Chapter 2
Gametogenesis:
conversion of germ cells
into male and female
gametes
Source of gametes
• Fertilization= Male gamete (Sperm) + female gamete (oocyte) zygote
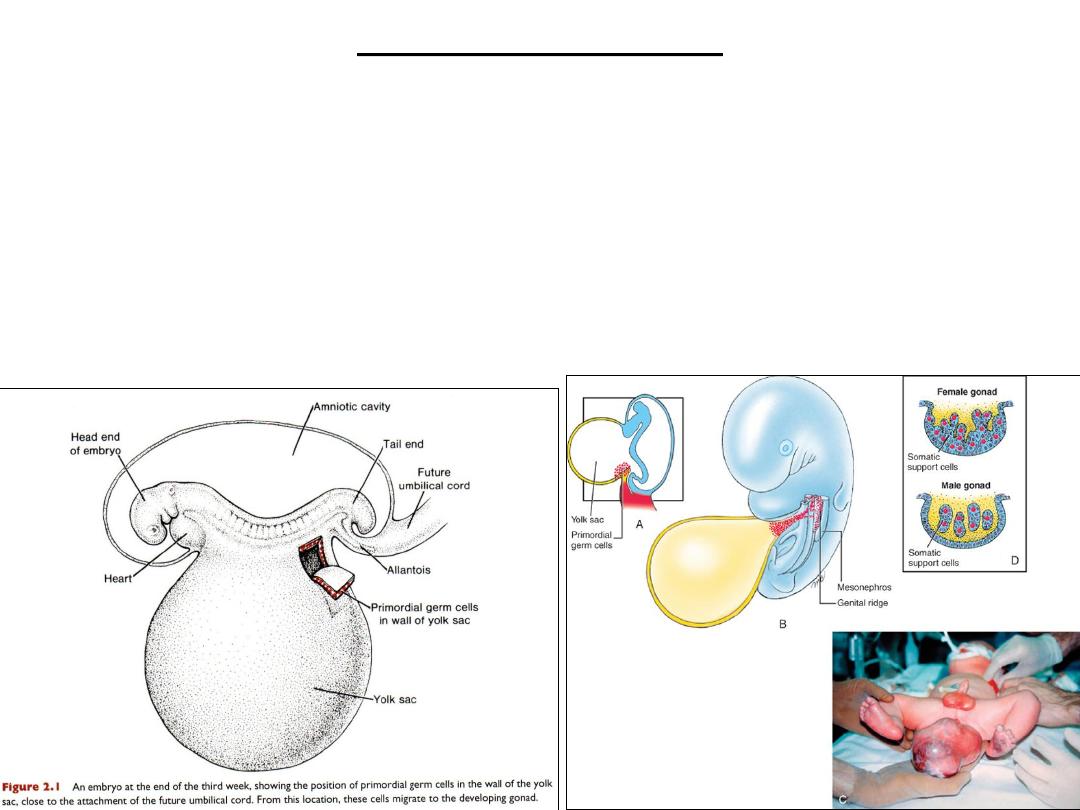
• Primordial Germ Cells (PGCs) are the source of GAMETES
Primordial germ cells
• Form in epiblast: 2
nd
wk
• Move to yolk sac
PGCs
Migrate to developing gonads: 4
th
wk
Reach gonads: end of 5
th
wk
PGCs mitosis = increase in number

PGCs
• PGCs = pluripotent cells
• PGC Gametogenesis = formation of Male & female gametes
• Gametogenesis = meiosis + cytodifferentiation
Clinical Correlates (CC)
PGCs and Teratomas
• Teratomas are tumors of disputed origin that often contain a variety of tissues,
such as bone, hair, muscle, gut epithelia, and others.
• It is thought that these tumors arise from pluripotent stem cells that can
differentiate into any of the three germ layers or their derivatives. Some evidence
suggests that PGCs that have strayed from their normal migratory paths could be
responsible for some of these tumors.
• Another source may be epiblast cells that give rise to all three germ layers during
gastrulation.
Oropharnyngeal teratoma.
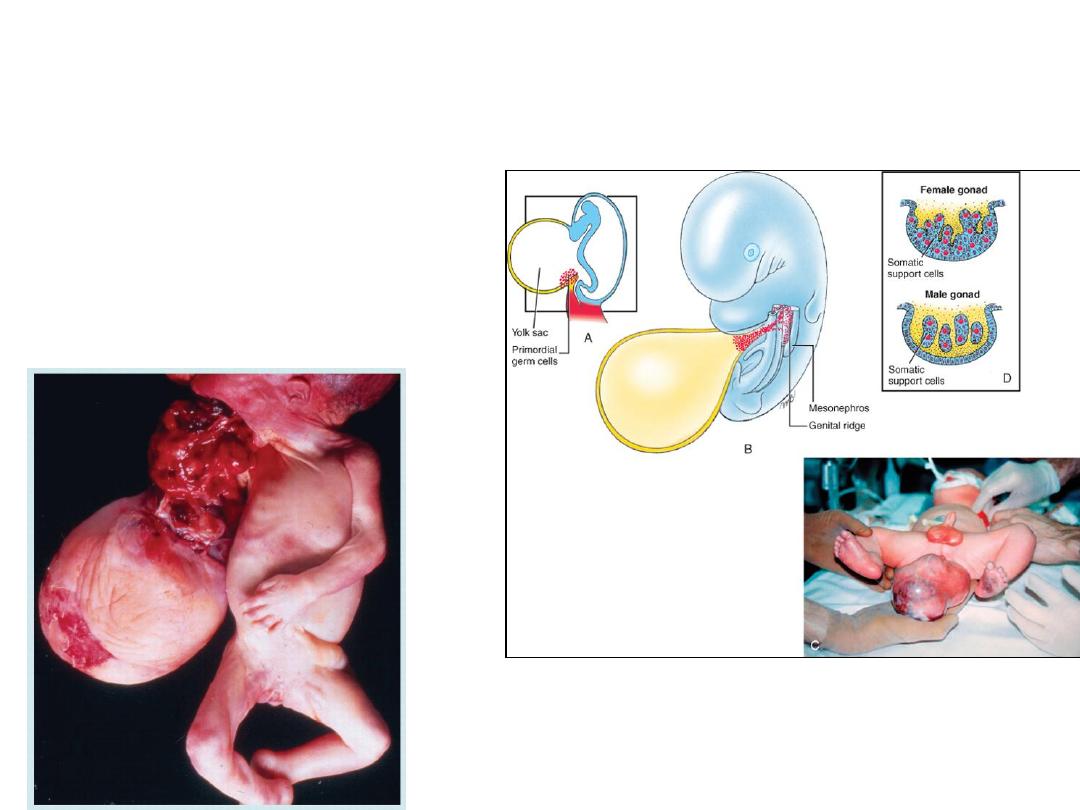
• These tumors may arise from
primordial germ cells or from
epiblast cells both of which are
pluripotent.
• Tissues within the tumors include
derivatives of all three germ layers
and may include gut, bone, skin,
teeth, etc.
Sacrococcygeal teratoma
THE CHROMOSOME THEORY OF INHERITANCE
• Traits = genes (maternal + paternal)
• 23000 genes on 46 chromosomes
• Genes on same chm. : LINKED GENES, inherited together
• Somatic cells: (DIPLOID NUMBER OF CHMS.)
– 23 pairs of homologous chms
• (23 maternal chms + 23 paternal chms)
– 22 (pairs) autosomes +1(pair) sex chms
»
XX: genetically female
»
XY: genetically male
• Gametes: (HAPLOID NUMBER)= 23 chms.
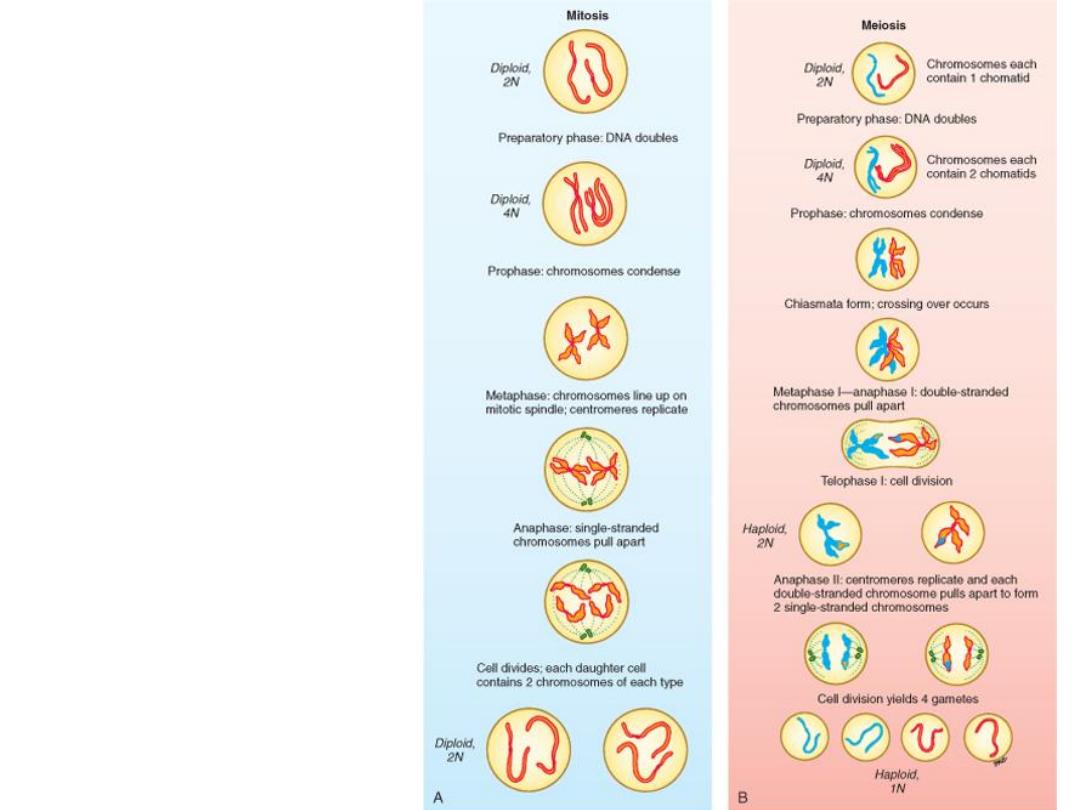
Mitosis vs
meiosis
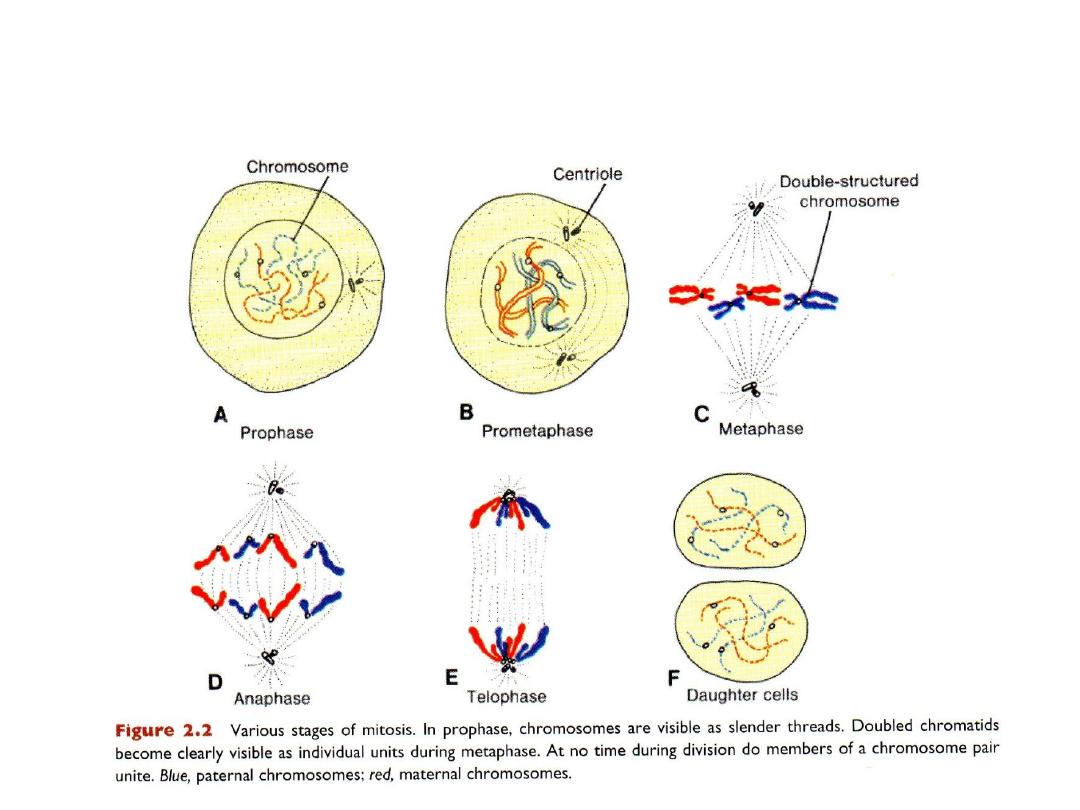
MITOSIS
one cell 2 daughter cells
daughter cells are genetically identical to parent cell
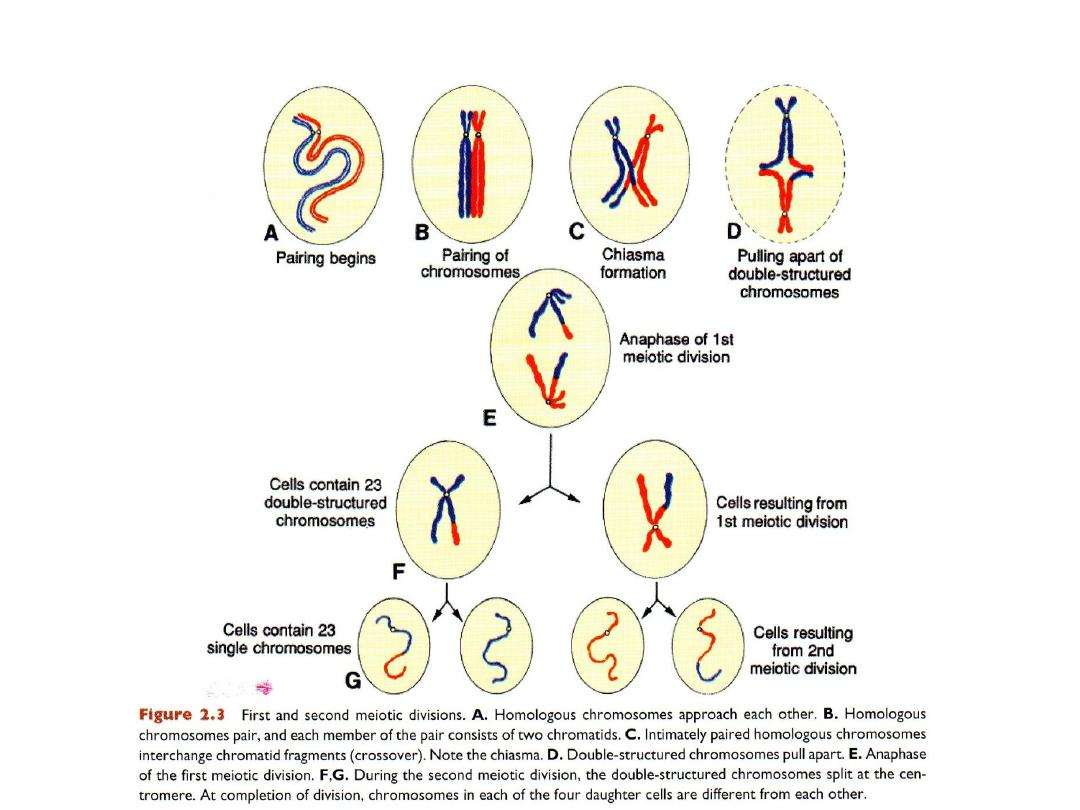
MEIOSIS: in germ cells, to produce gametes
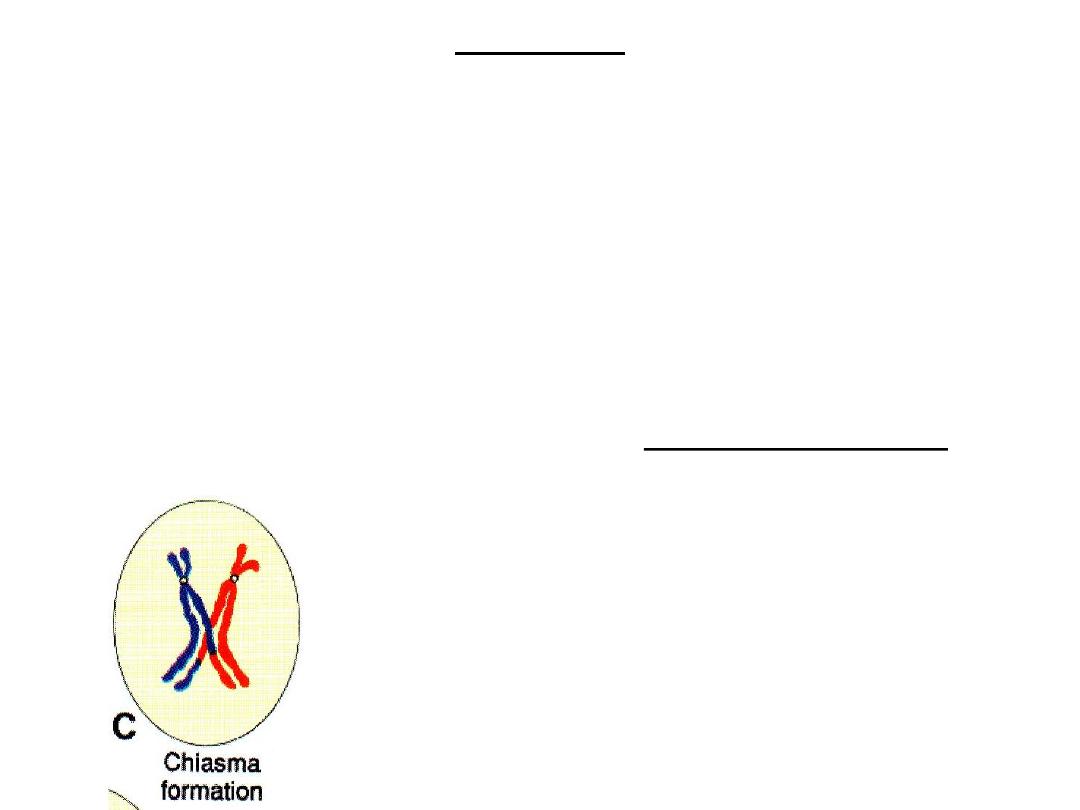
Crossover
• Crossovers, critical events in meiosis I, are
the interchange of chromatid segments
between paired homologous chromosomes
.
• Segments of chromatids break and are exchanged
• As separation occurs, points of interchange are temporarily united and form an X-
like structure, a (
chiasma
).
• Approximately
30 to 40 crossovers
with each meiotic I division (1 or 2 per chromo.)
• Most frequent between genes that are far apart on a chromosome.
CROSSOVER
Interchange of chromatid segments
30-40 crossovers/division
Results of meiosis
• Genetic variability
is enhanced through
– crossover
, which redistributes genetic
material
– random distribution
of homologous
chromosomes to the daughter cells
• Each germ cell contains a haploid number
of chromosomes, so that at fertilization the
diploid number of 46 is restored.
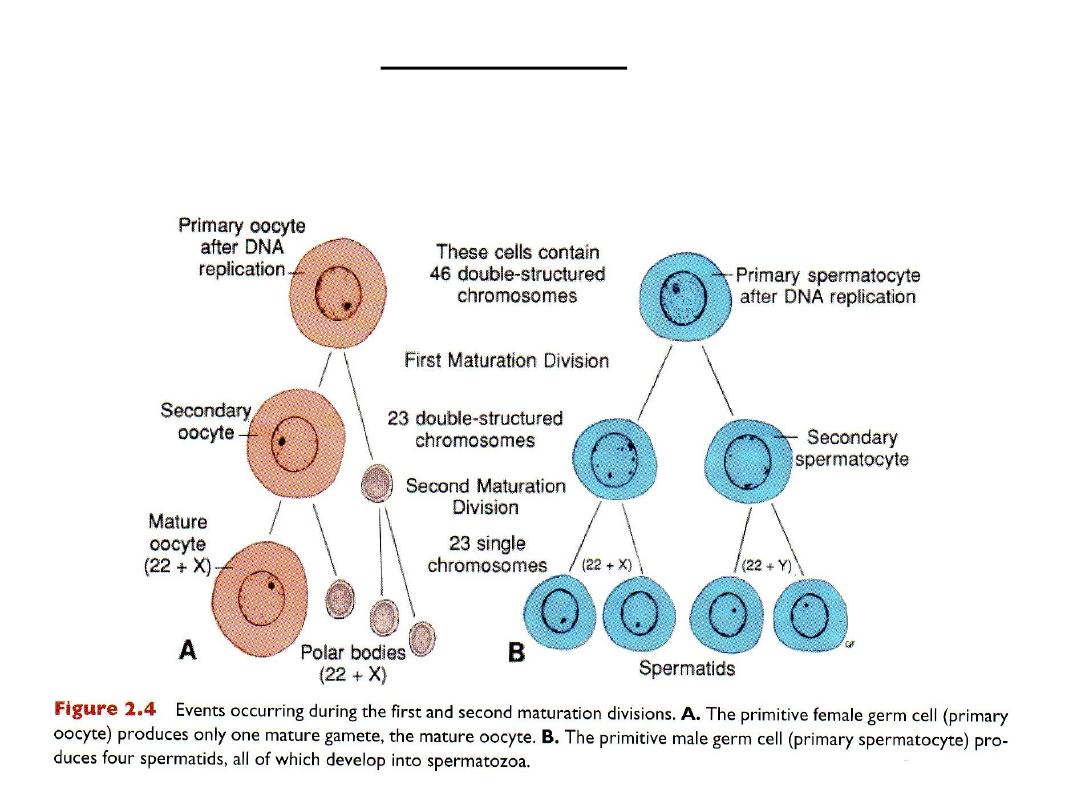
Polar bodies
Clinical correlates (CC)
BIRTH DEFECTS & SPONTANEOUS ABORTIONS:
CHROMOSOMAL & GENETIC FACTORS
• Chromosomal abnormalities:
– Numerical
– Structural
• Gene mutations
Numerical abnormalities
• Diploid (2n) 46 chromosomes: normal human somatic cells
• Haploid (n) 23 chromosomes: normal gamete
• Euploid (diploid, triploid): any exact multiple of n
• Aneuploid: any chm No. not euploid
– Trisomy: extra chm
– Monosomy: missing chm
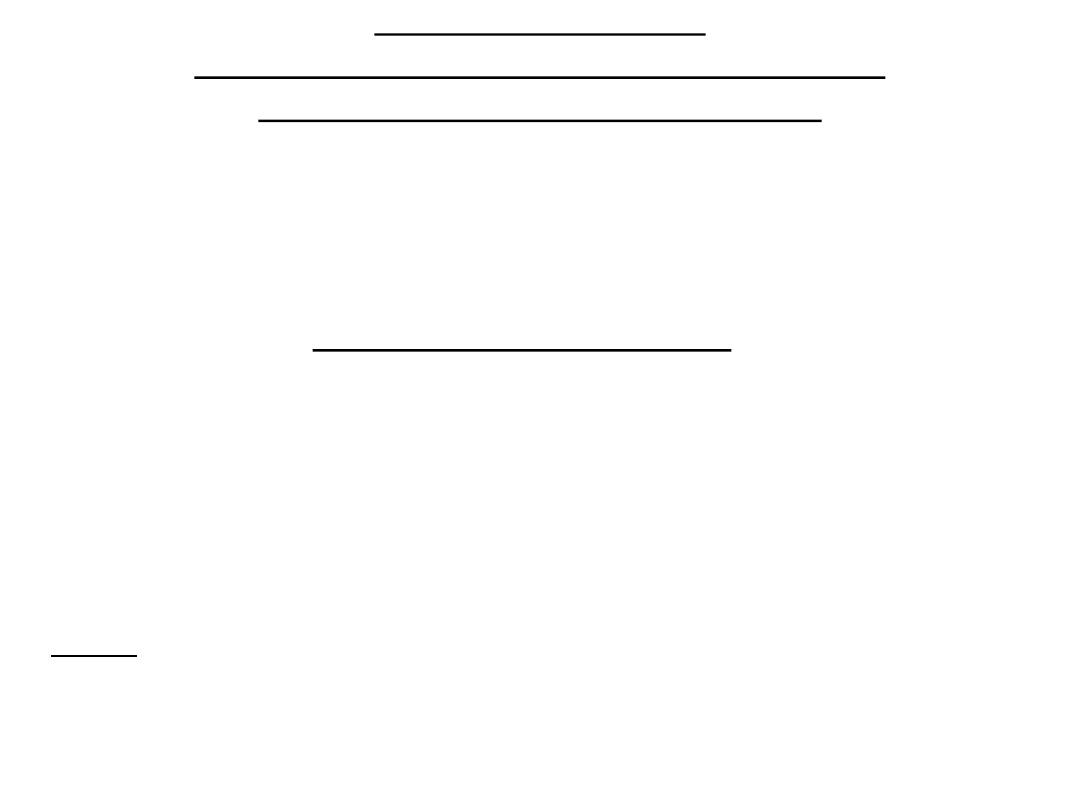
• Causes
Nondisjunction-meiosis
Nondisjunction-mitosis:mosaicism
Translocations
Nondisjunction
in meiosis
Mitotic nondisjunction
MOSAICISM
• During early cell division of the embryo:
EMBRYONIC CELL Normal cells + Cells with abnormal chm No. =
MOSAICISM
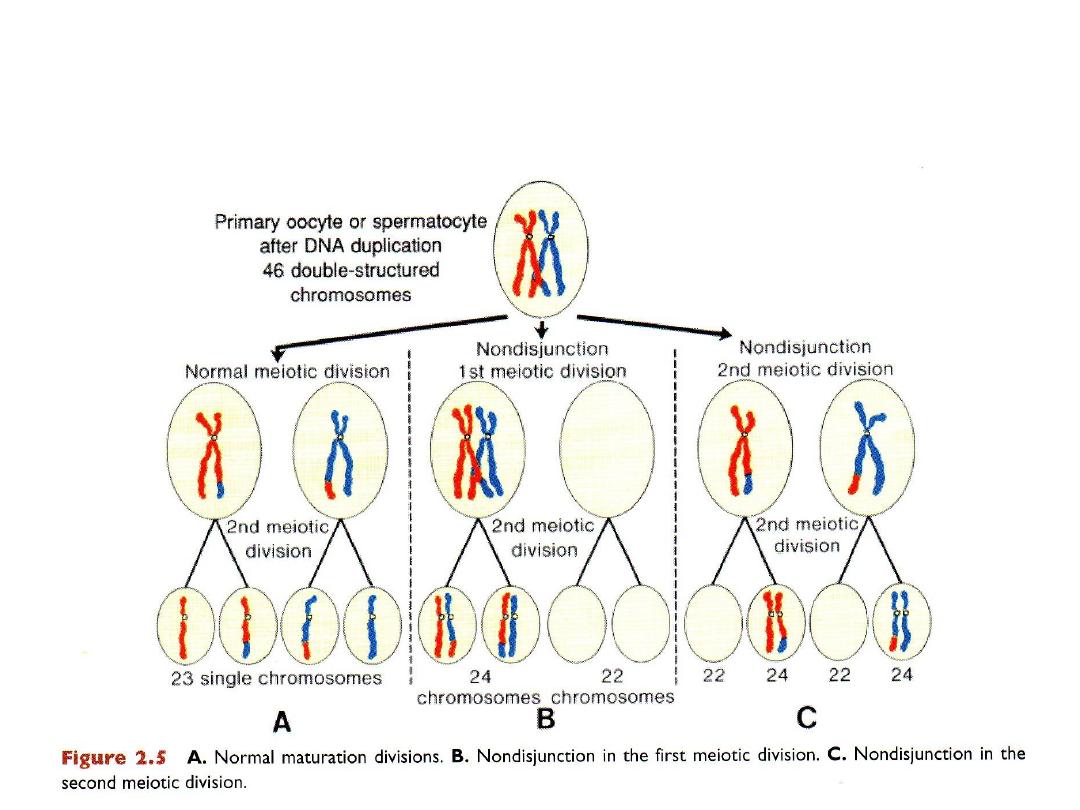
Translocations
• Breakage & reunion of
chromosomes pieces
• Balanced = no genetic material
is lost normal individual
• Unbalanced = lost genetic
material abnormal
individual e.g.: Down syndrome
(extra copy of Ch 21)
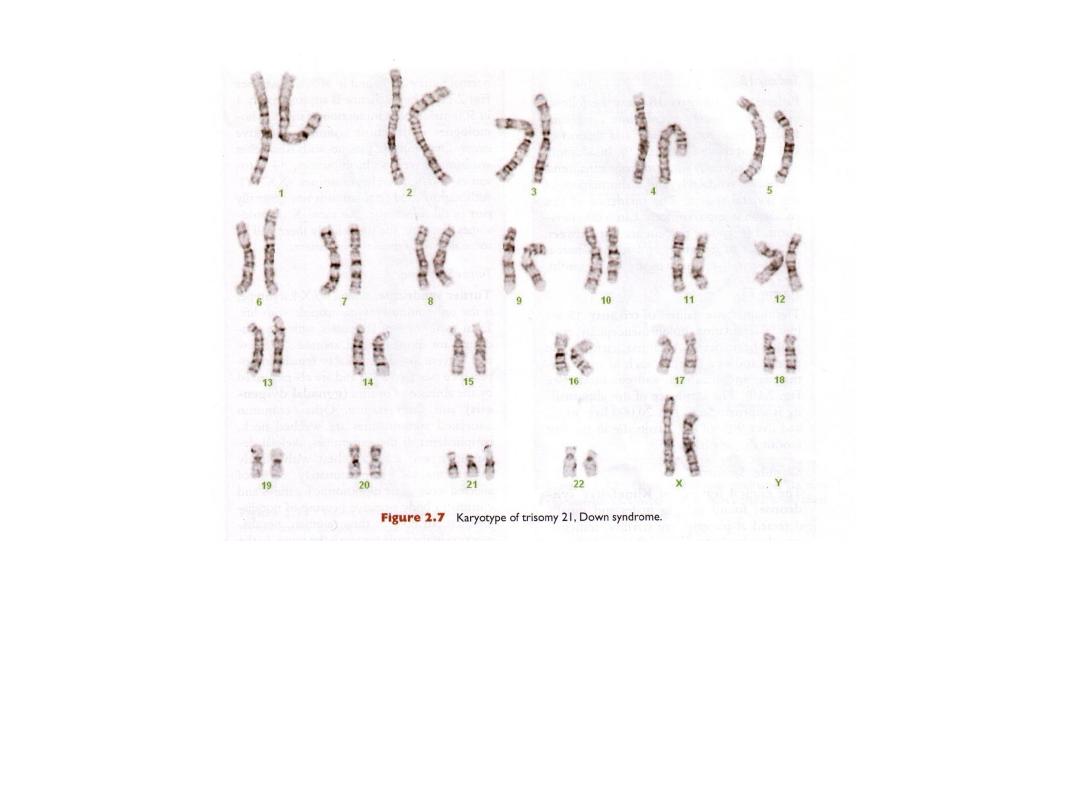
DOWN SYNDROME, TRISOMY 21
•meiotic nondisjunction
•unbalanced translocation
•mosaicism
TRISOMY21 (DOWN SYNDROME)
• Is caused by an extra copy of chromosome 21(trisomy 21)
• Features of children with Down syndrome include growth retardation; varying
degrees of mental retardation; craniofacial abnormalities, including upward
slanting eyes, epicanthal folds (extra skin folds at the medial corners of the eyes),
flat facies, and small ears; cardiac defects; and hypotonia. These individuals also
have relatively high incidences of leukemia, infections, thyroid dysfunction, and
premature aging. Furthermore, nearly all develop signs of Alzheimer’sdisease after
age 35.
• In 95% of cases: the syndrome is caused by trisomy 21 resulting from
meiotic
nondisjunction, during oocyte formation.
• The risk
increases with maternal age at age 35 & at age 40.
• In 4% of cases: there is an unbalanced translocation between chromosome 21 and
chromosome 13, 14, or 15.
• In 1% of cases: the cause is
mosaicism resulting from mitotic nondisjunction.
These individuals have some cells with a normal chromosome number and some
that are aneuploid. They may exhibit few or many of the characteristics of Down
syndrome.

A. Child with Down syndrome. Note the flat
broad face, oblique palpebral fissures, and
protruding tongue. Children with Down
syndrome usually have some degree of
mental retardation and many have cardiac
defects.
B .Another characteristic of
these children is a broad hand
with a single transverse (simian)
crease.
KLINFELTER SYNDROME
47,XXY, 48,XXXY
• Sex chromatin body (Barr body)
• Only in males
• Detected at puberty
• Sterility
• Testicular atrophy
• Gynecomastia
• Causes: meiosis nondisjunction
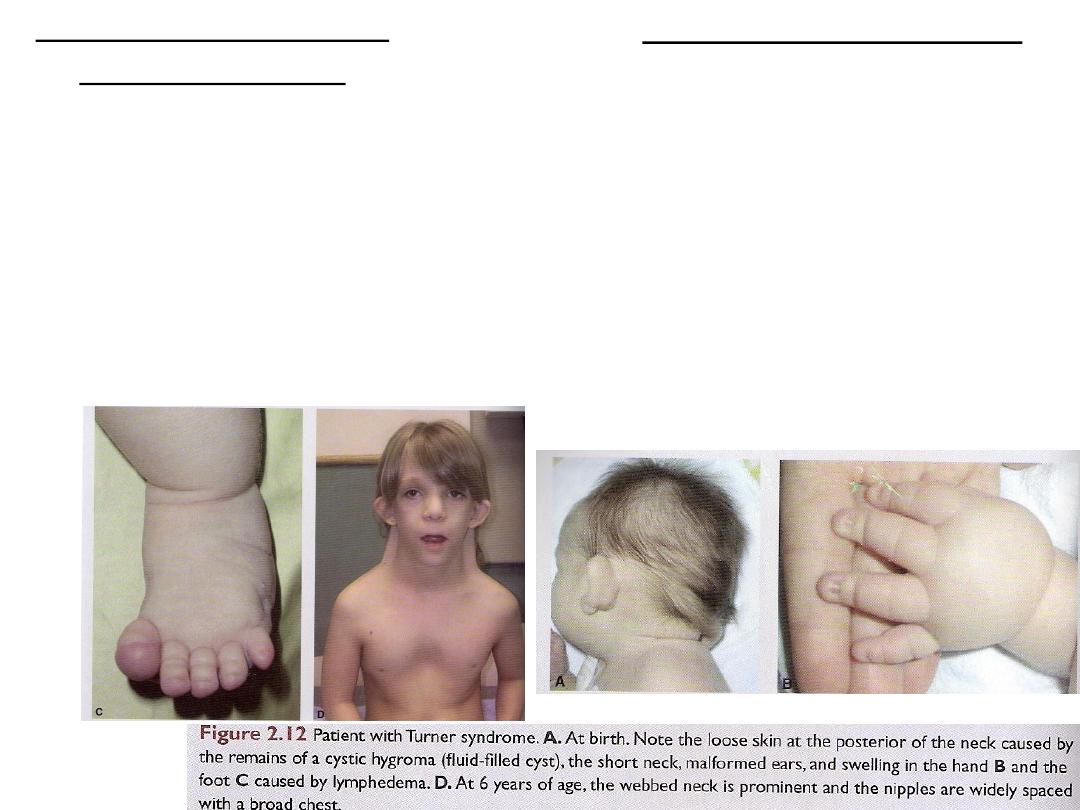
TURNER SYNDROME 45,X
• The only monosomy compatible with life
• Females
• Barr body negative
• Gonadal dysgenesis: (absence of ovaries)
• Short stature
• Causes:
– NDJ in male gamete
– structural abnormalities of X chm
– mosaicism
Structural abnormalities
• Chromosomal breakage: environmental factors, viruses, radiation & drugs
• Deletion: Cri-du-chat syndrome: partial deletion of short arm of chr. 5
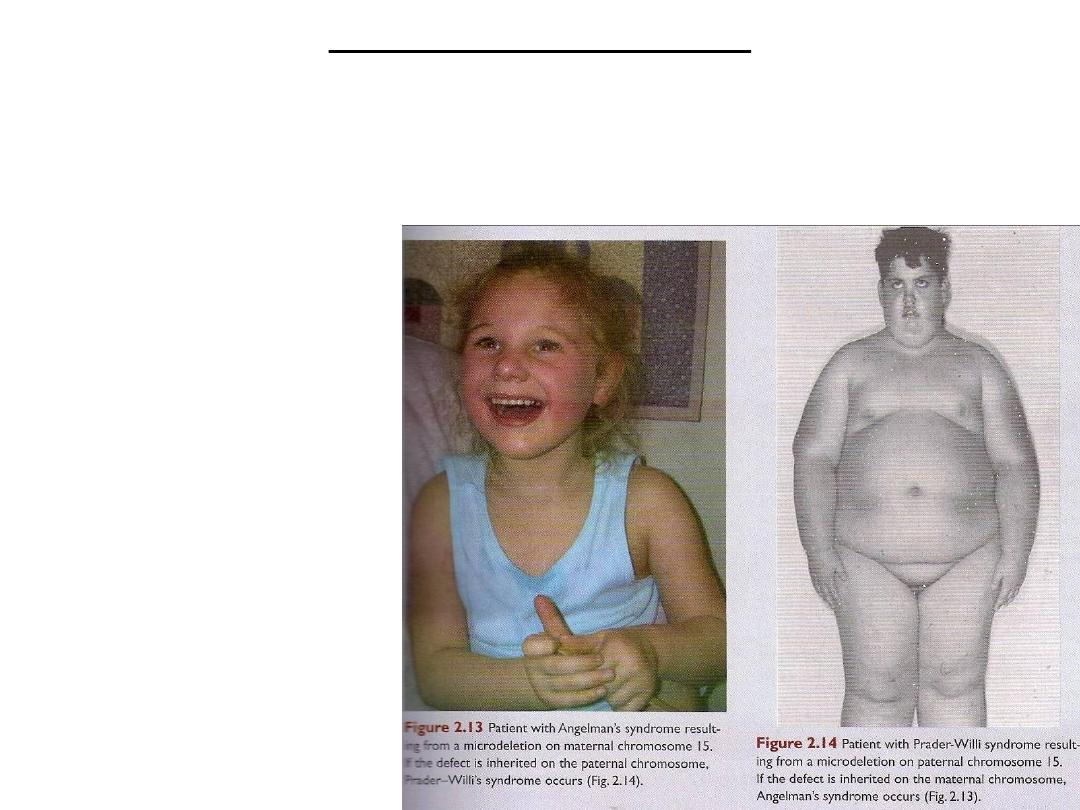
• Microdeletions: contiguous gene syndrome:
Angelman syndrome
& Prader-willi
syndrome
Long arm of chr. 15
Angelman syndrome:
maternal chr.
Prader-willi syndrome:
paternal chr.
Genomic imprinting
Gene mutations
• Gene mutations cause:
• 1- Congenital malformations:
– Inherited: Mendelian pattern of inheritance
– Single gene mutation: change in structure or function of a single gene
• Genes exist as pairs: Alleles (there are two doses for each genetic determinant)
• One from the mother and one from the father
• Dominant mutation: when a mutant gene produces an abnormality in a single
dose
• Recessive mutation: both alleles must be abnormal (double dose), or if the
mutation is X-linked in the male
2- Inborn errors of metabolism:
– Phenylketoneuria
– Homocystinuria
– Galactosemia
– Cause intellectual disabilities if proper diets and medical care are not given.

Diagnostic techniques for identifying genetic abnormalities
• Cytogenic analysis: assess chrm No. & integrity
– Arrest mitosis at metaphase
– Giemsa stain
– G-bands (No. of genes)
– High-resolution metaphase banding techniques
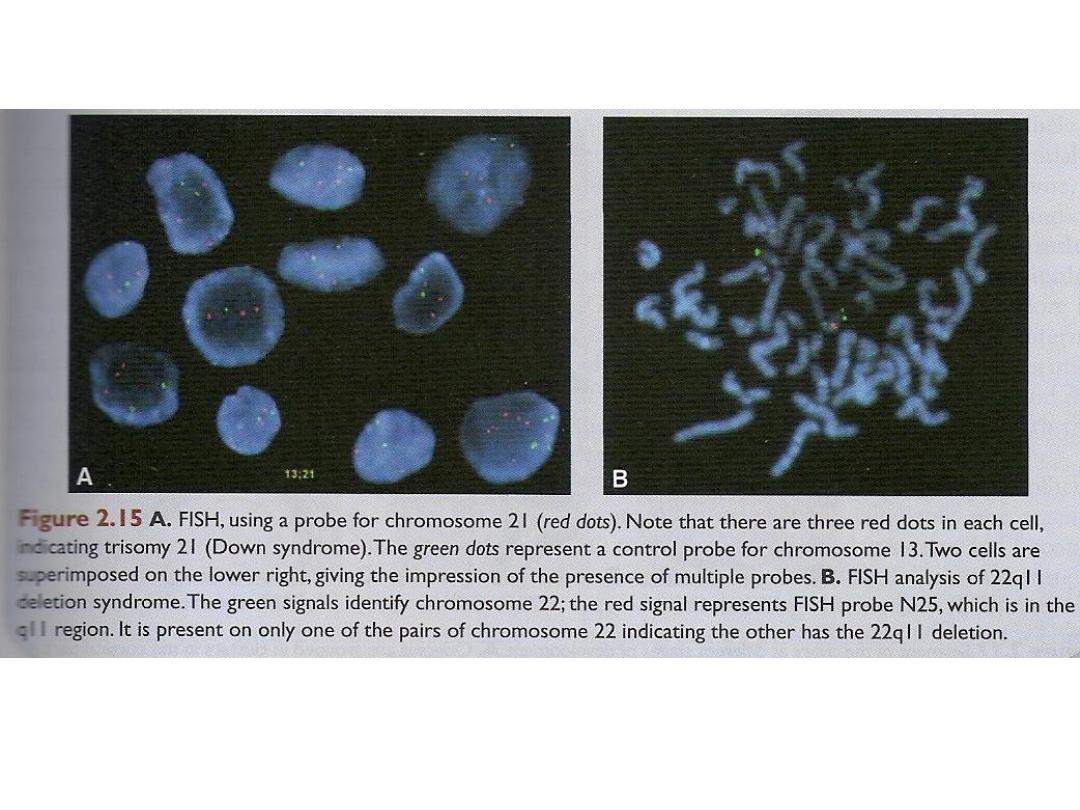
Fluoroscence in situ hybridization (FISH)
• FISH use specific DNA probes to identify ploidy for a few selected
chromosomes and for detecting microdeletions.
• Fluorescent probes are hybridized to chromosomes or genetic loci using cells
on a slide, and the results are visualized with a fluorescence microscope.
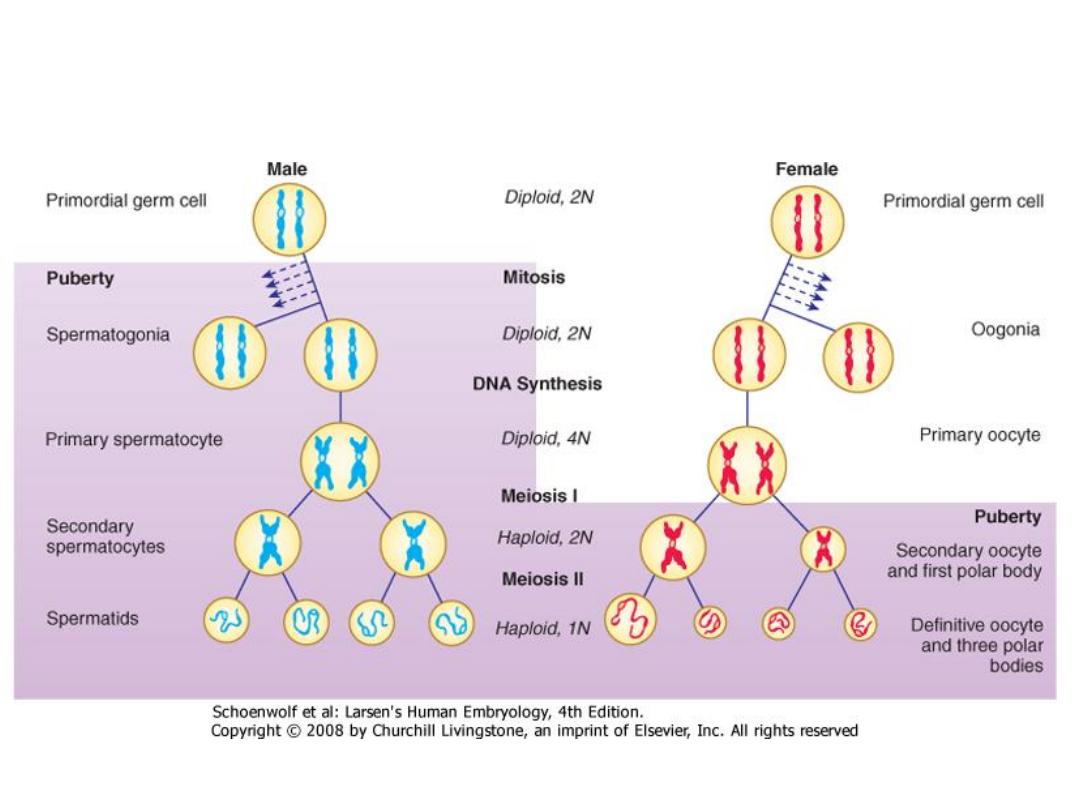
Gametogenesis
Oogenesis
Maturation of female gametes (oocyte)
Begins during intrauterine life
Stops
Continues at puberty
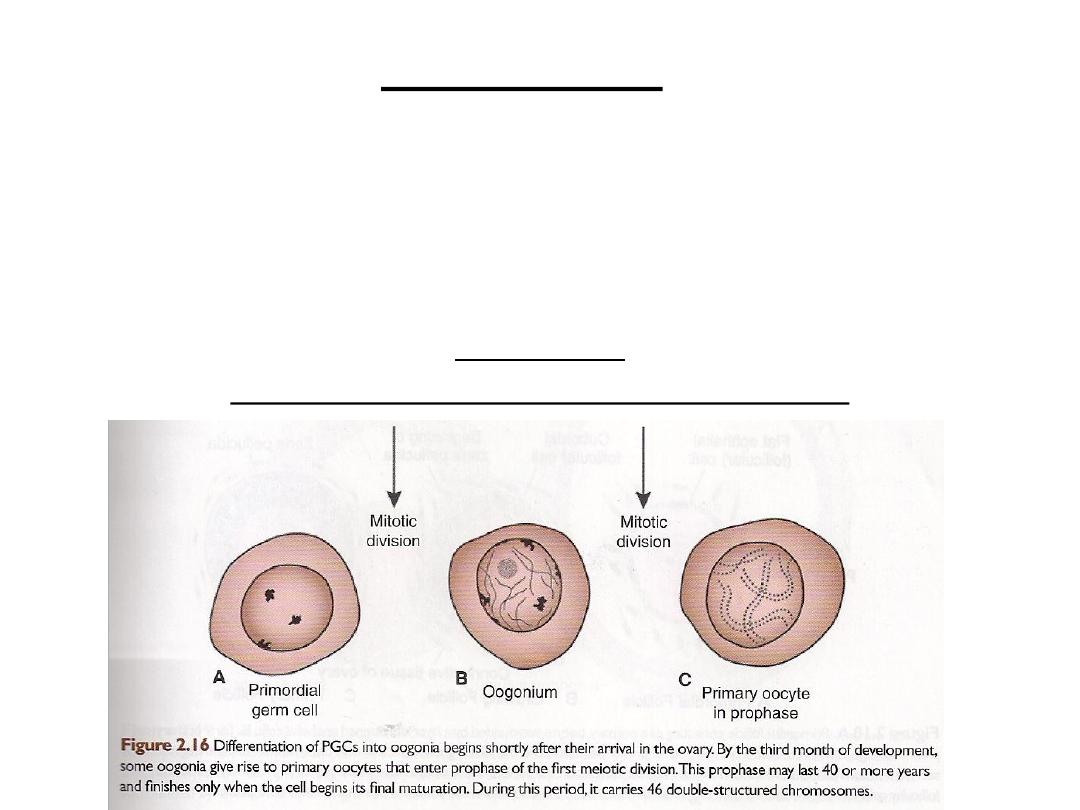
OOGENESIS
Maturation of oocytes begins before birth
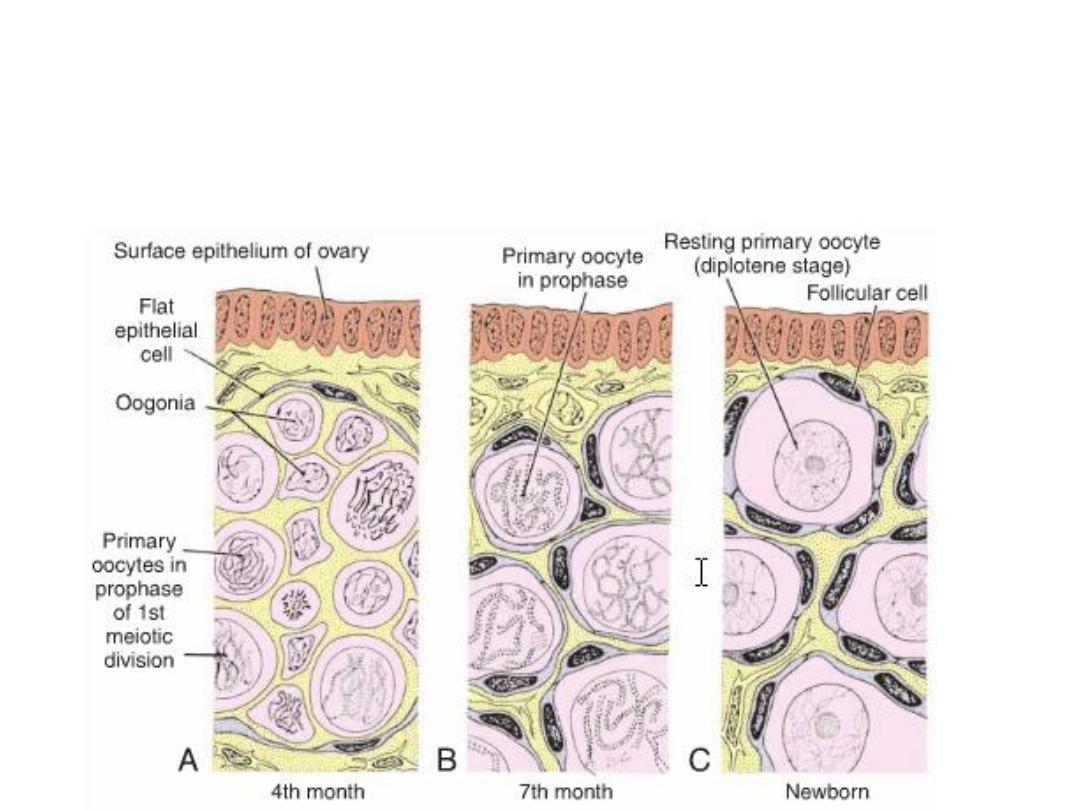
OOGENESIS
Maturation of oocytes begins before birth
Maturation of oocytes continues after puberty
Maturation of oocytes continues after puberty
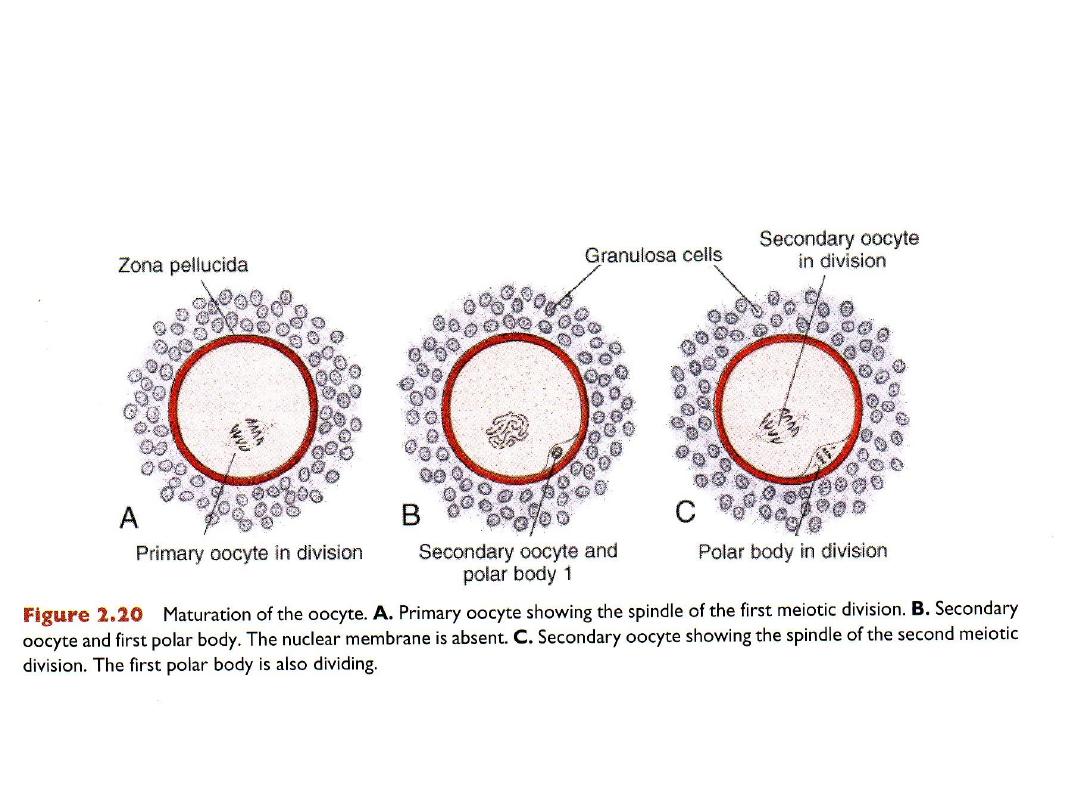
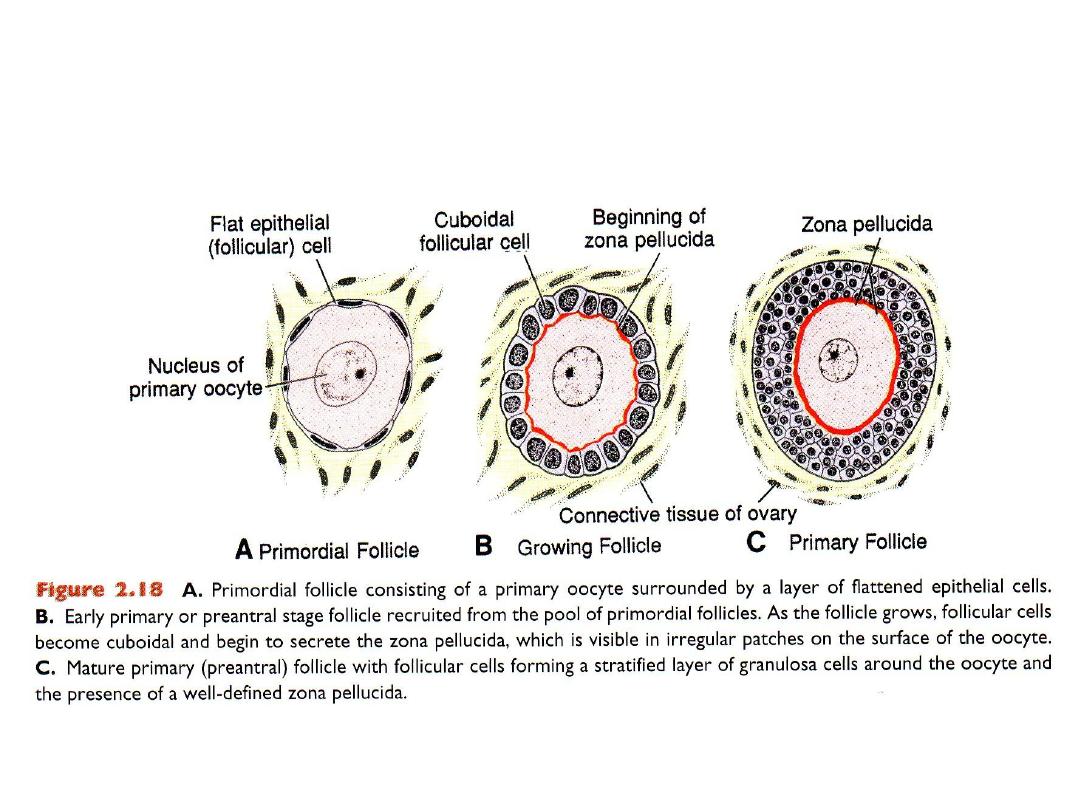
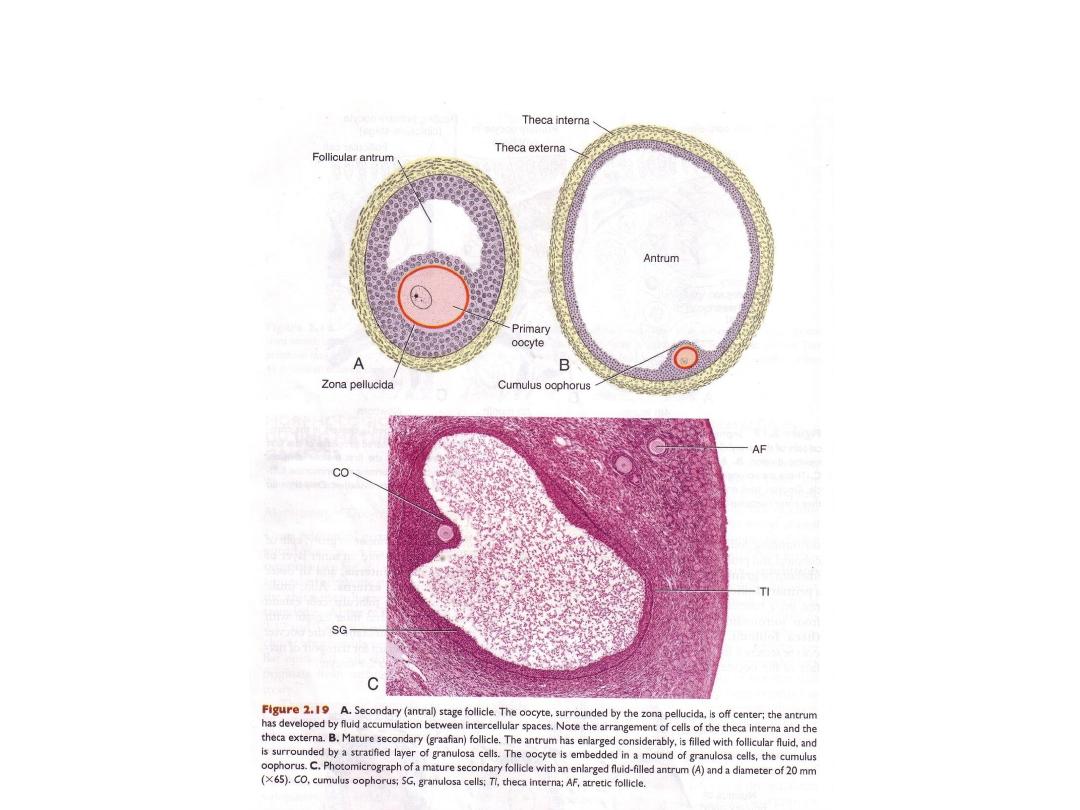
Maturation of the oocyte
SPERMATOGENESIS
Maturation of male gametes (sperm)
Begins after puberty
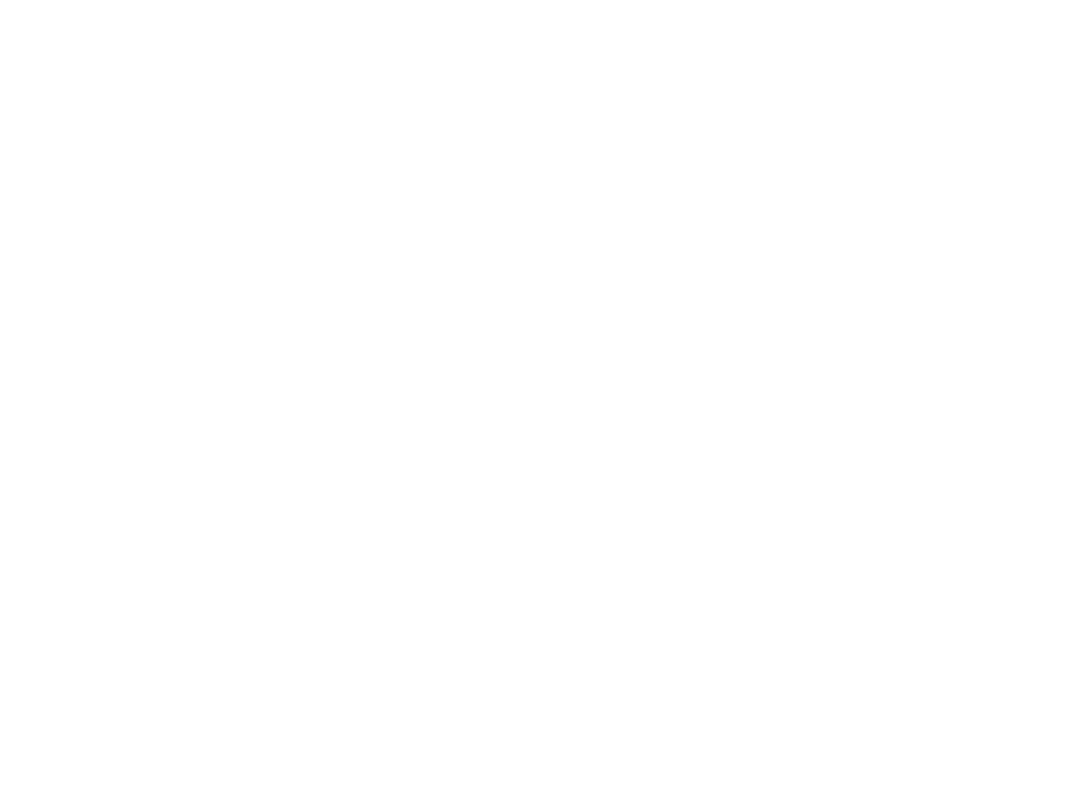
Testis
A. Cross section through primitive sex
cords of a newborn boy showing
primordial germ cells and supporting cells.
B. Cross section through a seminiferous
tubule at puberty. Note the different
stages of spermatogenesis and that
developing sperm cells are embedded in
the cytoplasmic processes of a Sertoli cell.
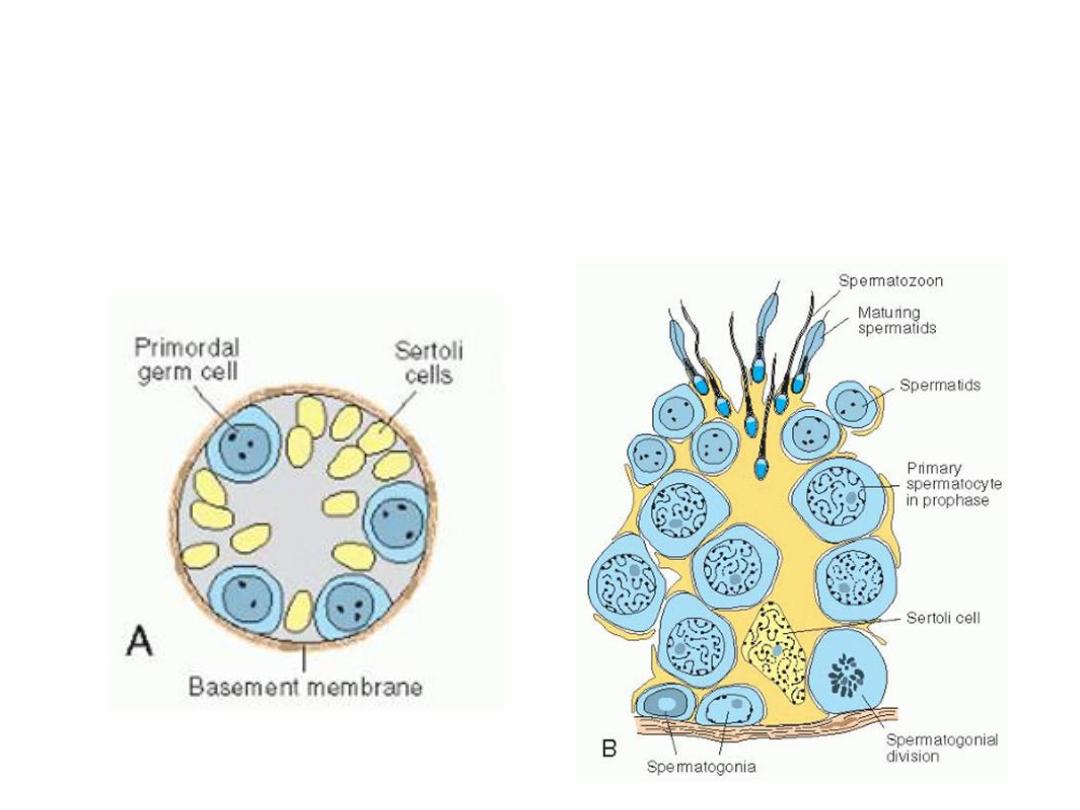
• Spermatogenesis
&
Spermeiogenesis
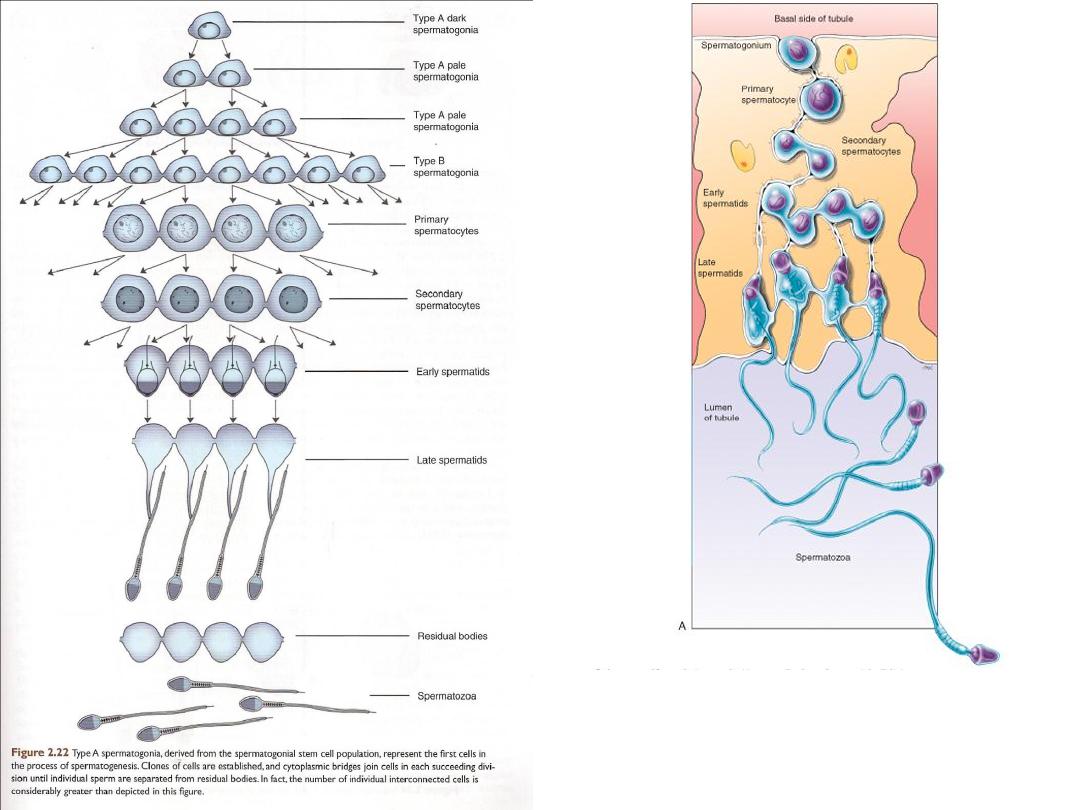
The products of meiosis
SPERMIOGENESIS
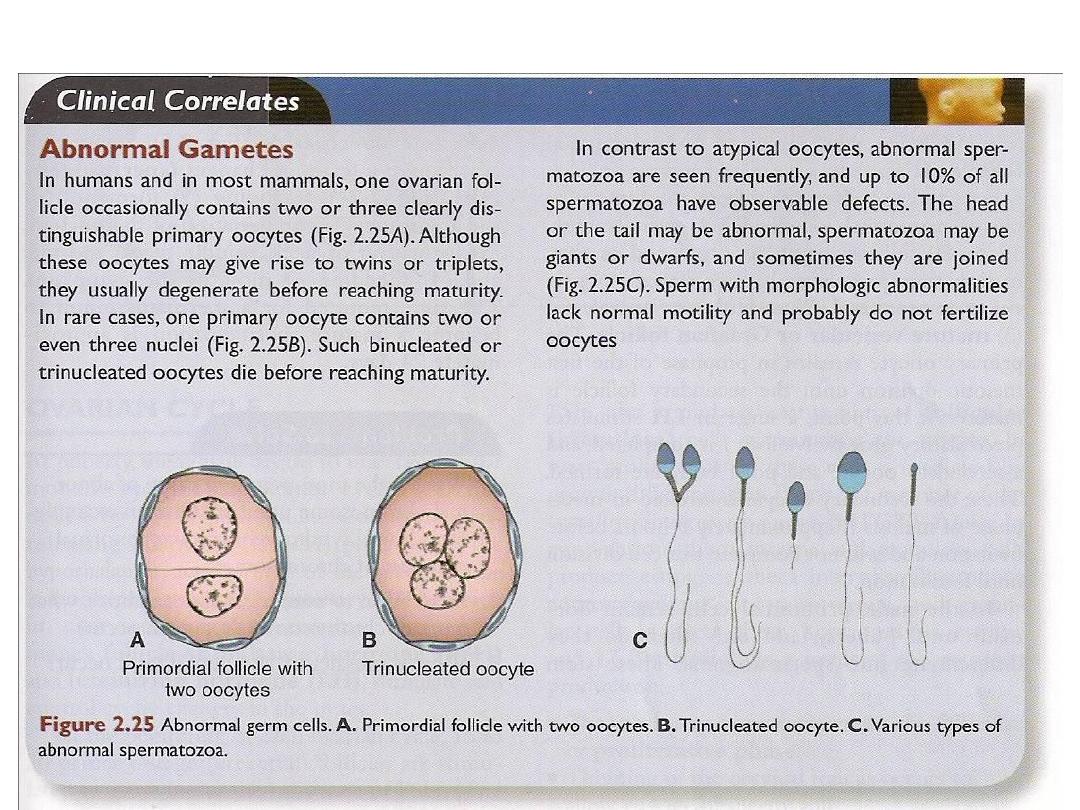
ABNORMAL GAMETES