
activity, and the dreams of slow-wave sleep usually are not remembered. That
sometimes even nightmares do occur during slow-wave sleep. The difference
Although slow-wave sleep is frequently called “dreamless sleep,” dreams and
basal metabolic rate.
there are 10 to 30 per cent decreases in blood pressure, respiratory rate, and
vascular tone and many other vegetative functions of the body. For instance,
then the deep sleep that occurred during the first hour after going to sleep. This
Slow-Wave Sleep
restful, and it is usually associated with vivid dreaming.
episode normally recurs about every 90 minutes. This type of sleep is not so
episodes that occupy about 25 per cent of the sleep time in young adults; each
having been awake for many hours. REM sleep, on the other hand, occurs in
Most sleep during each night is of the slow-wave variety; this is the deep,
that the person is still asleep.
rapid eye movement sleep
quency, as we discuss later, and (2)
slow-wave sleep
of sleep that alternate with each other. They are called (1)
During each night, a person goes through stages of two types
Two Types of Sleep.
follows.
sleep into two entirely different types of sleep that have different qualities, as
of sleep, from very light sleep to very deep sleep; sleep researchers also divide
sciousness from which the person cannot be aroused. There are multiple stages
, which is uncon-
sensory or other stimuli. It is to be distinguished from
sleep.
we present brief surveys of specific states of brain activity, beginning with
systems that are capable of activating large portions of the brain. In this chapter,
brain itself. In Chapter 58, we began a partial dis-
mood such as exhilaration, depression, and fear. All
extreme excitement, and even different levels of
of brain activity, including sleep, wakefulness,
Brain Waves, Epilepsy, Psychoses
States of Brain Activity—Sleep,
C
H
A
P
T
E
R
5
9
739
All of us are aware of the many different states
these states result from different activating
or inhibiting forces generated usually within the
cussion of this subject when we described different
Sleep
Sleep is defined as unconsciousness from which the person can be aroused by
coma
,
because in this type of sleep the brain waves are very strong and very low fre-
(REM sleep),
because in this type of sleep the eyes undergo rapid movements despite the fact
restful sleep that the person experiences during the first hour of sleep after
Most of us can understand the characteristics of deep slow-wave sleep by
remembering the last time we were kept awake for more than 24 hours and
sleep is exceedingly restful and is associated with decrease in both peripheral
between the dreams that occur in slow-wave sleep and those that occur in REM
sleep is that those of REM sleep are associated with more bodily muscle
awake for several days. When only micrograms of this
low-molecular-weight substance that accumulates in
brain ventricular system of another animal. One likely
Other Possible Transmitter Substances Related to Sleep.
causing the intense wakefulness. Indeed, sometimes
pons seem to become released from inhibition, thus
. In both instances, the excita-
medial rostral suprachiasmal area in the
high state of wakefulness. This is also true of bilateral
Lesions in Sleep-Promoting Centers Can Cause Intense Wake-
the diffuse nuclei of the thalamus.
suprachiasmal area, and (2) an occasional area in
part of the hypothalamus, mainly in the
can also promote sleep, including (1) the rostral
3. Stimulation of several regions in the diencephalon
vagus and glossopharyngeal nerves.
can also cause sleep. This nucleus
2. Stimulation of some areas in the
of sleep.
Therefore, it has been assumed that serotonin is a
often cannot sleep for the next several days.
serotonin is administered to an animal, the animal
When a drug that blocks the formation of
including pain, as discussed in Chapter 48. It is
they can inhibit incoming sensory signals,
cord, terminating in the posterior horns where
addition, fibers extend downward into the spinal
and even the neocortex of the cerebrum. In
hypothalamus, most areas of the limbic system,
formation and also upward into the thalamus,
in the midline. Nerve fibers from these nuclei
These
lower half of the pons and in the medulla.
1. The most conspicuous stimulation area for causing
of natural sleep. Some of these areas are the
A Possible Specific Role for Serotonin
Neuronal Centers, Neurohumoral Substances,
brain whose cortex never goes to sleep. In other words,
: it was discovered that transecting
sleep is caused by an active
. An important experiment changed this view
inactive as a result. This was called the
of the upper brain stem, the
Sleep Is Believed to Be Caused by an Active Inhibitory Process.
fore the person is truly asleep.
to be fully aware of his or her surroundings, and there-
the brain is quite active. However, the brain activity is
In summary, REM sleep is a type of sleep in which
paradoxical sleep
those that occur during wakefulness. This type of
much as 20 per cent. The electroencephalogram
6. The brain is highly active in REM sleep, and
the eyes.
These are in addition to the rapid movements of
muscles, irregular muscle movements do occur.
5. Despite the extreme inhibition of the peripheral
state.
irregular, which is characteristic of the dream
4. Heart rate and respiratory rate usually become
spinal muscle control areas.
depressed, indicating strong inhibition of the
3. Muscle tone throughout the body is exceedingly
the morning during an episode of REM sleep.
sensory stimuli than during deep slow-wave sleep,
2. The person is even more difficult to arouse by
active bodily muscle movements.
1. It is usually associated with active dreaming and
There are several important characteristics of REM
increase.
through the night, the durations of the REM bouts
Conversely, as the person becomes more rested
bout of REM sleep is short, and it may even be absent.
90 minutes. When the person is extremely sleepy, each
5 to 30 minutes usually appear on the average every
In a normal night of sleep, bouts of REM sleep lasting
in memory does not occur.
is, during slow-wave sleep, consolidation of the dreams
The Nervous System: C. Motor and Integrative Neurophysiology
740
Unit XI
REM Sleep (Paradoxical Sleep,
Desynchronized Sleep)
sleep:
and yet people usually awaken spontaneously in
overall brain metabolism may be increased as
(EEG) shows a pattern of brain waves similar to
sleep is also called
because it is
a paradox that a person can still be asleep despite
marked activity in the brain.
not channeled in the proper direction for the person
Basic Theories of Sleep
An earlier theory of sleep was that the excitatory areas
reticular activating system,
simply fatigued during the waking day and became
passive theory
of sleep
to the current belief that
inhibitory process
the brain stem at the level of the midpons creates a
there seems to be some center located below the mid-
pontile level of the brain stem that is required to cause
sleep by inhibiting other parts of the brain.
and Mechanisms That Can Cause Sleep—
Stimulation of several specific areas of the brain
can produce sleep with characteristics near those
following:
almost natural sleep is the raphe nuclei in the
nuclei are a thin sheet of special neurons located
spread locally in the brain stem reticular
also known that many nerve endings of fibers
from these raphe neurons secrete serotonin.
transmitter substance associated with production
nucleus of the
tractus solitarius
is the termination in the medulla and pons for
visceral sensory signals entering by way of the
fulness.
Discrete lesions in the raphe nuclei lead to a
lesions in the
anterior hypothalamus
tory reticular nuclei of the mesencephalon and upper
lesions of the anterior hypothalamus can cause such
intense wakefulness that the animal actually dies of
exhaustion.
Experiments have shown that the cerebrospinal fluid
as well as the blood or urine of animals that have been
kept awake for several days contains a substance or
substances that will cause sleep when injected into the
substance has been identified as muramyl peptide, a
the cerebrospinal fluid and urine in animals kept
such as epilepsy, which is discussed later.
other times, distinct patterns do appear, some of which
no specific pattern can be discerned in the EEG. At
Much of the time, the brain waves are irregular, and
of the cerebral cortex, and the waves change markedly
50 or more per second. The character of the waves is
surface of the scalp range from 0 to 200 microvolts, and
The intensities of brain waves recorded from the
potentials, shown in Figure 59–1, are called
The undulations in the recorded electrical
psychoses.
, or brain diseases such as
Brain Waves
remain a mystery, and they are the subject of much
. The specific physiologic functions of sleep
We might postulate that
lose their “baseline” of operation; it is reasonable to
longed use, because computers of this type gradually
“rezeroing” of electronic analog computers after pro-
central nervous system. This might be likened to the
normal “balance” among the different functions of the
Therefore, we can assume that sleep in multiple ways
irritable or even psychotic after forced wakefulness.
wakeful period, but in addition, a person can become
We are all familiar with the increased sluggishness
causes abnormal behavioral activities.
functions of the central nervous system. Prolonged
Lack of sleep certainly does, however, affect the
wakefulness cycle.
wakefulness cycle below the transection) shows no
effects on other functional systems of the body. The
first, effects on the nervous system itself, and second,
Physiologic Effects of Sleep
duced by bodily physical activity.
pied with a thought, and the wakefulness that is pro-
that occurs when a person’s mind becomes preoccu-
to sleep. It could also explain arousal, the insomnia
This overall theory could explain the rapid transi-
back to sleep.
take over, leading to rapid transition from wakefulness
cephalic reticular nuclei and the cerebral cortex fades,
the positive feedback cycle between the mesen-
system presumably become fatigued. Consequently,
hours, even the neurons themselves in the activating
Then, after the brain remains activated for many
feedback activity.
tendency to sustain itself because of all this positive
Therefore, once wakefulness begins, it has a natural
reticular activating nuclei to activate them still further.
positive feedback
the peripheral nervous system, both of which send
active. This in turn excites both the cerebral cortex and
nuclei are released from inhibition, which allows the
activated, the mes-
When the sleep centers are
cycle.
There is as yet no explanation. Therefore, we can let
reciprocal operation of the sleep-wakefulness cycle.
related to sleep. They have not explained the cyclical,
neuronal areas, transmitters, and mechanisms that are
The preceding discussions have merely identified
Cycle Between Sleep and Wakefulness
wakefulness.
brain regions in REM sleep, even though the signals
activate many portions of the brain. This theoretically
mation might, through their extensive efferent fibers,
increase the occurrence of REM sleep. Therefore, it
However, drugs that mimic the action of acetylcholine
Why slow-wave sleep is
fluid that lead to sleep.
awake for days. It is possible that prolonged wakeful-
yet identified molecularly, has been isolated from the
of sleeping animals. And still a third sleep factor, not
hours. Another substance that has similar effects in
minutes, and the animal may stay asleep for several
ventricle, almost natural sleep occurs within a few
States of Brain Activity—Sleep, Brain Waves, Epilepsy, Psychoses
Chapter 59
741
sleep-producing substance are injected into the third
causing sleep is a nonapeptide isolated from the blood
neuronal tissues of the brain stem of animals kept
ness causes progressive accumulation of a sleep factor
or factors in the brain stem or in the cerebrospinal
Possible Cause of REM Sleep.
broken periodically by REM sleep is not understood.
has been postulated that the large acetylcholine-
secreting neurons in the upper brain stem reticular for-
could cause the excess activity that occurs in certain
are not channeled appropriately in the brain to cause
normal conscious awareness that is characteristic of
our imaginations run wild and suggest the following
possible mechanism for causing the sleep-wakefulness
not
encephalic and upper pontile reticular activating
reticular activating nuclei to become spontaneously
numerous
signals back to the same
and the sleep-promoting effects of the sleep centers
tions from sleep to wakefulness and from wakefulness
Sleep causes two major types of physiologic effects:
nervous system effects seem to be by far the more
important because any person who has a transected
spinal cord in the neck (and therefore has no sleep-
harmful effects in the body beneath the level of
transection that can be attributed directly to a sleep-
wakefulness is often associated with progressive mal-
function of the thought processes and sometimes even
of thought that occurs toward the end of a prolonged
restores both normal levels of brain activity and
assume that the same effect occurs in the central
nervous system because overuse of some brain areas
during wakefulness could easily throw these areas out
of balance with the remainder of the nervous system.
the principal value of sleep
is to restore natural balances among the neuronal
centers
research.
Electrical recordings from the surface of the brain or
even from the outer surface of the head demonstrate
that there is continuous electrical activity in the brain.
Both the intensity and the patterns of this electrical
activity are determined by the level of excitation of dif-
ferent parts of the brain resulting from sleep, wakeful-
ness
epilepsy or even
brain waves,
and the entire record is called an EEG (electroen-
cephalogram).
their frequencies range from once every few seconds to
dependent on the degree of activity in respective parts
between the states of wakefulness and sleep and coma.
are characteristic of specific abnormalities of the brain
brain—to cause the delta waves.
the cortex.This indicates that some synchronizing mech-
alpha waves, nevertheless does not block delta waves in
the thalamus to the cerebral cortex, which blocks thal-
Transection of the fiber tracts from
Origin of Delta Waves.
cortical neurons during each wave.
system in the brain stem as well. This oscillation pre-
system, possibly including the reticular activating
natural frequency of the alpha waves. Therefore, it is
frequency between 8 and 13 per second, which is the
in “diffuse” nuclei deep inside the thalamus often sets
thalamus. Conversely, stimulation in the nonspecific
Origin of Alpha Waves.
beta waves.
voltage waves of generally high but irregular frequency,
lified one another, and the resultant effect was very low
the brain increased greatly, but synchronization of the
Then, when the eyes were opened, the activity of
waves.
frequency of about 12 per second, thus causing
which shows, when the eyes were closed, synchronous
opposing polarities. This is demonstrated in Figure 59–2,
nonsynchronous
fact, strong
by the total level of electrical activity in the brain. In
with one another, not
in synchrony
skull. Thus, the intensity of the brain waves from the
; only then will
must fire synchronously
the head. Instead, many thousands or even millions of
The discharge of a single neuron or single nerve fiber
Origin of Brain Waves
from the thalamus. Therefore, delta waves can occur
They also occur in the cortex of animals that have had
sleep, in infancy, and in serious organic brain disease.
other types of brain waves. They occur in very deep
frequencies less than 3.5 cycles per second, and they
many brain disorders, often in degenerative brain states.
appointment and frustration. Theta waves also occur in
emotional stress in some adults, particularly during dis-
temporal regions in children, but they also occur during
per second. They occur normally in the parietal and
have frequencies between 4 and 7 cycles
per second and as high as 80 cycles per second. They are
occur at frequencies greater than 14 cycles
nous beta waves.
and that these are replaced by low-voltage, asynchro-
light and then closing the eyes. Note that the visual sen-
. Figure 59–2 shows the effect
beta waves
lower-voltage
are replaced by asynchronous, higher-frequency but
some specific type of mental activity, the alpha waves
When the awake person’s attention is directed to
disappear.
about 50 microvolts. During deep sleep, the alpha waves
and frontal regions of the scalp. Their voltage usually is
cerebration. These waves occur most intensely in the oc-
when they are awake and in a quiet, resting state of
quencies between 8 and 13 cycles per second and are
are shown in Figure 59–1.
, which
, and
In normal healthy people, most waves in the EEG can
The Nervous System: C. Motor and Integrative Neurophysiology
742
Unit XI
be classified as alpha, beta, theta
delta waves
Alpha waves are rhythmical waves that occur at fre-
found in the EEGs of almost all normal adult people
cipital region but can also be recorded from the parietal
on the alpha waves of simply opening the eyes in bright
sations cause immediate cessation of the alpha waves
Beta waves
recorded mainly from the parietal and frontal regions
during specific activation of these parts of the brain.
Theta waves
Delta waves include all the waves of the EEG with
often have voltages two to four times greater than most
subcortical transections separating the cerebral cortex
strictly in the cortex independent of activities in lower
regions of the brain.
in the brain can never be recorded from the surface of
neurons or fibers
the potentials from the individual neurons or fibers
summate enough to be recorded all the way through the
scalp is determined mainly by the numbers of neurons
and fibers that fire
nerve signals often nullify
one another in the recorded brain waves because of
discharge of many neurons in the cerebral cortex at a
alpha
signals became so little that the brain waves mainly nul-
the
Alpha waves will not occur in the
cerebral cortex without cortical connections with the
layer of reticular nuclei that surround the thalamus or
up electrical waves in the thalamocortical system at a
believed that the alpha waves result from spontaneous
feedback oscillation in this diffuse thalamocortical
sumably causes both the periodicity of the alpha waves
and the synchronous activation of literally millions of
amic activation of the cortex and thereby eliminates the
anism can occur in the cortical neuronal system by
itself—mainly independent of lower structures in the
Delta waves also occur during deep slow-wave sleep;
this suggests that the cortex then is mainly released
Alpha
Beta
Theta
Delta
1 sec
50
m
V
in the normal electro-
Different types of
Figure 59–1
brain waves
encephalogram.
Eyes open
Eyes closed
rhythm when the eyes are opened.
rhythm by an asynchronous, low-
Figure 59–2
Replacement of the alpha
voltage beta
that cyanosis occurs. Also, signals transmitted from the
may have difficulty breathing, sometimes to the extent
the person bites or “swallows” his or her tongue and
tonic-clonic seizures.
of the entire body, followed toward
even in the brain stem. Also, discharges transmitted all
bral cortex, in the deeper parts of the cerebrum, and
focal epilepsy.
, and
below this threshold, no attack occurs.
threshold. As long as the degree of excitability is held
central nervous system. A person who is predisposed to
Epilepsy (also called “seizures”) is characterized by
firing of the neurons, despite significant brain activity.
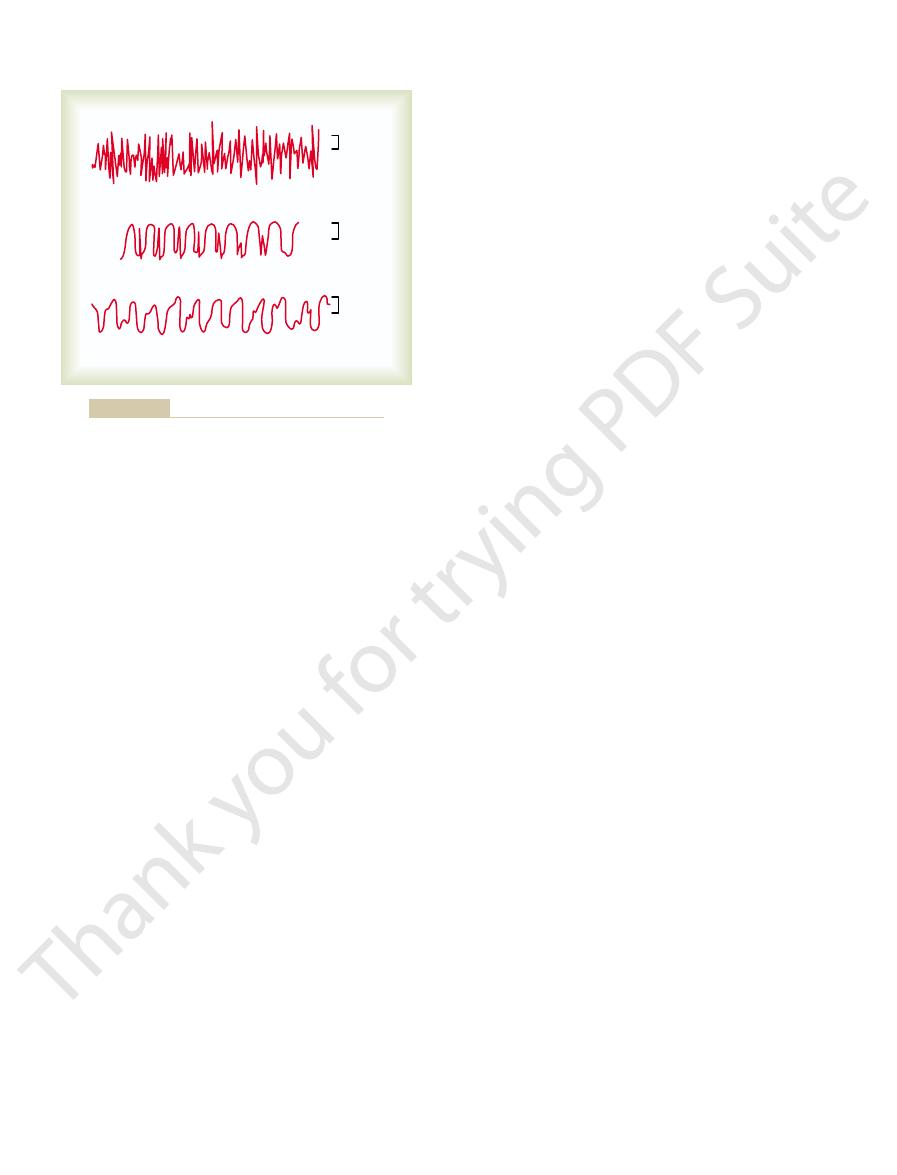
nized sleep
desynchro-
Therefore, REM sleep is frequently called
chronized nervous activity as found in the awake state.
high-frequency, which are normally suggestive of desyn-
an awake, active person. The waves are irregular and
EEG during REM sleep. It is often difficult to tell the
Finally, the bottom record in Figure 59–4 shows the
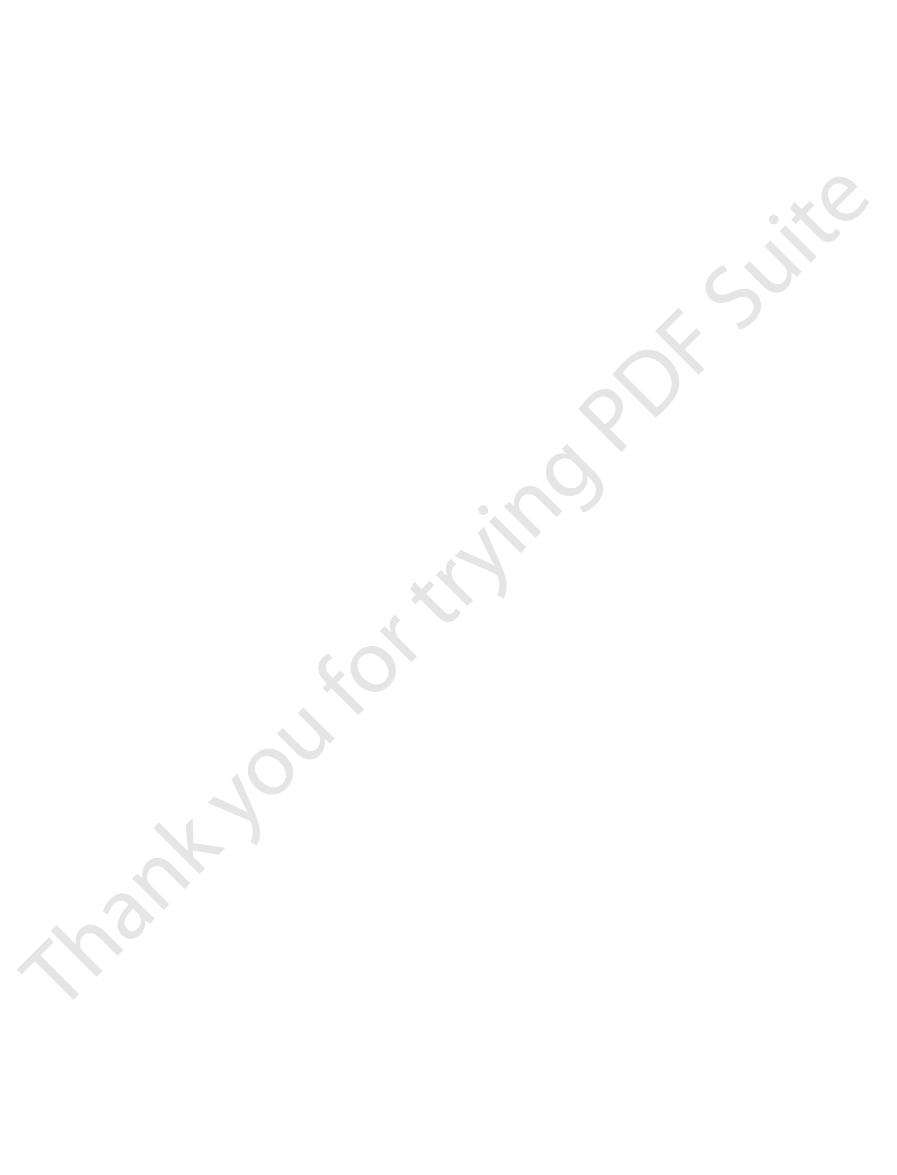
delta waves.
per second in stage 4; these are
slower until it reaches a frequency of only 1 to 3 waves
sleep, the frequency of the EEG becomes progressively
that occur periodically. In stages 2, 3, and 4 of slow-wave
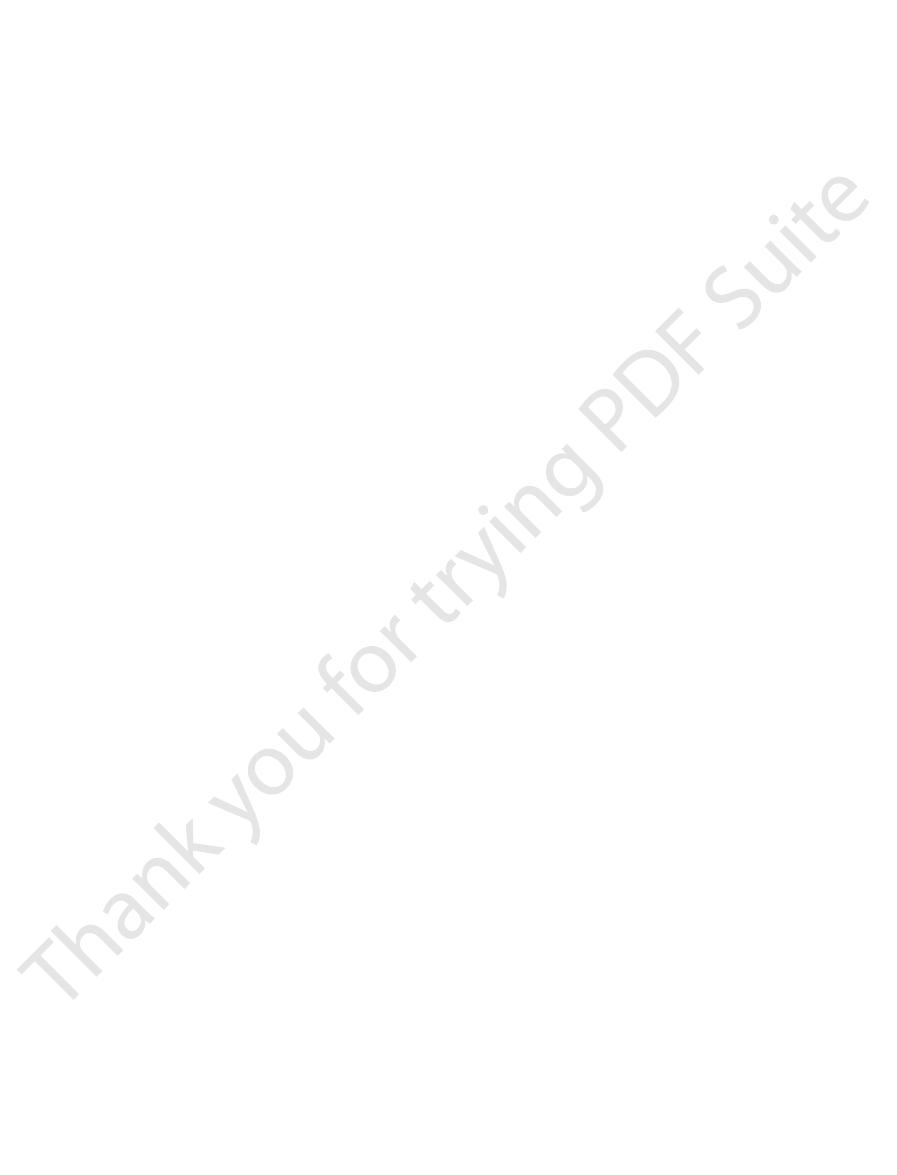
,” that is, short spindle-shaped bursts of alpha waves
waves becomes very low; this is broken by “
stage, a stage of very light sleep, the voltage of the EEG
Slow-wave sleep is divided into four stages. In the first
the figure.
alpha waves,
beta waves,
fulness is characterized by high-frequency
in different stages of wakefulness and sleep. Alert wake-
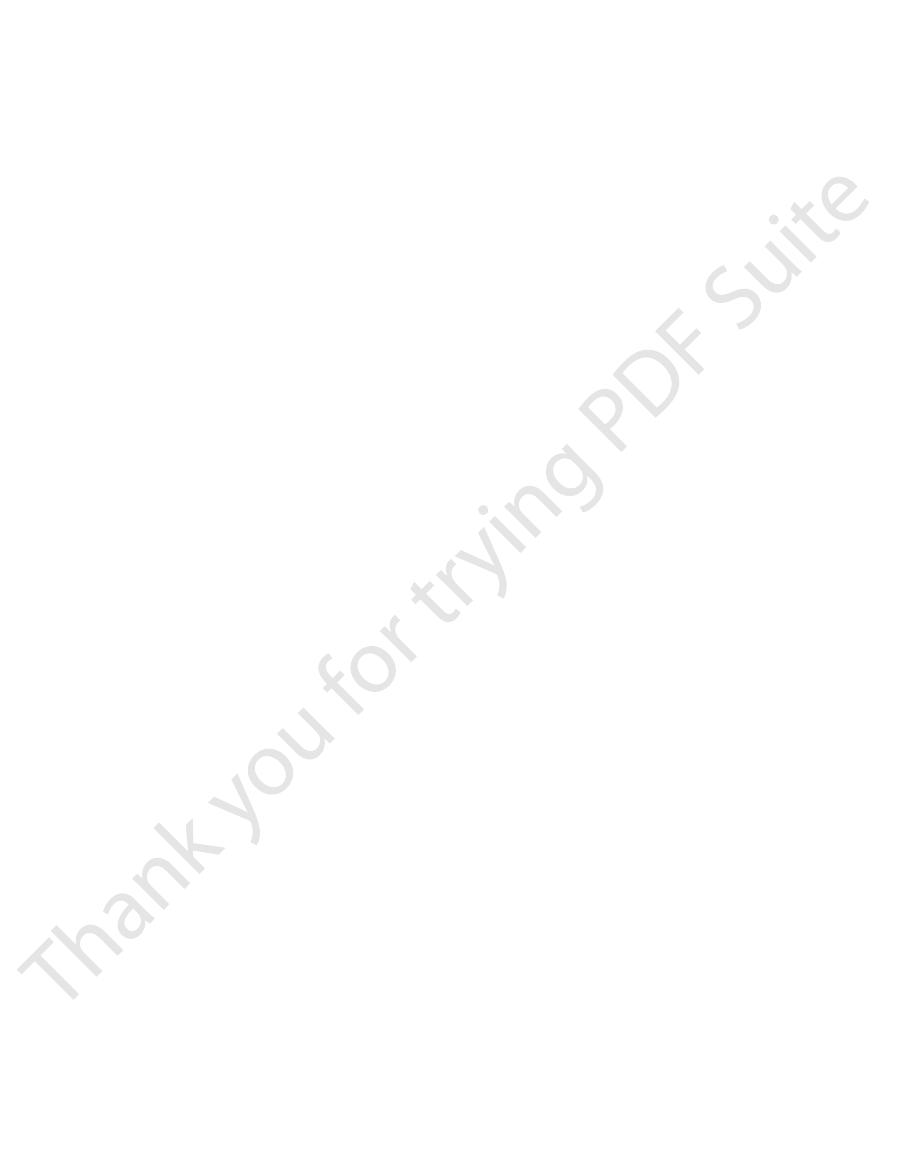
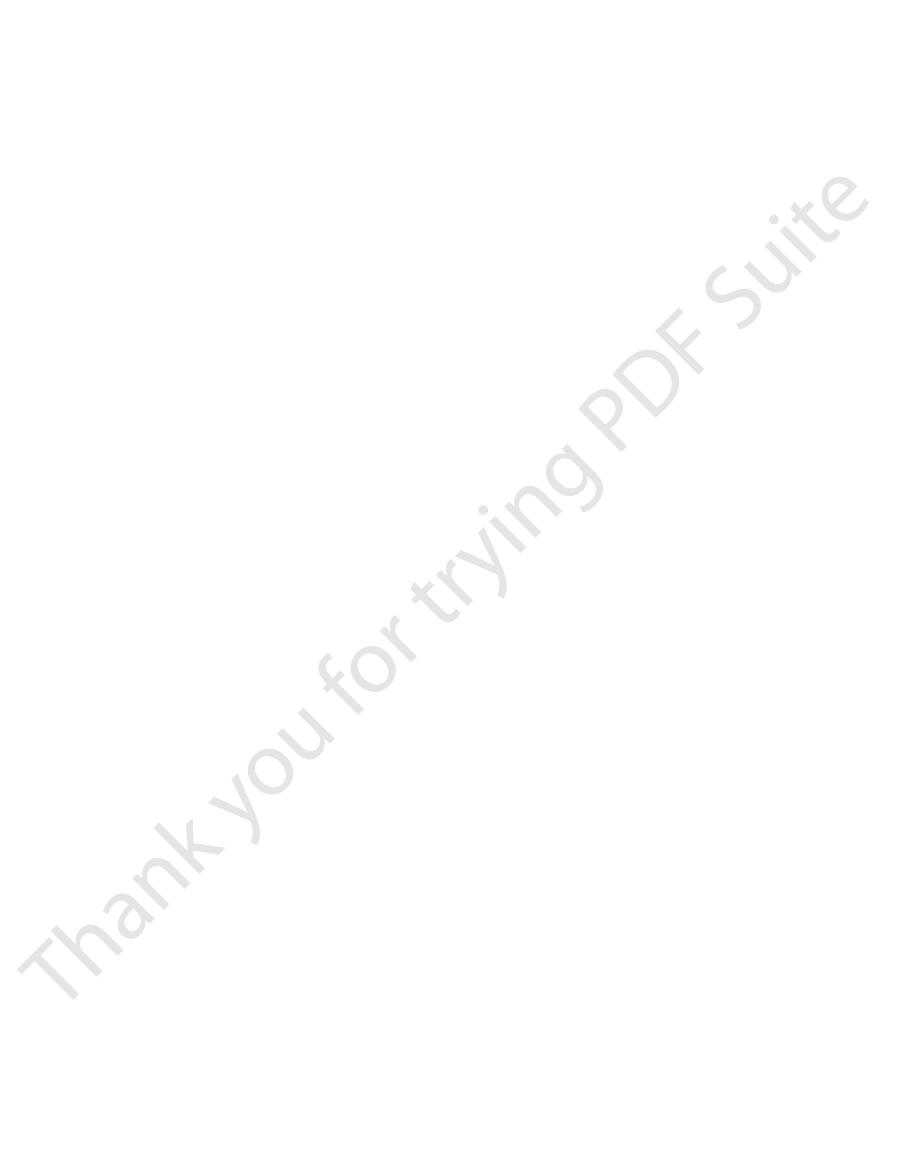
Figure 59–4 shows EEG patterns from a typical person
Stages of Wakefulness and Sleep
Changes in the EEG at Different
Figure 59–2.
markedly increased cortical activity,
chronous, so that the voltage falls considerably, despite
waves usually become asynchronous rather than syn-
During periods of mental activity, the
mental activity.
relaxed states; and beta waves during periods of intense
psychomotor states and in infants; alpha waves during
surgical anesthesia, and deep sleep; theta waves in
which shows the existence of delta waves in stupor,
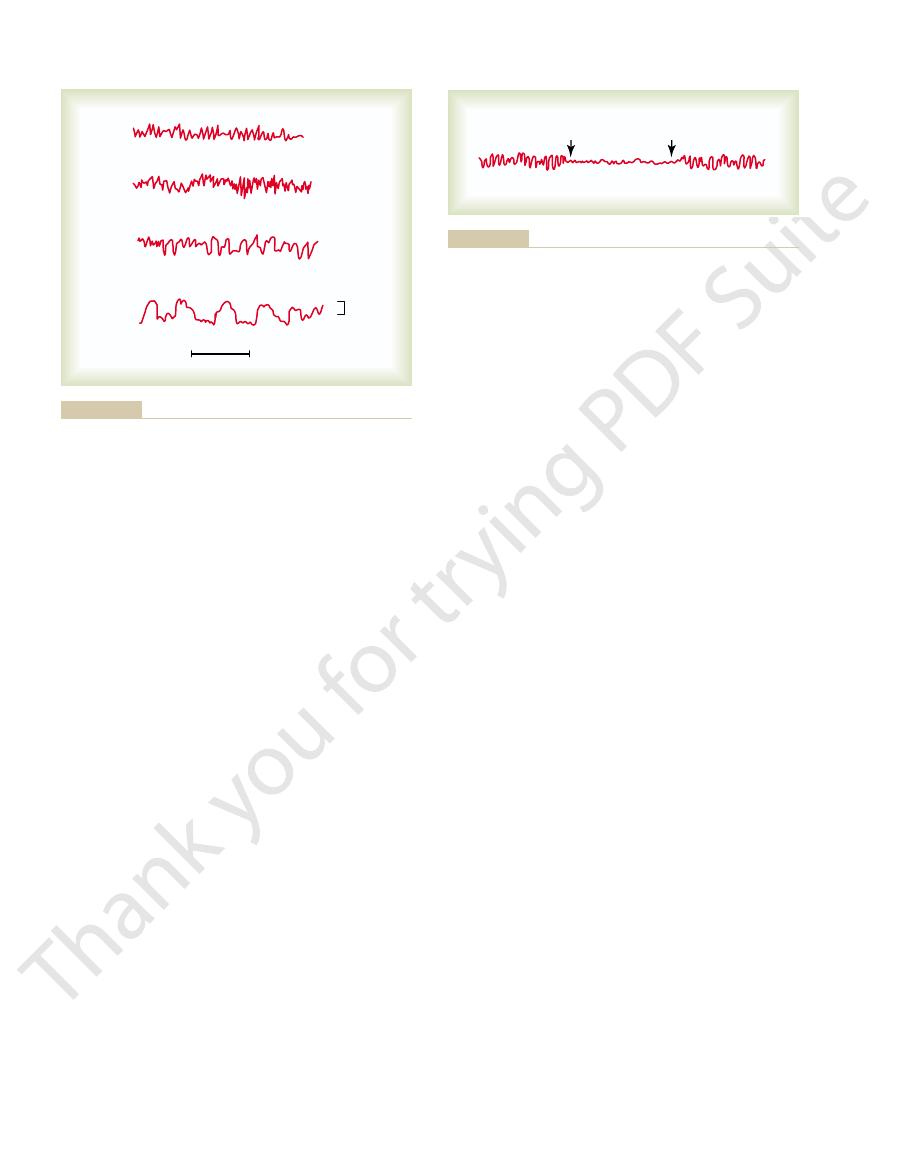
degrees of activity. This is demonstrated in Figure 59–3,
average frequency increasing progressively with higher
activity and average frequency of the EEG rhythm, the
There is a general correlation between level of cerebral
of the EEG
Cerebral Activity on the Frequency
Effect of Varying Levels of
lower centers.
States of Brain Activity—Sleep, Brain Waves, Epilepsy, Psychoses
Chapter 59
743
from the activating influences of the thalamus and other
as shown in
whereas quiet wakefulness is usually associated with
as demonstrated by the first two EEGs of
sleep spin-
dles
difference between this brain wave pattern and that of
because there is lack of synchrony in the
Epilepsy
uncontrolled excessive activity of either part or all of the
epilepsy has attacks when the basal level of excitability
of the nervous system (or of the part that is susceptible
to the epileptic state) rises above a certain critical
Epilepsy can be classified into three major types:
grand mal epilepsy, petit mal epilepsy
Grand Mal Epilepsy
Grand mal epilepsy is characterized by extreme neu-
ronal discharges in all areas of the brain—in the cere-
the way into the spinal cord sometimes cause general-
ized tonic seizures
the end of the attack by alternating tonic and spasmodic
muscle contractions called
Often
Stupor
Surgical
anesthesia
Sleep Psychomotor
Slow component
of petit mal
Infants Relaxation
Deteriorated epileptics
Attention
Fright
Grand mal
Fast component
of petit mal
Confusion
1 second
Inc., Upper Saddle River, NJ.)
by permission of Prentice-Hall,
and Controls.
phy, 2nd ed, Vol I: Methodology
EL: Atlas of Electroencephalogra-
(Redrawn from Gibbs FA, Gibbs
of the electroencephalogram.
Effect of varying degrees of cere-
Figure 59–3
bral activity on the basic rhythm
“ 1974. Reprinted
Alert wakefulness (beta waves)
Quiet wakefulness (alpha waves)
Stage 1 sleep (low voltage and spindles)
Stages 2 and 3 sleep (theta waves)
Stage 4 slow wave sleep (delta waves)
REM sleep (beta waves)
1 sec
50
m
V
during different stages of wakefulness and sleep.
Progressive change in the characteristics of the brain waves
Figure 59–4
motor cortex, it causes progressive “march” of muscle
second.When such a wave of excitation spreads over the
cortex into the epileptic discharge zone. The process
localized reverber-
These waves presumably result from
waves begin to spread over adjacent cortical regions.
rises above several hundred per second, synchronous
discharges in the local neurons; when the discharge rate
deranged local circuitry.
(3) a destroyed area of brain tissue, or (4) congenitally
tissue, (2) a tumor that compresses an area of the brain,
organic lesion or functional abnormality, such as (1) scar
Most often, focal epilepsy results from some localized
brain, either localized regions of the cerebral cortex or
Focal epilepsy can involve almost any local part of the
thalamocortical and corticothalamic neurons.
acid [GABA]–producing neurons) and (2)
the brain. In fact, animal studies suggest that it results
bral cortex, showing that the seizure involves much
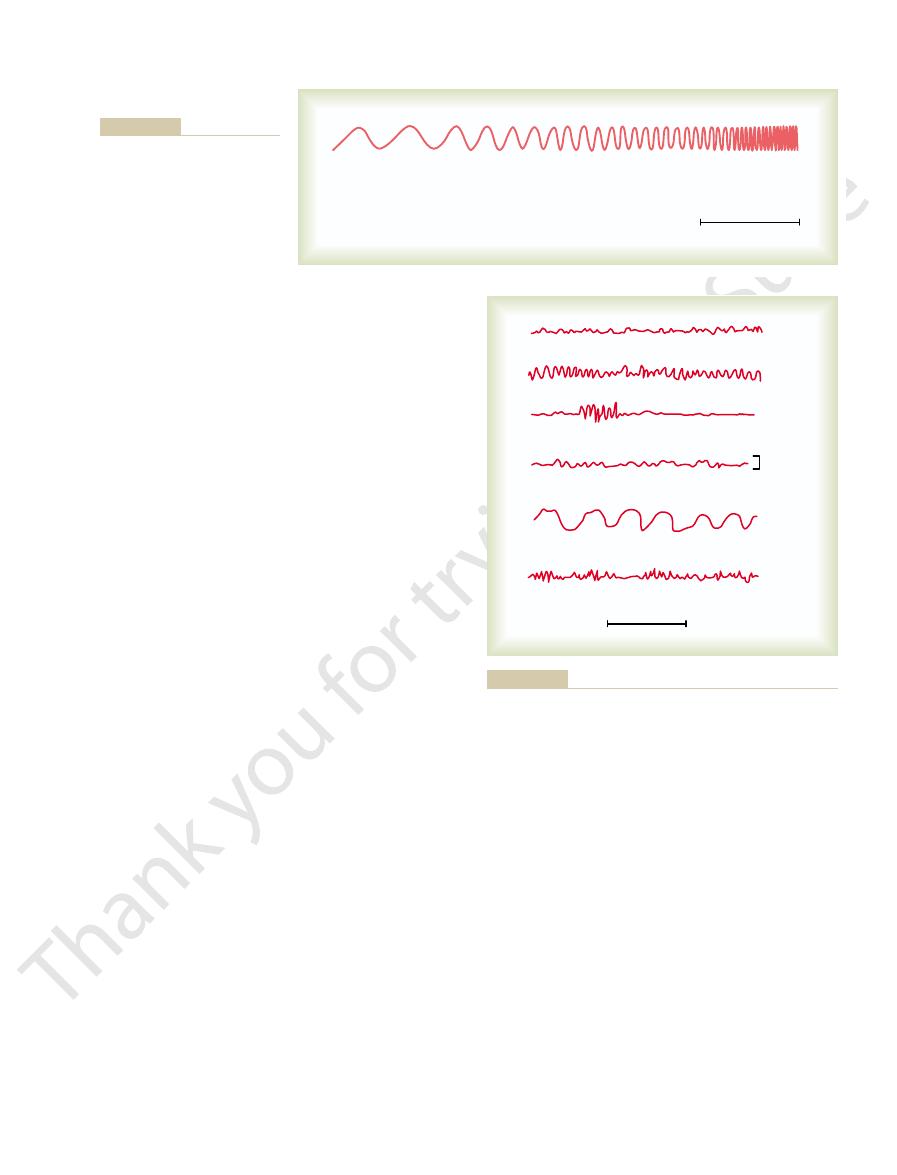
The spike
demonstrated by the middle recording of Figure 59–5,
The brain wave pattern in petit mal epilepsy is
pear by the age of 30. On occasion, a petit mal epilep-
the other. The usual course is for the petit mal attacks
instances, may have a rapid series of attacks, one after
may have one such attack in many months or, in rare
or absence epilepsy. The patient
previous activities. This total sequence is called the
the head region, especially blinking of the eyes; this is
mocortical brain activating system. It is usually charac-
neuronal fatigue.
Presumably, the major factor that stops the attack after
The cause of the extreme
elicit grand mal seizures.
areas, as we discuss shortly; these, too, sometimes trans-
or flashing lights.
overbreathing, (3) drugs, (4) fever, and (5) loud noises
(1) strong emotional stimuli, (2) alkalosis caused by
genic” circuitry enough to precipitate attacks include
increase the excitability of the abnormal “epilepto-
50 to 100 persons. In such people, factors that can
epilepsy, a predisposition that occurs in about 1 of every
activating system itself.
from the cerebral cortex. Presumably, therefore, a grand
the brain. Electrical recordings from the thalamus as
or they can be caused by insulin hypoglycemia, or by
In laboratory animals and even in human beings,
the cerebrum simultaneously.
time, demonstrating that the abnormal neuronal cir-
the entire cortex. Furthermore, the same type of dis-
that high-voltage, high-frequency discharges occur over
tonic phase of a grand mal attack. This demonstrates
The top recording of Figure 59–5 shows a typical
fatigued and asleep for hours thereafter.
seizure attack is over, and then often remains severely
of the entire nervous system; the person
to 3 to 4 minutes. It is also characterized by
The usual grand mal seizure lasts from a few seconds
The Nervous System: C. Motor and Integrative Neurophysiology
744
Unit XI
brain to the viscera frequently cause urination and defe-
cation.
postseizure
depression
remains in stupor for 1 to many minutes after the
EEG from almost any region of the cortex during the
charge occurs on both sides of the brain at the same
cuitry responsible for the attack strongly involves the
basal regions of the brain that drive the two halves of
grand mal attacks can be initiated by administering a
neuronal stimulant such as the drug pentylenetetrazol,
passage of alternating electrical current directly through
well as from the reticular formation of the brain stem
during the grand mal attack show typical high-voltage
activity in both of these areas similar to that recorded
mal attack involves not only abnormal activation of the
thalamus and cerebral cortex but also abnormal activa-
tion in the subthalamic brain stem portions of the brain
What Initiates a Grand Mal Attack?
Most people who have
grand mal attacks have hereditary predisposition to
Even in people who are not genetically predisposed,
certain types of traumatic lesions in almost any part of
the brain can cause excess excitability of local brain
mit signals into the activating systems of the brain to
What Stops the Grand Mal Attack?
neuronal overactivity during a grand mal attack is pre-
sumed to be massive simultaneous activation of many
reverberating neuronal pathways throughout the brain.
a few minutes is
A second factor is
probably active inhibition by inhibitory neurons that
have been activated by the attack.
Petit Mal Epilepsy
Petit mal epilepsy almost certainly involves the thala-
terized by 3 to 30 seconds of unconsciousness (or
diminished consciousness) during which time the
person has twitch-like contractions of muscles usually in
followed by return of consciousness and resumption of
absence syndrome
to appear first during late childhood and then to disap-
tic attack will initiate a grand mal attack.
which is typified by a spike and dome pattern.
and dome can be recorded over most or all of the cere-
or most of the thalamocortical activating system of
from oscillation of (1) inhibitory thalamic reticular
neurons (which are inhibitory gamma-aminobutyric
excitatory
Focal Epilepsy
deeper structures of both the cerebrum and brain stem.
tissue in the brain that pulls on the adjacent neuronal
Lesions such as these can promote extremely rapid
ating circuits that gradually recruit adjacent areas of the
spreads to adjacent areas at a rate as slow as a few mil-
limeters a minute to as fast as several centimeters per
Grand mal
Petit mal
Psychomotor
100
m
V
50
m
V
50
m
V
Electroencephalograms in different types of epilepsy.
Figure 59–5
posture and even rigidity.
and (3) are often withdrawn, sometimes with abnormal
sociation of ideas, and abnormal sequences of thought;
outside sources; (2) may develop incoherent speech, dis-
(1) are highly paranoid, with a sense of persecution from
types of feelings that are unreal. Many schizophrenics
and has delusions of grandeur, intense fear, or other
Schizophrenia comes in many varieties. One of the most
Exaggerated Function of Part of the
serotonin systems.
much of a good thing can cause mania. In support of this
ate sex drive, and psychomotor balance—although too
create happiness, contentment, good appetite, appropri-
the brain to increase a person’s sense of well-being, to
pounds, can be effective in treating the manic phase of
norepinephrine and serotonin, such as lithium com-
episodes. Drugs that diminish the formation or action of
, and a
manic-depressive psychosis
bipolar disorder
between depression and mania, which is called either
phrine activity.
tic attack. This has been shown to enhance norepine-
therapy, electrical current is passed through the brain to
sive therapy—commonly called “shock therapy.” In this
, such as
and serotonin once they are formed; and (2)
, which block destruction of norepinephrine
monoamine oxidase
nerve endings—for instance, (1)
Conversely, about 70 per cent of depressive patients can
tonin, such as reserpine, frequently cause depression.
and cerebral cortex. Also, many
to most parts of the brain limbic system, thalamus,
These neurons send fibers upward
locus ceruleus.
are located in the brain stem, especially in
drive and have severe insomnia. Often associated with
In addition, they often lose their appetite and sex
symptoms of grief, unhappiness, despair, and misery.
neurotransmitters.) Depressed patients experience
. (New evidence has implicated still other
tonin, or both
people in the United States, might be caused by
, which occurs in about 8 million
depression psychosis
Psychoses—Decreased Activity of
GABA-secreting neurons and acetylcholine-secreting
56, we pointed out that in Huntington’s disease, loss of
in the caudate nucleus and putamen. Also in Chapter
disease. This disease results from loss of neurons in the
In Chapter 56, we discussed the cause of Parkinson’s
patients.
neurons that secrete a specific neurotransmitter. Use of
Neurotransmitter Systems
prevents future attacks.
point is found, surgical excision of the focus frequently
predispose to focal epileptic attacks. Once such a focal
The EEG can be used to localize abnormal spiking
imposed 14-per-second waves.
low-frequency rectangular wave with a frequency
typical EEG during a psychomotor seizure, showing a
The lowest tracing of Figure 59–5 demonstrates a
the hippocampus, the amygdala, the septum, and/or por-
involve part of the limbic portion of the brain, such as
unable to control it. Attacks of this type frequently
activities during the attack, but at other times, he or she
incoherent speech or mumbling of some trite phrase.
anxiety, discomfort, or fear; and/or (4) a moment of
amnesia; (2) an attack of abnormal rage; (3) sudden
, which may cause (1) a short period of
chomotor seizure
single area of the brain, but in many instances, the
jacksonian epilepsy.
other times marching in the opposite direction. This is
contractions throughout the opposite side of the body,
States of Brain Activity—Sleep, Brain Waves, Epilepsy, Psychoses
Chapter 59
745
beginning most characteristically in the mouth region
and marching progressively downward to the legs but at
called
A focal epileptic attack may remain confined to a
strong signals from the convulsing cortex excite the
mesencephalic portion of the brain activating system so
greatly that a grand mal epileptic attack ensues as well.
Another type of focal epilepsy is the so-called psy-
Sometimes the person cannot remember his or her
is conscious of everything that he or she is doing but
tions of the temporal cortex.
between 2 and 4 per second and with occasional super-
Surgical Excision of Epileptic Foci Can Often Prevent Seizures.
waves originating in areas of organic brain disease that
Psychotic Behavior and
Dementia—Roles of Specific
Clinical studies of patients with different psychoses or
different types of dementia have suggested that many
of these conditions result from diminished function of
appropriate drugs to counteract loss of the respective
neurotransmitter has been successful in treating some
substantia nigra whose nerve endings secrete dopamine
neurons is associated with specific abnormal motor pat-
terns plus dementia occurring in the same patient.
Depression and Manic-Depressive
the Norepinephrine and Serotonin
Neurotransmitter Systems
Much evidence has accumulated suggesting that mental
dimin-
ished formation in the brain of norepinephrine or sero-
these is a state of psychomotor agitation despite the
depression.
Moderate numbers of norepinephrine-secreting
neurons
the
serotonin-producing
neurons located in the midline raphe nuclei of the lower
pons and medulla send fibers to many areas of the
limbic system and to some other areas of the brain.
A principal reason for believing that depres-
sion might be caused by diminished activity of
norepinephrine- and serotonin-secreting neurons is that
drugs that block secretion of norepinephrine and sero-
be treated effectively with drugs that increase the exci-
tatory effects of norepinephrine and serotonin at the
inhibitors
tricyclic
antidepressants
imipramine and amitriptyline,
which block reuptake of norepinephrine and serotonin
by nerve endings so that these transmitters remain
active for longer periods after secretion.
Mental depression can be treated by electroconvul-
cause a generalized seizure similar to that of an epilep-
Some patients with mental depression alternate
or
few people exhibit only mania without the depressive
the condition.
It is presumed that the norepinephrine and serotonin
systems normally provide drive to the limbic areas of
concept is the fact that pleasure and reward centers of
the hypothalamus and surrounding areas receive large
numbers of nerve endings from the norepinephrine and
Schizophrenia—Possible
Dopamine System
common types is seen in the person who hears voices
folded proteins. Lancet 363:1139, 2004.
Alzheimer’s disease: inflammation, cholesterol, and mis-
Casserly I, Topol E: Convergence of atherosclerosis and
4:457, 2004.
Bryant PA, Trinder J, Curtis N: Sick and tired: does sleep
Beardsley T: Waking up. Sci Am Jul 18, 1996.
ders. New York: Oxford University Press, 1999.
Aldrich MS: Sleep Medicine: Normal Sleep and Its Disor-
disease.
to greatly increase the risk for developing Alzheimer’s
sion, diabetes, and hyperlipidemia, are also recognized
factors for cerebrovascular disease, such as hyperten-
Alzheimer’s disease. In fact, many of the common risk
may play a role in Alzheimer’s disease.
There is also accumulating evidence that
Vascular Disorders May Contribute to Progression of Alzheimer’s
process.
Alzheimer’s disease appears to attenuate the disease
tion with the accumulation of amyloid plaques; and (5)
increased risk for Alzheimer’s disease; (4) transgenic
blood protein that transports cholesterol to the tissues,
abnormality of a gene that controls apolipoprotein E, a
Alzheimer’s disease by midlife; (3) patients who have
peptide; (2) patients with trisomy 21 (Down syndrome)
rently known mutations associated with Alzheimer’s
suggested by the following observations: (1) all cur-
peptide in the pathogenesis of Alzheimer’s disease is
appears to be a metabolic degenerative disease.
and even the cerebellum. Thus, Alzheimer’s disease
cerebral cortex, hippocampus, basal ganglia, thalamus,
found in widespread areas of the brain, including in the
lates in amyloid plaques, which range in diameter from
patients with Alzheimer’s disease. The peptide accumu-
Pathologically, one finds increased
Alzheimer’s Disease Is Associated with Accumulation of Brain
percent of 85-year-olds having the disease.
age, with about 1 percent of 60-year-olds and about 30
disorder. The percentage of persons with Alzheimer’s
Alzheimer’s disease is the most common form of
disease begins.
disease. Patients with Alzheimer’s disease usually
the person’s ability to perform activities of daily living
Alzheimer’s disease is a progressive and fatal neu-
this memory function is devastating.
limbic pathway that drives the memory process. Loss of
Alzheimer’s disease is loss of neurons in that part of the
the late phases of the disease. One consistent finding in
ties, gait disturbances, and seizures are uncommon until
(3) visuospatial deficits. Motor and sensory abnormali-
memory impairment, (2) deterioration of language, and
of Alzheimer’s disease include (1) an amnesic type of
to that seen in very, very old age. The clinical features
brain, usually beginning in mid-adult life and progress-
Alzheimer’s disease is defined as premature aging of the
Alzheimer’s Disease—Amyloid
, especially in the dominant hemisphere.
reduced in size
in schizophrenia
Finally, possible involvement of the hippocampus in
the effect of dopamine on subsequent neurons.
dol, and thiothixene—-all either decrease secretion of
ing schizophrenia—such as chlorpromazine, haloperi-
erful behavioral control centers.
portions of the prefrontal lobes. All of these are pow-
hippocampus, amygdala, anterior caudate nucleus, and
rior portions of the limbic system, especially into the
stantia nigra. These neurons give rise to the so-called
of the mesencephalon, medial and superior to the sub-
other related areas.
for treating Parkinson’s disease, but at the same time it
releases dopamine in the brain, which is advantageous
-dopa. This drug
schizophrenia because many patients with Parkinson’s
the prefrontal lobes.
The reason for believing that the prefrontal lobes are
control system centered around the hippocampus.
tion of a crucial part of the brain’s
including in the frontal lobes; and/or (3) abnormal func-
ter; (2) excessive excitement of a group of neurons that
results from one or more of three possibilities: (1) mul-
There are reasons to believe that schizophrenia
The Nervous System: C. Motor and Integrative Neurophysiology
746
Unit XI
tiple areas in the cerebral cortex prefrontal lobes in
which neural signals have become blocked or where
processing of the signals becomes dysfunctional because
many synapses normally excited by the neurotransmit-
ter glutamate lose their responsiveness to this transmit-
secrete dopamine in the behavioral centers of the brain,
limbic behavioral
involved in schizophrenia is that a schizophrenic-like
pattern of mental activity can be induced in monkeys by
making multiple minute lesions in widespread areas of
Dopamine has been implicated as a possible cause of
disease develop schizophrenic-like symptoms when
they are treated with the drug called
L
depresses various portions of the prefrontal lobes and
It has been suggested that in schizophrenia excess
dopamine is secreted by a group of dopamine-secreting
neurons whose cell bodies lie in the ventral tegmentum
mesolimbic dopaminergic system that projects nerve
fibers and dopamine secretion into the medial and ante-
An even more compelling reason for believing that
schizophrenia might be caused by excess production of
dopamine is that many drugs that are effective in treat-
dopamine at dopaminergic nerve endings or decrease
schizophrenia was discovered recently when it was
learned that
, the hippocampus is often
Plaques and Depressed Memory
ing rapidly to extreme loss of mental powers—similar
rodegenerative disorder that results in impairment of
as well as a variety of neuropsychiatric symptoms and
behavioral disturbances in the later stages of the
require continuous care within a few years after the
dementia in the elderly and about 5 million people in
the United States are estimated to be afflicted by this
disease approximately doubles with every five years of
Beta-Amyloid Peptide.
amounts of beta-amyloid peptide in the brains of
10 micrometers to several hundred micrometers and are
A key role for excess accumulation of beta-amyloid
disease increase the production of beta-amyloid
have three copies of the gene for amyloid precursor
protein and develop neurological characteristics of
have accelerated deposition of amyloid and greatly
mice that overproduce the human amyloid precursor
protein have learning and memory deficits in associa-
generation of anti-amyloid antibodies in humans with
Disease.
cerebrovascular disease caused by hypertension and
atherosclerosis
Cerebrovascular disease is the second most common
cause of acquired cognitive impairment and dementia
and likely contributes to cognitive decline in
References
have a vital role in the immune system? Nat Rev Immunol
Nat Rev Neurosci 5:400-408, 2004.
Steinlein OK: Genetic mechanisms that underlie epilepsy.
Physiol Rev 81:741, 2001.
Selkoe DJ: Alzheimer’s disease: genes, proteins, and therapy.
predicts novel therapies. Ann Intern Med 140:627, 2004.
Selkoe DJ: Alzheimer disease: mechanistic understanding
rosci 26:599, 2003.
Noebels JL: The biology of epilepsy genes. Annu Rev Neu-
bases of epileptic seizures. Annu Rev Physiol 63:815,
McCormick DA, Contreras D: On the cellular and network
entific review. JAMA 291:605, 2004.
LaRoche SM, Helmers SL: The new antiepileptic drugs: sci-
and in Alzheimer’s disease. Nat Rev Neurosci 5:347-360,
Iadecola C: Neurovascular regulation in the normal brain
malian torpor. Annu Rev Physiol 66:275, 2004.
Heller HC, Ruby NF: Sleep and circadian rhythms in mam-
lecular Med 5:59, 2004.
Greene R, Siegel J: Sleep: a functional enigma. Neuromo-
idiopathic epilepsies. Lancet Neurol 3:209, 2004.
Gourfinkel-An I, Baulac S, Nabbout R, et al: Monogenic
cascade be halted? J Clin Invest 111:11, 2003.
Golde TE: Alzheimer disease therapy: can the amyloid
and wakefulness. Mol Neurobiol 29:41, 2004.
Gerashchenko D, Shiromani PJ: Different neuronal pheno-
Neurol 61:473, 2004.
George AL Jr: Molecular basis of inherited epilepsy. Arch
Neurol 3:184, 2004.
or a vascular disorder? Data, dogma, and dialectics. Lancet
de la Torre JC: Is Alzheimer’s disease a neurodegenerative
Cummings JL: Alzheimer’s disease. N Engl J Med 351:56,
States of Brain Activity—Sleep, Brain Waves, Epilepsy, Psychoses
Chapter 59
747
2004.
types in the lateral hypothalamus and their role in sleep
2004.
2001.