond the apex
Pulmonary Vessels.
Circulatory System
Physiologic Anatomy of the Pulmonary
exchange in the lungs. The present discussion is con-
Pulmonary Edema, Pleural Fluid
C
H
A
P
T
E
R
3
8
483
Pulmonary Circulation,
Some aspects of blood flow distribution and other
hemodynamics are particular to the pulmonary cir-
culation and are especially important for gas
cerned with these special features of the pulmonary
circulation.
of the right ventricle and then divides into right and left main branches that supply
gives the pulmonary arterial tree a
allows the pulmonary arteries to accommodate the stroke volume output of the
through the systemic circulation.
Blood also flows to the lungs through small bronchial arteries that
enters the left atrium, rather
the left ventricular output are about 1 to 2 per cent greater than the right ventric-
ular output.
.
and plasma protein leaking from the lung capillaries is also removed from the lung
Also, loss of blood from the systemic circulation by
to twice normal. For instance, when a person blows out
and pathological conditions, the quantity of blood in
Lungs as a Blood Reservoir.
between the pulmonary arteries and the veins.
laries, and the remainder is divided about equally
circulatory system. Approximately 70 milliliters of this
The blood volume of the lungs is about 450 milliliters,
Blood Volume of the Lungs
failure.
the pulmonary wedge pressure also rises. Therefore,
When the left atrial pressure rises to high values,
only 2 to 3 mm Hg greater than the left atrial pressure.
pulmonary capillaries, this wedge pressure is usually
artery, and because the blood vessels extending
the “wedge pressure,” is about 5 mm Hg. Because all
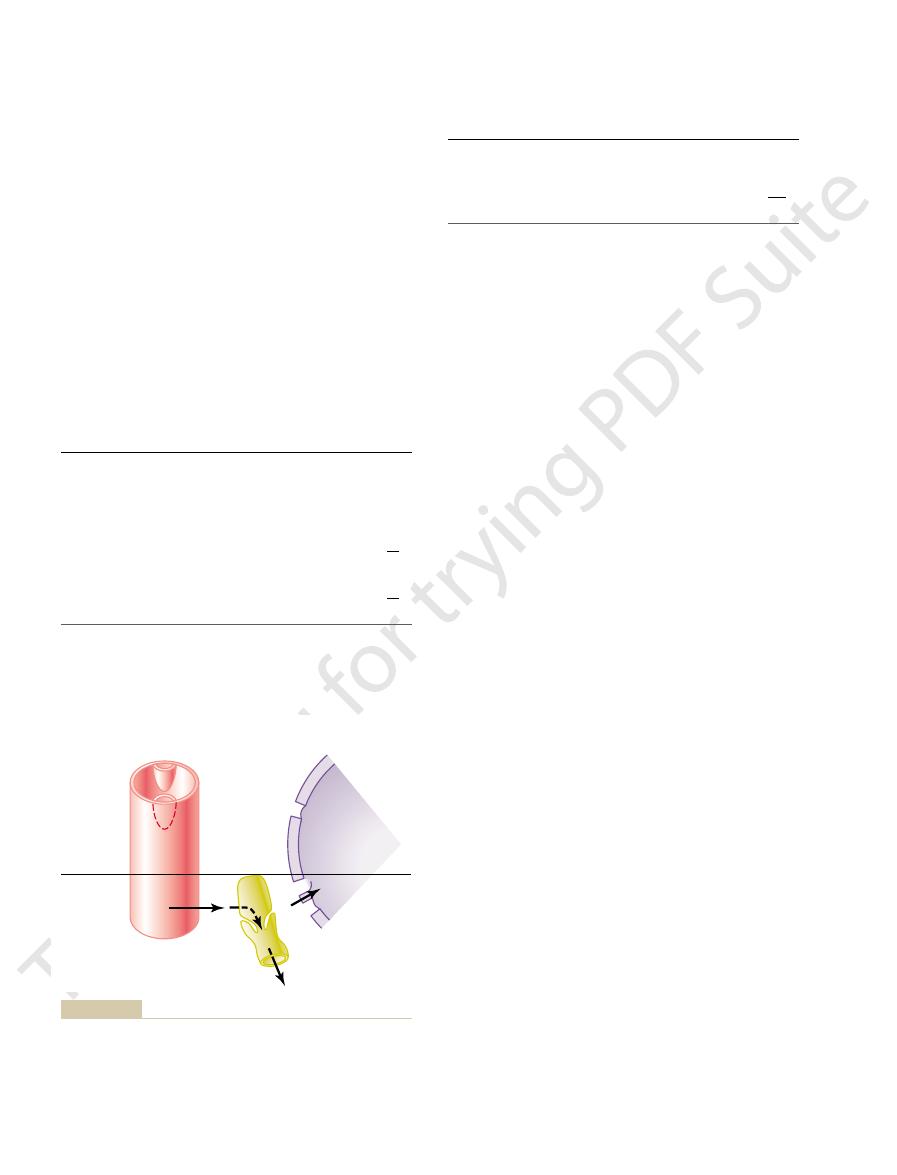
The pressure measured through the catheter, called
branch.
the small branches of the pulmonary artery, finally
to the right atrium, then through the right side of the
This is achieved
pulmonary wedge pressure.
estimated with moderate accuracy by measuring the
atrium. However, the left atrial pressure can often be
a human being’s left atrial pressure using a direct
high as 5 mm Hg. It usually is not feasible to measure
human being, varying from as low as 1 mm Hg to as
veins averages about 2 mm Hg in the recumbent
The mean
Left Atrial and Pulmonary Venous Pressures.
capillaries.
7 mm Hg. The importance of this low capillary pres-
illary pressure, as diagrammed in Figure 38–2, is about
The mean pulmonary cap-
Pulmonary Capillary Pressure.
is 15 mm Hg.
is about 8 mm Hg, and the
normal human being, the
averages about 25 mm Hg in the
As shown in Figure 38–2, the
capillaries of the lungs.
falls precipitously, whereas the pulmonary arterial
closes at the end of systole, the ventricular pressure
in Figure 38–1. However, after the pulmonary valve
to the pressure in the right ventricle, as also shown
systole,
Pressures in the Pulmonary Artery.
fifth those for the left ventricle.
averages about 0 to 1 mm Hg, values that are only one
484
Unit VII
Respiration
During
the
pressure in the pulmonary artery is essentially equal
pressure falls more slowly as blood flows through the
systolic pulmonary
arterial pressure
diastolic pulmonary arterial
pressure
mean pulmonary
arterial pressure
sure is discussed in detail later in the chapter in rela-
tion to fluid exchange functions of the pulmonary
pressure in the left atrium and the major pulmonary
measuring device because it is difficult to pass a
catheter through the heart chambers into the left
so-called
by inserting a catheter first through a peripheral vein
heart and through the pulmonary artery into one of
pushing the catheter until it wedges tightly in the small
blood flow has been stopped in the small wedged
beyond this artery make a direct connection with the
wedge pressure measurements can be used to clinically
study changes in pulmonary capillary pressure and
left atrial pressure in patients with congestive heart
about 9 per cent of the total blood volume of the entire
pulmonary blood volume is in the pulmonary capil-
Under various physiological
the lungs can vary from as little as one half normal up
air so hard that high pressure is built up in the lungs—
such as when blowing a trumpet—as much as 250 mil-
liliters of blood can be expelled from the pulmonary
circulatory system into the systemic circulation.
hemorrhage can be partly compensated for by the
0
0
8
25
75
120
2
1
Aortic pressure curve
Pulmonary artery curve
Right ventricular curve
Seconds
Pressure (mm Hg)
and aorta.
Pressure pulse contours in the right ventricle, pulmonary artery,
Figure 38–1
Pulmonary
artery
Left
atrium
Pulmonary
capillaries
0
2
8
7
15
M
D
S
25
Left
atrium
Pulmonary
capillaries
mm Hg
mean; S, systolic; red curve, arterial pulsations.
Pressures in the different vessels of the lungs. D, diastolic; M,
Figure 38–2
blood pressure inside them, but simultaneously, they are
The capillaries in the alveolar walls are distended by the
In each zone, the patterns of blood flow are quite
divided into three zones, as shown in Figure 38–4.
these differences, one often describes the lung as being
five times as much flow in the bottom. To help explain
rest, there is little flow in the top of the lung but about
the upright person. Note that in the standing position at
the lower curve in Figure 38–3, which depicts blood flow
the different areas of the lungs. This is demonstrated by
the lungs is about 8 mm Hg greater. Such pressure dif-
of the heart, and the pressure in the lowest portion of
portion of the lung of a standing person is about 15 mm
is, the pulmonary arterial pressure in the uppermost
15 mm Hg of which is above the heart and 8 below. That
This represents a 23 mm Hg pressure difference, about
In the normal, upright adult, the lowest point in the
same effect, but to a lesser degree, occurs in the lungs.
the weight of the blood itself in the blood vessels. The
—that is, by
heart. This is caused by
90 mm Hg greater than the pressure at the level of the
In Chapter 15, it was pointed out that the blood pres-
Pulmonary Blood Flow
Pressure Gradients in the
Effect of Hydrostatic
oxygen pressures.
lungs that are better aerated, thus providing an auto-
centration becomes low, the local vessels constrict.This
blood flow where it is most effective. That is, if some
resistance has an important function: to distribute
This effect of low oxygen on pulmonary vascular
hypoxic.
striction of the small arteries and arterioles. It has been
from the lung tissue; this substance promotes con-
than constrict in response to low oxygen. It is believed
effect observed in systemic vessels,
extremely low oxygen levels. This is
)—the adjacent blood vessels constrict, with the
falls below 70 per cent of normal (below 73 mm Hg
When the concentration of oxygen in the air of the
Flow—Automatic Control of Pulmonary Blood Flow Distribution.
best oxygenated. This is achieved by the following
occur, it is important for the blood to be distributed to
pressure. For adequate aeration of the blood to
vessels act as passive, distensible tubes that enlarge
blood flow. Under most conditions, the pulmonary
control cardiac output—mainly peripheral factors,
to the cardiac output. Therefore, the factors that
The blood flow through the lungs is essentially equal
Blood Flow Through the Lungs
has only mild systemic circulatory effects.
monary system, a shift of blood from one system to the
monary vascular pressures. Because the volume of the
to dam up in the pulmonary circulation, sometimes
Failure of the left side of the heart or increased resist-
Circulatory Systems as a Result of Cardiac Pathology.
temic vessels.
Pulmonary Circulation, Pulmonary Edema, Pleural Fluid
Chapter 38
485
automatic shift of blood from the lungs into the sys-
Shift of Blood Between the Pulmonary and Systemic
ance to blood flow through the mitral valve as a result
of mitral stenosis or mitral regurgitation causes blood
increasing the pulmonary blood volume as much as
100 per cent and causing large increases in the pul-
systemic circulation is about nine times that of the pul-
other affects the pulmonary system greatly but usually
and Its Distribution
as discussed in Chapter 20—also control pulmonary
with increasing pressure and narrow with decreasing
those segments of the lungs where the alveoli are
mechanism.
Effect of Diminished Alveolar Oxygen on Local Alveolar Blood
alveoli decreases below normal—especially when it
Po
2
vascular resistance increasing more than fivefold at
opposite to the
which dilate rather
that the low oxygen concentration causes some yet
undiscovered vasoconstrictor substance to be released
suggested that this vasoconstrictor might be secreted
by the alveolar epithelial cells when they become
alveoli are poorly ventilated so that their oxygen con-
causes the blood to flow through other areas of the
matic control system for distributing blood flow to the
pulmonary areas in proportion to their alveolar
Lungs on Regional
sure in the foot of a standing person can be as much as
hydrostatic pressure
lungs is about 30 centimeters below the highest point.
Hg less than the pulmonary arterial pressure at the level
ferences have profound effects on blood flow through
per unit of lung tissue at different levels of the lung in
different.
Zones 1, 2, and 3 of Pulmonary
Blood Flow
Top
Bottom
Middle
Lung level
Standing at rest
Exercise
Blood flow
(per unit of tissue)
through the bottom of the lung.
blood flow is very low at the top of the lungs; most of the flow is
Note that when the person is at rest, the
during exercise.
rest
Blood flow at different levels in the lung of an upright person
Figure 38–3
at
and
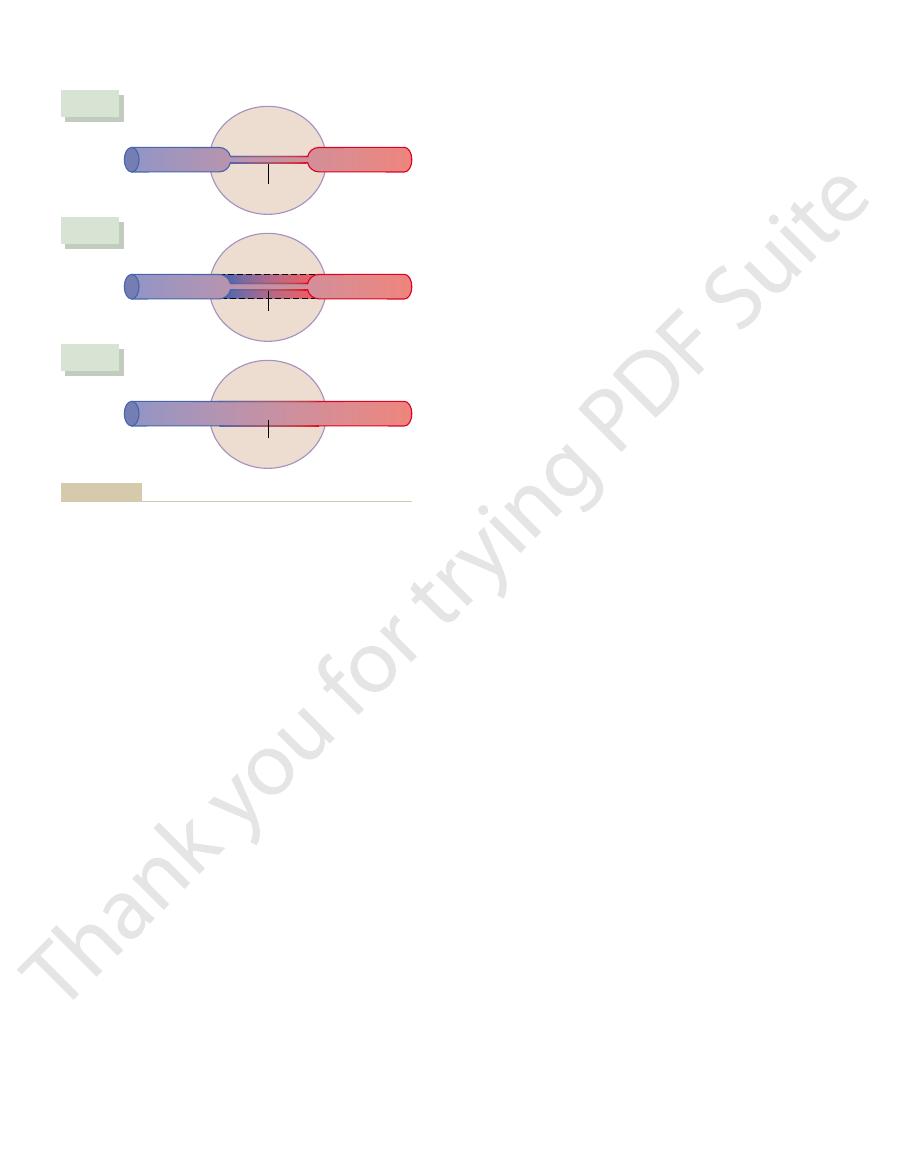
effect is shown in Figure 38–5.
rises very little, even during maximum exercise; this
pulmonary arterial pressure. In the normal person, the
capillary more than twofold; and (3) by increasing the
as much as threefold; (2) by distending all the capil-
increasing the number of open capillaries, sometimes
accommodated in the lungs in three ways: (1) by
increases fourfold to sevenfold. This extra flow is
During heavy exercise, blood flow through the lungs
Pulmonary Arterial Pressure During
on Pulmonary Blood Flow and
Effect of Increased Cardiac Output
zone 3 pattern of flow.
cent. The reason for these differences is that the pul-
be 700 to 800 per cent, whereas the increase in the lower
exercise. The increase in flow in the top of the lung may
Referring again to Figure 38–3, one sees that
blood loss.
sure is exceedingly low, as might occur after severe
flow—no blood flow—in the lung apices. Another
pressure is normal, one would expect zone 1 blood
that the intra-alveolar air pressure is at least 10 mm Hg
is too high to allow flow. For instance, if an upright
the cardiac cycle, occurs when either the pulmonary sys-
Zone 1 blood flow, which is blood flow at no time during
apices.
person is entirely zone 3 blood flow, including the lung
level of the heart. In this case, blood flow in a normal
blood flow. Also, when a person is lying down, no part
tinuous flow through the alveolar capillaries, or zone 3
the zero alveolar air pressure. Therefore, there is con-
bottom of the lungs, the pulmonary arterial pressure
In the lower regions of the lungs, from about 10 cen-
heart and extends from there to the top of the lungs.
blood flow. Zone 2 blood flow begins in the normal
cessation of flow during diastole; this is called zone 2
of the lung is intermittent, with flow during systole but
illary flow. Therefore, blood flow through the apical part
not sufficient to push the blood up the 15 mm Hg hydro-
8 mm Hg diastolic pressure at the level of the heart is
during cardiac systole. Conversely, during diastole, the
sure is greater than the zero alveolar air pressure, so that
pressure difference). This 10 mm Hg apical blood pres-
(25 mm Hg at heart level minus 15 mm Hg hydrostatic
fore, the apical systolic pressure is only 10 mm Hg
less than the pressure at the level of the heart. There-
arterial pressure at the lung apex is about 15 mm Hg
when a person is in the upright position, the pulmonary
3 (continuous flow) in all the lower areas. For example,
flow—zone 2 (intermittent flow) in the apices, and zone
Normally, the lungs have only zones 2 and 3 blood
pressure during the entire cardiac cycle
Zone 3: Continuous blood flow
sure, but the diastolic pressure is less than the alve-
Zone 2: Intermittent blood flow
cardiac cycle
cardiac cycle
Zone 1: No blood flow during all portions of the
blood flow, as follows:
different normal and pathological lung conditions, one
the capillaries close and there is no blood flow. Under
becomes greater than the capillary blood pressure,
sides. Therefore, any time the lung alveolar air pressure
486
Unit VII
Respiration
compressed by the alveolar air pressure on their out-
may find any one of three possible zones of pulmonary
because the local alveolar capillary
pressure in that area of the lung never rises higher
than the alveolar air pressure during any part of the
only during the pul-
monary arterial pressure peaks because the systolic
pressure is then greater than the alveolar air pres-
olar air pressure
because the alveolar
capillary pressure remains greater than alveolar air
blood flows through the pulmonary apical capillaries
static pressure gradient required to cause diastolic cap-
lungs about 10 centimeters above the midlevel of the
timeters above the level of the heart all the way to the
during both systole and diastole remains greater than
of the lung is more than a few centimeters above the
Zone 1 Blood Flow Occurs Only Under Abnormal Conditions.
tolic arterial pressure is too low or the alveolar pressure
person is breathing against a positive air pressure so
greater than normal but the pulmonary systolic blood
instance in which zone 1 blood flow occurs is in an
upright person whose pulmonary systolic arterial pres-
Effect of Exercise on Blood Flow Through the Different Parts of
the Lungs.
the blood flow in all parts of the lung increases during
part of the lung may be no more than 200 to 300 per
monary vascular pressures rise enough during exercise
to convert the lung apices from a zone 2 pattern into a
Heavy Exercise
laries and increasing the rate of flow through each
first two changes decrease pulmonary vascular resist-
ance so much that the pulmonary arterial pressure
Artery
Vein
Artery
Vein
Artery
Vein
P
ALV
ZONE 1
Ppc
P
ALV
ZONE 2
Ppc
P
ALV
ZONE 3
Ppc
remain greater than alveolar air pressure at all times.
arterial pressure and pulmonary capillary pressure (Ppc)
sure falls below alveolar air pressure; and
rises higher than alveolar air pressure, but diastolic arterial pres-
systolic arterial pressure
zone 2, intermittent flow
rial pressure;
) is greater than arte-
ALV
alveolar air pressure (P
Mechanics of blood flow in the three blood flow zones of the lung:
Figure 38–4
zone 1, no flow—
—
zone 3, continuous
flow—
about –8 mm Hg.)
pressure of fluid from the alveoli, giving a value of
–5 mm Hg, and by measuring the absorption
pulmonary interstitium, giving a value of about
two ways: by a micropipette inserted into the
subcutaneous tissue. (This has been measured in
2. The interstitial fluid pressure in the lung is
peripheral tissues of about 17 mm Hg.
7 mm Hg, in comparison with a considerably
1. The pulmonary capillary pressure is low, about
important differences, as follows:
quantitatively,
peripheral tissues. However,
The dynamics of fluid exchange across the lung capil-
Lungs, and Pulmonary Interstitial
Capillary Exchange of Fluid in the
excess carbon dioxide.
a fraction of a second, blood passing through the
accommodate the increased blood flow. Thus, in only
capillaries, which normally are collapsed, open up to
shorten to as little as 0.3 second. The shortening would
second. When the cardiac output increases, this can
lated that when the cardiac output is normal, blood
area of all the pulmonary capillaries, it can be calcu-
From histological study of the total cross-sectional
Length of Time Blood Stays in the Pulmonary Capillaries.
between these two values.
arterial pressure is only 15 mm Hg, so the mean
pressure is about 2 mm Hg and the mean pulmonary
probably nearly correct, because the mean left atrial
in Chapter 16, has given a value of 7 mm Hg. This is
monary capillary pressure, using a technique described
made. However, “isogravimetric” measurement of pul-
Pulmonary Capillary Pressure.
“sheet of flow,” rather than in individual capillaries.
one another side by side. Therefore, it is often said that
laries that, in most places, the capillaries almost touch
chapter. However, it is important for us to note here
Pulmonary Capillary Dynamics
discuss later in the chapter.
pressure, pulmonary edema is likely to develop, as we
above 30 mm Hg, causing similar increases in capillary
equally as much. When the left atrial pressure has risen
8 mm Hg increases the capillary pressure almost
heart. Any increase in left atrial pressure above 7 or
equally great increases in pulmonary arterial pressure,
rises to greater than 7 or 8 mm Hg, further increases
culatory function. But when the left atrial pressure
about 7 mm Hg, has very little effect on pulmonary cir-
50 mm Hg. The initial rise in atrial pressure, up to
value of 1 to 5 mm Hg all the way up to 40 to
begins to dam up in the left atrium. As a result, the
When the left side of the heart fails, however, blood
the pulmonary arteries.
strenuous exercise. These small changes in left atrial
6 mm Hg, even during the most
The left atrial pressure in a healthy person almost
as a Result of Left-Sided Heart Failure
When the Left Atrial Pressure Rises
Function of the Pulmonary Circulation
sure, thus also preventing the development of pul-
energy of the right side of the heart. This ability also
The ability of the lungs to accommodate greatly
Pulmonary Circulation, Pulmonary Edema, Pleural Fluid
Chapter 38
487
increased blood flow during exercise without increas-
ing the pulmonary arterial pressure conserves the
prevents a significant rise in pulmonary capillary pres-
monary edema.
never rises above
+
pressure have virtually no effect on pulmonary circu-
latory function because this merely expands the pul-
monary venules and opens up more capillaries so that
blood continues to flow with almost equal ease from
left atrial pressure can rise on occasion from its normal
in left atrial pressure above these levels cause almost
thus causing a concomitant increased load on the right
Exchange of gases between the alveolar air and the
pulmonary capillary blood is discussed in the next
that the alveolar walls are lined with so many capil-
the capillary blood flows in the alveolar walls as a
No direct measurements
of pulmonary capillary pressure have ever been
pulmonary capillary pressure must lie somewhere
passes through the pulmonary capillaries in about 0.8
be much greater were it not for the fact that additional
alveolar capillaries becomes oxygenated and loses its
Fluid Dynamics
lary membranes are qualitatively the same as for
there are
higher functional capillary pressure in the
slightly more negative than that in the peripheral
4
8
12
16
20
24
0
30
20
10
0
Normal value
Pulmonary arterial
pressure (mm Hg)
Cardiac output (L/min)
the cardiac output during exercise.
Effect on mean pulmonary arterial pressure caused by increasing
Figure 38–5
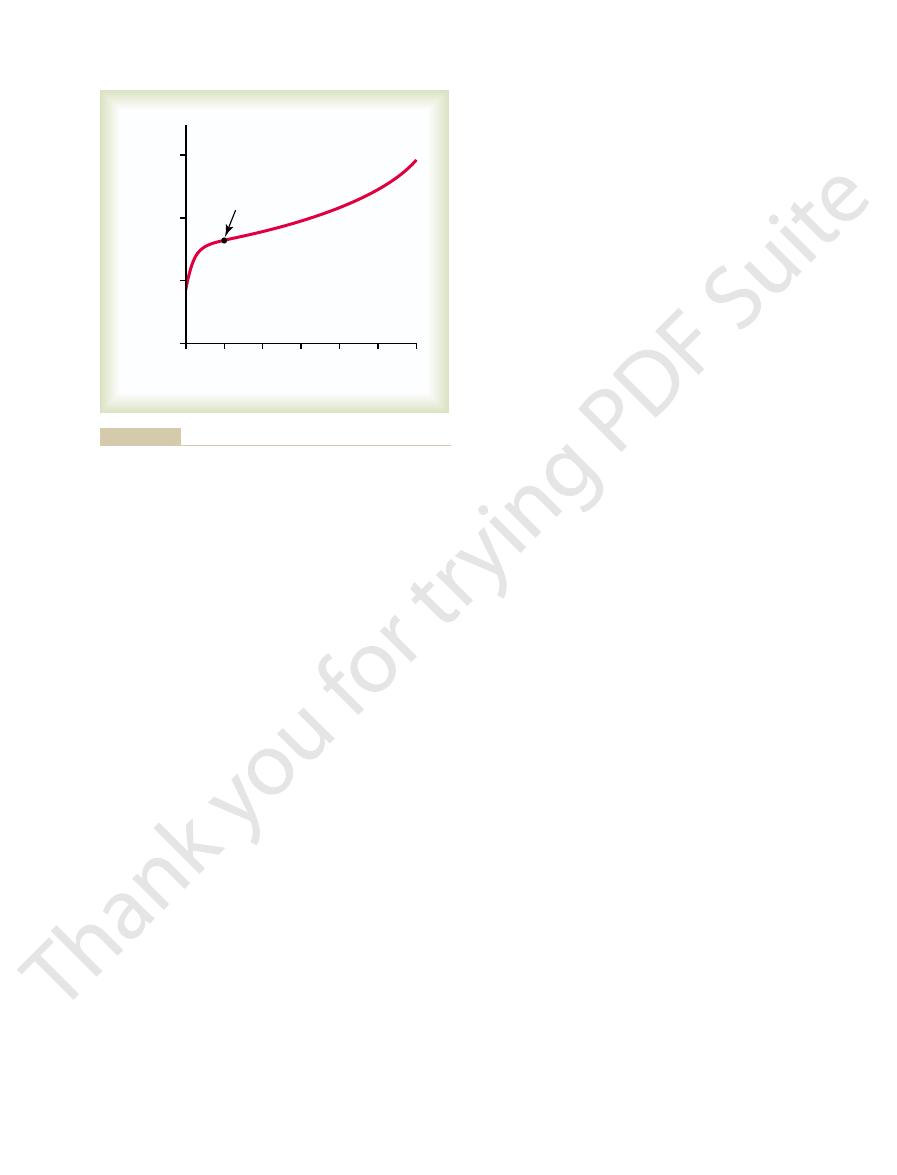
at the blood capillary membrane, as follows:
capillary and the alveolus. Note the balance of forces
capillary, a pulmonary alveolus, and a lymphatic capil-
Figure 38–6 shows a pulmonary
affect pulmonary fluid dynamics.
4. The alveolar walls are extremely thin, and the
half this value in the peripheral tissues.
about 14 mm Hg, in comparison with less than
protein molecules, so that the colloid osmotic
3. The pulmonary capillaries are relatively leaky to
488
Unit VII
Respiration
pressure of the pulmonary interstitial fluid is
alveolar epithelium covering the alveolar surfaces
is so weak that it can be ruptured by any positive
pressure in the interstitial spaces greater than
alveolar air pressure (greater than 0 mm Hg),
which allows dumping of fluid from the interstitial
spaces into the alveoli.
Now let us see how these quantitative differences
Interrelations Between Interstitial Fluid Pressure and Other
Pressures in the Lung.
lary draining the interstitial space between the blood
Interstitial fluid colloid osmotic pressure
14
Capillary pressure
7
Forces tending to cause movement of fluid outward from the
mm Hg
capillaries and into the pulmonary interstitium:
Forces tending to cause absorption of fluid into the capillaries:
TOTAL OUTWARD FORCE
29
Negative interstitial fluid pressure
8
Plasma colloid osmotic pressure
28
at the pulmonary capillary membrane; this
than the inward forces, providing a
Thus, the normal outward forces are slightly greater
TOTAL INWARD FORCE
28
mean filtration
pressure
can be calculated as follows:
Total outward force
mm Hg
+29
Total inward force
–28
“Pulmonary Edema Safety Factor.”
such as chlorine gas or sulfur dioxide gas. Each of
2. Damage to the pulmonary blood capillary
1. Left-sided heart failure or mitral valve disease, with
The most common causes of pulmonary edema are as
occurs elsewhere in the body. Any factor that causes the
“dry,” except for a small amount of fluid that seeps
Thus, under normal conditions, the alveoli are kept
lymphatics or absorbed into the pulmonary capillaries.
between the alveolar epithelial cells. Then the excess
in the alveoli, it will simply be sucked mechanically
spaces, it is clear that whenever extra fluid appears
However, if one remembers that the pulmonary cap-
ecules, as well as water and electrolytes, can pass.
This is not true, because experiments have shown
alveoli do not normally fill with fluid. One’s first incli-
for Keeping the Alveoli “Dry.”
Negative Pulmonary Interstitial Pressure and the Mechanism
orates in the alveoli, this fluid is pumped back to the
stitial spaces, and except for a small amount that evap-
This filtration pressure causes a slight continual flow
MEAN FILTRATION PRESSURE
+1
of fluid from the pulmonary capillaries into the inter-
circulation through the pulmonary lymphatic system.
One of the most important
problems in lung function is to understand why the
nation is to think that the alveolar epithelium is strong
enough and continuous enough to keep fluid from
leaking out of the interstitial spaces into the alveoli.
that there are always openings between the alveolar
epithelial cells through which even large protein mol-
illaries and the pulmonary lymphatic system normally
maintain a slight negative pressure in the interstitial
into the lung interstitium through the small openings
fluid is either carried away through the pulmonary
from the epithelium onto the lining surfaces of the
alveoli to keep them moist.
Pulmonary Edema
Pulmonary edema occurs in the same way that edema
pulmonary interstitial fluid pressure to rise from the
negative range into the positive range will cause rapid
filling of the pulmonary interstitial spaces and alveoli
with large amounts of free fluid.
follows:
consequent great increases in pulmonary venous
pressure and pulmonary capillary pressure and
flooding of the interstitial spaces and alveoli.
membranes caused by infections such as
pneumonia or by breathing noxious substances
these causes rapid leakage of both plasma proteins
and fluid out of the capillaries and into both the
lung interstitial spaces and the alveoli.
Experiments in animals
have shown that the pulmonary capillary pressure nor-
Lymphatic pump
Hydrostatic
pressure
-
8
+
7
-
14
-
8
Osmotic
pressure
Net
pressure
CAPILLARY
Pressures Causing Fluid Movement
ALVEOLUS
(
+
1 )
( 0 )
(Evaporation)
(Surface
tension
at pore)
-
28
-
5
-
4
-
8
Circulatory Physiology II: Dynamics and Control of the Body
stitial spaces. (Modified from Guyton AC, Taylor AE, Granger HJ:
that pumps fluid from the pulmonary inter-
Hydrostatic and osmotic forces at the capillary
Figure 38–6
(left) and alveolar
membrane (right) of the lungs. Also shown is the tip end of a lym-
phatic vessel (center)
Fluids. Philadelphia: WB Saunders, 1975.)
–4 mm Hg, the pleural fluid pressure must always be at
the normal collapse tendency of the lungs is about
sure found in most tissue spaces of the body). Because
in the normal pleural space. The basic cause of this neg-
lungs expanded. This is provided by negative pressure
is not obviously a physical space.
parietal pleura. Therefore, the
of the diaphragm, and (3) the lateral surfaces of the
cavity into (1) the mediastinum, (2) the superior surface
in the pleural cavity, the excess fluid is pumped away by
mally slight, only a few milliliters. Whenever the quan-
The total amount of fluid in each pleural cavity is nor-
moving lungs.
tic, which is what allows extremely easy slippage of the
proteins, giving the pleural fluid a mucoid characteris-
the pleural space. These fluids carry with them tissue
mesenchymal, serous membrane through which small
the pleural space. The pleural membrane is a porous,
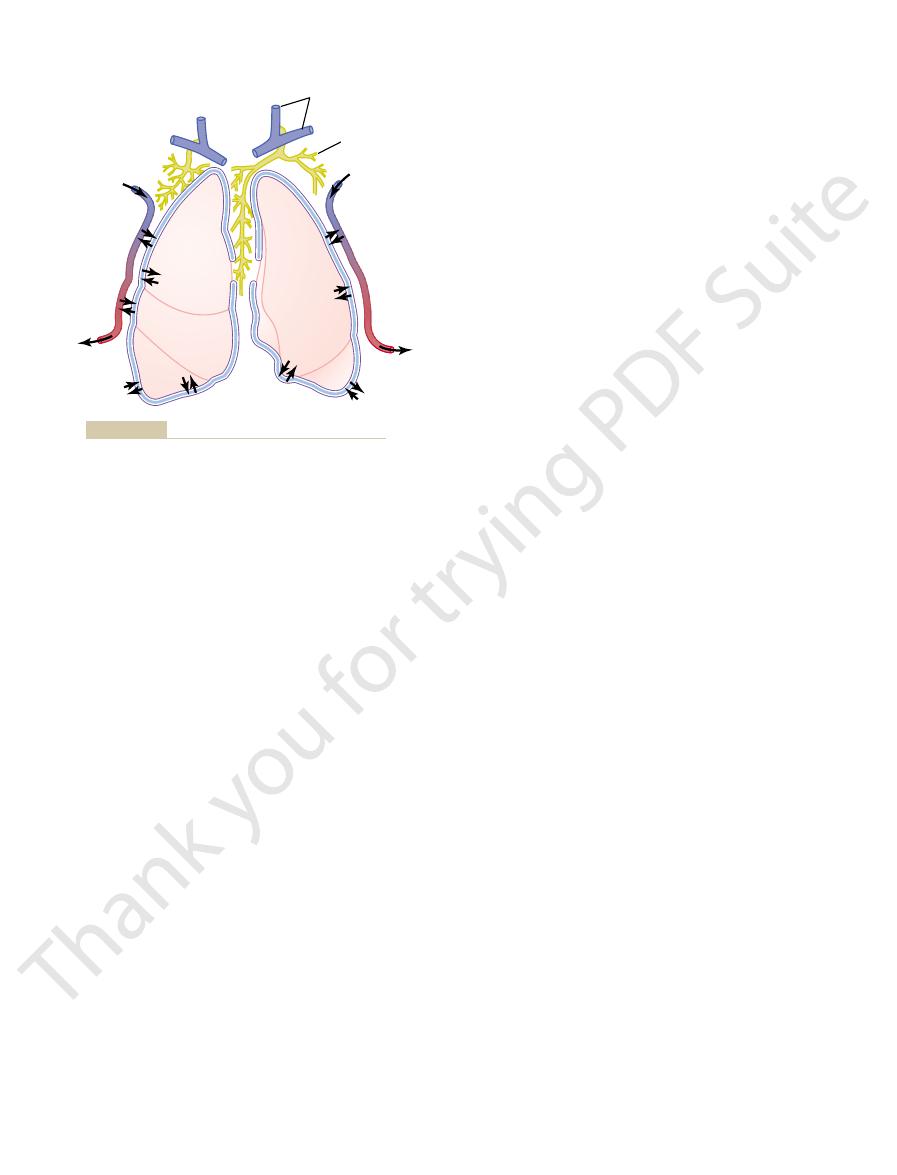
Figure 38–8 shows the dynamics of fluid exchange in
between the parietal and visceral pleurae.
cavity. To facilitate this, a thin layer of mucoid fluid lies
breathing, they slide back and forth within the pleural
When the lungs expand and contract during normal
does rise to 50 mm Hg, death frequently ensues in less
factor level. Thus, in acute left-sided heart failure, in
illary pressure rises 25 to 30 mm Hg above the safety
within hours, or even within 20 to 30 minutes if the cap-
safety factor level, lethal pulmonary edema can occur
When the pul-
Rapidity of Death in Acute Pulmonary Edema.
45 mm Hg have been measured without the develop-
mitral stenosis, pulmonary capillary pressures of 40 to
much as 10-fold. Therefore, in patients with chronic
vessels expand greatly, increasing their capability of car-
(for at least 2 weeks), the lungs become even more
When the pul-
of 21 mm Hg.
28 mm Hg to cause pulmonary edema, giving an
rise from the normal level of 7 mm Hg to more than
plasma colloid osmotic pressure is 28 mm Hg, one can
level. Therefore, in the human being, whose normal
ments was equal to this 25 mm Hg critical pressure
rapidly with further increases in capillary pressure. The
lungs. This fluid accumulation increased even more
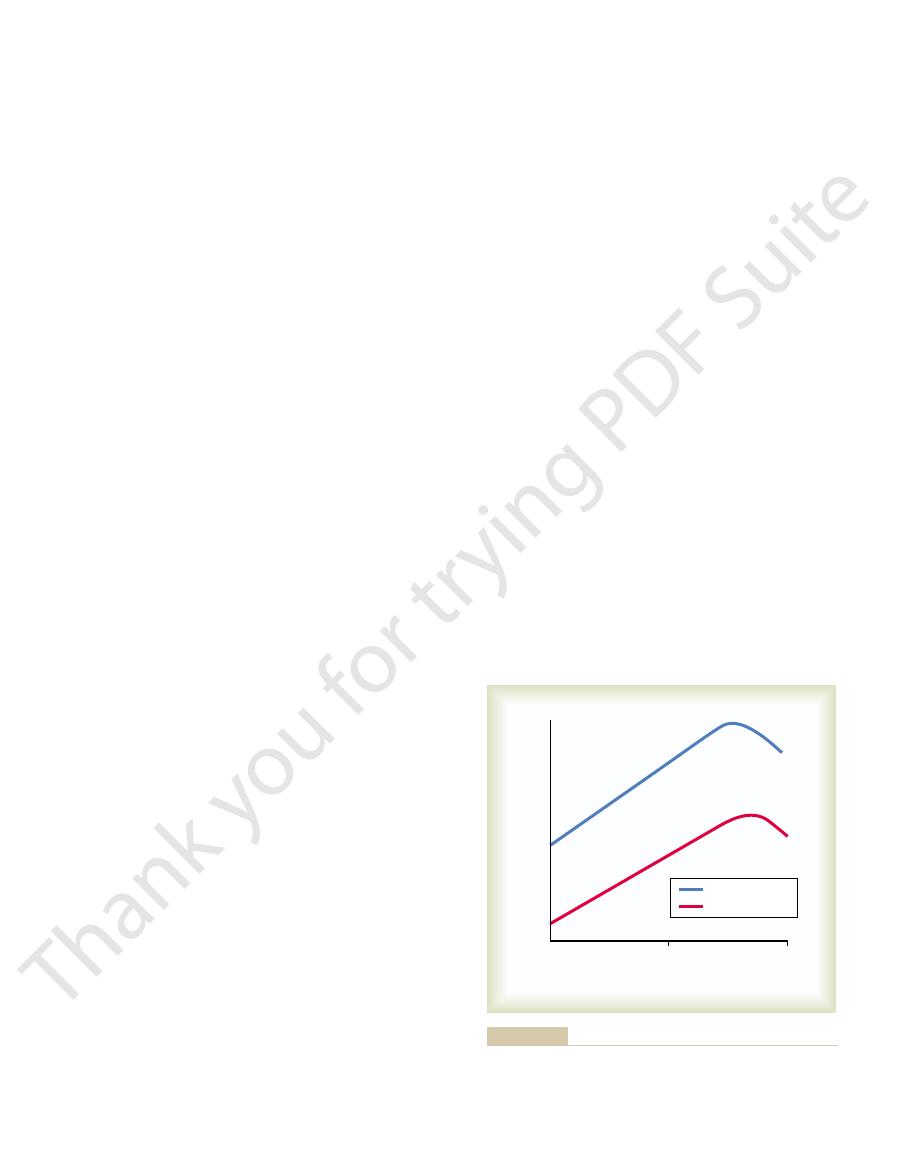
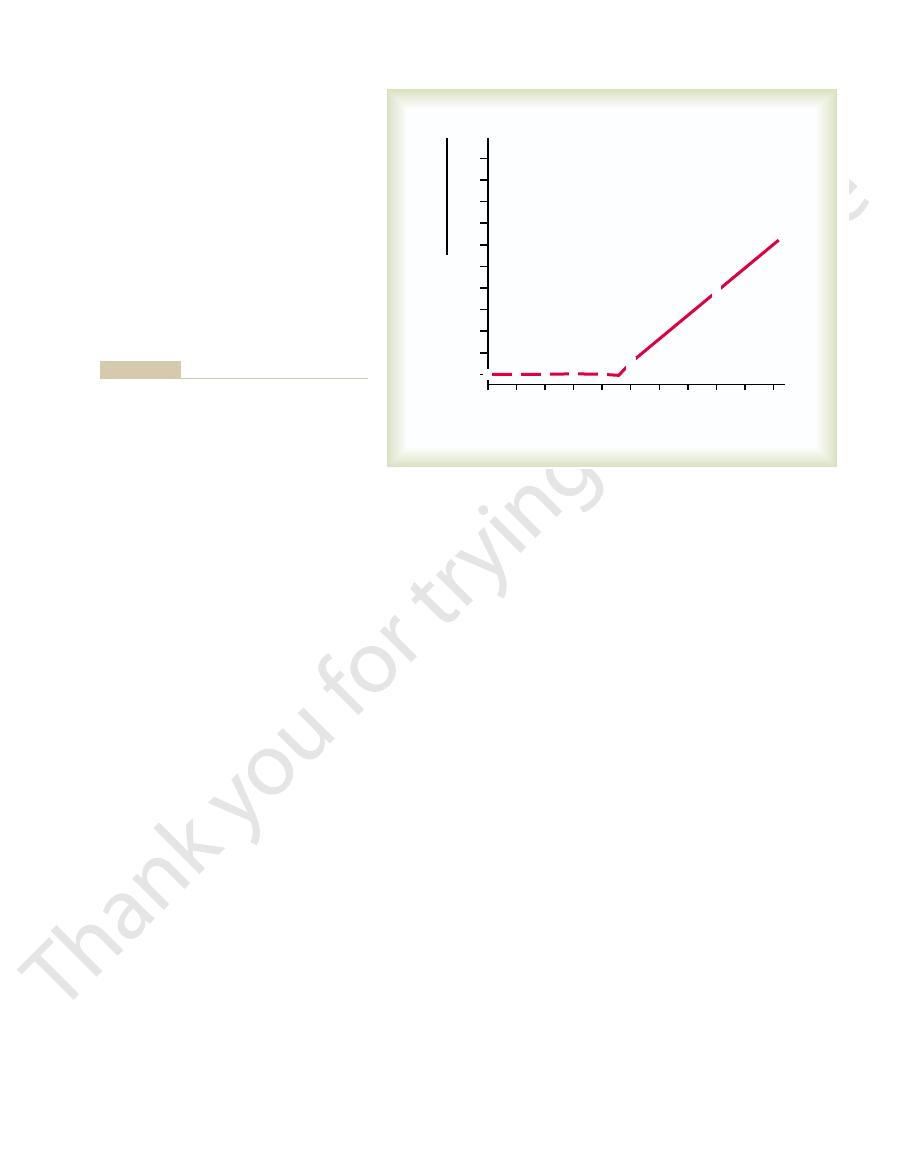
rise above 25 mm Hg), fluid began to accumulate in the
23 mm Hg (causing the pulmonary capillary pressure to
ments, as soon as the left atrial pressure rose above
greater than the left atrial pressure. In these experi-
monary capillary pressure rises to a level 1 to 2 mm Hg
the left atrial pressure rises to high values, the pul-
edema formation in dogs. Remember that every time
an example, Figure 38–7 shows how different levels of
before significant pulmonary edema will occur. To give
Pulmonary Circulation, Pulmonary Edema, Pleural Fluid
Chapter 38
489
mally must rise to a value at least equal to the colloid
osmotic pressure of the plasma inside the capillaries
left atrial pressure increase the rate of pulmonary
plasma colloid osmotic pressure during these experi-
predict that the pulmonary capillary pressure must
acute
safety factor against pulmonary edema
Safety Factor in Chronic Conditions.
monary capillary pressure remains elevated chronically
resistant to pulmonary edema because the lymph
rying fluid away from the interstitial spaces perhaps as
ment of lethal pulmonary edema.
monary capillary pressure rises even slightly above the
which the pulmonary capillary pressure occasionally
than 30 minutes from acute pulmonary edema.
Fluid in the Pleural Cavity
amounts of interstitial fluid transude continually into
tity becomes more than barely enough to begin flowing
lymphatic vessels opening directly from the pleural
pleural space—the space
between the parietal and visceral pleurae—is called a
potential space because it normally is so narrow that it
“Negative Pressure” in Pleural Fluid.
A negative force is
always required on the outside of the lungs to keep the
ative pressure is pumping of fluid from the space by the
lymphatics (which is also the basis of the negative pres-
x
x
x
x
x
x
x
x
x
x
x
x
x
x
x
x
x
x
x
30
35
40
45
50
0
5
10
15
20
25
x
x
x
x
x
x
10
9
8
7
6
5
4
3
2
1
0
Left atrial pressure (mm Hg)
Rate of edema formation =
edema fluid per hour
dry weight of lung
of pulmonary edema. Circ Res 7:649, 1959.)
plasma protein concentration on the development
of elevated left atrial pressure and decreased
is increased. (From Guyton AC, Lindsey AW: Effect
atrial pressure (and pulmonary capillary pressure)
Figure 38–7
Rate of fluid loss into the lung tissues when the left
J Appl Physiol 89:2483, 2000.
West JB: Invited review: pulmonary capillary stress failure.
Baltimore: Williams & Wilkins, 1994.
West JB: Respiratory Physiology—The Essentials, 5th ed.
139:499, 2003.
Wallace J: Update in pulmonary diseases. Ann Intern Med
olar membrane to solutes. Circ Res 16:353, 1965.
Taylor AE, Guyton AC, Bishop VS: Permeability of the alve-
J Exp Biol 204:3121, 2001.
Schoene RB: Limits of human lung function at high altitude.
structure. News Physiol Sci 16:66, 2001.
of lung edema: interstitial fluid dynamics and molecular
Miserocchi G, Negrini D, Passi A, De Luca G: Development
285:L1184, 2003.
nitrogen species. Am J Physiol Lung Cell Mol Physiol
Matalon S, Hardiman KM, Jain L, et al: Regulation of ion
Rev 84:385, 2004.
Lai-Fook SJ: Pleural mechanics and fluid exchange. Physiol
failure of reabsorption? News Physiol Sci 18:55, 2003.
Hoschele S, Mairbaurl H: Alveolar flooding at high altitude:
phia: WB Saunders, 1975.
II. Dynamics and Control of the Body Fluids. Philadel-
Guyton AC, Taylor AE, Granger HJ: Circulatory Physiology.
(eds): Pulmonary Edema. Baltimore: Waverly Press, 1979,
water movement in the lung. In: Fishman AP, Renkin EM
Guyton AC, Parker JC, Taylor AE, et al: Forces governing
development of pulmonary edema. Circ Res 7:649, 1959.
Guyton AC, Lindsey AW: Effect of elevated left atrial pres-
124:1090, 2003.
heart failure: evidence of a pathophysiologic role. Chest
Guazzi M: Alveolar-capillary membrane dysfunction in
left heart failure. Chest 125:669, 2004.
Gehlbach BK, Geppert E: The pulmonary manifestations of
plasma proteins and fluid into the cavity.
faces of the pleural cavity, which breaks down the cap-
thus allowing excessive transudation of fluid; and (4)
(3) greatly reduced plasma colloid osmotic pressure,
eral and pulmonary capillary pressures, leading to
(2) cardiac failure, which causes excessively high periph-
other tissues (discussed in Chapter 25), including (1)
be called “edema of the pleural cavity.” The causes of
large amounts of free fluid in the pleural space.The effu-
pleura of the chest cavity, except for an extremely thin
pressure of the lungs. Thus, the negativity of the pleural
pressure is usually about –7 mm Hg, which is a few mil-
expanded. Actual measurements have shown that the
least as negative as –4 mm Hg to keep the lungs
490
Unit VII
Respiration
limeters of mercury more negative than the collapse
fluid keeps the normal lungs pulled against the parietal
layer of mucoid fluid that acts as a lubricant.
Pleural Effusion.
Pleural effusion means the collection of
sion is analogous to edema fluid in the tissues and can
the effusion are the same as the causes of edema in
blockage of lymphatic drainage from the pleural cavity;
excessive transudation of fluid into the pleural cavity;
infection or any other cause of inflammation of the sur-
illary membranes and allows rapid dumping of both
References
sure and decreased plasma protein concentration on the
p 65.
channel structure and function by reactive oxygen-
Vein
Lymphatics
Venous system
Artery
Figure 38–8
Dynamics of fluid exchange in the intrapleural space.