358
CHAPTER 9
and are described in detail in Chapter 12.
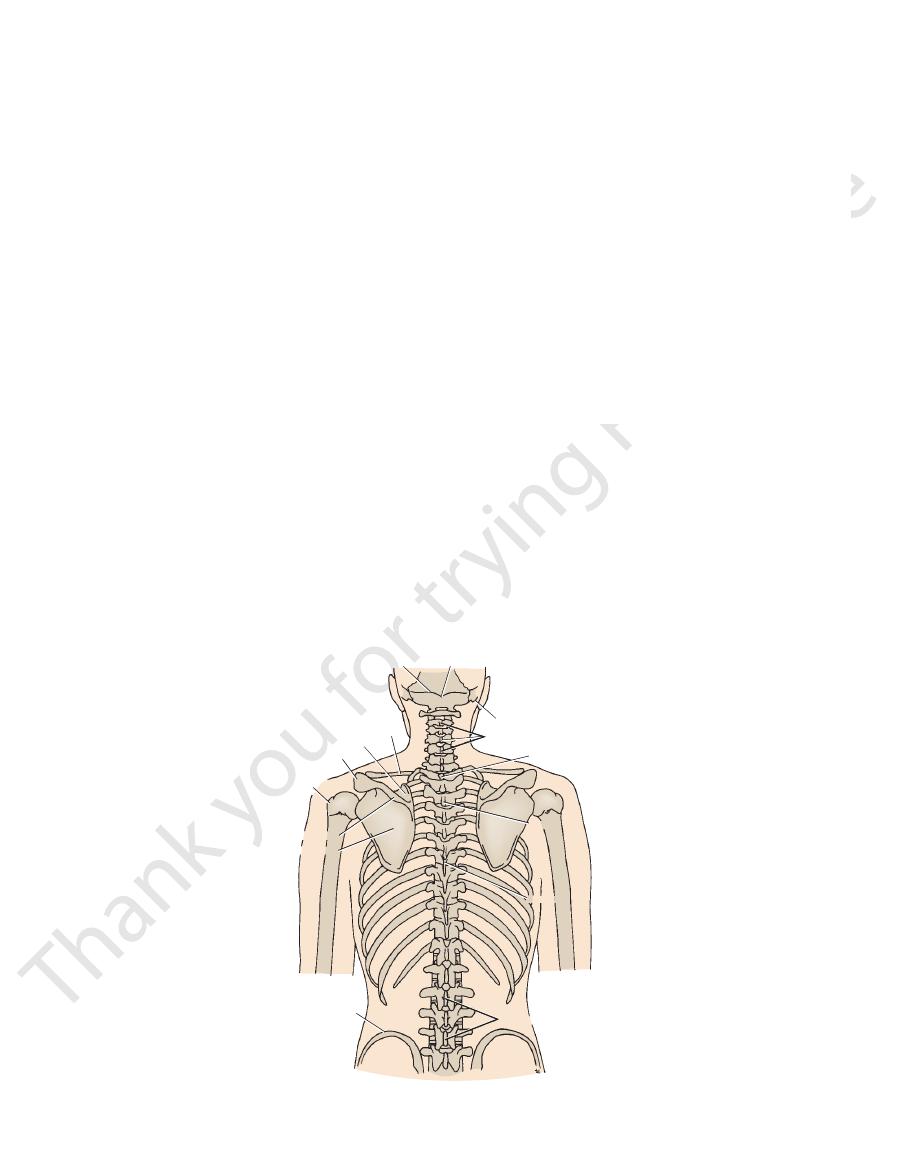
The underlying bones of the back are shown in Figure 9.27
axillary lymph nodes.
level of the iliac crests is upward into the posterior group of
of the skin of the back above the
lymph drainage
The
into the azygos veins and the inferior vena cava.
bar arteries. The veins correspond to the arteries and drain
branches of the posterior intercostal arteries and the lum
to the skin is from the posterior
blood supply
The
buttock.
bar nerves run downward to supply the skin over the
the skin, and the posterior rami of the upper three lum
1.24). The 1st and 8th cervical nerves do not supply
from the posterior rami of the spinal nerves (see Fig.
to the skin of the back is
sensory nerve supply
The
The Upper Limb
The Superficial Part of the Back and
the Scapular Region
Skin
-
-
Bones of the Back
Examination of the Axillary Lymph Nodes
The examination of the axillary lymph nodes always forms part of
examining hand high up in the axilla to the outer border of the
The examiner then gently places the tips of the fingers of the
der muscles and let the upper limb hang down at the side.
may be palpated against the medial side of
lateral nodes
forward against the posterior surface of the pectoralis major
With the patient standing or sitting, he or she is asked to place
the hand of the side to be examined on the hip and push hard
medially. This action of adduction of the shoulder joint causes
the pectoralis major muscle to contract maximally so that it
becomes hard like a board. The examiner then palpates the axil-
lary nodes (Fig. 9.26) as follows:
■
■
The anterior (pectoral) nodes may be palpated by pressing
muscle on the anterior wall of the axilla.
■
■
The posterior (subscapular) nodes may be palpated by
pressing backward against the anterior surface of the sub-
scapularis muscle on the posterior wall of the axilla.
■
■
The
the axillary vein. The examiner’s fingers are pressed laterally
against the subclavian vein and the pulsating axillary artery.
■
■
The central nodes may be palpated in the center of the ax-
illa between the pectoralis major (anterior wall) and the sub-
scapularis (posterior wall).
■
■
For the apical nodes, the patient is asked to relax the shoul-
first rib. If the nodes are enlarged, they can be felt.
the clinical examination of the breast.
C L I N I C A L N O T E S
superior nuchal line external occipital protuberance
mastoid process
spines of cervical vertebrae
first thoracic spine
spines of lumbar vertebrae
iliac crest
infraspinous fossa
spine of scapula
greater
tuberosity
acromion
clavicle
supraspinous fossa
seventh
third
FIGURE 9.27
Bones of the back.
Basic Anatomy
the thoracic wall and the vertebral column are shown in
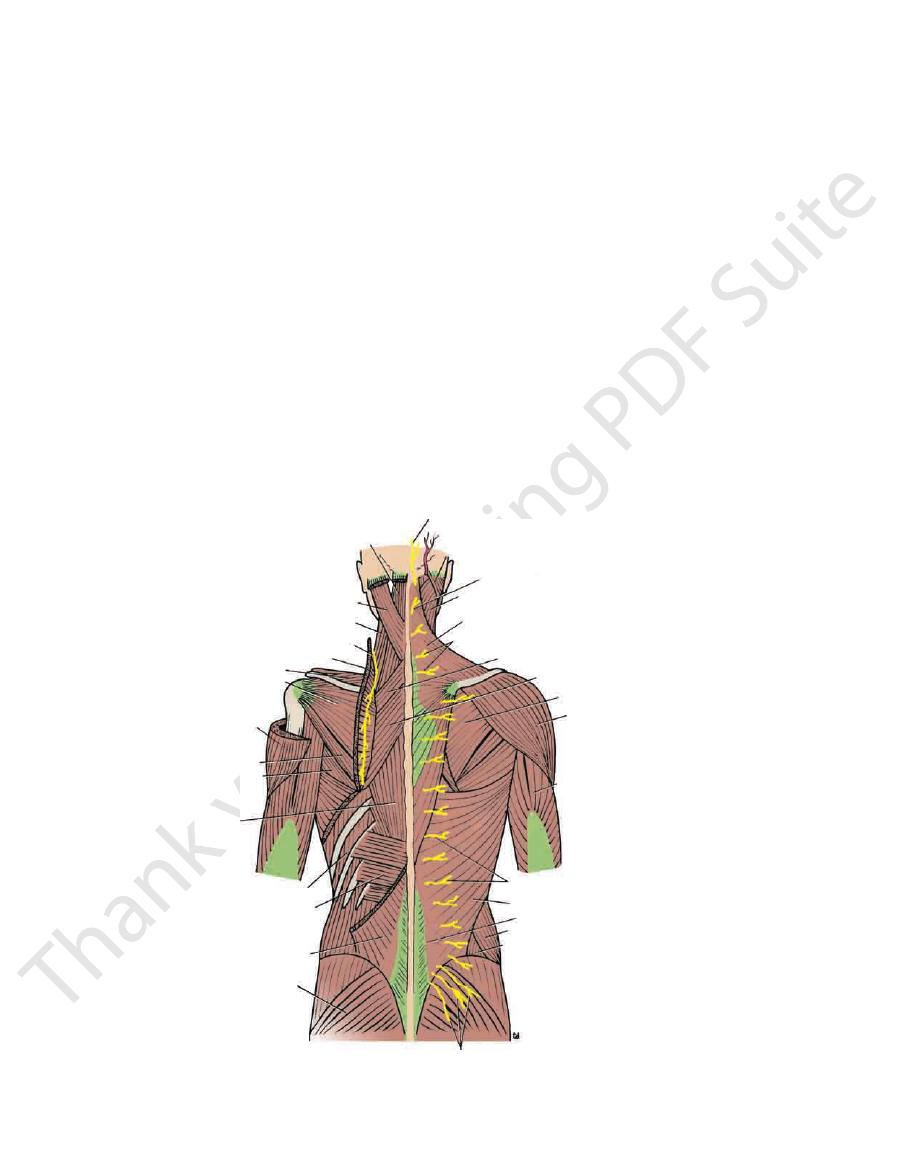
The muscles on the back connecting the upper limb to
359
Muscles
Figure 9.28 and are described in Tables 9.1 and 9.2, and the
with the cervical nerves, supplies the trapezius muscle.
at the junction of its middle and lower thirds and, together
beneath the anterior border of the trapezius muscle (Fig. 9.28)
third and fourth cervical nerves. The accessory nerve runs
It is accompanied by branches from the anterior rami of the
posterior triangle of the neck on the levator scapulae muscle.
The spinal part of the accessory nerve runs downward in the
Nerve XI)
Spinal Part of the Accessory Nerve (Cranial
vessels pass backward through this space (Fig. 9.29).
The axillary nerve and the posterior circumflex humeral
neck of the humerus.
by the long head of the triceps and laterally by the surgical
below by the teres major muscle. It is bounded medially
by the subscapularis and capsule of the shoulder joint and
immediately below the shoulder joint. It is bounded above
The quadrangular space is an intermuscular space, located
Quadrangular Space
weakness.
cuff is deficient inferiorly, and this is a site of potential
anterior, superior, and posterior aspects of the joint. The
movements at the shoulder joint. The cuff lies on the
the humerus in the glenoid cavity of the scapula during
The tone of these muscles assists in holding the head of
very important role in stabilizing the shoulder joint.
sule of the shoulder joint (Fig. 9.34). The cuff plays a
minor muscles, which are fused to the underlying cap
subscapularis, supraspinatus, infraspinatus, and teres
The rotator cuff is the name given to the tendons of the
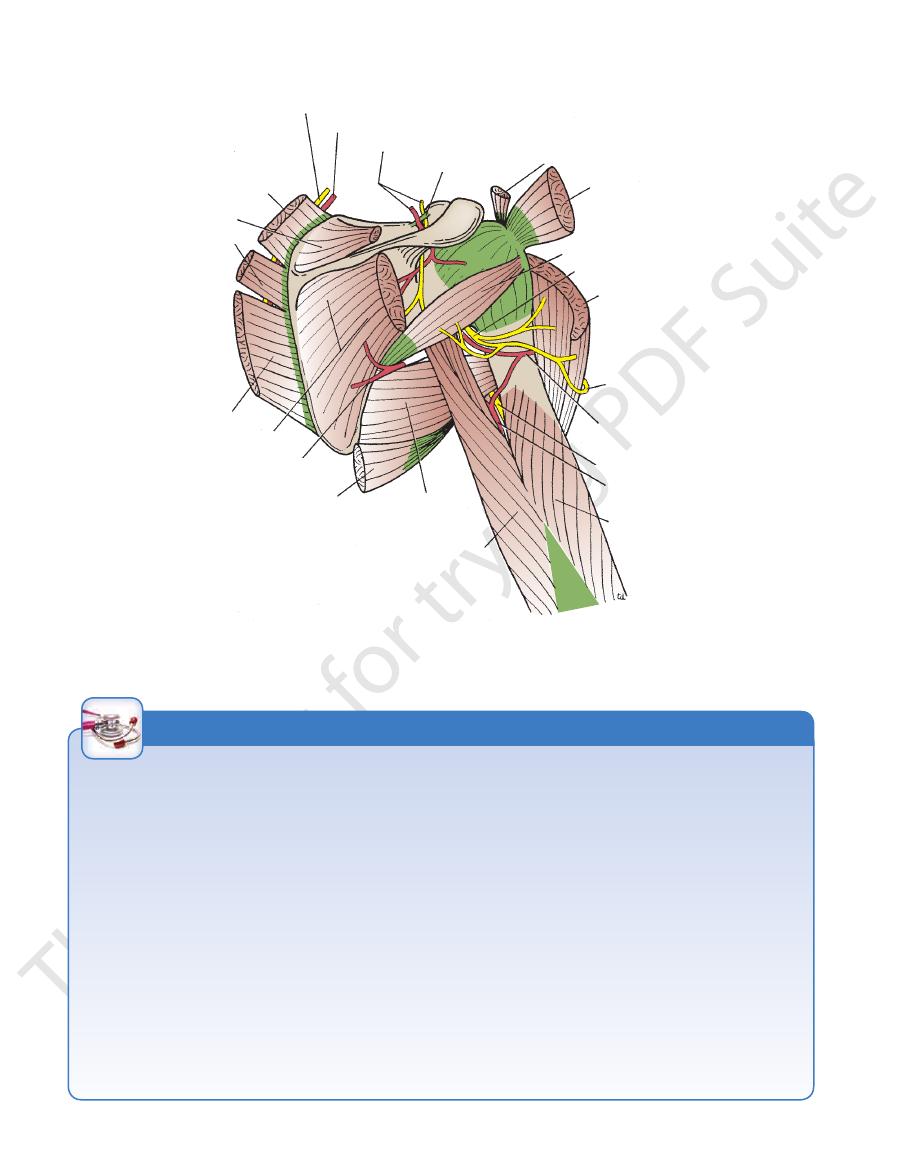
in Figure 9.29 and are described in Table 9.3.
muscles connecting the scapula to the humerus are shown
Rotator Cuff
-
Nerves
semispinalis capitis
splenius capitis
levator scapulae
spinal part of accessory nerve
supraspinatus
infraspinatus
deltoid
teres minor
teres major
postvertebral muscles
external intercostal
serratus posterior inferior
latissimus dorsi
gluteus maximus
cutaneous branches of posterior rami
of upper three lumbar nerves
internal oblique of abdomen
external oblique of abdomen
lumbar fascia
latissimus dorsi
cutaneous branches of posterior rami of thoracic nerves
lateral and long heads
of triceps
deltoid
infraspinatus
rhomboid major
rhomboid minor
posterior rami of cervical nerves
trapezius
splenius capitis
third occipital nerve
sternocleidomastoid
greater occipital nerve
trapezius
FIGURE 9.28
Superficial and deep muscles of the back.
360
CHAPTER 9
The Upper Limb
circumflex scapular artery
levator scapulae
supraspinatus
rhomboid minor
rhomboid major
infraspinatus
latissimus dorsi
teres major
long head of triceps
lateral head of triceps
profunda artery
radial nerve
posterior circumflex
humeral artery
upper lateral cutaneous
nerve of arm
deltoid
axillary nerve
teres minor
infraspinatus
supraspinatus tendon
suprascapular ligament
suprascapular nerve and artery
deep branch of superficial cervical artery
dorsal scapular nerve
FIGURE 9.29
y nerve to the
Muscles, nerves, and blood vessels of the scapular region. Note the close relation of the axillar
shoulder joint.
Rotator Cuff Tendinitis
deltoid can then take over and complete the movement to a
the arm is passively assisted for the first 15° of abduction, the
tendon is unable to initiate abduction of the arm. However, if
ment of abduction. The patient with a ruptured supraspinatus
the main function of the supraspinatus muscle is to hold the
movement of the shoulder joint. It will be remembered that
of the tendon seriously interferes with the normal abduction
spinatus tendon can become calcified or rupture. Rupture
without surgery using nonsteroidal anti-inflammatory drugs and
the deltoid. Degenerative changes in the bursa are followed by
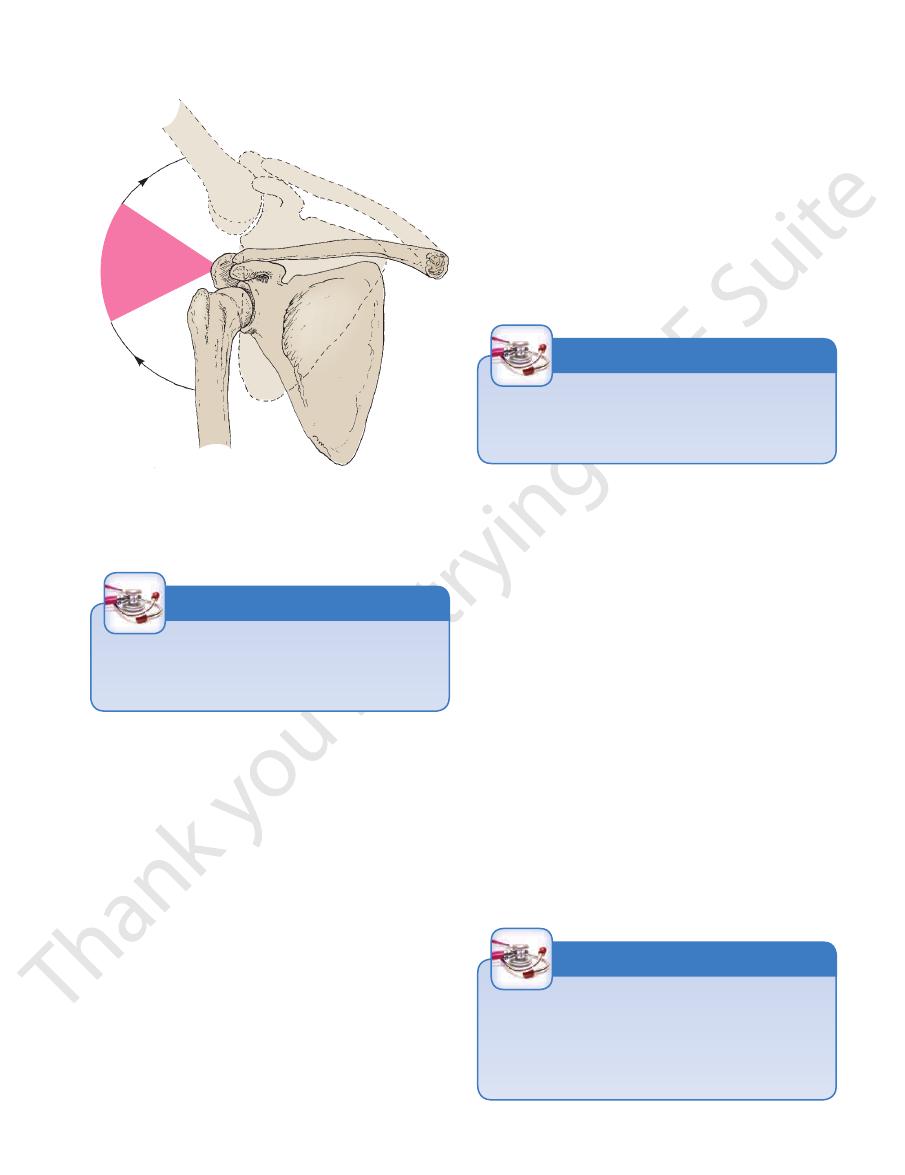
During abduction of the shoulder joint, the supraspinatus tendon
presses the humeral head into the glenoid cavity. Lesions of the
The rotator cuff, consisting of the tendons of the subscapularis,
supraspinatus, infraspinatus, and teres minor muscles, which
are fused to the underlying capsule of the shoulder joint, plays
an important role in stabilizing the shoulder joint. The rotator cuff
cuff are a common cause of pain in the shoulder region.
Failure of the cuff is due to either wear or tear. Wear is age
related. Excessive overhead activity of the upper limb may be the
cause of tendinitis, although many cases appear spontaneously.
is exposed to friction against the acromion (Fig. 9.30). Under nor-
mal conditions, the amount of friction is reduced to a minimum
by the large subacromial bursa, which extends laterally beneath
degenerative changes in the underlying supraspinatus tendon,
and these may extend into the other tendons of the rotator cuff.
Clinically, the condition is known as subacromial bursitis, supra-
spinatus tendinitis, or pericapsulitis. It is characterized by the
presence of a spasm of pain in the middle range of abduction
(Fig. 9.30), when the diseased area impinges on the acromion.
Extensive acute traumatic tears are best repaired surgically as
soon as possible. Small chronic cuff injuries are best managed
muscle exercises.
Rupture of the Supraspinatus Tendon
In advanced cases of rotator cuff tendinitis, the necrotic supra-
head of the humerus in the glenoid fossa at the commence-
right angle.
C L I N I C A L N O T E S
Basic Anatomy
361
130
50
˚
˚
FIGURE 9.30
Subacromial bursitis, supraspinatus tendinitis,
The axillary nerve has the following branches:
Branches
rior branches (Fig. 9.29).
humerus. It terminates by dividing into anterior and poste
joint and with the medial side of the surgical neck of the
ship with the inferior aspect of the capsule of the shoulder
nerve passes through the space, it comes into close relation
the posterior circumflex humeral artery (Fig. 9.29). As the
passes backward and enters the quadrangular space with
brachial plexus (C5 and 6) in the axilla (see page XXX). It
The axillary nerve arises from the posterior cord of the
Axillary Nerve
the shoulder joint.
supplies the supraspinatus and infraspinatus muscles and
ular notch, to reach the supraspinous fossa (Fig. 9.29). It
which bridges the suprascap
suprascapular ligament,
neck. It runs downward and laterally and passes beneath
brachial plexus (C5 and 6) in the posterior triangle in the
The suprascapular nerve arises from the upper trunk of the
Suprascapular Nerve
or pericapsulitis showing the painful arc in the middle range
of abduction, when the diseased area impinges on the
lateral edge of the acromion.
the
-
-
-
Arterial Anastomosis and Ligation of the Axillary
The existence of the anastomosis around the shoulder joint
Artery
is vital to preserving the upper limb should it be necessary to
ligate the axillary artery.
C L I N I C A L N O T E S
Accessory Nerve Injury
The accessory nerve can be injured as the result of stab
wounds to the neck.
C L I N I C A L N O T E S
Axillary Nerve Injury
The axillary nerve can be injured in dislocations of the shoul-
der joint.
C L I N I C A L N O T E S
■
around the surgical neck of the humerus (Fig. 9.31).
Both the circumflex arteries form an anastomosing circle
posterior circumflex humeral artery
The
anterior circumflex humeral artery
The
of the scapula, respectively.
branch supply the subscapular and infraspinous fossae
and its circumflex scapular
subscapular artery
The
Branches from the Axillary Artery
branch that runs down the medial border of the scapula
which gives off a deep
superficial cervical artery,
The
supraspinous and infraspinous fossae of the scapula
which is distributed to the
suprascapular artery,
The
Branches from the Subclavian Artery
tive of the position of the arm (Fig. 9.31).
quate blood flow takes place into the upper limb irrespec
artery and the axillary artery, thus ensuring that an ade
anastomosis exists between the branches of the subclavian
of its lumen. To compensate for this, an important arterial
kinking of the axillary artery and a temporary occlusion
The extreme mobility of the shoulder joint may result in
the deltoid muscle.
joint, two muscles, and the skin covering the lower half of
It is thus seen that the axillary nerve supplies the shoulder
(Fig. 9.29)
upper lateral cutaneous nerve of the arm
then emerges from the posterior border of the deltoid as
and a few branches to the deltoid,
the teres minor muscle
branch to
which gives off a
posterior terminal branch,
lower part.
cle; it supplies the deltoid and the skin that covers its
surgical neck of the humerus beneath the deltoid mus
which winds around the
anterior terminal branch,
An
to the shoulder joint
articular branch
An
■
■
■
-
■
■
A
the
Arterial Anastomosis around the
Shoulder Joint
-
-
■
■
■
■
■
■
■
■
■
■