proportional to the concentration of the gas molecules.
gas striking the surface at any given instant. This means that
fore, the pressure of a gas acting on the surfaces of the respiratory passages and
Pressure is caused by multiple impacts of moving molecules against a surface. There-
of Individual Gases
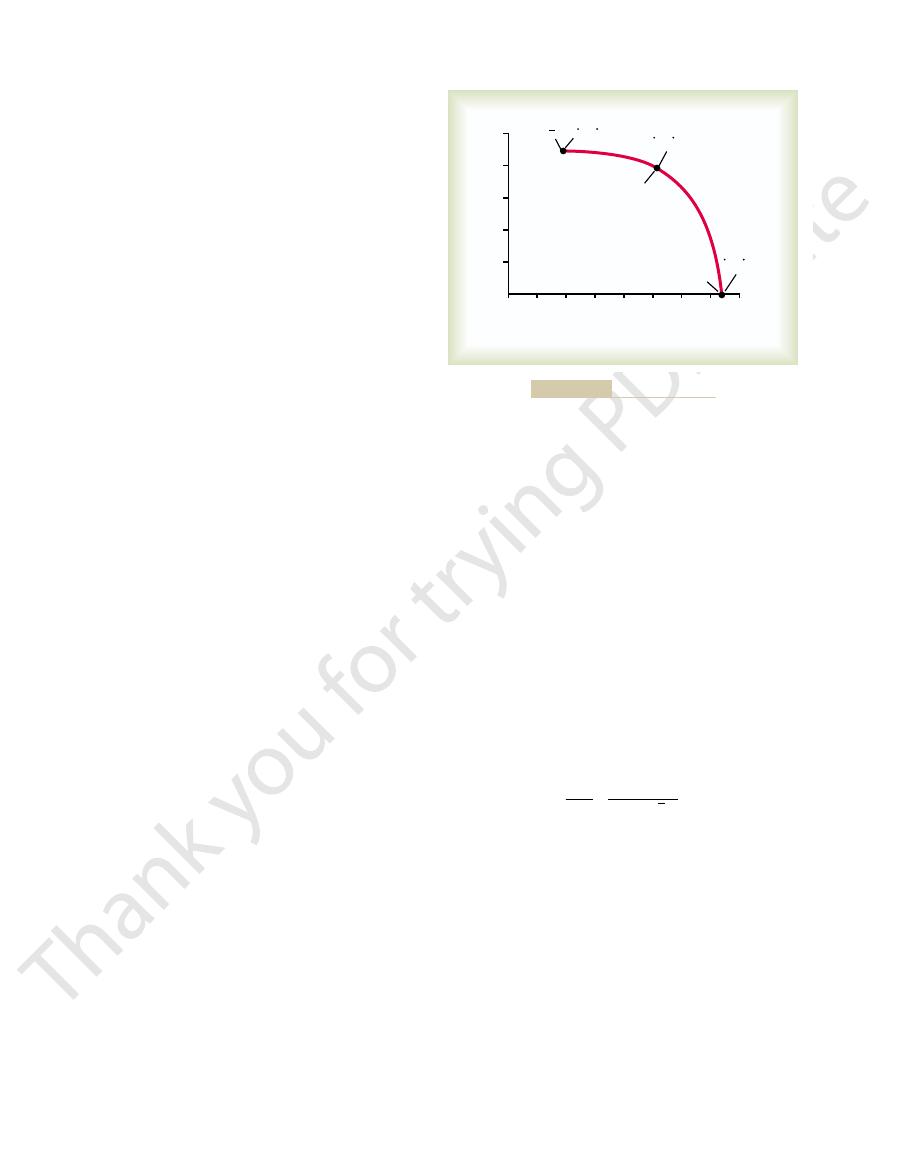
ately different, as demonstrated by the lengths of the arrows in the figure.
tion. Therefore, the rates of diffusion in each of the two directions are proportion-
area. The reason is obvious: There are far more molecules at end A of the chamber
and a low concentration at the other end, as shown in Figure 39–1, net diffusion of
rapidly and randomly among one another.
continue until striking other molecules again. In this way, the molecules move
ity until they strike other molecules. Then they bounce away in new directions and
that are not physically attached to others, this means linear movement at high veloc-
all molecules of all matter are continually undergoing motion. For free molecules
kinetic motion of the molecules themselves. Except at absolute zero temperature,
For diffusion to occur, there must be a source of energy. This is provided by the
of gases dissolved in the fluids and tissues of the body.
to move among one another, which is the process called “diffusion.” This is also true
Molecular Basis of Gas Diffusion
Partial Pressures
Physics of Gas Diffusion and Gas
physics of diffusion and gas exchange.
this is a much more complex problem, requiring a deeper understanding of the
However, in respiratory physiology, one is concerned not only with the basic
the respiratory membrane and adjacent fluids.
direction, out of the blood. The process of diffusion
After the alveoli are ventilated with fresh air, the
and Carbon Dioxide Through
Exchange; Diffusion of Oxygen
C
H
A
P
T
E
R
3
9
491
Physical Principles of Gas
the Respiratory Membrane
next step in the respiratory process is diffusion of
oxygen from the alveoli into the pulmonary blood
and diffusion of carbon dioxide in the opposite
is simply the random motion of molecules inter-
twining their way in all directions through
mechanism by which diffusion occurs but also with the rate at which it occurs;
All the gases of concern in respiratory physiology are simple molecules that are free
Net Diffusion of a Gas in One Direction—Effect of a Concentration Gradient.
If a gas chamber
or a solution has a high concentration of a particular gas at one end of the chamber
the gas will occur from the high-concentration area toward the low-concentration
to diffuse toward end B than there are molecules to diffuse in the opposite direc-
Gas Pressures in a Mixture of Gases—“Partial Pressures”
alveoli is proportional to the summated force of impact of all the molecules of that
the pressure is directly

Henry’s
are expressed by the following formula, which is
develop with fewer dissolved molecules. These relations
those that are repelled, high partial pressure will
pressure within the solution. Conversely, in the case of
are repelled. When molecules are attracted, far more of
chemically attracted to water molecules, whereas others
molecules, especially carbon dioxide, are physically or
of the gas. That is, some types of
The partial pressure of a gas in a solution is
e, and so forth.
in the gas state, that is, P
does. The partial pressures of the separate dissolved
such as the membrane of a cell, it exerts its own partial
when the gas dissolved in fluid encounters a surface,
moving randomly and have kinetic energy. Further,
pressure, because the dissolved gas molecules are
Water and Tissues
e, and
The partial pressures of individual gases in a mixture are
760 mm Hg, the sum of the individual partial pressures.
pressure” of oxygen is 160 mm Hg; the total pressure is
nitrogen in the mixture is 600 mm Hg, and the “partial
oxygen (160 mm Hg). Thus, the “partial pressure” of
caused by nitrogen (600 mm Hg) and 21 per cent by
tration. Therefore, 79 per cent of the 760 mm Hg is
760 mm Hg. It is clear from the preceding description of
of 79 per cent nitrogen and 21 per cent oxygen. The
Consider air, which has an approximate composition
concept of partial pressure can be explained as follows.
of that gas. The
proportional to the pressure caused by that gas alone,
The rate of diffusion of each of these gases is directly
carbon dioxide.
oxygen, nitrogen,
gases, mainly of
In respiratory physiology, one deals with mixtures of
492
Unit VII
Respiration
and
which is called the partial pressure
total pressure of this mixture at sea level averages
the molecular basis of pressure that each gas contributes
to the total pressure in direct proportion to its concen-
designated by the symbols Po
2
, Pco
2
, Pn
2
, Ph
2
o, Ph
so forth.
Pressures of Gases Dissolved in
Gases dissolved in water or in body tissues also exert
pressure in the same way that a gas in the gas phase
gases are designated the same as the partial pressures
o
2
, Pco
2
, Pn
2
, Ph
Factors That Determine the Partial Pressure of a Gas Dissolved in
a Fluid.
determined not only by its concentration but also by the
solubility coefficient
them can be dissolved without building up excess partial
law:
Partial pressure
Concentration of dissolved gas
Solubility coefficient
=
each volume of water, the solubility coef
(1 atmosphere pressure equals 760 mm Hg) and con-
When partial pressure is expressed in atmospheres
centration is expressed in volume of gas dissolved in
ficients for
important respiratory gases at body temperature are the
following:
Nitrogen
0.012
Carbon monoxide
0.018
Carbon dioxide
0.57
Oxygen
0.024
in many of our subsequent discussions.
sure at body temperature, 47 mm Hg; this value appears
C it is 760 mm Hg. But the
C is 5 mm Hg, and at 100
gas phase. For instance, the water vapor pressure at
therefore, the greater the likelihood that the water mol-
temperature of the water. The greater the temperature,
The vapor pressure of water depends entirely on the
pressure, like the other partial pressures, is designated
water vapor in the gas mixture is 47 mm Hg. This partial
that is, once it is in
pressure is 47 mm Hg. Therefore, once the gas mixture
C, this vapor
water. At normal body temperature, 37
from the water surface into the gas phase. The partial
ferent dissolved gas molecules, are continually escaping
results from the fact that water molecules, like the dif-
es the air. This
passageways, water immediately evaporates from the
When nonhumidi
Vapor Pressure of Water
for carbon dioxide, then net diffusion will occur toward
the dissolved state in the blood, which is normally true
natively, if the partial pressure of the gas is greater in
diffuse into the blood than in the other direction. Alter-
as is normally true for oxygen, then more molecules will
the difference between the two partial pressures. If the
occur? The answer is that net diffusion is determined by
alveoli. The rate at which they escape is directly pro-
uid of the blood, and
of the alveolar capillaries. Conversely, the molecules of
The partial pressure
Dissolved Phase in the Pulmonary Blood.
more than 20 times as soluble as oxygen. Therefore, the
From this table, one can see that carbon dioxide is
Helium
0.008
partial pressure of carbon dioxide (for a given concen-
tration) is less than one twentieth that exerted by
oxygen.
Diffusion of Gases Between the Gas Phase in the Alveoli and the
of each gas in the alveolar respiratory gas mixture tends
to force molecules of that gas into solution in the blood
the same gas that are already dissolved in the blood
are bouncing randomly in the fl
some of these bouncing molecules escape back into the
portional to their partial pressure in the blood.
But in which direction will net diffusion of the gas
partial pressure is greater in the gas phase in the alveoli,
the gas phase in the alveoli.
fied air is breathed into the respiratory
surfaces of these passages and humidifi
pressure that the water molecules exert to escape
through the surface is called the vapor pressure of the
°
has become fully humidified—
“equi-
librium” with the water—the partial pressure of the
Ph
2
o.
the greater the kinetic activity of the molecules and,
ecules will escape from the surface of the water into the
0°
°
most important value to remember is the vapor pres-
Dissolved gas molecules
A
B
net diffusion.
(B). The difference between the lengths of the arrows represents
Diffusion of oxygen from one end of a chamber (A) to the other
Figure 39–1
in which D is the diffusion rate,
expressed in a single formula, as follows:
the rate of diffusion of the gas. All these factors can be
to the square root of the molecular weight, the greater
ment of the molecules, which is inversely proportional
tance. Finally, the greater the velocity of kinetic move-
the greater the distance the molecules must diffuse, the
total number of molecules that diffuse. Conversely,
sectional area of the diffusion pathway, the greater the
partial pressure difference. The greater the cross-
The greater the solubility of the gas, the greater the
factors, the temperature, remains reasonably constant
uid. In the body, the last of these
diffuse, (4) the molecular weight of the gas, and (5) the
uid, (3) the distance through which the gas must
uid, (2) the cross-sectional area of
uid. They are (1) the solubil-
the pressure difference, several other factors affect the
between the two areas, called simply the
sure. Therefore, the
However, some molecules do bounce randomly from
greater number, have a greater statistical chance of
ecules in the area of high pressure, because of their
1, one can readily see that the mol-
turning to Figure 39
area toward the low-pressure area. For instance, re-
area, there will be net diffusion from the high-pressure
preceding discussion, it is clear that when the partial
Now, let us return to the problem of diffusion. From the
Diffusion of Gases Through
Physical Principles of Gas Exchange; Diffusion of Oxygen and Carbon Dioxide
Chapter 39
493
Fluids—Pressure Difference Causes
Net Diffusion
pressure of a gas is greater in one area than in another
–
moving randomly into the area of low pressure than
do molecules attempting to go in the other direction.
the area of low pressure toward the area of high pres-
net diffusion of gas from the area of
high pressure to the area of low pressure is equal to the
number of molecules bouncing in this forward direction
minus the number bouncing in the opposite direction;
this is proportional to the gas partial pressure difference
pressure dif-
ference for causing diffusion.
Quantifying the Net Rate of Diffusion in Fluids.
In addition to
rate of gas diffusion in a fl
ity of the gas in the fl
the fl
temperature of the fl
and usually need not be considered.
number of molecules available to diffuse for any given
longer it will take the molecules to diffuse the entire dis-
DP is the partial pres-
sure difference between the two ends of the diffusion
d
MW
P
A
S
D
µ
¥
¥
¥
D
,
for oxygen is 1, the
cients. Assuming that the diffusion coef
which is proportional to S/
. That is, the relative
diffusion coefficient of the gas,
solubility and molecular weight. Together, these two
and MW is the molecular weight of the gas.
is the solubility of the gas, d is the distance of diffusion,
pathway, A is the cross-sectional area of the pathway, S
It is obvious from this formula that the characteristics
of the gas itself determine two factors of the formula:
factors determine the
rates at which different gases at the same partial pres-
sure levels will diffuse are proportional to their diffu-
sion coeffi
ficient
relative diffusion coefficients for dif-
ferent gases of respiratory importance in the body fluids
are as follows:
Nitrogen
0.53
Carbon monoxide
0.81
Carbon dioxide
20.3
Oxygen
1.0
the pulmonary blood into the alveoli. And fourth, dry
air. Third, carbon dioxide is constantly diffusing from
with each breath. Second, oxygen is constantly being
are several reasons for the differences. First, the alve-
1 with that of atmospheric air. There
sition in Table 39
gases as atmospheric air by any means, which can
sion of gases in water, as given in the preceding list.
the respiratory membrane, is almost equal to the diffu-
fusion of gases through the tissues, including through
instead of through the cell membranes. Therefore, dif-
soluble in cell membranes. Because of this, the major
highly soluble in lipids and, consequently, are highly
The gases that are of respiratory importance are all
Diffusion of Gases Through Tissues
Helium
0.95
limitation to the movement of gases in tissues is the rate
at which the gases can diffuse through the tissue water
Composition of Alveolar
Air—Its Relation to
Atmospheric Air
Alveolar air does not have the same concentrations of
readily be seen by comparing the alveolar air compo-
–
olar air is only partially replaced by atmospheric air
absorbed into the pulmonary blood from the alveolar
MW
Table 39–1
0.3
(0.04%)
0.3
(0.04%)
40.0
(5.3%)
27.0
(3.6%)
159.0
(20.84%)
149.3
(19.67%)
104.0
(13.6%)
120.0
(15.7%)
597.0
(78.62%)
563.4
(74.09%)
569.0
(74.9%)
566.0
(74.5%)
(mm Hg)
(mm Hg)
(mm Hg)
(mm Hg)
Atmospheric Air*
Humidified Air
Alveolar Air
Expired Air
Partial Pressures of Respiratory Gases as They Enter and Leave the Lungs (at Sea Level)
N
2
O
2
CO
2
TOTAL
760.0
(100.0%)
760.0
(100.0%)
760.0
(100.0%)
760.0
(100.0%)
O
3.7
(0.50%)
47.0
(6.20%)
47.0
(6.2%)
47.0
(6.2%)
H
2
* On an average cool, clear day.
the ventilatory process.
alveoli, and its partial pressure as well, is controlled by
tion becomes. Therefore, oxygen concentration in the
alveoli from the atmosphere, the higher its concentra-
its concentration in the alveoli becomes; conversely,
phere. The more rapidly oxygen is absorbed, the lower
into the blood of the lungs, and new oxygen is contin-
Pressure in the Alveoli
Oxygen Concentration and Partial
tion, and tissue pH when respiration is temporarily
tissue oxygenation, tissue carbon dioxide concentra-
nism much more stable than it would be otherwise, and
the blood. This makes the respiratory control mecha-
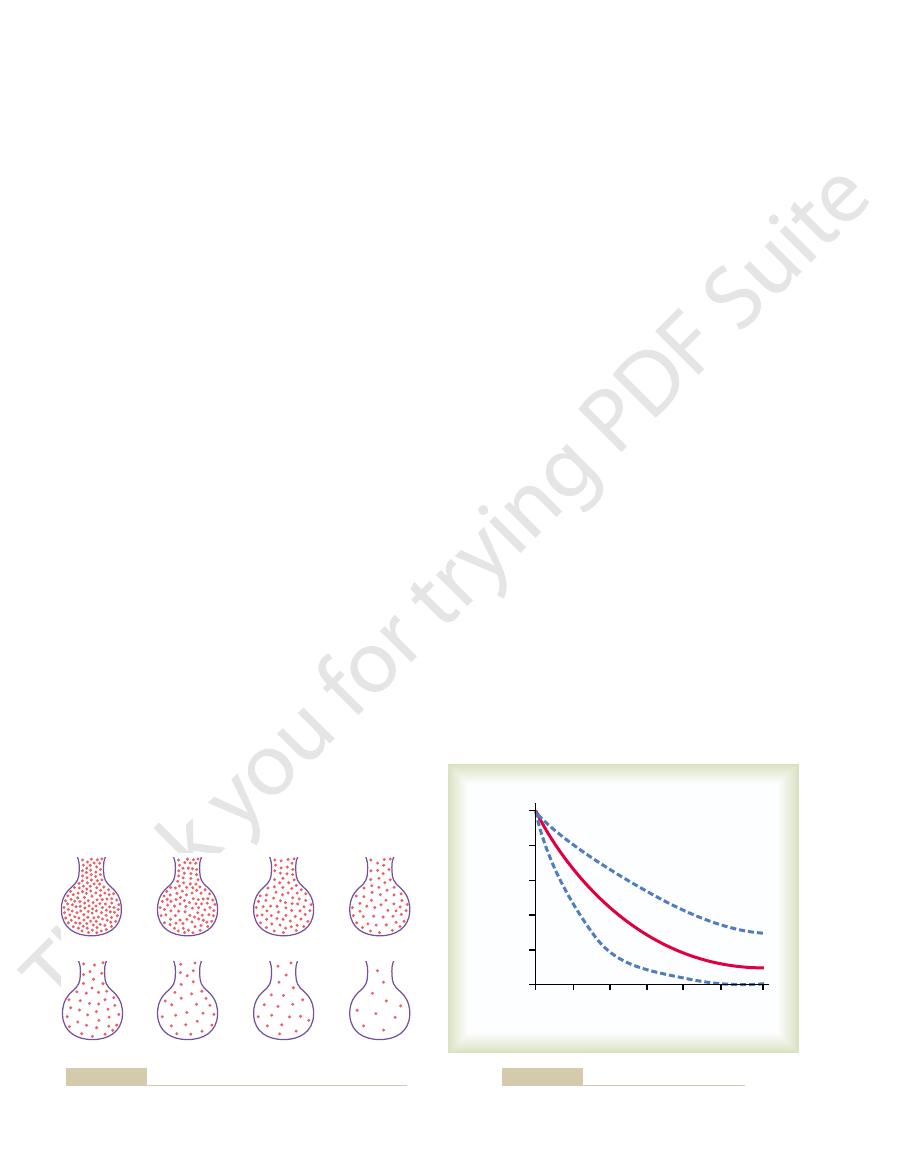
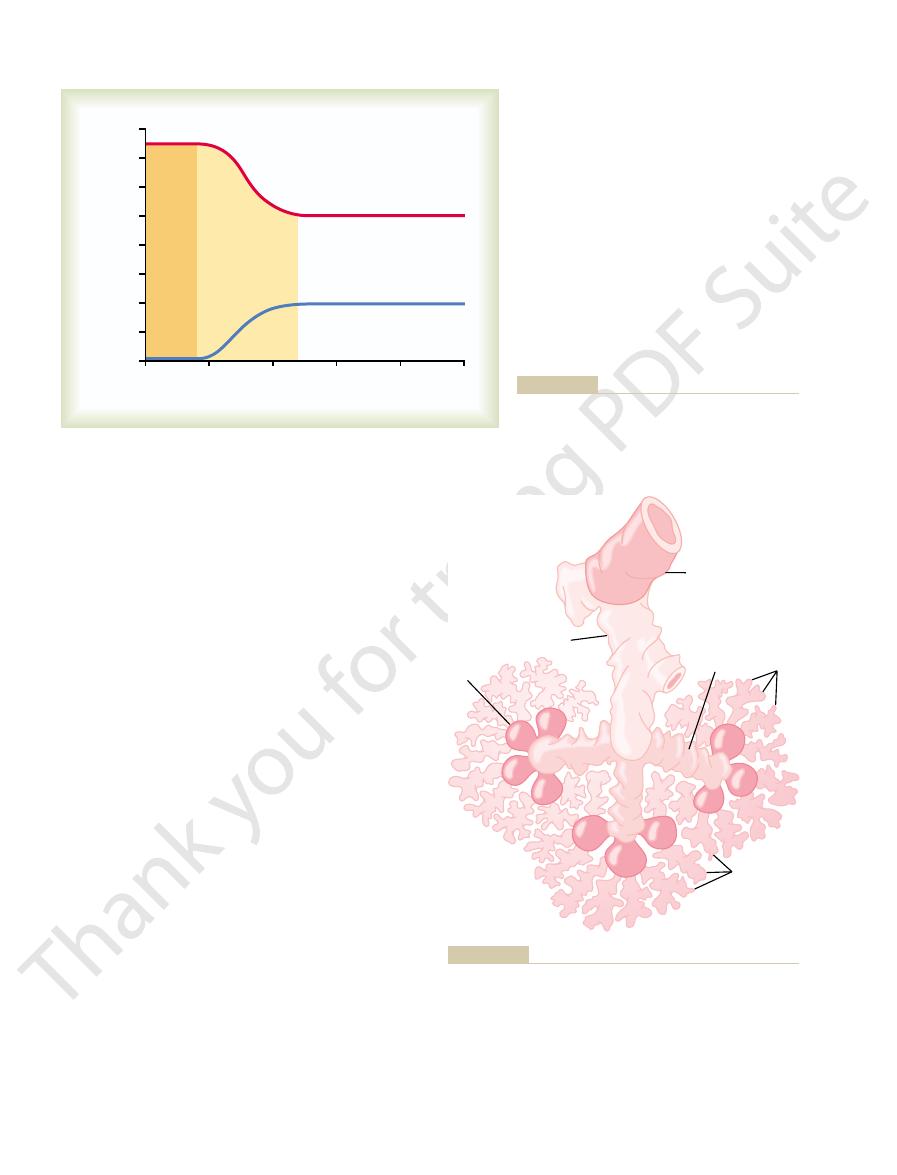
The slow
Importance of the Slow Replacement of Alveolar Air.
is removed in about 8 seconds.
when the rate of ventilation is twice normal, one half
normal, one half the gas is removed in 34 seconds, and
one half the gas is removed in 17 seconds. When a
showing that with normal alveolar ventilation, about
Figure 39
note that even at the end of 16 breaths, the excess
excess amount of a gas is present in the alveoli, but
gure, an
the alveolar air. In the
olar air. Figure 39
breath is only one seventh of the total, so that multi-
alveolar air is expired. Therefore, the volume of alve-
each normal inspiration, and this same amount of old
ration) measures about 2300 milliliters. Yet only 350
In Chapter 37, it was pointed out that the average male
Rate at Which Alveolar Air Is Renewed
sure from 597 to 563 mm Hg.
ed air, and it dilutes the nitrogen partial pres-
of 159 mm Hg in atmospheric air to 149 mm Hg in the
oxygen partial pressure at sea level from an average
all the other gases in the inspired air. Table 39
(760 mm Hg at sea level), this water vapor simply
lar air. Because the total pressure in the alveoli
C is 47 mm Hg, which is there-
The partial pressure of water vapor at a normal
alveoli, it becomes (for all practical purposes) totally
the respiratory surfaces. Even before the air enters the
piratory passages, it is exposed to the
However, as soon as the atmospheric air enters the res-
almost no carbon dioxide and little water vapor.
entirely of nitrogen and oxygen; it normally contains
Table
Humidification of the Air in the Respiratory Passages.
494
Unit VII
Respiration
atmospheric air that enters the respiratory passages is
humidified even before it reaches the alveoli.
39–1 shows that atmospheric air is composed almost
fluids that cover
humidified.
body temperature of 37°
fore the partial pressure of water vapor in the alveo-
cannot rise to more than the atmospheric pressure
dilutes
–1
also shows that humidification of the air dilutes the
humidifi
by Atmospheric Air
functional residual capacity of the lungs (the volume
of air remaining in the lungs at the end of normal expi-
milliliters of new air is brought into the alveoli with
olar air replaced by new atmospheric air with each
ple breaths are required to exchange most of the alve-
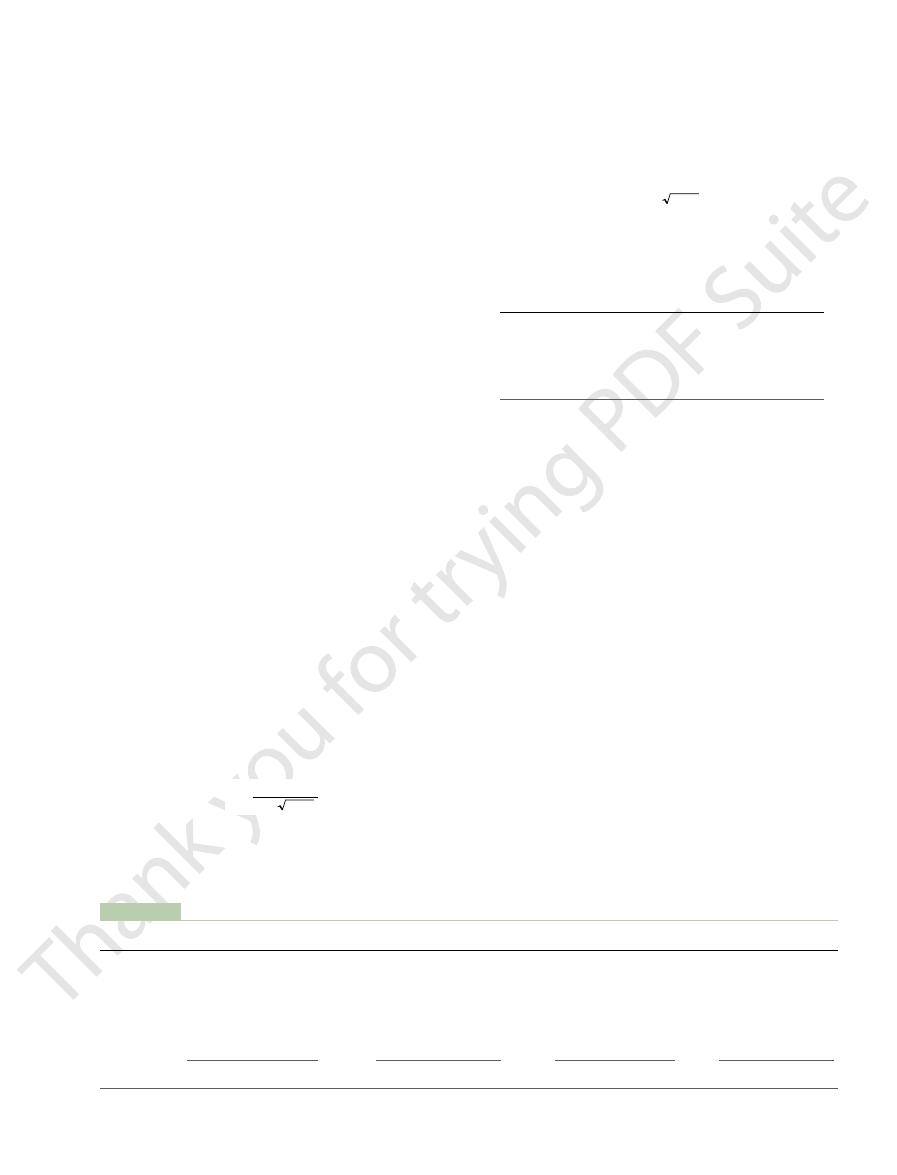
–2 shows this slow rate of renewal of
first alveolus of the fi
gas still has not been completely removed from the
alveoli.
–3 demonstrates graphically the rate at
which excess gas in the alveoli is normally removed,
person’s rate of alveolar ventilation is only one half
replacement of alveolar air is of particular importance
in preventing sudden changes in gas concentrations in
it helps prevent excessive increases and decreases in
interrupted.
Oxygen is continually being absorbed from the alveoli
ually being breathed into the alveoli from the atmos-
the more rapidly new oxygen is breathed into the
(1) the rate of absorption of oxygen into the blood and
(2) the rate of entry of new oxygen into the lungs by
4th breath
12th breath
16th breath
1st breath
2nd breath
3rd breath
8th breath
Expiration of a gas from an alveolus with successive breaths.
Figure 39–2
20
60
10
40
50
0
100
80
60
40
20
0
30
Concentration of gas
(per cent of original concentration)
Time (seconds)
1/2
nor
ma
l alv
eola
r v
e
ntilati
on
2
¥
n
or
m
al
alv
eola
r ventilati
on
N
orm
al
alv
eo
lar
v
entil
a
t
io
n
Rate of removal of excess gas from alveoli.
Figure 39–3
olar air; its overall composition is therefore determined
Therefore, the concentrations and
are excreted per minute). Second,
to the rate of carbon dioxide excretion,
First,
Two other facts are also evident from Figure 39
that is, 40 mm Hg.
Figure 39
is at point A in
At the normal rate of alveolar ventilation of 4.2 L/min,
tion, 200 and 800 ml/min. One curve represents a
lation. Figure 39
body and then carried in the blood to the alveoli; it is
Pressure in the Alveoli
higher than 149 mm Hg, the alveolar P
ed air at this pressure. If the person
air at sea level pressure, because this is the maximum
above 149 mm Hg as
Another effect shown in Figure 39
value of 104 mm Hg.
exercise, the rate of alveolar ventilation must increase
absorbed each minute, as occurs during moderate
4 is point A. The
operating point in Figure 39
and an oxygen consumption of 250 ml/min, the normal
1000 ml/min. At a normal ventilatory rate of 4.2 L/min
250 ml/min, and the other curve represents a rate of
). One
Figure 39
Physical Principles of Gas Exchange; Diffusion of Oxygen and Carbon Dioxide
Chapter 39
495
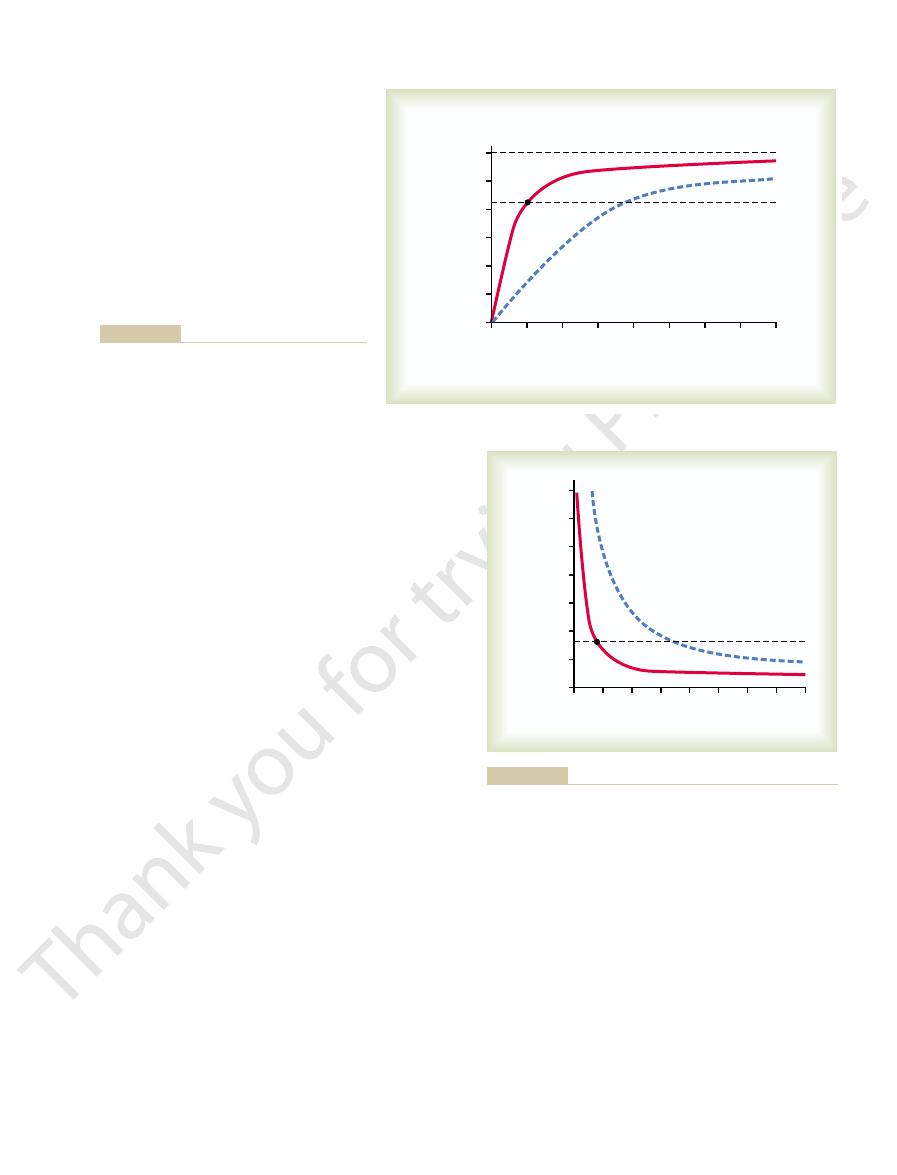
–4 shows the effect of both alveolar venti-
lation and rate of oxygen absorption into the blood on
the alveolar partial pressure of oxygen (Po
2
curve represents oxygen absorption at a rate of
–
figure
also shows that when 1000 milliliters of oxygen is being
fourfold to maintain the alveolar Po
2
at the normal
–4 is that an
extremely marked increase in alveolar ventilation can
never increase the alveolar Po
2
long as the person is breathing normal atmospheric
Po
2
in humidifi
breathes gases that contain partial pressures of oxygen
o
2
can approach
these higher pressures at high rates of ventilation.
CO
2
Concentration and Partial
Carbon dioxide is continually being formed in the
continually being removed from the alveoli by venti-
–5 shows the effects on the alveolar
partial pressure of carbon dioxide (Pco
2
) of both alve-
olar ventilation and two rates of carbon dioxide excre-
normal rate of carbon dioxide excretion of 200 ml/min.
the operating point for alveolar Pco
2
–5—
–5:
the alveolar P
CO
2
increases directly in proportion
as represented
by the fourfold elevation of the curve (when 800
milliliters of CO
2
the alveolar P
CO
2
decreases in inverse proportion to
alveolar ventilation.
partial pressures of both oxygen and carbon dioxide in
the alveoli are determined by the rates of absorption
or excretion of the two gases and by the amount of
alveolar ventilation.
Expired Air
Expired air is a combination of dead space air and alve-
5
20
40
10
15
25
0
150
125
100
75
50
25
0
35
30
Upper limit at maximum ventilation
250 ml O
2
/min
1000 ml O
2
/min
Normal alveolar P
O
2
Alveolar partial pressure
of oxygen (mm Hg)
Alveolar ventilation (L/min)
A
250 ml/min and 1000 ml/min. Point A is the normal
two rates of oxygen absorption from the alveoli—
Effect of alveolar ventilation on the alveolar P
Figure 39–4
O
2
at
operating point.
5
20
40
10
15
25
Normal alveolar P
CO
2
0
175
150
125
100
75
50
25
0
35
30
A
200 ml CO
2
/min
800 ml CO
2
/min
Alveolar partial pressure
of CO
2
(mm Hg)
Alveolar ventilation (L/min)
min. Point A is the normal operating point.
carbon dioxide excretion from the blood—800 ml/min and 200 ml/
Effect of alveolar ventilation on the alveolar P
Figure 39–5
CO
2
at two rates of
pulmonary membrane.
respiratory membrane,
merely in the alveoli themselves. All these membranes
branes of all the terminal portions of the lungs, not
laries. Further, gas exchange between the alveolar air
Thus, it is obvious that the alveolar gases are in very
the capillary plexus, the
8. Indeed, because of the extensiveness of
Figure 39
network of interconnecting capillaries, shown in
thin, and between the alveoli is an almost solid
about 0.2 millimeter. The alveolar walls are extremely
lungs, and each alveolus has an average diameter of
There are about 300 million alveoli in the two
respiratory bronchiole, alveolar ducts, atria,
), which is composed
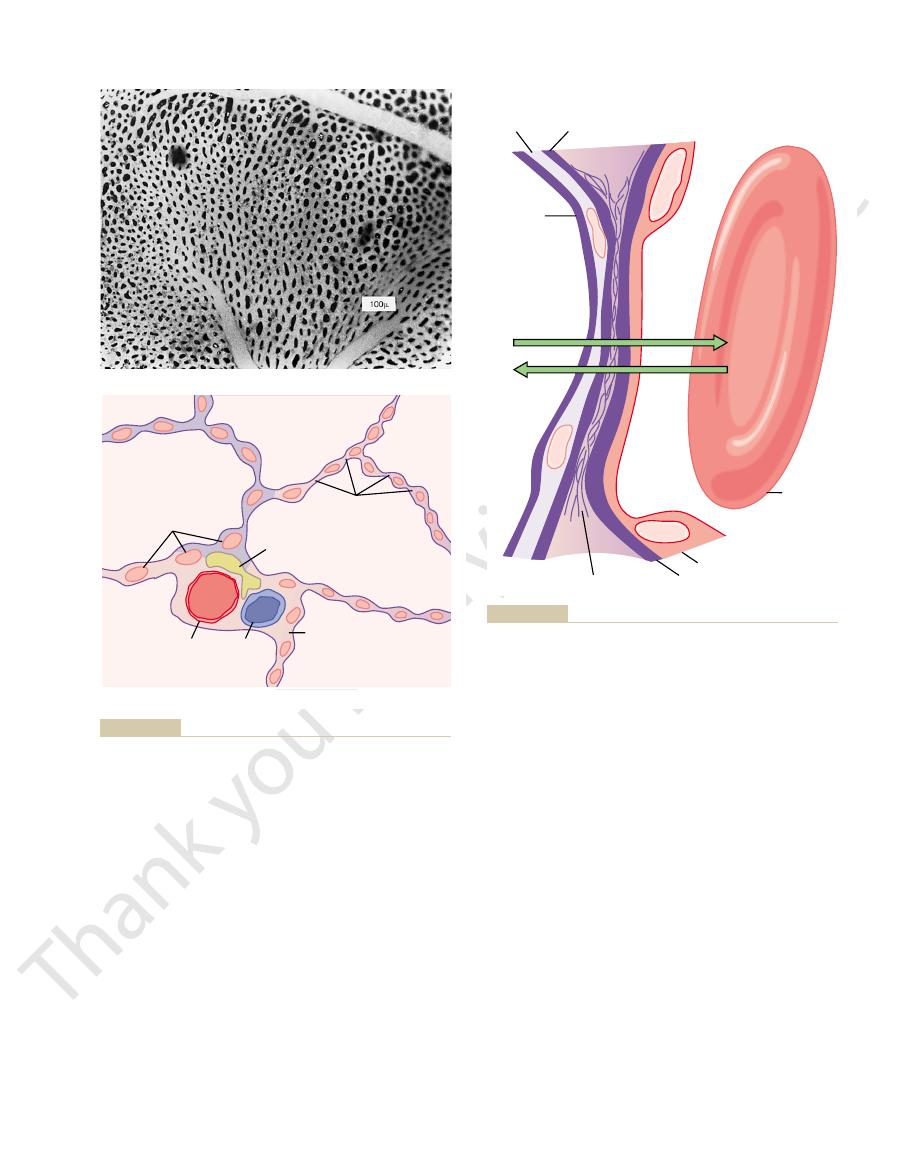
7 shows the
Figure 39
Respiratory Unit.
the Respiratory Membrane
Diffusion of Gases Through
ed atmospheric air.
is, concentrations between those of alveolar air and
pressures approximately as shown in Table 39
and alveolar air, has gas concentrations and partial
Normal expired air, containing both dead space air
air.
expired at the end of expiration. Therefore, the method
1. Then, pro-
ed air, as shown in Table 39
dead space air from the respiratory passageways, is
rst portion of this air, the
course of expiration. The
air and (2) the amount that is alveolar air. Figure 39
496
Unit VII
Respiration
by (1) the amount of the expired air that is dead space
–6
shows the progressive changes in oxygen and carbon
dioxide partial pressures in the expired air during the
fi
typical humidifi
–
gressively more and more alveolar air becomes mixed
with the dead space air until all the dead space air has
finally been washed out and nothing but alveolar air is
of collecting alveolar air for study is simply to collect
a sample of the last portion of the expired air after
forceful expiration has removed all the dead space
–1—that
humidifi
–
respiratory unit
(also called “respiratory lobule”
of a
and
alveoli.
–
flow of blood in the alveolar
wall has been described as a “sheet” of flowing blood.
close proximity to the blood of the pulmonary capil-
and the pulmonary blood occurs through the mem-
are collectively known as the
also called the
100
200
Carbon dioxide (P
CO
2
)
Oxygen (P
O
2
)
0
160
140
120
100
80
60
40
20
0
Milliliters of air expired
Pressures of O
2
and CO
2
(mm Hg)
500
400
300
Alveolar air
Alveolar air
and dead
space air
Dead
space
air
various portions of normal expired air.
Oxygen and carbon dioxide partial pressures in the
Figure 39–6
Terminal bronchiole
Atrium
Alveoli
Alveolar
duct
Alveolar sacs
Respiratory bronchiole
Respiratory unit. (Redrawn from Miller WS: The Lung. Springfield,
Figure 39–7
Ill: Charles C Thomas, 1947.)
the alveolus and the red cell. This, too, increases the
cell membrane usually touches the capillary wall, so
blood cells must squeeze through them. The red blood
is only about 5 micrometers, which means that red
The average diameter of the pulmonary capillaries
of oxygen and carbon dioxide.
oor, and it is easy
lungs at any given instant is 60 to 140 milliliters. Now
The total quantity of blood in the capillaries of the
square meters in the normal adult human male. This is
histological studies, it has been estimated that the total
micrometer, except where there are cell nuclei. From
is as little as 0.2 micrometer, and it averages about 0.6
Despite the large number of layers, the overall
6. The capillary endothelial membrane
5. A capillary basement membrane that in many
4. A thin interstitial space between the alveolar
3. An epithelial basement membrane
2. The alveolar epithelium composed of thin
1. A layer of
in the opposite direction. Note the following different
section on the left and a red blood cell on the right. It
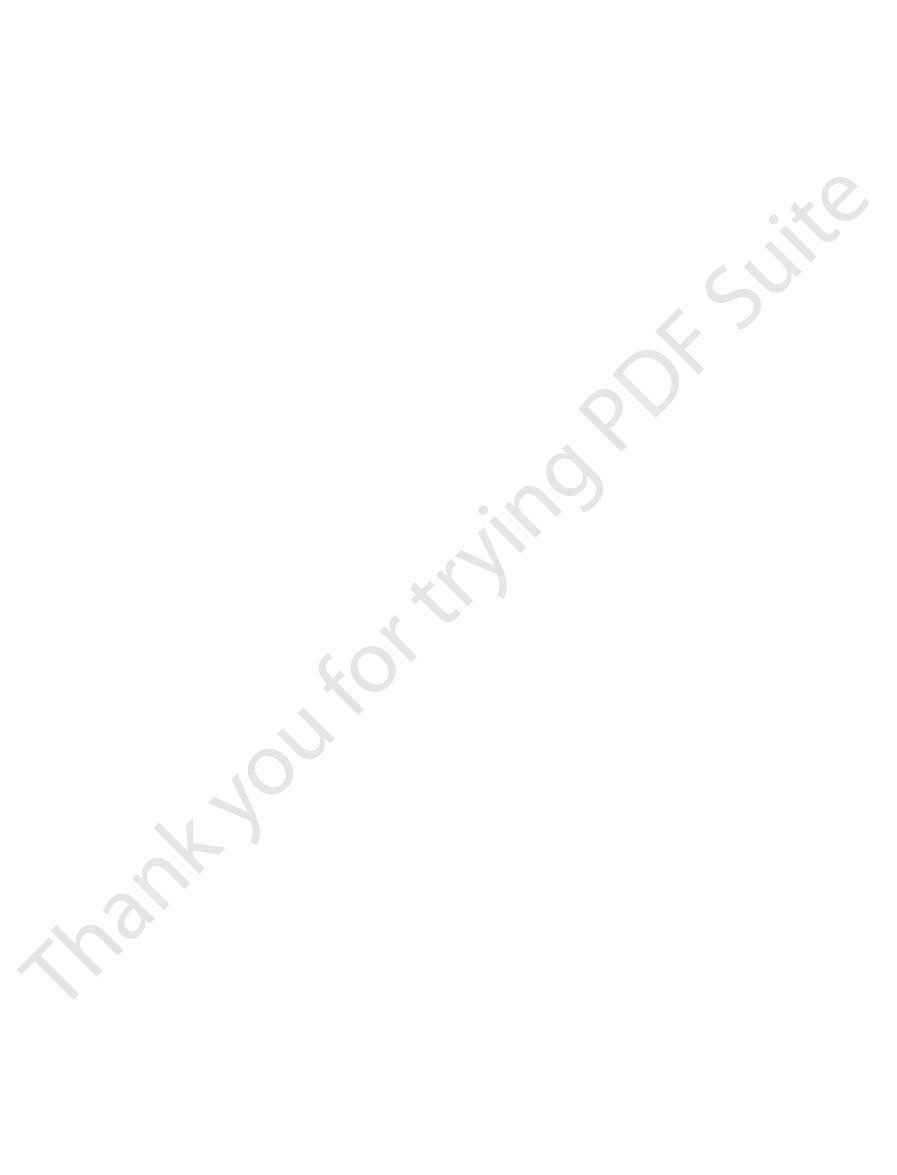
Figure 39
Respiratory Membrane.
Physical Principles of Gas Exchange; Diffusion of Oxygen and Carbon Dioxide
Chapter 39
497
–9 shows the ultrastruc-
ture of the respiratory membrane drawn in cross
also shows the diffusion of oxygen from the alveolus
into the red blood cell and diffusion of carbon dioxide
layers of the respiratory membrane:
fluid lining the alveolus and containing
surfactant that reduces the surface tension of the
alveolar fluid
epithelial cells
epithelium and the capillary membrane
places fuses with the alveolar epithelial basement
membrane
thickness of the respiratory membrane in some areas
surface area of the respiratory membrane is about 70
equivalent to the floor area of a 25–by-30–foot room.
imagine this small amount of blood spread over the
entire surface of a 25–by-30–foot fl
to understand the rapidity of the respiratory exchange
that oxygen and carbon dioxide need not pass through
significant amounts of plasma as they diffuse between
rapidity of diffusion.
Lymphatic
Vein
Artery
Perivascular
interstitial space
Interstitial space
Capillaries
vessel
Alveolus
Alveolus
Alveolus
B
A
Alveolus
North-Holland Division.)
Reproduced by permission of ASP Biological and Medical Press,
and small blood vessels in frog lung. Respir Physiol 7:150, 1969.
Maloney JE, Castle BL: Pressure-diameter relations of capillaries
From
tional view of alveolar walls and their vascular supply. (
Cross-sec-
Surface view of capillaries in an alveolar wall.
Figure 39–8
A,
B,
A,
Diffusion
Diffusion
Alveolus
Capillary
Capillary basement membrane
Capillary endothelium
Epithelial
basement
membrane
Alveolar
epithelium
Fluid and
surfactant
layer
Interstitial space
Oxygen
Red blood
cell
Carbon dioxide
cross section.
Ultrastructure of the alveolar respiratory membrane, shown in
Figure 39–9
The diffusing capac-
this chapter. Therefore, during exercise, oxygenation of
perfusion ratio,
alveolar capillaries with blood, called the
oxygen can diffuse; and (2) a better match between
extra dilation of already open capillaries, thereby
several factors, among which are (1) opening up of
under resting conditions. This increase is caused by
mm Hg, which is three times the diffusing capacity
in young men to a maximum of about 65 ml/min/
ventilation, the diffusing capacity for oxygen increases
normal, quiet breathing is about 11 mm Hg. Multipli-
what does this mean? The mean oxygen pressure
. In functional terms,
21 ml/min/mm Hg
diffusing capacity for oxygen
In the average young man,
this diffusing capacity.
1 mm Hg.
brane each minute for a partial pressure difference of
membrane’s diffusing capacity,
The ability of the respiratory membrane to exchange
Diffusing Capacity of the
from the blood into the alveoli occurs.
the alveoli, as is true for carbon dioxide, net diffusion
alveoli into the blood occurs; when the pressure of the
the blood, as is true for oxygen, net diffusion from the
membrane. When the partial pressure of a gas in the
in the opposite direction. Therefore, the difference
alveolar surface of the membrane in unit time, and the
gas in the pulmonary capillary blood. The partial pres-
The
oxygen. Oxygen diffuses about twice as rapidly as
earlier. Therefore, for a given pressure difference,
exactly the same as that in water, for reasons explained
The rate
in the membrane and, inversely, on the
The
gases.
competitive sports and other strenuous exercise, even
even under resting conditions,
cant degree,
about one third to one fourth normal, exchange of
walls. When the total surface area is decreased to
larger than the original alveoli, but the total surface
walls. Therefore, the new alveolar chambers are much
the alveoli coalesce, with dissolution of many alveolar
area to one half normal. Also, in
greatly decreased by many conditions. For instance,
The
cantly with normal respiratory exchange of gases.
membrane, any factor that increases the thickness to
brane. Because the rate of diffusion through the mem-
brosis of the lungs, which can increase the
uid. Also, some pulmonary diseases
for instance, as a result of edema
thickness of the respiratory membrane
The
the two sides of the membrane.
of the gas in the substance of the membrane, and
surface area of the membrane,
thickness of the membrane,
respiratory membrane. Thus, the factors that deter-
in water, one can apply the same principles and math-
Factors That Affect the Rate
498
Unit VII
Respiration
of Gas Diffusion Through the
Respiratory Membrane
Referring to the earlier discussion of diffusion of gases
ematical formulas to diffusion of gases through the
mine how rapidly a gas will pass through the mem-
brane are (1) the
(2) the
(3) the diffusion coeffi-
cient
(4) the partial pressure difference of the gas between
occa-
sionally increases—
fluid in the interstitial space of the membrane and in
the alveoli—so that the respiratory gases must then
diffuse not only through the membrane but also
through this fl
cause fi
thickness of some portions of the respiratory mem-
brane is inversely proportional to the thickness of the
more than two to three times normal can interfere sig-
nifi
surface area of the respiratory membrane can be
removal of an entire lung decreases the total surface
emphysema, many of
area of the respiratory membrane is often decreased
as much as fivefold because of loss of the alveolar
gases through the membrane is impeded to a signifi-
and during
the slightest decrease in surface area of the lungs can
be a serious detriment to respiratory exchange of
diffusion coefficient for transfer of each gas
through the respiratory membrane depends on the
gas’s solubility
square root of the gas’s molecular weight.
of diffusion in the respiratory membrane is almost
carbon dioxide diffuses about 20 times as rapidly as
nitrogen.
pressure difference across the respiratory mem-
brane is the difference between the partial pressure of
the gas in the alveoli and the partial pressure of the
sure represents a measure of the total number of mol-
ecules of a particular gas striking a unit area of the
pressure of the gas in the blood represents the number
of molecules that attempt to escape from the blood
between these two pressures is a measure of the net
tendency for the gas molecules to move through the
alveoli is greater than the pressure of the gas in
gas in the blood is greater than the partial pressure in
Respiratory Membrane
a gas between the alveoli and the pulmonary blood
is expressed in quantitative terms by the respiratory
which is defined as
the volume of a gas that will diffuse through the mem-
All the factors discussed earlier that affect
diffusion through the respiratory membrane can affect
Diffusing Capacity for Oxygen.
the
under resting condi-
tions averages
difference across the respiratory membrane during
cation of this pressure by the diffusing capacity (11
¥
21) gives a total of about 230 milliliters of oxygen dif-
fusing through the respiratory membrane each minute;
this is equal to the rate at which the resting body uses
oxygen.
Change in Oxygen Diffusing Capacity During Exercise.
During strenuous exercise or other conditions that
greatly increase pulmonary blood flow and alveolar
many previously dormant pulmonary capillaries or
increasing the surface area of the blood into which the
the ventilation of the alveoli and the perfusion of the
ventilation-
which is explained in detail later in
the blood is increased not only by increased alveolar
ventilation but also by greater diffusing capacity of
the respiratory membrane for transporting oxygen into
the blood.
Diffusing Capacity for Carbon Dioxide.
ity for carbon dioxide has never been measured
the respiratory membrane of the affected alveoli, which
nity, there is no exchange of gases through
nity. At a ratio of either
), the ratio V
is zero. Or, at the other extreme,
alveolus, the V
) is zero, yet there is still perfusion (Q
lation (V
) is also said to be normal. When the venti-
normal for the same alveolus, the ventilation-perfusion
. When V
is expressed as V
In quantitative terms, the ventilation-perfusion ratio
ventilation-perfusion ratio.
ow. This
parts of the lungs. Therefore, a highly quantitative
ow, but
brane is seriously impaired, and the person may suffer
conditions, gas exchange through the respiratory mem-
ow but little or no ventilation. In either of these
ow, whereas other areas may have excellent
some extent, and especially in many lung diseases, some
the same for each alveolus. However, even normally to
tory membrane. These earlier discussions made the
in the alveoli: (1)
In the early part of this chapter, we learned that two
Perfusion Ratio on Alveolar
Effect of the Ventilation-
21 ml/min/mm Hg.
diffusing capacity for oxygen is 1.23 times this, or
in young men at rest is 17 ml/min/mm Hg, and the
oxygen is 1.23 times that for carbon monoxide. Thus,
oxygen diffusing capacity, the value is multiplied by a
To convert carbon monoxide diffusing capacity to
capacity.
alveolar carbon monoxide partial pressure, one can
Then, by measuring the volume of carbon monoxide
equal to its partial pressure in the alveolar air sample.
has time to build up. Therefore, the pressure difference
sure in the blood is essentially zero, because hemoglobin
priate alveolar air samples. The carbon monoxide pres-
breathed into the alveoli, and the partial pressure of the
the following: A small amount of carbon monoxide is
this. The principle of the carbon monoxide method is
oxygen diffusing capacity directly, physiologists usually
To obviate the dif
imental basis.
capacity by such a direct procedure, except on an exper-
uptake by the blood. However, measuring the P
pulmonary capillary blood, and (3) the rate of oxygen
, (2) P
The oxygen diffusing capacity can be calculated
capacity of each of these gases.
oxygen, and carbon dioxide at rest and during exercise,
calculated diffusing capacities of carbon monoxide,
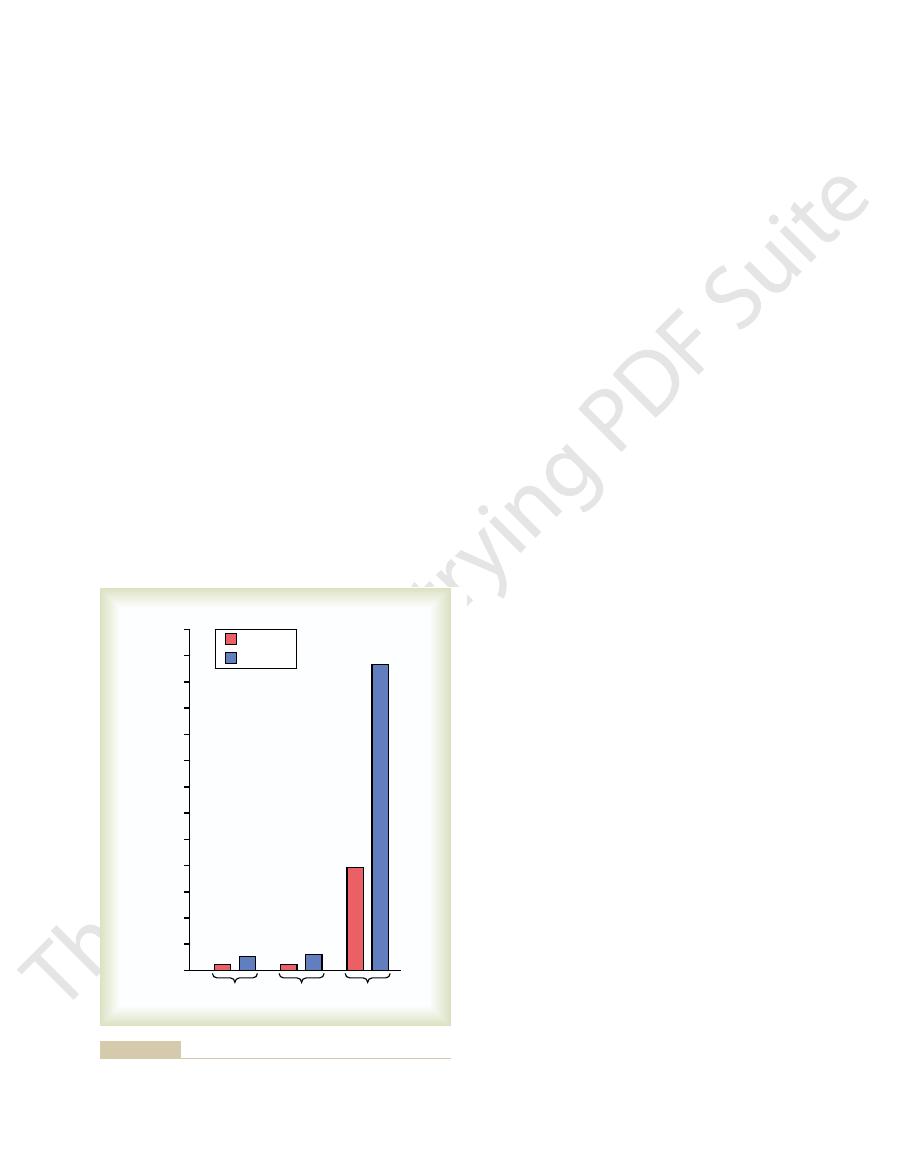
min/mm Hg. Figure 39
mm Hg and during exercise of about 1200 to 1300 ml/
is slightly more than 20 times that of oxygen, one
gas. Because the diffusion coef
Nevertheless, measurements of diffusion of other
available techniques, this difference is too small to be
average difference is less than 1 mm Hg
culty: Carbon
Physical Principles of Gas Exchange; Diffusion of Oxygen and Carbon Dioxide
Chapter 39
499
because of the following technical diffi
dioxide diffuses through the respiratory membrane so
rapidly that the average Pco
2
in the pulmonary blood
is not far different from the Pco
2
in the alveoli—the
—and with the
measured.
gases have shown that the diffusing capacity varies
directly with the diffusion coefficient of the particular
ficient of carbon dioxide
would expect a diffusing capacity for carbon dioxide
under resting conditions of about 400 to 450 ml/min/
–10 compares the measured or
showing the extreme diffusing capacity of carbon
dioxide and the effect of exercise on the diffusing
Measurement of Diffusing Capacity—The Carbon Monoxide
Method.
from measurements of (1) alveolar Po
2
o
2
in the
o
2
in the
pulmonary capillary blood is so difficult and so impre-
cise that it is not practical to measure oxygen diffusing
ficulties encountered in measuring
measure carbon monoxide diffusing capacity instead
and then calculate the oxygen diffusing capacity from
carbon monoxide in the alveoli is measured from appro-
combines with this gas so rapidly that its pressure never
of carbon monoxide across the respiratory membrane is
absorbed in a short period and dividing this by the
determine accurately the carbon monoxide diffusing
factor of 1.23 because the diffusion coefficient for
the average diffusing capacity for carbon monoxide
Gas Concentration
factors determine the Po
2
and the Pco
2
the rate of alveolar ventilation and (2) the rate of trans-
fer of oxygen and carbon dioxide through the respira-
assumption that all the alveoli are ventilated equally
and that blood flow through the alveolar capillaries is
areas of the lungs are well ventilated but have almost
no blood fl
blood fl
severe respiratory distress despite both normal total
ventilation and normal total pulmonary blood fl
with the ventilation and blood flow going to different
concept has been developed to help us understand res-
piratory exchange when there is imbalance between
alveolar ventilation and alveolar blood fl
concept is called the
.
a/Q
.
.
a (alveolar ventilation) is
normal for a given alveolus and Q
.
(blood flow) is also
ratio (V
.
a/Q
.
.
a
.
) of the
.
a/Q
.
when there is adequate ventilation (V
.
a) but zero perfu-
sion (Q
.
.
a/Q
.
is infi
zero or infi
1300
1200
1100
1000
900
800
700
600
500
400
300
200
100
0
CO
2
O
2
CO
Resting
Exercise
Diffusing capacity (ml/min/mm Hg)
exercise.
dioxide in the normal lungs under resting conditions and during
Diffusing capacities
Figure 39–10
for carbon monoxide, oxygen, and carbon
ow is low, there is far more available
When ventilation of some of the alveoli is great but
(When V
through the lungs.
amount of blood that fails to be oxygenated
The greater the physiologic shunt, the greater the
concentration of oxygen in the arterial blood, and C
ventilation-perfusion ratio, Ca
is cardiac output per minute, Ci
minute, Q
these values, the physiologic shunt can be calculated by
simultaneous measurement of cardiac output. From
both mixed venous blood and arterial blood, along with
This physiologic
The total quantitative amount of shunted blood per
too, is unoxygenated, shunted blood.
ies, normally about 2 per cent of the cardiac output; this,
Also, some additional blood
not become oxygenated. This fraction is called
laries. Therefore, a certain fraction of the venous
is below normal, there is inadequate
Whenever V
Is Below Normal)
is 40 mm Hg.
is 104 mm Hg and
is normal. At this point, P
is zero. Also plotted on the curve
mm Hg while P
to be 149
ity, point I represents inspired air, showing P
At the other end of the curve, when V
is 45 mm Hg, which are the
is 40 mm Hg and the P
equals zero. At this point, the P
air at sea-level pressure. Thus, point v
binations between the limits of V
diagram. The curve in
11, called the P
shown in graphical form, as demonstrated in Figure
The concepts presented in the preceding sections can be
averages 40 mm Hg.
averages 104 mm Hg and the P
0 mm Hg in inspired air. Thus, under normal conditions,
40 mm Hg, in contrast to 45 mm Hg in venous blood and
lies between two extremes; it is normally
and that of venous blood (40 mm Hg). Likewise,
which lies between that of the inspired air (149 mm Hg)
is normally at a level of 104 mm Hg,
olar perfusion), exchange of oxygen and carbon dioxide
When there is both normal alveolar ventilation
of 0 mm Hg, these will be the partial pressures of these
of 149 mm Hg and a P
ed air has a P
dioxide from the blood. And because normal inspired
ed inspired air. That is, the air that is inspired
venous blood, the alveolar air becomes equal to the
to bring carbon dioxide to the alveoli. Therefore, instead
from the effect when V
sures when V
The effect on the alveolar gas partial pres-
Equals Infinity.
Therefore, these are also the normal partial pressures of
of 45 mm Hg.
of 40 mm Hg and a P
Chapter 40, we will learn that the normal venous blood
blood with which the alveolar gases equilibrate. In
from the systemic circulation, it is the gases in this
and the alveolar air. Because the blood that perfuses
that is, without
When V
extremes.
explains the importance of this concept. Therefore, let
500
Unit VII
Respiration
us explain the respiratory consequences of these two
Alveolar Oxygen and Carbon Dioxide Partial Pressures When V
.
A
/Q
.
Equals Zero.
.
a/Q
.
is equal to zero—
any alveolar ventilation—the air in the alveolus
comes to equilibrium with the blood oxygen and carbon
dioxide because these gases diffuse between the blood
the capillaries is venous blood returning to the lungs
(v¯) has a Po
2
co
2
these two gases in alveoli that have blood flow but no
ventilation.
Alveolar Oxygen and Carbon Dioxide Partial Pressures When V
.
A
/Q
.
.
a/Q
.
equals infinity is entirely different
.
a/Q
.
equals zero because now
there is no capillary blood flow to carry oxygen away or
of the alveolar gases coming to equilibrium with the
humidifi
loses no oxygen to the blood and gains no carbon
and humidifi
o
2
co
2
two gases in the alveoli.
Gas Exchange and Alveolar Partial Pressures When V
.
A
/Q
.
Is
Normal.
and normal alveolar capillary blood flow (normal alve-
through the respiratory membrane is nearly optimal,
and alveolar Po
2
alveolar Pco
2
the alveolar air Po
2
co
2
P
O
2
-P
CO
2
, V
.
A
/Q
.
Diagram
39–
o
2
-Pco
2
, V
.
a/Q
.
the diagram represents all possible Po
2
and Pco
2
com-
.
a/Q
.
equals zero and
V
.
a/Q
.
equals infinity when the gas pressures in the
venous blood are normal and the person is breathing
¯ is the plot of Po
2
and Pco
2
when V
.
a/Q
.
o
2
co
2
values in normal venous blood.
.
a/ Q
.
equals infin-
o
2
co
2
is the point that represents normal alveolar air when
V
.
a/Q
.
o
2
Pco
2
Concept of “Physiologic Shunt”
(When V
.
A
/Q
.
.
a/Q
.
ventilation to provide the oxygen needed to fully oxy-
genate the blood flowing through the alveolar capil-
blood passing through the pulmonary capillaries does
shunted
blood.
flows through
bronchial vessels rather than through alveolar capillar-
minute is called the physiologic shunt.
shunt is measured in clinical pulmonary function labo-
ratories by analyzing the concentration of oxygen in
the following equation:
in which Q
.
ps is the physiologic shunt blood flow per
.
t
O
2
is the con-
centration of oxygen in the arterial blood if there is an
“ideal”
O
2
is the measured
v¯
O
2
is the measured concentration of oxygen in the mixed
venous blood.
as it passes
Concept of the “Physiologic Dead
Space”
.
A
/Q
.
Is Greater
Than Normal)
alveolar blood fl
oxygen in the alveoli than can be transported away from
Ci
C
Ci
Ca
Q
.
Q
.
O
O
O
O
2
2
2
2
ps
t
v
=
-
-
.
0
20
40
60
80 100 120 140 160
50
40
30
20
10
(P
O
2
= 40)
(P
CO
2
= 45)
Normal alveolar
air
(P
O
2
= 104)
(P
CO
2
= 40)
(P
O
2
= 149)
(P
CO
2
= 0)
I
V
A
/Q = 0
V
A
/Q = Normal
v
V
A
/Q =
∞
P
CO
2
(mm Hg)
P
O
2
(mm Hg)
Normal P
Figure 39–11
O
2
-P
CO
2
, V
.
A
/Q
.
diagram.
causes many of the alveolar walls to be destroyed. Thus,
and resultant emphysema. The emphysema in turn
these persons, this condition eventually becomes so
degrees of bronchial obstruction; in a large share of
space occurs, and the effectiveness of gas exchange now
increases markedly, so that far less physiologic dead
during exercise, blood
for exchanging oxygen and carbon dioxide. However,
In both extremes, inequalities of ventilation and
normally oxygenated, and this represents a
area, a small fraction of the blood fails to become
as low as 0.6 times the ideal value. In this
ow,
At the other extreme, in the bottom of the lung, there
in this area of the lung.
ideal value, which causes a moderate degree of
the lung, V
ably more than ventilation is. Therefore, at the top of
lower part; however, blood
normal person in the upright position, both pulmonary
In a
Abnormalities of Ventilation-
When the physiologic dead space is great, much of the
air.
dioxide in the arterial blood, and
is the average
tidal volume, Pa
is the physiologic dead space, V
in which V
This is measured in the clinical pulmonary function lab-
physiologic dead space.
sageways is also wasted. The sum of these two types of
The ventilation of the
owing blood. Thus, the ventilation of
Physical Principles of Gas Exchange; Diffusion of Oxygen and Carbon Dioxide
Chapter 39
501
the alveoli by the fl
these alveoli is said to be wasted.
anatomical dead space areas of the respiratory pas-
wasted ventilation is called the
oratory by making appropriate blood and expiratory
gas measurements and using the following equation,
called the Bohr equation:
d
phys
t is the
CO
2
is the partial pressure of carbon
partial pressure of carbon dioxide in the entire expired
work of ventilation is wasted effort because so much of
the ventilating air never reaches the blood.
Perfusion Ratio
Abnormal V
.
A
/Q
.
in the Upper and Lower Normal Lung.
capillary blood flow and alveolar ventilation are con-
siderably less in the upper part of the lung than in the
flow is decreased consider-
.
a/Q
.
is as much as 2.5 times as great as the
physio-
logic dead space
is slightly too little ventilation in relation to blood fl
with V
.
a/Q
.
physiologic
shunt.
perfusion decrease slightly the lung’s effectiveness
flow to the upper part of the lung
approaches optimum.
Abnormal V
.
A
/Q
.
in Chronic Obstructive Lung Disease.
Most
people who smoke for many years develop various
severe that they develop serious alveolar air trapping
P
CO
2
e
CO
CO
Pa
P
V
V
Pa
phys
CO
2
2
2
d
t
e
=
-
,
development. Annu Rev Physiol 65:669, 2003.
Williams MC:Alveolar type I cells: molecular phenotype and
Lippincott Williams & Wilkins, 2003.
The Essentials. Baltimore:
West JB: Pulmonary Physiology
cott Williams & Wilkins, 2001.
Integrated, Case-Based Approach. Philadelphia: Lippin-
West JB: Pulmonary Physiology and Pathophysiology: An
Birkhauser Verlag, 1998.
Uhlig S, Taylor AE: Methods in Pulmonary Research. Basel:
& Wilkins, 1964, p 125.
Handbook of Physiology. Sec 3, Vol 1. Baltimore: Williams
the Va/Q concept. In: Fenn WO, Rahn H (eds):
Rahn H, Farhi EE: Ventilation, perfusion, and gas
Sci 19:55, 2004.
complexity: implications for gas exchange. News Physiol
Powell FL, Hopkins SR: Comparative physiology of lung
mice. Am J Physiol Lung Cell Mol Physiol 286:L231, 2004.
Parker JC,Townsley MI: Evaluation of lung injury in rats and
iology. Sec 3, Vol 1. Baltimore: Williams & Wilkins, 1964,
exchange. In: Fenn WQ, Rahn H (eds): Handbook of Phys-
Otis AB: Quantitative relationships in steady-state gas
ogy 8:432, 2003.
and functional properties in health and disease. Respirol-
Knight DA, Holgate ST: The airway epithelium: structural
concept and application. Chest 122:1774, 2002.
Hsia CC: Recruitment of lung diffusing capacity: update of
124:1090, 2003.
heart failure: evidence of a pathophysiologic role. Chest
Guazzi M: Alveolar-capillary membrane dysfunction in
tion. Crit Care Med 32:1240, 2004.
Cole RP: CO
cine. Philadelphia: Mosby, 2002.
Albert R, Spiro S, Jett J: Comprehensive Respiratory Medi-
ability today.
fact, this is the most prevalent cause of pulmonary dis-
their effectiveness to as little as one tenth normal. In
the lungs as gas exchange organs, sometimes reducing
serious physiologic dead space.
Thus, in chronic obstructive lung disease, some areas
gases.
alveolar ventilation, most of the ventilation is wasted
Second, in those areas of the lung where the alveolar
that approaches zero.
unventilated, causing a V
obstructed, the alveoli beyond the obstructions are
. First, because many of the small bronchioles are
two abnormalities occur in smokers to cause abnormal
V
.
a/Q
.
.
a/Q
.
walls have been mainly destroyed but there is still
because of inadequate blood flow to transport the blood
of the lung exhibit serious physiologic shunt, and other
areas exhibit
Both these
conditions tremendously decrease the effectiveness of
References
2
and lung mechanical or gas exchange func-
p 681.
exchange—
—