
it usually exists as 100 per cent fat, whereas both proteins and carbohydrates are
bohydrate in most vegetable and grain products. Fat is deceptive in the diet because
Table 71–1 gives the compositions of selected foods, demonstrating especially the
from both proteins and fats. Indeed, in some parts of the world where meat is scarce,
tries, the quantity of energy derived from carbohydrates far exceeds that derived
per cent from fat, and 45 per cent from carbohydrate. In most non-Western coun-
Average Americans receive about 15 per cent of their energy from protein, 40
Protein
4
Fat
9
Carbohydrate
4
per cent of protein. Therefore, the average
gastrointestinal tract: about 98 per cent of carbohydrate, 95 per cent of fat, and 92
Also, these substances vary in the average percentages that are absorbed from the
protein as each gram is oxidized to carbon dioxide, water, and urea is 4.35 Calories.
from fat is 9.3 Calories. The energy liberated from metabolism of the average dietary
dioxide and water is 4.1 Calories (1 Calorie equals 1 kilocalorie), and that liberated
The energy liberated from each gram of carbohydrate as it is oxidized to carbon
Energy Available in Foods
Dietary Balances
different types of foods.
mechanisms by which food intake is regulated in accordance with the body’s
systems can be supplied with the requisite materials. This chapter discusses the
tained among these constituents so that all segments of the body’s metabolic
drates, fats, minerals, and vitamins, appropriate balances must also be main-
Because different foods contain different proportions of proteins, carbohy-
occur when energy intake is insufficient to meet the body’s metabolic needs.
fat, and body weight increases; conversely, loss of body mass and starvation
intake persistently exceeds expenditure, most of the excess energy is stored as
and energy expenditure be balanced. When a person is overfed and energy
weight and composition over long periods requires that a person’s energy intake
functions or stored for later use. Stability of body
Intake of carbohydrates, fats, and proteins provides
Are Balanced Under Steady-
Energy Intake and Output
Vitamins and Minerals
Feeding; Obesity and Starvation;
Dietary Balances; Regulation of
C
H
A
P
T
E
R
7
1
865
State Conditions
energy that can be used to perform various body
metabolic needs and some of the problems of maintaining balance among the
physiologically available energy in each
gram of these three foodstuffs is as follows:
Calories
the energy received from fats and proteins combined may be no greater than 15 to
20 per cent.
high proportions of fat and protein in meat products and the high proportion of car-
mixed in watery media so that each of these normally represents less than 25 per
protein are decreasing daily.
balance,
protein, the person is said to have a
been about 55 grams of protein breakdown. If the daily
metabolism in grams per day. Thus, excretion of 8 grams
(i.e., 100/16) to determine the total amount of protein
nitrogen excreted in the feces, and multiplying by 6.25
nitrogen in the urine, then adding 10 per cent for the
in the feces. Therefore, the rate of protein breakdown in
nitrogen products. The remaining 10 per cent is excreted
of urea, uric acid, creatinine, and other less important
gen. During metabolism of the protein, about 90 per
The average protein contains about 16 per cent nitro-
Utilization of Proteins,
to 50 grams.
body’s protein stores are consumed rapidly for energy,
carbohydrates and fats have been depleted, the
Conversely, in starvation, after the
protein sparers.
Therefore, both carbohydrates and fats are said to
two substances, and little is derived from proteins.
fats, almost all the body’s energy is derived from these
When the
depressed mentality, and edema caused by low plasma
which consists of failure to grow, lethargy,
orkor,
develop the protein-deficiency syndrome called
one of the essential amino acids. Therefore, individuals
example, the protein of corn has almost no tryptophan,
teins derived from vegetable and grain sources. For
much greater than normal. In general, proteins derived
quantities in the diet, the daily protein requirement is
partial proteins,
replace the degraded proteins. Such proteins are called
daily intake is above 30 to 50 grams.
of protein is needed in the diet for this purpose. An
the place of those that are being destroyed, and a supply
fore, all cells must continue to form new proteins to take
and used to produce other body chemicals daily. There-
Twenty to 30 grams of the body proteins are degraded
Average Daily Requirement for Protein Is 30 to 50 Grams.
tains as much energy as the potato itself.
cent of the weight. Therefore, the fat of one pat of butter
Metabolism and Temperature Regulation
866
Unit XIII
mixed with an entire helping of potato sometimes con-
average person can maintain normal stores of protein,
provided the
Some proteins have inadequate quantities of certain
essential amino acids and therefore cannot be used to
and when they are present in large
from animal foodstuffs are more complete than are pro-
in economically disadvantaged countries who consume
cornmeal as the principal source of protein sometimes
kwashi-
protein concentration.
Carbohydrates and Fats Act as “Protein Sparers.”
diet contains an abundance of carbohydrates and
be
sometimes at rates approaching several hundred
grams per day rather than the normal daily rate of 30
Methods for Determining Metabolic
Carbohydrates, and Fats
Nitrogen Excretion Can Be Used to Assess Protein Metabolism.
cent of this nitrogen is excreted in the urine in the form
the body can be estimated by measuring the amount of
of nitrogen in the urine each day means that there has
intake of protein is less than the daily breakdown of
negative nitrogen
which means that his or her body stores of
Table 71–1
Tuna, canned
24.2
10.8
0.5
194
Tomatoes
1.0
0.3
4.0
23
Strawberries
0.8
0.6
8.1
41
Spinach
2.3
0.3
3.2
25
Potatoes
2.0
0.1
19.1
85
Pork, ham
15.2
31.0
1.0
340
Peas, fresh
6.7
0.4
17.7
101
Peanuts
26.9
44.2
23.6
600
Oranges
0.9
0.2
11.2
50
Oatmeal, dry, uncooked
14.2
7.4
68.2
396
Molasses
0.0
0.0
60.0
240
Milk, fresh whole
3.5
3.9
4.9
69
Lamb, leg (average)
18.0
17.5
1.0
230
Haddock
17.2
0.3
0.5
72
Corn (maize)
10.0
4.3
73.4
372
Chocolate
5.5
52.9
18.0
570
Chicken, total edible
21.6
2.7
1.0
111
Cheese, cheddar, American
23.9
32.3
1.7
393
Cashew nuts
19.6
47.2
26.4
609
Carrots
1.2
0.3
9.3
45
Cabbage
1.4
0.2
5.3
29
Butter
0.6
81.0
0.4
733
Bread, white
9.0
3.6
49.8
268
Beets, fresh
1.6
0.1
9.6
46
Beef (average)
17.5
22.0
1.0
268
broiled
25.0
55.0
1.0
599
Bacon, fat
6.2
76.0
0.7
712
Asparagus
2.2
0.2
3.9
26
Apples
0.3
0.4
14.9
64
Food
% Protein
% Fat
% Carbohydrate
Fuel Value per 100 Grams (Calories)
Protein, Fat, and Carbohydrate Content of Different Foods
Walnuts, English
15.0
64.4
15.6
702

metabolism. The lateral hypothalamic feeding center
marked weight loss, muscle weakness, and decreased
Conversely, destruction of the lateral
the hypothalamus serve as a feeding center,
pate in the control of food intake. The
brain, especially the hypothalamus.
ronmental and cultural factors, as well as by physio-
occurs. Each of these feelings is influenced by envi-
If the quest for food is successful, the feeling of
for food, often of a particular type, and is useful in
adequate food supply. A person’s
restlessness, which cause the person to search for an
for food and several other several physiologic effects,
The sensation of
in physiologic conditions, as well as in obesity and
energy stores. In the next few sections we describe
changes in energy balance and influence the quest
What are the physiologic mechanisms that sense
caloric intake.
Thus, a large energy expenditure associated with phys-
about 2000 Calories per day for sedentary individuals.
6000 to 7000 Calories per day, compared with only
seek food. In athletes and laborers, energy expenditure
energy stores, for example, rapidly activate multiple
that help maintain adequate energy intake. Deficits of
is necessary for survival. Therefore, the body is
individuals, maintenance of an adequate energy supply
amount of energy storage (i.e., fat mass) in different
energy intake or death occurs.
Excess energy intake is stored mainly as fat, whereas
activities of the various organs and tissues of the body.
result of protein metabolism, muscle activity, and
eventually converted to heat, which is generated as a
functional systems of the cells, and much of this is
expenditure. As discussed in Chapter 72, only about 27
Stability of the body’s total mass and composition over
Energy Storage
fat metabolism, 0.70.
Therefore, when diabetes is severe, most of the
conditions, because insulin is required for this.
can be used by the body’s cells under any
3. In untreated diabetes mellitus, little carbohydrate
approaches that for fat metabolism, about 0.70.
carbohydrates, and the respiratory quotient
2. About 8 to 10 hours after a meal, the body has
that is metabolized is carbohydrates, so that the
1. Immediately after a meal, almost all the food
lization of the three foodstuffs.
mathematical formula, calculate almost exactly the uti-
nitrogen excretion and then, using the appropriate
carbohydrate to fat metabolism. To be more exact, one
amount of protein metabolism, respiratory quotients
proteins. And, finally, if we ignore the normally small
entirely fats, to the exclusion of carbohydrates and
quotient is about 0.70, the body is metabolizing almost
siderably less than 1.0. Likewise, when the respiratory
almost entirely carbohydrates, because the respiratory
a respiratory quotient of 1.0, he or she is metabolizing
metabolic reactions throughout the body. If a person has
period of 1 hour or more, the respiratory exchange ratio
respiratory exchange ratio.
ferent foods by the body. First, it will be recalled from
excess hydrogen atoms present in their molecules, so
quotient is 0.80. The reason that the respiratory quo-
teins are oxidized by the cells, the average respiratory
tient for the metabolism of fat averages 0.70. When pro-
molecules of oxygen consumed. The respiratory quo-
When fat is oxidized in the body’s cells, an average of
for each molecule of oxygen consumed. This ratio of
oxygen, exactly one carbon dioxide molecule is formed
When carbohydrates are metabolized with
“Respiratory Quotient” Is the Ratio of CO
Dietary Balances; Regulation of Feeding; Obesity and Starvation; Vitamins and Minerals
Chapter 71
867
2
Production to O
2
Utilization and Can Be Used to Estimate Fat and Carbohydrate
Utilization.
carbon dioxide output to oxygen usage is called the
respiratory quotient, so the respiratory quotient for
carbohydrates is 1.0.
70 carbon dioxide molecules are formed for each 100
tients for fats and proteins are lower than that for
carbohydrates is that a large share of the oxygen metab-
olized with these foods is required to combine with the
that less carbon dioxide is formed in relation to the
oxygen used.
Now let us see how one can make use of the respira-
tory quotient to determine the relative utilization of dif-
Chapter 39 that the output of carbon dioxide by the
lungs divided by the uptake of oxygen during the same
period is called the
Over a
exactly equals the average respiratory quotient of the
quotients for both fat and protein metabolism are con-
between 0.70 and 1.0 describe the approximate ratios of
can first determine the protein utilization by measuring
Some of the important findings from studies of respi-
ratory quotients are the following:
respiratory quotient at that time approaches 1.0.
already used up most of its readily available
time the respiratory quotient remains near that for
Regulation of Food Intake and
long periods requires that energy intake match energy
per cent of the energy ingested normally reaches the
a deficit of energy intake causes loss of total body
mass until energy expenditure eventually equals
Although there is considerable variability in the
endowed with powerful physiologic control systems
mechanisms that cause hunger and drive a person to
for the high level of muscle activity may be as high as
ical work usually stimulates equally large increases in
for food? Maintenance of adequate energy supply in
the body is so critical that there are multiple short-
term and long-term control systems that regulate not
only food intake but also energy expenditure and
some of these control systems and their operation
starvation.
Neural Centers Regulate Food Intake
hunger is associated with a craving
such as rhythmical contractions of the stomach and
appetite is a desire
helping to choose the quality of the food to be eaten.
satiety
logic controls that influence specific centers of the
The Hypothalamus Contains Hunger and Satiety Centers.
Several neuronal centers of the hypothalamus partici-
lateral nuclei of
and stimu-
lation of this area causes an animal to eat voraciously
(hyperphagia).
hypothalamus causes lack of desire for food and
progressive inanition, a condition characterized by
operates by exciting the motor drives to search for
food.
and decreases energy expenditure. The effect of MCR
increasing energy expenditure. Conversely, inhibition
in regulating food intake and energy balance. Activa-
. Although there
-MSH, which then
The POMC neurons release
late energy stores.
many of the nervous and peripheral signals that regu-
. In fact, the neurons of the
, and
cholecys-
regulate appetite, including
As discussed later, these neurons appear to be the
increases food intake and reduces energy expenditure.
ture, whereas activation of the NPY-AGRP neurons
decreases food intake and increases energy expendi-
. Activation of the POMC neurons
protein (AGRP)
substances neuropeptide Y (NPY) and agouti-related
(CART), and (2)
with cocaine- and amphetamine-related transcript
melanocyte-stimulating hormone (
and energy expenditure (Figure 71–2): (1)
There are two distinct types of
substances that inhibit feeding.
substances that stimulate feeding, or
are listed in Table 71–2 and are generally categorized
hormones that influence feeding behavior. A few of
The hypothalamic feeding and satiety centers have
these inputs to the hypothalamus are shown in Figure
and taste) that influence feeding behavior. Some of
and signals from the cerebral cortex (sight, smell,
signals from hormones released by adipose tissue,
signify satiety, signals from gastrointestinal hormones,
in the blood (glucose, amino acids, and fatty acids) that
about stomach filling, chemical signals from nutrients
The hypothalamus receives neural signals from the
atic islet cells.
the thyroid and adrenal glands, as well as the pancre-
energy balance and metabolism, including those from
behavior and the perception of satiety. These nuclei
neurons on the hypothalamus, and together, these
There is much chemical cross-talk among the
as energy expenditure.
eating behavior. As discussed later, the arcuate nuclei
tricular nuclei often cause excessive eating, whereas
ing food intake. For example, lesions of the paraven-
paraventricular, dorsomedial,
The
animal becomes extremely obese, sometimes as large
Conversely, destruction of the ventromedial
of highly appetizing food, the animal refuses to eat
cause complete satiety, and even in the presence
feeding center. Electrical stimulation of this region can
This center is believed to give a
as the satiety center.
The
Metabolism and Temperature Regulation
868
Unit XIII
ventromedial nuclei of the hypothalamus serve
sense of nutritional satisfaction that inhibits the
(aphagia).
nuclei causes voracious and continued eating until the
as four times normal.
and arcuate nuclei
of the hypothalamus also play a major role in regulat-
lesions of the dorsomedial nuclei usually depress
are the sites in the hypothalamus where multiple hor-
mones released from the gastrointestinal tract and
adipose tissue converge to regulate food intake as well
centers coordinate the processes that control eating
of the hypothalamus also influence the secretion of
several hormones that are important in regulating
gastrointestinal tract that provide sensory information
71–1.
a high density of receptors for neurotransmitters and
the many substances that have been shown to alter
appetite and feeding behavior in experimental studies
as (1) orexigenic
(2) anorexigenic
Neurons and Neurotransmitters in the Hypothalamus That Stim-
ulate or Inhibit Feeding.
neurons in the arcuate nuclei of the hypothalamus that
are especially important as controllers of both appetite
pro-
opiomelanocortin (POMC) neurons that produce
a-
a-MSH) together
neurons that produce the orexigenic
major targets for the actions of several hormones that
leptin, insulin,
tokinin (CCK)
ghrelin
arcuate nuclei appear to be a site of convergence of
a
acts on melanocortin receptors found especially in
neurons of the paraventricular nuclei
are at least five subtypes of melanocortin receptor
(MCR), MCR-3 and MCR-4 are especially important
tion of these receptors reduces food intake while
of MCR-3 and MCR-4 greatly increases food intake
activation to increase energy expenditure appears to
Hypothalamus
Stomach
Leptin
PYY
Insulin
CCK
Ghrelin
Vagus nerve
Small intestine
Large intestine
+ -
-
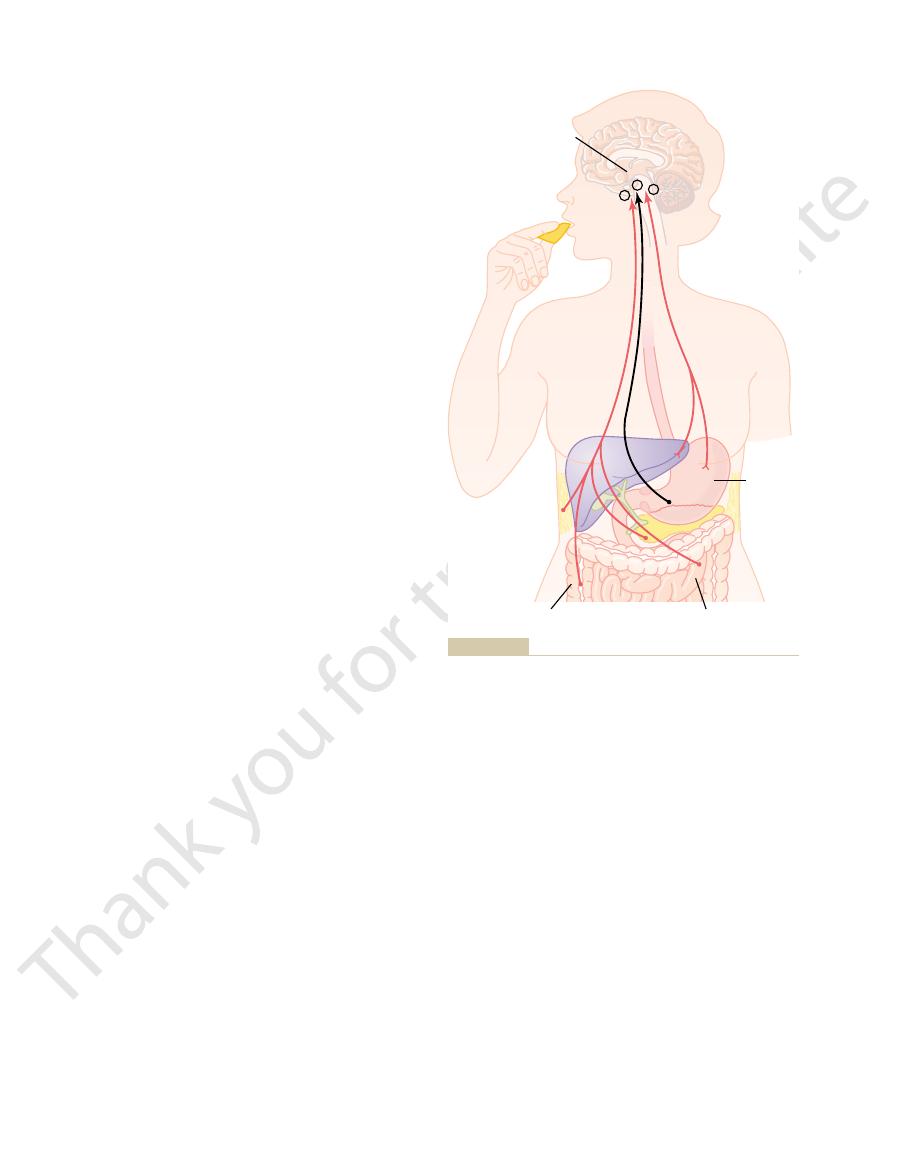
amounts by fat cells as they increase in size; it inhibits food intake.
stimulates appetite. Leptin is a hormone produced in increasing
Ghrelin is released by the stomach, especially during fasting, and
released by the ingestion of food and suppress further feeding.
tokinin (CCK), and insulin are gastrointestinal hormones that are
tors in the stomach activate sensory afferent pathways in the
Feedback mechanisms for control of food intake. Stretch recep-
Figure 71–1
vagus nerve and inhibit food intake. Peptide YY (PYY), cholecys-

Dietary Balances; Regulation of Feeding; Obesity and Starvation; Vitamins and Minerals
Chapter 71
869
Table 71–2
Cocaine- and amphetamine-regulated transcript (CART)
Ghrelin
Glucagon-like peptide (GLP)
Cortisol
Cholecystokinin (CCK)
Amino acids (glutamate and
Corticotropin-releasing hormone
Endorphins
Orexins A and B
Agouti-related protein (AGRP)
-MSH)
Neuropeptide Y (NPY)
-Melanocyte-stimulating hormone (
Decrease Feeding (Anorexigenic)
Increase Feeding (Orexigenic)
Neurotransmitters and Hormones That Influence Feeding and Satiety Centers in the Hypothalamus
a
a
Leptin
Serotonin
Melanin-concentrating hormone (MCH)
Norepinephrine
Insulin
Galanin (GAL)
g-aminobutyric acid)
Peptide YY (PYY)
To nucleus
tractus solitarius
(NTS)
•Sympathetic activity
•Energy expenditure
Neurons
of PVN
Neuron
Y
1
r
Y
1
r
Third
ventricle
MCR-4
MCR-3
MCR-3
Arcuate
nucleus
Food
intake
Food
intake
POMC/
CART
AGRP/
NPY
LepR
LepR
a
-MSH
a
-MSH
Insulin,
leptin,
CCK
Ghrelin
+
-
+
Food intake
melanocortin system reduces appetite. Some studies
in children. In contrast, excessive activation of the
as much as 5 to 6 percent of early-onset severe obesity
genic (single-gene) cause of human obesity, and some
MCR-4 represent the most common known mono-
associated with extreme obesity. In fact, mutations of
erful role in regulating energy stores of the body, and
The hypothalamic melanocortin system plays a pow-
thetic nervous system activity.
be mediated, at least in part, by activation of neuronal
receptor. (Redrawn from Barsh GS, Schwartz MW: Nature Rev Genetics 3:589, 2002).
R, neuropeptide Y1
secreted from the stomach, activates AGRP-NPY neurons and stimulates food intake. LepR, leptin receptor; Y
mones that inhibit AGRP-NPY neurons and stimulate adjacent POMC-CART neurons, thereby reducing food intake. Ghrelin, a hormone
sympathetic activity and energy expenditure. AGRP acts as an antagonist of MCR-4. Insulin, leptin, and cholecystokinin (CCK) ar
d increase
the paraventricular nuclei (PVN), which then activate neuronal pathways that project to the nucleus tractus solitarius (NTS) an
-MSH released by POMC neurons stimulates melanocortin receptors (MCR-3 and MCR-4) in
intake and reducing energy expenditure.
and neuropeptide Y (NPY), increasing food
increasing energy expenditure; and (2) neurons that produce agouti-related protein
-MSH) and cocaine- and amphetamine-regulated transcript (CART), decreasing food intake and
melanocyte-stimulating hormone (
Control of energy balance by two types of neurons of the arcuate nuclei: (1) pro-opiomelanocortin (POMC) neurons that release
Figure 71–2
a-
a
(AGRP)
a
e hor-
1
pathways that project from the paraventricular nuclei
to the nucleus tractus solitarius and stimulate sympa-
defective signaling of the melanocortin pathway is
studies suggest that MCR-4 mutations may account for
However, its physiologic role in humans is still
the possibility that it may be an orexigenic hormone.
intake in experimental animals, further supporting
feeding. Also, administration of ghrelin increases food
after a meal, suggesting a possible role in stimulating
fasting, peak just before eating, and then fall rapidly
the intestine. Blood levels of ghrelin rise during
cells of the stomach but also, to a much less extent, by
is a hormone released mainly by the oxyntic
intake of food (see Fig. 71–1).
both tend to suppress appetite. Thus, eating a meal
from the pancreas. Glucagon-like peptide and insulin
glucagon-like peptide,
For reasons that are not entirely understood, the
appetite in humans is still unclear.
decrease food intake for 12 hours or more, the impor-
observed after meals with a high fat content. Although
composition of the food, with higher levels of PYY
influenced by the number of calories ingested and the
after ingesting a meal. These peak levels of PYY are
colon. Food intake stimulates release of PYY, with
trointestinal tract, but especially from the ileum and
Peptide YY (PYY)
in the hypothalamus.
pathway
activation of the melanocortin
feeding centers to reduce subsequent eating. Studies in
food (Fig. 71–1).
the feeding center, thereby reducing the desire for
stomach and the duodenum, stretch inhibitory signals
trointestinal tract becomes distended, especially the
When the gas-
tant for these purposes.
approximates nutritional needs. The following are
tion of eating. Yet it is important that the person not
changes in the body’s energy stores to occur, and
has eaten enough? There has not been enough time for
and rapidly, what turns off the eating when he or she
When a person is driven by hunger to eat voraciously
Short-Term Regulation of Food Intake
stores in the body.
primarily with preventing overeating at each meal, and
Factors That Regulate Quantity
type and quality of food it eats.
choice of foods. In other words, the animal (and pre-
both sides of the brain is a “psychic blindness” in the
amygdala elicits the mechanical act of feeding. An
feeding. In addition, stimulation of some areas of the
of its areas increase feeding, whereas others inhibit
part of the olfactory nervous system. Destructive
closely coupled with the hypothalamus. It will be
ularly in the control of appetite. These centers include
play important roles in the control of feeding, partic-
mechanics to activity.
centers in feeding, then, is to control the quantity of
The function of the other
the actual mechanics of feeding are controlled by
vate, lick its lips, chew food, and swallow. Therefore,
mechanical features of the feeding process. It can sali-
cephalon, the animal can still perform the basic
act of the feeding process itself. If the brain is sec-
ulating appetite.
the POMC neurons is reduced, thereby decreasing the
which stimulates appetite. At the same time, firing of
low, orexigenic neurons are activated to release NPY,
arcuate nuclei. When energy stores of the body are
feeding and obesity.
due to gene mutations, is associated with excessive
excessive formation of AGRP in mice and humans,
normal physiologic control of food intake is unclear,
tors (see Figure 71–2). Although the role of AGRP in
AGRP released from the orexigenic neurons of the
cancer tumors.
Metabolism and Temperature Regulation
870
Unit XIII
suggest that this activation may play a role in causing
the anorexia associated with severe infections or
hypothalamus is a natural antagonist of MCR-3 and
MCR-4 and probably increases feeding by inhibiting
the effects of
a-MSH to stimulate melanocortin recep-
NPY is also released from orexigenic neurons of the
activity of the melanocortin pathway and further stim-
Neural Centers That Influence the Mechanical Process of
Feeding.
Another aspect of feeding is the mechanical
tioned below the hypothalamus but above the mesen-
centers in the brain stem.
food intake and to excite these centers of feeding
Neural centers higher than the hypothalamus also
the amygdala and the prefrontal cortex, which are
recalled from the discussion of the sense of smell in
Chapter 53 that portions of the amygdala are a major
lesions in the amygdala have demonstrated that some
important effect of destruction of the amygdala on
sumably the human being as well) loses or at least par-
tially loses the appetite control that determines the
of Food Intake
Regulation of the quantity of food intake can be
divided into short-term regulation, which is concerned
long-term regulation, which is concerned primarily
with maintenance of normal quantities of energy
it takes hours for enough nutritional factors to be
absorbed into the blood to cause the necessary inhibi-
overeat and that he or she eat an amount of food that
several types of rapid feedback signals that are impor-
Gastrointestinal Filling Inhibits Feeding.
are transmitted mainly by way of the vagi to suppress
Gastrointestinal Hormonal Factors Suppress Feeding.
Chole-
cystokinin is released mainly in response to fat enter-
ing the duodenum and has a direct effect on the
experimental animals suggest that CCK may decrease
feeding mainly by
is secreted from the entire gas-
blood concentrations rising to peak levels 1 to 2 hours
injections of PYY into mice have been shown to
tance of this gastrointestinal hormone in regulating
presence of food in the intestines stimulates them to
secrete
which in turn enhances
glucose-dependent insulin production and secretion
stimulates the release of several gastrointestinal hor-
mones that may induce satiety and reduce further
Ghrelin—a Gastrointestinal Hormone—Increases Feeding.
Ghrelin
uncertain.
Summary of Long-Term Regulation.
feeding behavior, as well as social and cultural factors
people, who continue to eat despite very high levels of
is, leptin receptors or post-receptor signaling pathways
adiposity. Therefore, some physiologists believe that
to be a deficiency of leptin production, because plasma
most obese humans, however, there does not appear
marked hyperphagia and morbid obesity occur. In
cause defective leptin receptors in the hypothalamus,
necessary.
Thus, leptin may be an important means by which
creatic beta cells, which decreases energy storage.
ture; and (5)
that decrease food intake; (4)
hormone,
mus of substances, such as
receptors; (3) increased production in the hypothala-
activation of POMC neurons,
AGRP;
hypothalamus of appetite stimulators, such as
storage, including (1) decreased production in the
hypothalamus, especially the POMC neurons of the
Leptin then circulates to the brain, where it moves
amounts of leptin, which is released into the blood.
energy storage), the adipocytes produce increased
peptide hormone released from adipocytes. When the
ent individuals. What regulates this energy reserve, and
Feedback Signals from Adipose Tissue Regulate Food Intake.
which tend to correct the cold state.
and (2) provides increased fat for insulation, both of
system. This is important, because increased food
intake. This is caused by interaction within the hypo-
it is exposed to heat, it tends to decrease its caloric
is exposed to cold, it tends to increase feeding; when
When an animal
Temperature Regulation and Food Intake.
neurons or other closely associated neurons.
In addition, some amino acids and lipid
hypothalamus.
(2) The same increase in blood
the hypothalamus.
vations: (1) A rise in blood
static, and lipostatic theories, by the following obser-
areas of the brain also support the glucostatic, amino-
decreases, the desire for feeding is increased, eventu-
theories of regulation. That is, when the avail-
and some fatty acids, leading to the
hunger, which has led to the so-called
Lipids on Hunger and Feeding.
tional status of the body.
eat according to its own desires. Thus, the feeding
regular diet. Conversely, an animal that has been force-
Intermediate and Long-Term Regulation
nal filling.
minutes, than is the inhibition caused by gastrointesti-
of shorter duration, usually lasting for only 20 to 40
inhibited. However, the inhibition caused by this
passed, the hypothalamic feeding center becomes
through the mouth, and after a certain amount has
lowing, and tasting, “meter” the food as it passes
related to feeding, such as chewing, salivation, swal-
Therefore, it is postulated that various “oral factors”
mouth. This effect occurs despite the fact that the gas-
exterior, the degree of hunger is decreased after a
an esophageal fistula is fed large quantities of food,
When an animal with
Dietary Balances; Regulation of Feeding; Obesity and Starvation; Vitamins and Minerals
Chapter 71
871
Oral Receptors Meter Food Intake.
even though this food is immediately lost again to the
reasonable quantity of food has passed through the
trointestinal tract does not become the least bit filled.
metering mechanism is considerably less intense and
of Food Intake
An animal that has been starved for a long time and
is then presented with unlimited food eats a far greater
quantity than does an animal that has been on a
fed for several weeks eats very little when allowed to
control mechanism of the body is geared to the nutri-
Effect of Blood Concentrations of Glucose, Amino Acids, and
It has long been known that
a decrease in blood glucose concentration causes
glucostatic
theory of hunger and feeding regulation. Similar
studies have demonstrated the same effect for blood
amino acid concentration and blood concentration of
breakdown products of lipids such as the keto acids
aminostatic and
lipostatic
ability of any of the three major types of food
ally returning the blood metabolite concentrations
back toward normal.
Neurophysiologic studies of function in specific
glucose level increases the
rate of firing of glucoreceptor neurons in the satiety
center in the ventromedial and paraventricular nuclei of
glucose level simultaneously decreases the firing of glu-
cosensitive neurons in the hunger center of the lateral
substances affect the rates of firing of these same
thalamus between the temperature-regulating system
(see Chapter 73) and the food intake–regulating
intake in a cold animal (1) increases its metabolic rate
Most of the stored energy in the body consists of fat,
the amount of which can vary considerably in differ-
why is there so much variability among individuals?
Recent studies suggest that the hypothalamus
senses energy storage through the actions of leptin, a
amount of adipose tissue increases (signaling excess
across the blood-brain barrier by facilitated diffusion
and occupies leptin receptors at multiple sites in the
arcuate nuclei and neurons of the paraventricular
nuclei.
Stimulation of leptin receptors in these hypothala-
mic nuclei initiates multiple actions that decrease fat
NPY
and
(2)
causing
release of
a-MSH and activation of melanocortin
corticotropin-releasing
increased
sympathetic nerve activity (through neural projections
from the hypothalamus to the vasomotor centers),
which increases metabolic rate and energy expendi-
decreased insulin secretion by the pan-
the adipose tissue signals the brain that enough energy
has been stored and that intake of food is no longer
In mice or humans with mutations that render their
fat cells unable to produce leptin or mutations that
leptin levels increase in proportion with increasing
obesity may be associated with leptin resistance; that
normally activated by leptin may be defective in obese
leptin.
Another explanation for the failure of leptin to
prevent increasing adiposity in obese individuals is
that there are many redundant systems that control
that can cause continued excess food intake even in
the presence of high levels of leptin.
Even though our
information on the different feedback factors in
As discussed previously,
tribute to Abnormal Feeding.
behavior, excessive energy intake, and obesity.
food intake, there are also important environmental and
Abnormal Feeding Behavior Is an Important Cause of Obesity.
means of reducing fat stores.
body, increased physical activity is often an effective
stopped. Because muscular activity is by far the most
resulting in significant weight loss. Even a single episode
increases energy expenditure more than food intake,
way. In obese people, increased physical activity usually
in a laborer, as much as 60 to 70 per cent is used in this
by the average person goes into muscular activity, and
sion watching, and obesity.
between sedentary behaviors, such as prolonged televi-
For example, studies have shown a close association
with decreased muscle mass and increased adiposity.
muscle mass and decrease body fat mass, whereas
ical activity and physical training are known to increase
Sedentary Lifestyle Is a Major Cause of Obesity.
could not have occurred so rapidly.
and environmental factors, because genetic changes
may play the dominant role in many obese people. The
energy metabolism, lifestyle and environmental factors
play an important role in determining food intake and
The causes of obesity are complex. Although genes
Causes of Obesity
Decreased Physical Activity and
than energy expenditure.
output. For a person to lose weight, energy intake must
is obtained, energy intake once again equals energy
taining twice as much lipid, as a lean person.
as many as four times as many adipocytes, each con-
size, of adipocytes.An extremely obese person may have
accompanied by increased numbers, as well as increased
life and that the development of obesity in adults is
tiate from fibroblast-like preadipocytes at any period of
however, have shown that new adipocytes can differen-
. Recent studies,
size, resulting in
oping in adults was thought to increase only adipocyte
increases in adipocyte size. In contrast, obesity devel-
increased numbers of adipocytes and only small
hyperplastic obesity,
infancy and childhood and that excess energy intake
adipocytes could increase substantially only during
nificant amounts of lipids in obese persons. The meta-
tissue and in the intraperitoneal cavity, although the
Fat is stored mainly in adipocytes in subcutaneous
9.3 Calories of excess energy that enter the body,
by energy intake in excess of energy output. For each
as fat. Therefore, excessive adiposity (obesity) is caused
weight increases, and most of the excess energy is stored
food) enter the body than are expended, the body
When greater quantities of energy (in the form of
nearly 33 per cent of adults are obese.
cent of adults in the United States are overweight, and
per cent over the past decade. Approximately 64 per
countries is rapidly increasing, rising by more than 30
The prevalence of obesity in children and adults in
assess obesity.
in clinical practice, where BMI is commonly used to
or underwater weighing, these methods are rarely used
measuring skin-fold thickness, bioelectrical impedance,
body fat can be estimated with various methods, such as
per cent or greater in women. Although percentage of
percentage of total body fat. Obesity is usually defined
viduals have a high BMI due to a large muscle mass. A
called obese. BMI is not a direct estimate of adiposity
called overweight, and a BMI greater than 30 kg/m
In clinical terms, a BMI between 25 and 29.9 kg/m
Weight in kg/Height m
index (BMI), which is calculated as:
rogate marker for body fat content is the body mass
Obesity can be defined as an excess of body fat. A sur-
becoming periodically overburdened. Second, they
steadier pace, so that its digestive and absorptive
smaller quantities at each eating session, thus allowing
other purposes. First, they tend to make the person eat
too high. The short-term regulatory stimuli serve two
the tissues, preventing them from becoming too low or
nisms, helps maintain constant stores of nutrients in
The long-term regulatory system for feeding, which
Term Regulatory Systems for Feeding
Importance of Having Both Long- and Short-
the sensation of hunger and develops a state of satiety.
stores) are already abundant, the person usually loses
conversely, when the energy stores (mainly the fat
of the brain become highly active, and the person
energy stores of the body fall below normal, the
make the following general statement: When the
long-term feeding regulation is imprecise, we can
Metabolism and Temperature Regulation
872
Unit XIII
feeding centers of the hypothalamus and other areas
exhibits increased hunger as well as searching for food;
includes all the nutritional energy feedback mecha-
food to pass through the gastrointestinal tract at a
mechanisms can work at optimal rates rather than
help prevent the person from eating amounts at each
meal that would be too much for the metabolic storage
systems once all the food has been absorbed.
Obesity
BMI
=
2
2
is
2
is
and does not take into account the fact that some indi-
better way to define obesity is to actually measure the
as 25 per cent or greater total body fat in men and 35
the United States and in many other industrialized
Obesity Results from Greater Energy Intake than Energy Expendi-
ture.
approximately 1 gram of fat is stored.
liver and other tissues of the body often accumulate sig-
bolic processes involved in fat storage were discussed in
Chapter 68.
It was previously believed that the number of
in children led to
associated with
hypertrophic obesity
Once a person has become obese and a stable weight
be less
Abnormal Feeding Regulation as
rapid increase in the prevalence of obesity in the past
20 to 30 years emphasizes the important role of lifestyle
Regular phys-
inadequate physical activity is typically associated
About 25 to 30 per cent of the energy used each day
of strenuous exercise may increase basal energy expen-
diture for several hours after the physical activity is
important means by which energy is expended in the
Although powerful physiologic mechanisms regulate
psychological factors that can cause abnormal feeding
Environmental, Social, and Psychological Factors Con-
the importance of environmental factors is evident from
persons with increased physical activity. The more
as well as loss of fat-soluble vitamins in the feces.
loss may cause unpleasant gastrointestinal side effects,
therefore reduces energy absorption. However, fecal fat
This causes a
orlistat, a lipase inhibitor,
metabolism. For example,
to the drug, so that weight reduction is usually no
elevating the blood pressure. Also, a person soon adapts
central nervous system, making the person nervous and
and increases energy expenditure. The danger in using
tramine,
in the brain. One drug for treating obesity is
derivatives), which directly inhibit the feeding centers
have been used in the treatment of obesity. The most
Various
nection with starvation, it is important to prevent
much by habit as by hunger. As pointed out later in con-
even more, but human beings can often fool themselves
appeases hunger. In most lower animals, such a proce-
This bulk distends the stomach and thereby partially
generally made up of non-nutritive cellulose substances.
designed to contain large quantities of “bulk,” which is
To decrease energy intake, most reducing diets are
weight loss.
attempting to lose weight, increasing physical activity is
10 per cent weight loss after 6 months. For most people
weight loss of about 1 to 2 pounds per week, or about a
deficit, if it can be achieved and sustained, will cause a
. Typically, such an energy
BMIs greater than 35 kg/m
week. A more aggressive energy deficit of 500 to 1000
persons (BMI greater than 25 but less than 35 kg/m
ing energy intake or increasing energy expenditure. The
loss is achieved. In other words, this means either reduc-
Treatment of obesity depends on decreasing energy
Treatment of Obesity
ence the amount and distribution of body fat.
small percentage of obesity. It is likely that many gene
also very rare. All these
tions of the leptin receptor,
of the leptin gene, which are very rare; and (3)
far; (2)
of obesity are (1)
fat storage. Three of the monogenic (single-gene) causes
factors.
Current evidence, however, suggests that 20 to 25 per
same eating habits and physical activity patterns.
the precise role of genetics in contributing to obesity,
runs in families. Yet it has been difficult to determine
Genetic Factors as a Cause of Obesity.
loss. Some of these changes include increased formation
when food intake is restricted in obese animals, there
that the “set-point” of an obese person’s feeding control
far greater than that of a normal person. This indicates
feeding. In support of this theory, an obese person who
that in nonobese persons. Also, there may be abnor-
found in obese people, it is possible that the functional
hypothalamus.
in human beings, too, can result from damage to the
develop progressive obesity, demonstrating that obesity
excessively and become obese. People with hypophysial
We pre-
Neurogenic Abnormalities as a Cause of Obesity.
obesity.
especially in infancy and, to a lesser extent, during the
much as three times that in normal children. Therefore,
The number of fat cells in obese children is often as
rate of fat storage, the greater the number of fat cells.
rapid in the first few years of life, and the greater the
The rate of formation of new fat cells is especially
throughout life.
parents, and the children continue to practice it
a day and that each meal must be filling. Many young
Childhood Overnutrition as a Possible Cause of Obesity.
mental depression. It seems that eating can be a means
such as the death of a parent, a severe illness, or even
amounts of weight during or after stressful situations,
some people. For example, people often gain large
and sedentary lifestyles.
industrialized countries, which has coincided with an
Dietary Balances; Regulation of Feeding; Obesity and Starvation; Vitamins and Minerals
Chapter 71
873
the rapid increase in the prevalence of obesity in most
abundance of high-energy foods (especially fatty foods)
Psychological factors may contribute to obesity in
of releasing tension.
One factor that may contribute to obesity is the preva-
lent idea that healthy eating habits require three meals
children are forced into this habit by overly solicitous
it has been suggested that overnutrition of children—
later years of childhood—can lead to a lifetime of
viously pointed out that lesions in the ventromedial
nuclei of the hypothalamus cause an animal to eat
tumors that encroach on the hypothalamus often
Although hypothalamic damage is almost never
organization of the hypothalamic or other neurogenic
feeding centers in obese individuals is different from
malities of neurotransmitters or receptor mechanisms in
the neural pathways of the hypothalamus that control
has reduced to normal weight by strict dietary measures
usually develops intense hunger that is demonstrably
system is at a much higher level of nutrient storage than
that of a nonobese person.
Studies in experimental animals also indicate that
are marked neurotransmitter changes in the hypothala-
mus that greatly increase hunger and oppose weight
of orexigenic neurotransmitters such as NPY and
decreased formation of anorexic substances such as
leptin and
a-MSH.
Obesity definitely
because family members generally share many of the
cent of cases of obesity may be caused by genetic
Genes can contribute to obesity by causing abnor-
malities of (1) one or more of the pathways that regu-
late the feeding centers and (2) energy expenditure and
mutations of MCR-4, the most
common monogenic form of obesity discovered thus
congenital leptin deficiency caused by mutations
muta-
monogenic forms of obesity account for only a very
variations interact with environmental factors to influ-
input below energy expenditure and creating a sus-
tained negative energy balance until the desired weight
current National Institutes of Health (NIH) guidelines
recommend a decrease in caloric intake of 500 kilo-
calories per day for overweight and moderately obese
2
) to
achieve a weight loss of approximately 1 pound each
kilocalories per day is recommended for persons with
2
also an important component of successful long-term
dure simply makes the animal increase its food intake
because their food intake is sometimes controlled as
vitamin deficiencies during the dieting period.
drugs for decreasing the degree of hunger
widely used drugs are amphetamines (or amphetamine
sibu-
a sympathomimetic that reduces food intake
these drugs is that they simultaneously overexcite the
greater than 5 to 10 per cent.
Another group of drugs works by altering lipid
reduces the intestinal digestion of fat.
portion of the ingested fat to be lost in the feces and
Significant weight loss can be achieved in many obese
by the brain. After the readily mobilized protein stores
finally, rapid depletion again shortly before death. The
depletion at first, then greatly slowed depletion, and,
Protein undergoes three phases of depletion: rapid
body are gone.
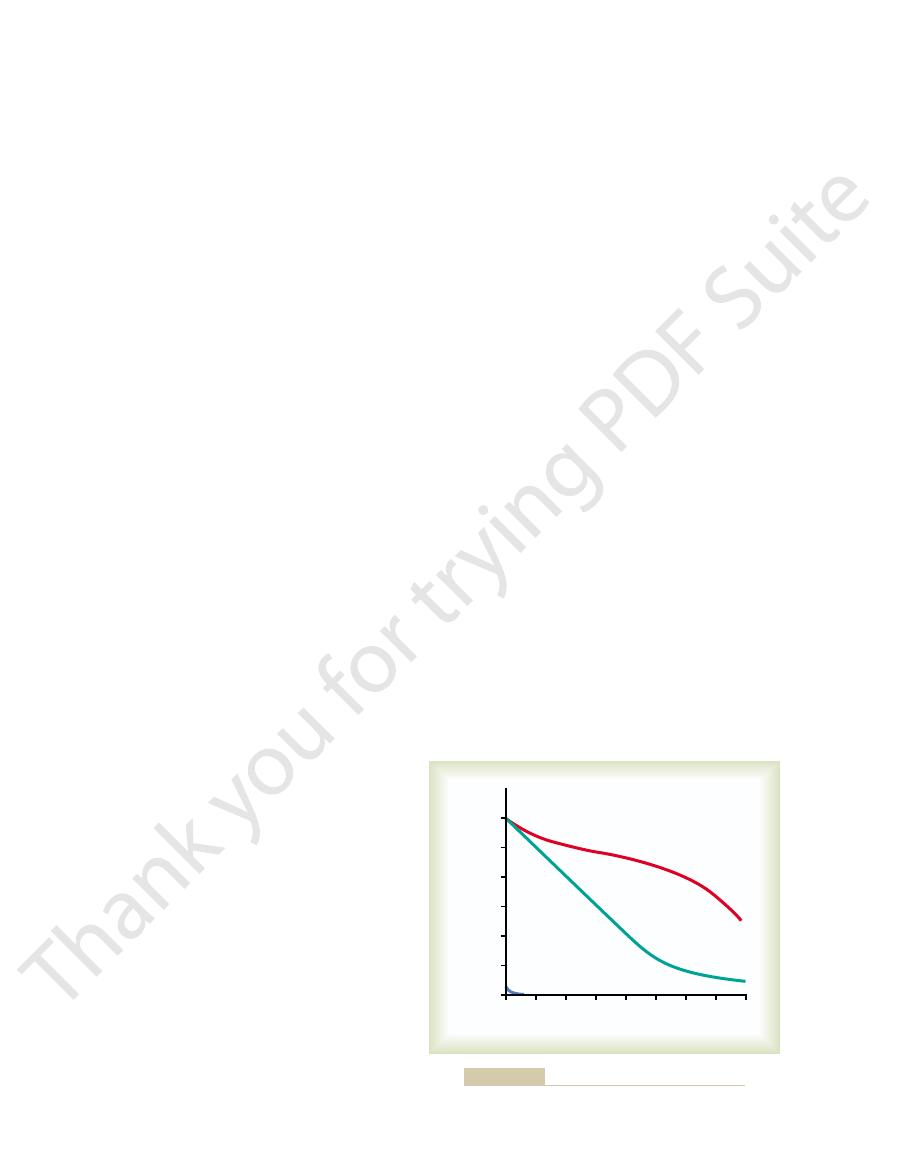
shown in Figure 71–3, until most of the fat stores in the
energy), the rate of fat depletion continues unabated, as
progressive depletion of tissue fat and protein. Because
the first few hours of starvation, the major effects are
functions for perhaps half a day. Therefore, except for
muscles), and it can supply the energy required for body
for energy over both fat and protein, the quantity of car-
Depletion of Food Stores in the Body Tissues During Starvation.
Starvation
and to develop therapeutic agents to improve their
in experimental animals. Additional research, however,
food intake are still unclear, but blockade of the hypo-
ucts interact with the melanocortin pathway to decrease
precise mechanisms by which cytokines or tumor prod-
in the hypothalamus. The
cytokines appear to mediate anorexia by activation of
anorexia and cachexia. Most of these inflammatory
, have been shown to cause
proteolysis-inducing factor
, interleukin-6
necrosis factor-
Several inflammatory cytokines,
including
contribute to cancer-induced anorexia and cachexia.
drome during the course of their disease.
half of cancer patients develop anorexia-cachexia syn-
cancer cause both anorexia and cachexia, and more than
chronic inflammatory disorders. Almost all types of
with acquired immunodeficiency syndrome (AIDS) and
or in the “wasting syndrome” observed in patients
cachexia often occur together in many types of cancer
caused by reduced food intake alone. Anorexia and
expenditure leading to weight loss greater than that
Cachexia
occurs.
becomes nauseated by food; as a result, severe inanition
less food.
pain and nausea, may also cause a person to consume
such as cancer, when other common problems, such as
anisms in the pathophysiology of anorexia in diseases
the literal definition of “not eating.” This definition
, as opposed to
caused primarily by diminished appetite
a reduction in food intake
weight loss.
with increased energy expenditure, causing serious
as cancer, the reduced desire for food may be associated
instances, especially in those with serious diseases such
and factors released from peripheral tissues. In many
chogenic disturbances, hypothalamic abnormalities,
that greatly decrease the desire for food, including psy-
by extreme weight loss. It can be caused by inadequate
Inanition, Anorexia, and
patients, they are major operations, and their long-
eaten at each meal. Although these surgical procedures
near its upper end; this also creates a small stomach
involves placing an adjustable band around the stomach
Gastric banding surgery
of the stomach with staples.
lengths; the pouch is separated from the remaining part
bypass surgery
bypass surgery and gastric banding surgery.
Two of the most common surgical procedures used in
them to other serious diseases, various surgical proce-
morbidly obese patients with BMIs greater than 40, or
activity combined with a reduction in caloric intake. For
treatment. The current clinical guidelines for the treat-
Therefore, forced exercise is often an essential part of
ture and the more rapidly the obesity disappears.
exercise one gets, the greater the daily energy expendi-
Metabolism and Temperature Regulation
874
Unit XIII
ment of obesity recommend that the first step be
lifestyle modifications that include increased physical
for patients with BMIs greater than 35 and conditions
such as hypertension or type II diabetes that predispose
dures can be used to decrease the fat mass of the body
or to decrease the amount of food that can be eaten at
each meal.
the United States to treat morbid obesity are gastric
Gastric
involves construction of a small pouch in
the proximal part of the stomach that is then connected
to the jejunum with a section of small bowel of varying
pouch that restricts the amount of food that can be
generally produce substantial weight loss in obese
term effects on overall health and mortality are still
uncertain.
Cachexia
Inanition is the opposite of obesity and is characterized
availability of food or by pathophysiologic conditions
Anorexia can be defined as
emphasizes the important role of central neural mech-
Anorexia nervosa is an abnormal psychic state
in which a person loses all desire for food and even
is a metabolic disorder of increased energy
Central neural and peripheral factors are believed to
tumor
a
, interleukin-1
b, and a
the melanocortin system
thalamic melanocortin receptors appears to almost
completely prevent their anorexic and cachectic effects
is needed to better understand the pathophysiologic
mechanisms of anorexia and cachexia in cancer patients
nutritional status and survival.
Even though the tissues preferentially use carbohydrate
bohydrate normally stored in the entire body is only a
few hundred grams (mainly glycogen in the liver and
fat is the prime source of energy (100 times as much fat
energy is stored in the normal person as carbohydrate
initial rapid depletion is caused by the use of easily
mobilized protein for direct metabolism or for conver-
sion to glucose and then metabolism of glucose mainly
have been depleted during the early phase of starvation,
1
2
3
4
5
6
7
8
0
Fat
Protein
Carbohydrate
Quantities of stored foodstuffs
(kilograms)
Weeks of starvation
12
10
8
6
4
2
0
Effect of starvation on the food stores of the body.
Figure 71–3
associated with thiamine deficiency.
hydrates and many amino acids. The decreased utiliza-
tissues, but increased utilization of fats. Thus, thiamine
Thiamine deficiency
-keto acids, as discussed
cocarboxylase,
thiamine pyrophosphate;
Thiamine operates in the metabolic systems of the body
Thiamine (Vitamin B
“anti-infection” vitamin.
respiratory passages. Vitamin A has been called an
tivae of the eyes, the linings of the urinary tract, and the
tures often become infected, for example, the conjunc-
In vitamin A deficiency, the damaged epithelial struc-
corneal opacity and blindness.
and (4) keratinization of the cornea, with resultant
sometimes with interruption of the female sexual cycle;
(3) failure of reproduction, associated especially with
young animals, including cessation of skeletal growth;
the skin and sometimes acne; (2) failure of growth of
Vitamin A deficiency manifests itself by (1) scaliness of
cells. When vitamin A is lacking, the epithelial structures
Vitamin A is also necessary for normal growth of
prevent night blindness.
needed to form the visual pigments and, therefore, to
eye, which is discussed in Chapter 50. Vitamin A is
One basic function of vitamin A is
A, can be changed into vitamin A in the liver.
which, because
carotenoid pigments,
abundance in many vegetable foods. These are the
for the formation of vitamin A do occur in
provitamins
vitamin does not occur in foods of vegetable origin, but
This
Vitamin A occurs in animal tissues as
Vitamin A
weeks.
water-soluble vitamin, can cause symptoms within a few
for a year or longer). Absence of vitamin C, another
, which can last in the liver in a bound form
B compounds, clinical symptoms of the deficiency can
compounds. When a person’s diet is deficient in vitamin
tively slight. This applies especially to most vitamin B
The storage of most water-soluble vitamins is rela-
months without any additional intake of vitamin D.
vitamin A. The quantity of vitamin D stored in the liver
vitamin A stored in the liver may be sufficient to main-
major extent in the liver. For instance, the quantity of
slight extent in all cells. Some vitamins are stored to a
Vitamins are stored to a
Storage of Vitamins in the Body.
of exercise, and pregnancy.
ing on such factors as body size, rate of growth, amount
person. These requirements vary considerably, depend-
tant metabolic deficits. Table 71–3 lists the amounts
the body. Lack of vitamins in the diet can cause impor-
Vitamins
ciencies can occur. These deficiencies can add to the
appear, and after several weeks, severe vitamin defi-
starvation, mild vitamin deficiencies usually begin to
starvation. Consequently, after a week or more of
vitamins, especially the water-soluble vitamins—the
The stores of some of the
Vitamin Deficiencies in Starvation.
tion, death ordinarily ensues when the proteins of the
again enter a stage of rapid depletion. Because proteins
energy is protein. At that time, the protein stores once
almost depleted, and the only remaining source of
There finally comes a time when the fat stores are
protein stores of the body.
principally from beta-hydroxybutyrate. This sequence
brain’s energy is now derived from these ketone bodies,
cells for energy. Therefore, about two thirds of the
Chapter 68. The ketone bodies, like glucose, can cross
ketosis,
some of the fat breakdown products to ketone bodies,
of protein becomes greatly decreased. The lessened
to one fifth its previous rate, and the rate of depletion
time, the rate of gluconeogenesis decreases to one third
the remaining protein is not so easily removed. At this
Dietary Balances; Regulation of Feeding; Obesity and Starvation; Vitamins and Minerals
Chapter 71
875
availability of glucose then initiates a series of events
that leads to excessive fat utilization and conversion of
producing the state of
which is discussed in
the blood-brain barrier and can be used by the brain
of events leads to at least partial preservation of the
are also essential for the maintenance of cellular func-
body have been depleted to about half their normal
level.
vitamin B group and vitamin C—do not last long during
debility that leads to death.
Daily Requirements of Vitamins.
A vitamin is an organic
compound needed in small quantities for normal
metabolism that cannot be manufactured in the cells of
of important vitamins required daily by the average
tain a person for 5 to 10 months without any intake of
is usually sufficient to maintain a person for 2 to 4
sometimes be recognized within a few days (except for
vitamin B
12
weeks and can cause death from scurvy in 20 to 30
retinol.
yellow and red
their chemical structures are similar to that of vitamin
Vitamin A Deficiency Causes “Night Blindness” and Abnormal
Epithelial Cell Growth.
its use in the formation of the retinal pigments of the
most cells of the body and especially for normal growth
and proliferation of the different types of epithelial
of the body tend to become stratified and keratinized.
atrophy of the germinal epithelium of the testes and
1
)
principally as
this compound
functions as a
operating mainly in con-
junction with a protein decarboxylase for decarboxyla-
tion of pyruvic acid and other
a
in Chapter 67.
(beriberi) causes decreased uti-
lization of pyruvic acid and some amino acids by the
is specifically needed for the final metabolism of carbo-
tion of these nutrients is responsible for many debilities
Table 71–3
Pyridoxine
2 mg
Folic acid
0.4 mg
K
70
E
15 IU
D
400 IU
Ascorbic acid
45 mg
Niacin
20 mg
Riboflavin
1.8 mg
Thiamine
1.5 mg
A
5000 IU
Vitamin
Amount
Required Daily Amounts of Vitamins
mg
B
12
3
mg
Pantothenic acid
Unknown
activity.
Vitamin B
combined deficiency of a number of vitamins, as well as
kwashiorkor,
beriberi, sprue,
or both. Many deficiency syndromes, including
occurs in association with deficiency of thiamine, niacin,
are usually relatively mild, this deficiency frequently
Although the manifestations of riboflavin deficiency
mouth, headaches, mental depression, forgetfulness, and
of the skin and eyes, cracking at the corners of the
ciency causes digestive disturbances, burning sensations
riboflavin deficiency is probably common. Such defi-
debilities noted in experimental animals, but mild
riboflavin deficiency severe enough to cause the marked
In the human being, there are no known cases of
ally depressed oxidative processes within the cells.
effects as a lack of niacin in the diet; presumably, the
severe riboflavin deficiency can cause many of the same
and decline in body temperature, and then death. Thus,
spasticity that finally becomes muscle weakness, coma
causes severe dermatitis, vomiting, diarrhea, muscle
Deficiency of riboflavin in experimental animals
and then passes the hydrogen to FMN or FAD; finally,
in association with specific dehydrogenases, usually
tive systems of the mitochondria. NAD, operating
They operate as hydrogen carriers in important oxida-
flavin adenine dinucleotide (FAD).
phoric acid to form two coenzymes,
Riboflavin (Vitamin B
ties to niacin in the body.
tryptophan, which can be converted in limited quanti-
a corn diet, because corn is deficient in the amino acid
deficiency. Pellagra is greatly exacerbated in people on
black tongue
The clinical entity called
and failure of appropriate epithelial repair.
widespread gastrointestinal hemorrhage in severe cases.
and other portions of the gastrointestinal tract, result-
Niacin deficiency causes intense irritation and
to repair irritative damage.
that in persons with niacin deficiency, the skin is unable
mechanical irritation or sun irradiation; thus, it appears
choses may result. Also, the skin develops a cracked,
system, and permanent dementia or many types of psy-
deficiency, actual tissue death ensues. Pathological
dular secretion may occur, but in severe niacin
In the early stages of niacin deficiency, simple phys-
ments of all cells cannot occur at normal rates.
tion cannot be maintained; therefore, oxidative delivery
ciency of niacin exists, the normal rate of dehydrogena-
coenzymes is presented in Chapter 67. When a defi-
of dehydrogenases. The typical operation of both these
hydrogen acceptors; they combine with hydrogen atoms
cleotide phosphate (NADP). These coenzymes are
dinucleotide (NAD) and nicotinamide adenine dinu-
Niacin, also called
predominate.
intestinal disorders, is frequently referred to as
polyneuritis, cardiovascular symptoms, and gastro-
The overall picture of thiamine deficiency, including
gastric atony, and hypochlorhydria.All these effects pre-
ciency are indigestion, severe constipation, anorexia,
Thiamine Deficiency Causes Gastrointestinal Tract Disturbances.
because of cardiac failure.
extent in some people with thiamine deficiency, mainly
Peripheral edema
partly to primary weakness of the cardiac muscle.
cular dilation. The cardiac effects of thiamine deficiency
of metabolic energy in the tissues, leading to local vas-
tory system, presumably as a result of decreased release
times normal. This occurs because thiamine deficiency
ened cardiac muscle. Further, the venous return of
cardiac failure
A person with severe thiamine deficiency
Vasodilation.
Thiamine Deficiency Weakens the Heart and Causes Peripheral
ing in severe weakness.
in the absence of paralysis, the muscles atrophy, result-
occasionally results; even
nerves. Also, fiber tracts in the cord can degenerate to
table, resulting in “polyneuritis,” characterized by pain
the central nervous system. Lesions in the peripheral
Thiamine deficiency can cause
cells with poor nutrition. These changes can disrupt
ciency, changes that are characteristic of neuronal
ketone bodies derived from fat metabolism. The neu-
drates for its energy. In thiamine deficiency, the utiliza-
The central nervous system normally
Nervous Systems.
Metabolism and Temperature Regulation
876
Unit XIII
Thiamine Deficiency Causes Lesions of the Central and Peripheral
depends almost entirely on the metabolism of carbohy-
tion of glucose by nervous tissue may be decreased 50
to 60 per cent and is replaced by the utilization of
ronal cells of the central nervous system frequently
show chromatolysis and swelling during thiamine defi-
communication in many portions of the central nervous
system.
degeneration of myelin
sheaths of nerve fibers in both the peripheral nerves and
nerves frequently cause them to become extremely irri-
radiating along the course of one or many peripheral
such an extent that paralysis
eventually develops
because of weak-
blood to the heart may be increased to as much as two
causes peripheral vasodilation throughout the circula-
are due partly to high blood flow into the heart and
and ascites also occur to a major
Among the gastrointestinal symptoms of thiamine defi-
sumably result from failure of the smooth muscle and
glands of the gastrointestinal tract to derive sufficient
energy from carbohydrate metabolism.
beriberi—especially when the cardiovascular symptoms
Niacin
nicotinic acid, functions in the body
as coenzymes in the form of nicotinamide adenine
as they are removed from food substrates by many types
of energy from the foodstuffs to the functioning ele-
iologic changes such as muscle weakness and poor glan-
lesions appear in many parts of the central nervous
pigmented scaliness in areas that are exposed to
inflammation of the mucous membranes of the mouth
ing in many digestive abnormalities that can lead to
It is possible that this results from generalized depres-
sion of metabolism in the gastrointestinal epithelium
pellagra and the canine
disease called
are caused mainly by niacin
2
)
Riboflavin normally combines in the tissues with phos-
flavin mononu-
cleotide (FMN) and
accepts hydrogen removed from various food substrates
the hydrogen is released as an ion into the mitochon-
drial matrix to become oxidized by oxygen (described
in Chapter 67).
debilities that result in each instance are due to gener-
so on.
pellagra,
and
are probably due to a
other aspects of malnutrition.
12
Several cobalamin compounds that possess the common
prosthetic group shown next exhibit so-called vitamin
B
12
membranes.
olism, especially protein metabolism. Also, it is believed
As a result, pyridoxine plays many key roles in metab-
transamination process for the synthesis of amino acids.
pyridoxal phosphate
Pyridoxine (Vitamin B
acid alone.
anemia. This often can be treated effectively with folic
deficiency is the development of
cells. One of the significant effects of folic acid
in Chapter 32. However, vitamin B
for the maturation of red blood cells, as discussed
, is important
and, like vitamin B
Folic acid is an even more potent growth promoter
very little.
Indeed, when it is absent from the diet, an animal grows
the cellular genes. This may explain one of the most
, is required for replication of
folic acid, like vitamin B
Therefore,
which are required for formation of DNA.
use in the body is in the synthesis of purines and thymine,
Perhaps its most important
methyl and formyl groups.
effect.” Folic acid functions as a carrier of hydroxy-
Several pteroylglutamic acids exhibit the “folic acid
Folic Acid (Pteroylglutamic Acid)
cussed in Chapters 32 and 66.
by the ileal mucosa. This is dis-
intrinsic factor,
of this vitamin in the food but deficiency of formation
deficiency is not lack
The usual cause of vitamin B
sensation and, in severe cases, even become paralyzed.
lateral columns, of the spinal cord. As a result, many
cially in the posterior columns, and occasionally the
deficiency occurs espe-
The demyelination of nerve
Deficiency Causes Demyelination of the Large Nerve
32 in relation to pernicious anemia, a type of anemia
This red cell function is described in detail in Chapter
: (1) promotion of growth and (2)
replication of genes. This could explain the major func-
deoxyribonucleotides, a step that is necessary in the
gen acceptor coenzyme. Its most important function is
performs several metabolic functions, acting as a hydro-
Vitamin B
combine reversibly with other substances.
molecule. It is likely that the cobalt atom functions in
Note that this prosthetic group contains cobalt, which
Dietary Balances; Regulation of Feeding; Obesity and Starvation; Vitamins and Minerals
Chapter 71
877
has bonds similar to those of iron in the hemoglobin
much the same way that the iron atom functions to
Vitamin B
12
Deficiency Causes Pernicious Anemia.
12
to act as a coenzyme for reducing ribonucleotides to
tions of vitamin B
12
promotion of red blood cell formation and maturation.
caused by failure of red blood cell maturation when
vitamin B
12
is deficient.
Vitamin B
12
Fibers of the Spinal Cord.
fibers in people with vitamin B
12
people with pernicious anemia have loss of peripheral
12
of
which is normally secreted by the
parietal cells of the gastric glands and is essential for
absorption of vitamin B
12
12
important functions of folic acid—to promote growth.
than vitamin B
12
12
12
and folic acid
each perform specific and different chemical functions
in promoting growth and maturation of red blood
macrocytic anemia,
almost identical to that which occurs in pernicious
6
)
Pyridoxine exists in the form of
in
the cells and functions as a coenzyme for many chemi-
cal reactions related to amino acid and protein metab-
olism. Its most important role is that of coenzyme in the
to act in the transport of some amino acids across cell
Co
N
CH
2
N
N
N
N
Pyridoxine
H
2
C
OH
OH
OH
CH
2
CH
3
N
subcutaneous tissue, cartilage, bone, and teeth.
the body are defective and weak. Therefore, this vitamin
gral constituent of collagen. Without ascorbic acid, the
ylation step in the formation of hydroxyproline, an inte-
prolyl hydroxylase,
the Body.
Ascorbic Acid Deficiency Weakens Collagen Fibers Throughout
Ascorbic Acid (Vitamin C)
the body; indeed, it is perhaps as necessary as any other
synthesized in the body. This does not mean that pan-
deficiency syndrome has been proved, presumably
adrenocortical necrosis. In the human being, no definite
of the hair, dermatitis, fatty liver, and hemorrhagic
cause retarded growth, failure of reproduction, graying
Deficiency of pantothenic acid in lower animals can
carbohydrates and fats.
Thus, lack of pan-
cycle, and (2) degradation of fatty acid molecules into
the cells. Two of these discussed at length in Chapters
(CoA), which has many metabolic roles in
disturbances such as nausea and vomiting.
known to cause seizures, dermatitis, and gastrointestinal
tion. Rarely, in children, pyridoxine deficiency has been
fatty liver, anemia, and evidence of mental deteriora-
dermatitis, decreased rate of growth, development of
Dietary lack of pyridoxine in lower animals can cause
Pantothenic Acid
Pantothenic acid mainly is incorporated in the body into
coenzyme A
67 and 68 are (1) conversion of decarboxylated pyruvic
acid into acetyl-CoA before its entry into the citric acid
multiple molecules of acetyl-CoA.
tothenic acid can lead to depressed metabolism of both
because of the wide occurrence of this vitamin in almost
all foods and because small amounts can probably be
tothenic acid is not of value in the metabolic systems of
vitamin.
Ascorbic acid is essential for activating the
enzyme
which promotes the hydrox-
collagen fibers that are formed in virtually all tissues of
is essential for the growth and strength of the fibers in
tability of the nervous system, peripheral vasodilation,
activity as well as skeletal muscle contraction. This latter
slight, only 1.8 to 2.5 mEq/L. Increased extracellular
The extracellular fluid magnesium concentration is
for many intracellular enzymatic reactions, particularly
cells as potassium. Magnesium is required as a catalyst
Table 71–5.
71–4, and the daily requirements of these are given in
content of the most important minerals is listed in Table
not covered elsewhere are mentioned here. The body
points in the text. Only specific functions of minerals
potassium, and chloride, are presented at appropriate
The functions of many of the minerals, such as sodium,
tities of antibiotic drugs, vitamin K deficiency occurs
ciency in the diet. However, when the bacteria of the
have a bleeding tendency because of vitamin K defi-
sized by bacteria in the colon, it is rare for a person to
exhibit vitamin K activity. Because vitamin K is synthe-
Several compounds, both natural and synthetic,
dicumarol, are presented in greater detail in Chapter 35.
its relation to some of the anticoagulants, such as
clotting is retarded. The function of this vitamin and
tion. Therefore, when vitamin K deficiency occurs, blood
Factor X, all of which are important in blood coagula-
prothrombin, Factor VII (proconvertin), Factor IX, and
Vitamin K is necessary for the formation by the liver of
Vitamin K
membrane.
the mitochondria, the lysosomes, and even the cell
in the cells becomes diminished, causing abnormal
absence of vitamin E, the quantity of unsaturated fats
prevention of oxidation of unsaturated fats.
Vitamin E is believed to play a protective role in the
the muscle cells.
ciency of vitamin E prevents normal growth and some-
E is sometimes called the “antisterility vitamin.” Defi-
Because of these effects of vitamin E deficiency, vitamin
resorption of a fetus after conception in the female.
cause male sterility. Lack of vitamin E can also cause
germinal epithelium in the testis and, therefore, can
animals, lack of vitamin E can cause degeneration of the
ciency have occurred in human beings. In experimental
activity. Only rare instances of proved vitamin E defi-
Vitamin E
in calcium absorption. The specific functions of vitamin
particular, it increases the formation of a calcium-
port of calcium through the epithelium of the ileum. In
The mechanism by which vitamin D increases
the bone.
Vitamin D increases calcium absorption from the gas-
Vitamin D
occur. Finally, high fever often develops before death.
blood, bloody stools, and cerebral hemorrhage can all
teeth; infections of the mouth develop; and vomiting of
ment; lesions of the gums occur, with loosening of the
In extreme scurvy, the muscle cells sometimes frag-
acid deficiency is sufficiently severe.
the venous return of blood, the capillary pressure rises,
blood pressure cuff over the upper arm; this occludes
body. To test for ascorbic acid deficiency, one can
skin cause purpuric blotches, sometimes over the entire
throughout the body. The hemorrhages beneath the
a result, many small petechial hemorrhages occur
The capillaries are especially likely to rupture, and as
the collagen fibrils normally present in vessel walls.
The
bone matrix. Consequently, the fractured bone does not
bic acid deficiency, the osteoblasts cannot form new
growth because of failure to ossify. Also, when an
the cells, and the bones fracture easily at the point of
proliferate, but no new collagen is laid down between
The cells of the growing epiphyses continue to
growth.
necessary.
stances. As a result, healing of a wound may require
This is caused by failure of the cells to
scurvy.
during long ship voyages in the past, causes
bic acid for 20 to 30 weeks, which occurred frequently
Deficiency of ascor-
Ascorbic Acid Deficiency Causes Scurvy.
Metabolism and Temperature Regulation
878
Unit XIII
One
of the most important effects of scurvy is failure of
wounds to heal.
deposit collagen fibrils and intercellular cement sub-
several months instead of the several days ordinarily
Lack of ascorbic acid also causes cessation of bone
already ossified bone fractures in a person with ascor-
heal.
blood vessel walls become extremely fragile in
scurvy because of (1) failure of the endothelial cells to
be cemented together properly and (2) failure to form
produce such petechial hemorrhages by inflating a
and red blotches occur on the forearm if the ascorbic
trointestinal tract and helps control calcium deposition in
calcium absorption is mainly to promote active trans-
binding protein in the intestinal epithelial cells that aids
D in relation to overall body calcium metabolism and
bone formation are presented in Chapter 79.
Several related compounds exhibit so-called vitamin E
times causes degeneration of the renal tubular cells and
In the
structure and function of such cellular organelles as
colon are destroyed by the administration of large quan-
rapidly because of the paucity of this compound in the
normal diet.
Mineral Metabolism
Magnesium.
Magnesium is about one sixth as plentiful in
those related to carbohydrate metabolism.
concentration of magnesium depresses nervous system
effect can be blocked by the administration of calcium.
Low magnesium concentration causes increased irri-
Table 71–4
Iron
3
Sulfur
112
Phosphorus
670
Chloride
85
Magnesium
21
Calcium
1,160
Potassium
150
Sodium
63
Carbohydrate
300
Protein
12,600
Fat
12,600
Water
41,400
Constituent
Amount (grams)
Average Content of a 70-Kilogram Man
Iodine
0.014
mechanism. Endocrinology 145:2604, 2004.
Cowley MA, Grove KL: Ghrelin—satisfying a hunger for the
Ann N Y Acad Sci 994:175, 2003.
actions of peripheral hormones on melanocortin neurons.
Cowley MA, Cone RD, Enriori P, et al: Electrophysiological
genetics. J Clin Endocrinol Metab 89:2557, 2004.
and energy balance: insights from human and murine
Coll AP, Farooqi IS, Challis BG, et al: Proopiomelanocortin
Genet 3:589, 2002.
energy balance: perception and integration. Nat Rev
Barsh GS, Schwartz MW: Genetic approaches to studying
the mottling process.
resistant to the development of caries, the structural
osteoblasts. Even though the mottled teeth are highly
become partially inactivated. According to this theory,
ing the phosphatases, so that various metabolic systems
trace metals in some of the metabolic enzymes, includ-
tulated that in this condition, fluorine combines with
more severe state by enlarged bones. It has been pos-
fluorosis,
caries.
present, the enzymes remain inactive and cause no
enzymes that cause caries. Therefore, when fluorine is
suppressing the cariogenic process. It has been sug-
against caries. Fluorine does not make the teeth them-
element for metabolism, but the presence of a small
pyruvic acid and lactic acid. Finally, zinc is a component
the body. Consequently, zinc in small quantities is essen-
of the kidney, and the epithelial cells of many glands of
major extent in the gastrointestinal mucosa, the tubules
the alveoli. Carbonic anhydrase is also present to a
cells. This enzyme is responsible for rapid combination
carbonic anhydrase,
Zinc is an integral part of many enzymes, one of
normal metabolic rates in all cells of the body.
triiodothyronine,
thyroxine
average of only 14 milligrams. Iodine is essential for the
shown in Table 71–4, the entire body contains an
with the formation and function of thyroid hormone; as
This element is discussed in Chapter 76 in connection
The best known of the trace elements is iodine.
fluorine.
Three of the most important are iodine, zinc, and
them, a specific deficiency syndrome is likely to develop.
in foods are also usually minute. Yet without any one of
The amounts of these elements
trace elements.
Important Trace Elements in the Body.
few seconds.
the tissue cells, without which life would cease within a
oxidation that occurs in the cells. Therefore, iron is
cially the cytochromes) are present in the mitochondria
bone marrow. Electron carriers containing iron (espe-
present in other forms, especially in the liver and the
Two thirds of the iron in the body is in the
tion to the formation of hemoglobin, is discussed in
The function of iron in the body, especially in rela-
of calcium phosphate, which is discussed in Chapter 79.
and so forth. Also, bone contains a tremendous amount
triphosphate, adenosine diphosphate, phosphocreatine,
metabolic processes. Many important reactions of phos-
taneous discharge of nerve fibers, resulting in tetany, as
the other extreme, low levels of calcium can cause spon-
stop in systole and can act as a mental depressant. At
content of extracellular fluid. Excess quantities of
discussed in detail in Chapter 79, as is the calcium
form of calcium phosphate in the bone. This subject is
and cardiac arrhythmias, especially after acute myocar-
Dietary Balances; Regulation of Feeding; Obesity and Starvation; Vitamins and Minerals
Chapter 71
879
dial infarction.
Calcium.
Calcium is present in the body mainly in the
calcium ions in extracellular fluid can cause the heart to
discussed in Chapter 79.
Phosphorus.
Phosphate is the major anion of intracellular
fluid. Phosphates have the ability to combine reversibly
with many coenzyme systems and with multiple other
compounds that are necessary for the operation of
phates have been catalogued at other points in this text,
especially in relation to the functions of adenosine
Iron.
Chapter 32.
form of hemoglobin, although smaller quantities are
of all cells of the body and are essential for most of the
absolutely essential for both the transport of oxygen to
the tissues and the operation of oxidative systems within
A few elements are
present in the body in such small quantities that they
are called
Iodine.
formation of
and
the two
thyroid hormones that are essential for maintenance of
Zinc.
the most important of which is
present in especially high concentration in the red blood
of carbon dioxide with water in the red blood cells of
the peripheral capillary blood and for rapid release of
carbon dioxide from the pulmonary capillary blood into
tial for the performance of many reactions related to
carbon dioxide metabolism.
Zinc is also a component of lactic dehydrogenase and
is therefore important for the interconversions between
of some peptidases and is important for the digestion of
proteins in the gastrointestinal tract.
Fluorine.
Fluorine does not seem to be a necessary
quantity of fluorine in the body during the period of life
when the teeth are being formed subsequently protects
selves stronger but has a poorly understood effect in
gested that fluorine is deposited in the hydroxyapatite
crystals of the tooth enamel and combines with and
therefore blocks the functions of various trace metals
that are necessary for activation of the bacterial
Excessive intake of fluorine causes
which
manifests in its mild state by mottled teeth and in its
the mottled teeth and enlarged bones are due to ab-
normal enzyme systems in the odontoblasts and
strength of these teeth may be considerably lessened by
References
Table 71–5
Manganese
Unknown
Copper
Unknown
Cobalt
Unknown
Magnesium
0.4 g
Iodine
150.0
Iron
18.0 mg
Phosphorus
1.2 g
Calcium
1.2 g
Chloride
3.5 g
Potassium
1.0 g
Sodium
3.0 g
Mineral
Amount
Average Required Daily Amounts of Minerals for Adults
mg
Zinc
15 mg
weight. J Clin Endocrinol Metab 89:2576, 2004.
Wynne K, Stanley S, Bloom S:The gut and regulation of body
Physiol Gastrointest Liver Physiol 286:G7, 2004.
gastrointestinal signals that influence food intake. Am J
Woods SC: Gastrointestinal satiety signals. I. An overview of
Acad Sci 994:275, 2003.
naling and anorexia in chronic disease states. Ann N Y
Wisse BE, Schwartz MW, Cummings DE: Melanocortin sig-
Gastrointest Liver Physiol 286:G693, 2004.
peptide YY, and pancreatic polypeptide. Am J Physiol
signals. III. Glucagon-like peptide 1, oxyntomodulin,
Stanley S, Wynne K, Bloom S: Gastrointestinal satiety
901, 2003.
by the CNS: implications for obesity. Nat Rev Neurosci 4:
Seeley R, Woods S: Monitoring of stored and available fuel
66:419, 2004.
absorption of water-soluble vitamins. Annu Rev Physiol
Said HM: Recent advances in carrier-mediated intestinal
in embryonal development. Physiol Rev 80:1021, 2000.
Ross SA, McCaffery PJ, Drager UC, De Luca LM: Retinoids
224:246, 2000.
related issues: recent aspects. Proc Soc Exp Biol Med
Rindi G, Laforenza U: Thiamine intestinal transport and
Invest 109:1537, 2002.
Ravussin E: Cellular sensors of feast and famine. J Clin
Nutr 77:1352, 2003.
) and health. Am J Clin
Powers HJ: Riboflavin (vitamin B
ogy 144:3757, 2003.
obesity—lessons from monogenic disorders. Endocrinol-
O’Rahilly S, Farooqi IS, Yeo GS, Challis BG: Human
Diseases, 1998. Available at: http://www.nhlbi.nih.gov/
MD: National Heart, Lung, and Blood Institute and
and Obesity in Adults: The Evidence Report. Bethesda
Identification, Evaluation, and Treatment of Overweight
National Institutes of Health: Clinical Guidelines on the
nent for disease prevention? BMJ 328:211, 2004.
Lucock M: Is folic acid the ultimate functional food compo-
renal function. Hypertension 41:768, 2003.
Kuo JJ, Silva AA, Hall JE: Hypothalamic melanocortin
to the brain. N Engl J Med 349:926, 2003.
Korner J, Leibel RL: To eat or not to eat—how the gut talks
89:2616, 2004.
reduction: therapeutic targets. J Clin Endocrinol Metab
Korner J, Aronne LJ: Pharmacological approaches to weight
J Clin Endocrinol Metab 89:2548, 2004.
Kershaw EE, Flier JS: Adipose tissue as an endocrine organ.
78:1193, 1998.
of the molecular actions of vitamin D. Physiol Rev
Jones G, Strugnell SA, DeLuca HF: Current understanding
Physiol Rev 79:451, 1999.
Jequier E, Tappy L: Regulation of body weight in humans.
Rep 5:386, 2003.
demic on hypertension and renal disease. Curr Hypertens
Hall JE, Jones DW, Kuo JJ, et al: Impact of the obesity epi-
of obesity. Am J Hypertens 15:657, 2002.
Hall JE, Jones DW: What can we do about the “epidemic”
11:41, 2004.
cause of chronic kidney disease? Adv Ren Replace Ther
Hall JE, Henegar JR, Dwyer TM, et al: Is obesity a major
lar disease. J Clin Endocrinol Metab 89:2595, 2004.
Grundy SM: Obesity, metabolic syndrome, and cardiovascu-
weight in mammals. Nature 395:763, 1998.
Friedman JM, Halaas JL: Leptin and the regulation of body
uses of carotenoids. Prog Lipid Res 43:228, 2004.
Fraser PD, Bramley PM: The biosynthesis and nutritional
expanding epidemic. Cell 116:337, 2004.
Flier JS: Obesity wars: molecular progress confronts an
Nutr 22:258, 2003.
of atherosclerosis and carcinogenesis: a review. J Am Coll
Dutta A, Dutta SK: Vitamin E and its role in the prevention
satiety. Endocrinology 145:2660, 2004.
Druce MR, Small CJ, Bloom SR: Gut peptides regulating
286:R803, 2004.
or one? Am J Physiol Regul Integr Comp Physiol
Davy KP, Hall JE: Obesity and hypertension: two epidemics
sion 43:1312, 2004.
vascular, renal, and metabolic actions of leptin. Hyperten-
da Silva AA, Kuo JJ, Hall JE: Role of hypothalamic
Metabolism and Temperature Regulation
880
Unit XIII
melanocortin 3/4-receptors in mediating chronic cardio-
receptors and chronic regulation of arterial pressure and
National Institute of Diabetes and Digestive and Kidney
guidelines/index.htm.
2