362
CHAPTER 9
scapula and the lateral end of the clavicle (Fig. 9.32).
This occurs between the acromion of the
Articulation:
phalic vein and the left common carotid artery
brachiocephalic artery; on the left, the left brachioce
The sternohyoid muscle; on the right, the
Posteriorly:
omastoid and pectoralis major muscles
The skin and some fibers of the sternocleid
Anteriorly:
Important Relations
subclavius muscles (Fig. 9.33).
of the clavicle is produced by the pectoralis minor and the
toid, levator scapulae, and rhomboid muscles. Depression
the clavicle is produced by the trapezius, sternocleidomas
duced by the trapezius and rhomboid muscles. Elevation of
serratus anterior muscle. The backward movement is pro
The forward movement of the clavicle is produced by the
of the clavicle take place in the lateral compartment.
place in the medial compartment. Elevation and depression
Forward and backward movement of the clavicle takes
to the subclavius muscle.
The supraclavicular nerve and the nerve
Nerve supply:
articular surfaces.
attached to the margins of the cartilage covering the
This lines the capsule and is
Synovial membrane:
the sternal end of the clavicle (Fig. 9.32).
rib with the 1st costal cartilage to the inferior surface of
strong ligament that runs from the junction of the 1st
costoclavicular ligament
The
Accessory ligament:
below.
face of the clavicle above and to the first costal cartilage
attached to the superior margin of the articular sur
to the interior of the capsule, but it is also strongly
compartments (Fig. 9.32). Its circumference is attached
within the joint and divides the joint’s interior into two
This flat fibrocartilaginous disc lies
Articular disc:
ments.
sternoclavicular liga
behind the joint by the strong
The capsule is reinforced in front of and
Ligaments:
margins of the articular surfaces.
This surrounds the joint and is attached to the
Capsule:
Synovial double-plane joint
Type:
lage (Fig. 9.32).
clavicle, the manubrium sterni, and the 1st costal carti
This occurs between the sternal end of the
Articulation:
The Upper Limb
Sternoclavicular Joint
■
■
-
■
■
■
■
■
■
-
■
■
-
■
■
is a
■
■
■
■
Movements
Muscles Producing Movement
-
-
■
■
-
■
■
-
Acromioclavicular Joint
■
■
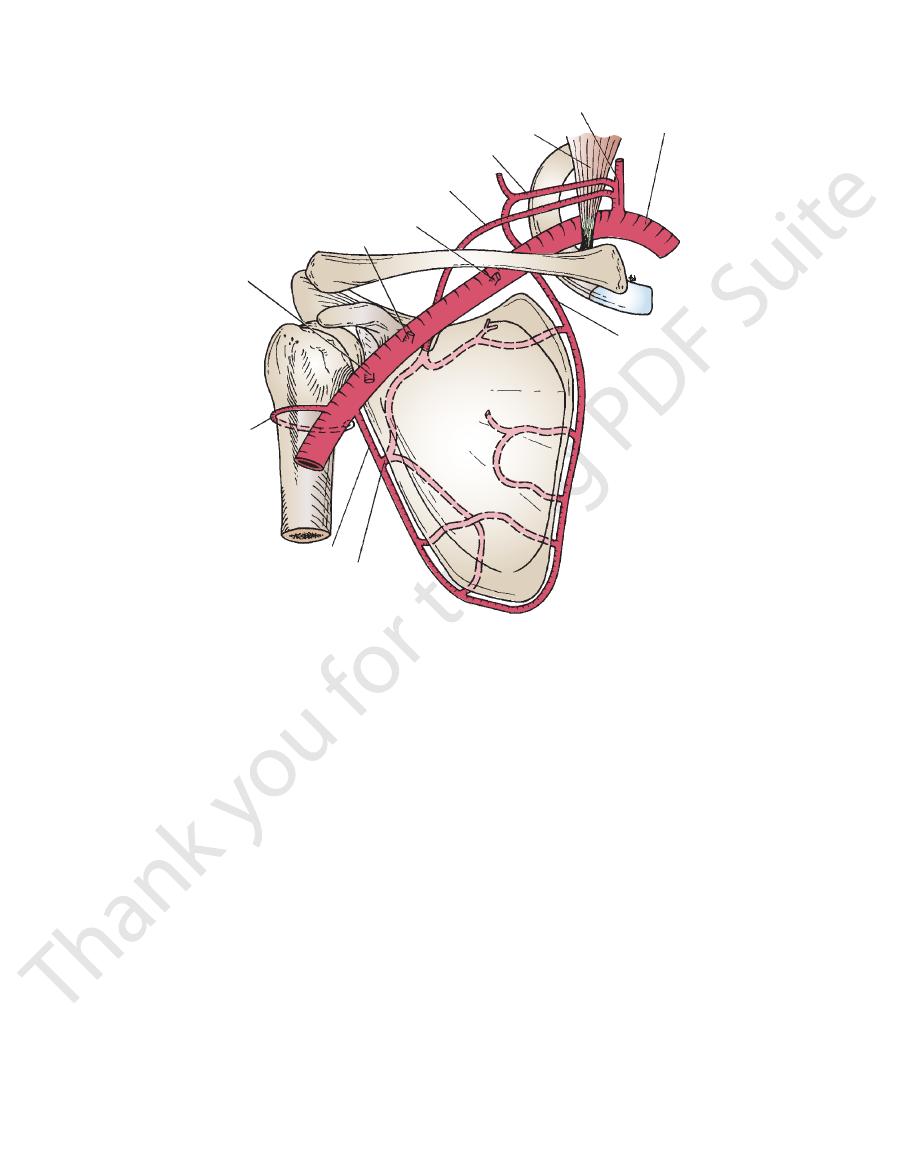
scalenus anterior
suprascapular artery
highest thoracic artery
thoracoacromial artery
lateral thoracic artery
anterior and
posterior circumflex
humeral arteries
subscapular artery
circumflex scapular artery
deep branch of
superficial cervical
artery
subclavian artery
thyrocervical trunk
superficial cervical artery
FIGURE 9.31
Arteries that take part in anastomosis around the shoulder joint.
Basic Anatomy
363
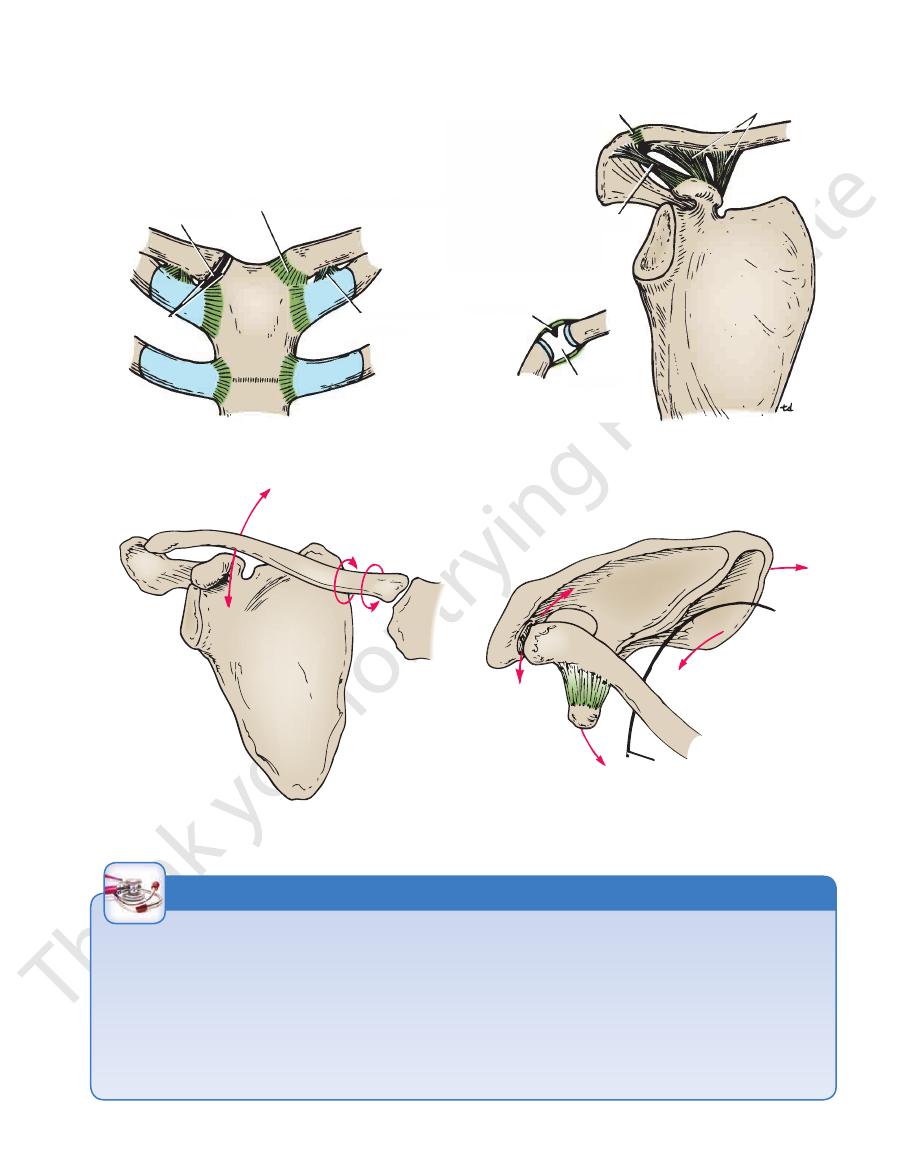
articular disc
capsule and anterior sternoclavicular ligament
costoclavicular
ligament
joint cavity
superior acromioclavicular ligament and capsule
coracoclavicular ligament
coracoacromial ligament
articular disc
joint cavity
A
B
articular disc
capsule and anterior sternoclavicular ligament
costoclavicular
ligament
nt cavity
coracoacromial ligament
articular disc
joint cavity
B
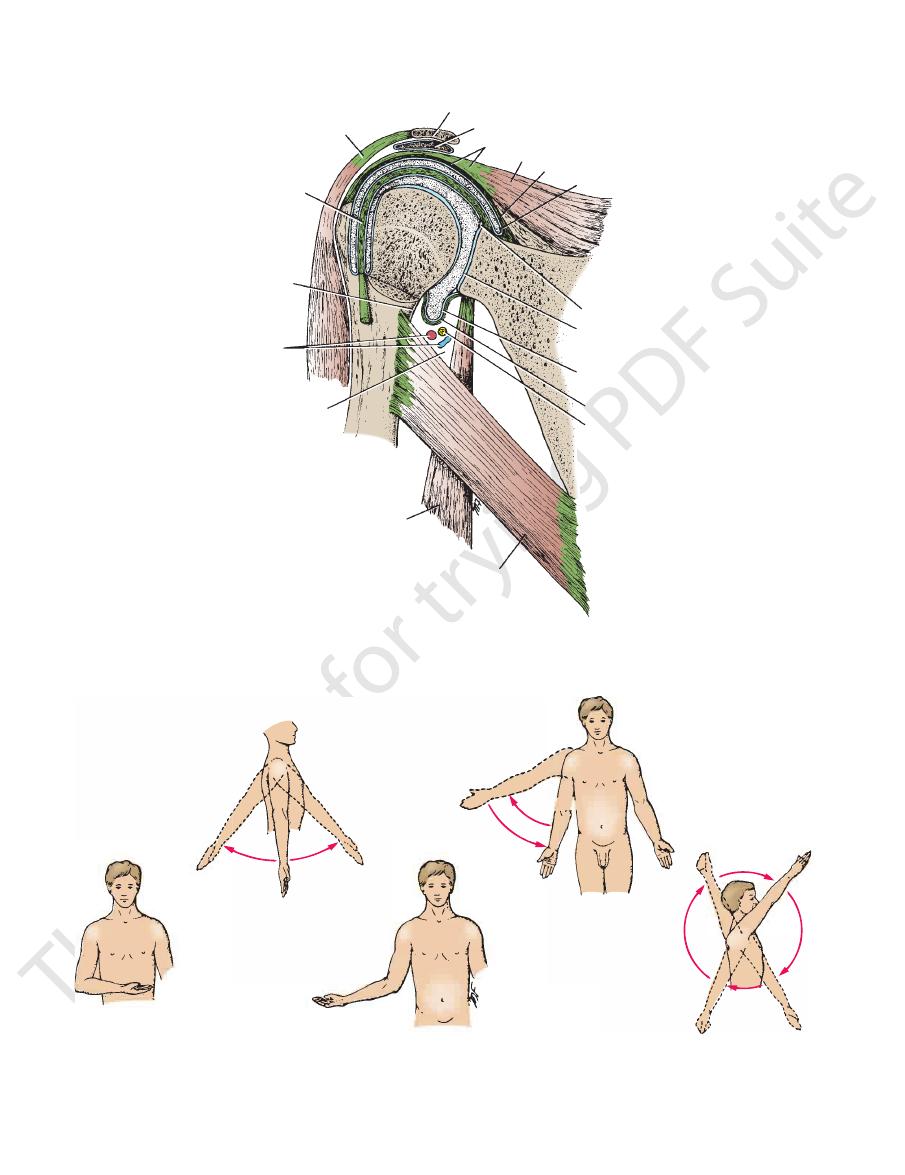
FIGURE 9.32
A.
Acromioclavicular joint.
Sternoclavicular joint. B.
trapezius (upper part)
sternocleidomastoid,
levator scapulae,
and rhomboid muscles
pectoralis
minor and
subclavius
trapezius
(middle fibers), levator
scapulae, and rhomboids
serratus
anterior
outer edge of
fourth rib
pectoralis
minor
FIGURE 9.33
The wide range of movements possible at the sternoclavicular and the acromioclavicular joints gives great
mobility to the clavicle and the upper limb.
Sternoclavicular Joint Injuries
is the more serious one because the displaced clavicle may
The strong costoclavicular ligament firmly holds the medial end
of the clavicle to the 1st costal cartilage. Violent forces directed
along the long axis of the clavicle usually result in fracture of that
bone, but dislocation of the sternoclavicular joint takes place
occasionally.
Anterior dislocation results in the medial end of the clav-
icle projecting forward beneath the skin; it may also be pulled
upward by the sternocleidomastoid muscle.
Posterior dislocation usually follows direct trauma applied to
the front of the joint that drives the clavicle backward. This type
press on the trachea, the esophagus, and major blood vessels in
the root of the neck.
If the costoclavicular ligament ruptures completely, it is
difficult to maintain the normal position of the clavicle once
reduction has been accomplished.
C L I N I C A L N O T E S
364
CHAPTER 9
The skin
Superiorly:
The trapezius muscle
Posteriorly:
The deltoid muscle
Anteriorly:
Important Relations
when the clavicle is elevated or depressed (Fig. 9.33).
A gliding movement takes place when the scapula rotates or
The suprascapular nerve
Nerve supply:
articular surfaces.
attached to the margins of the cartilage covering the
This lines the capsule and is
Synovial membrane:
the upper limb from the clavicle.
responsible for suspending the weight of the scapula and
undersurface of the clavicle (Fig. 9.32). It is largely
extends from the coracoid process to the
lar ligament
coracoclavicu
The very strong
Accessory ligament:
joint cavity from above (Fig. 9.32).
projects into the
fibrocartilaginous disc
wedge-shaped
reinforce the capsule; from the capsule, a
ligaments
inferior acromioclavicular
Ligaments: Superior
margins of the articular surfaces.
This surrounds the joint and is attached to the
Capsule:
Synovial plane joint
Type:
The Upper Limb
■
■
■
■
■
■
and
■
■
-
■
■
■
■
Movements
■
■
■
■
■
■
ing blocking or tackling in football or any severe fall, can result
and rotary movements of the scapula occur at this important
upper limb is transmitted to the clavicle through this ligament,
eral part of the clavicle. The greater part of the weight of the
binds the coracoid process to the undersurface of the lat
depends on the strong coracoclavicular ligament, which
upper surface of the acromion. The strength of the joint
dency for the lateral end of the clavicle to ride up over the
The plane of the articular surfaces of the acromioclavicular
Acromioclavicular Joint Injuries
joint passes downward and medially so that there is a ten-
-
ligament.
Acromioclavicular Dislocation
A severe blow on the point of the shoulder, as is incurred dur-
in the acromion being thrust beneath the lateral end of the
clavicle, tearing the coracoclavicular ligament. This condition
is known as shoulder separation. The displaced outer end of
the clavicle is easily palpable. As in the case of the sternocla-
vicular joint, the dislocation is easily reduced, but withdrawal
of support results in immediate redislocation.
C L I N I C A L N O T E S
Shoulder Joint
head of the humerus against the glenoid fossa of the
cle initiates the movement of abduction and holds the
supraspinatus, are involved. The supraspinatus mus
367). The middle fibers of the deltoid, assisted by the
thoracic wall (see scapular–humeral mechanism, page
at the shoulder joint and between the scapula and the
Abduction of the upper limb occurs both
Abduction:
dorsi, and teres major muscles.
formed by the posterior fibers of the deltoid, latissimus
Normal extension is about 45° and is per
Extension:
biceps, and coracobrachialis muscles.
by the anterior fibers of the deltoid, pectoralis major,
Normal flexion is about 90° and is performed
Flexion:
The following movements are possible (Fig. 9.36):
capsule is the weakest area.
support to the humerus. In addition, the inferior part of the
bows downward because of its length and gives little actual
humerus is supported by the long head of the triceps, which
the joint is abducted, the lower surface of the head of the
laris, supraspinatus, infraspinatus, and teres minor. When
front, above, and behind the joint—namely, the subscapu
the tone of the short rotator cuff muscles that cross in
in its movements.) The strength of the joint depends on
(Compare with the hip joint, which is stable but limited
the stability of the joint has been sacrificed to permit this.
The shoulder joint has a wide range of movement, and
The axillary and suprascapular nerves
Nerve supply:
subscapularis muscle (Fig. 9.34).
beneath the
subscapularis bursa
the capsule to form the
biceps brachii. It extends through the anterior wall of
lar sheath around the tendon of the long head of the
articular surfaces (Figs. 9.34 and 9.35). It forms a tubu
attached to the margins of the cartilage covering the
This lines the capsule and is
Synovial membrane:
(Fig. 9.34).
Its function is to protect the superior aspect of the joint
extends between the coracoid process and the acromion.
coracoacromial ligament
The
Accessory ligaments:
the humerus (Fig. 9.34).
root of the coracoid process to the greater tuberosity of
strengthens the capsule above and stretches from the
coracohumeral ligament
tuberosities (Fig. 9.34). The
ens the capsule and bridges the gap between the two
strength
transverse humeral ligament
the capsule. The
weak bands of fibrous tissue that strengthen the front of
are three
glenohumeral ligaments
The
Ligaments:
(the rotator cuff muscles).
supraspinatus, infraspinatus, and teres minor muscles
by fibrous slips from the tendons of the subscapularis,
allowing a wide range of movement. It is strengthened
of the humerus (Fig. 9.35). The capsule is thin and lax,
labrum; laterally, it is attached to the anatomic neck
ally to the margin of the glenoid cavity outside the
This surrounds the joint and is attached medi
Capsule:
Synovial ball-and-socket joint
Type:
(Figs. 9.34 and 9.35).
glenoid labrum
called the
deepened by the presence of a fibrocartilaginous rim
by hyaline articular cartilage, and the glenoid cavity is
cavity of the scapula. The articular surfaces are covered
of the humerus and the shallow, pear-shaped glenoid
This occurs between the rounded head
Articulation:
■
■
■
■
■
■
-
■
■
-
■
■
■
■
-
■
■
Movements
-
■
■
■
■
-
■
■
-
Basic Anatomy
vessels and brachial plexus
The subscapularis muscle and the axillary
Anteriorly:
Important Relations
movements.
This is a combination of the above
Circumduction:
deltoid muscle.
mus dorsi, the teres major, and the anterior fibers of the
55°. This is performed by the subscapularis, the latissi
Normal medial rotation is about
Medial rotation:
minor, and the posterior fibers of the deltoid muscle.
45°. This is performed by the infraspinatus, the teres
Normal lateral rotation is 40° to
Lateral rotation:
teres minor muscles.
the pectoralis major, latissimus dorsi, teres major, and
45° across the front of the chest. This is performed by
Normally, the upper limb can be swung
Adduction:
joint.
to contract and abduct the humerus at the shoulder
scapula; this latter function allows the deltoid muscle
365
■
■
■
■
■
■
-
■
■
■
■
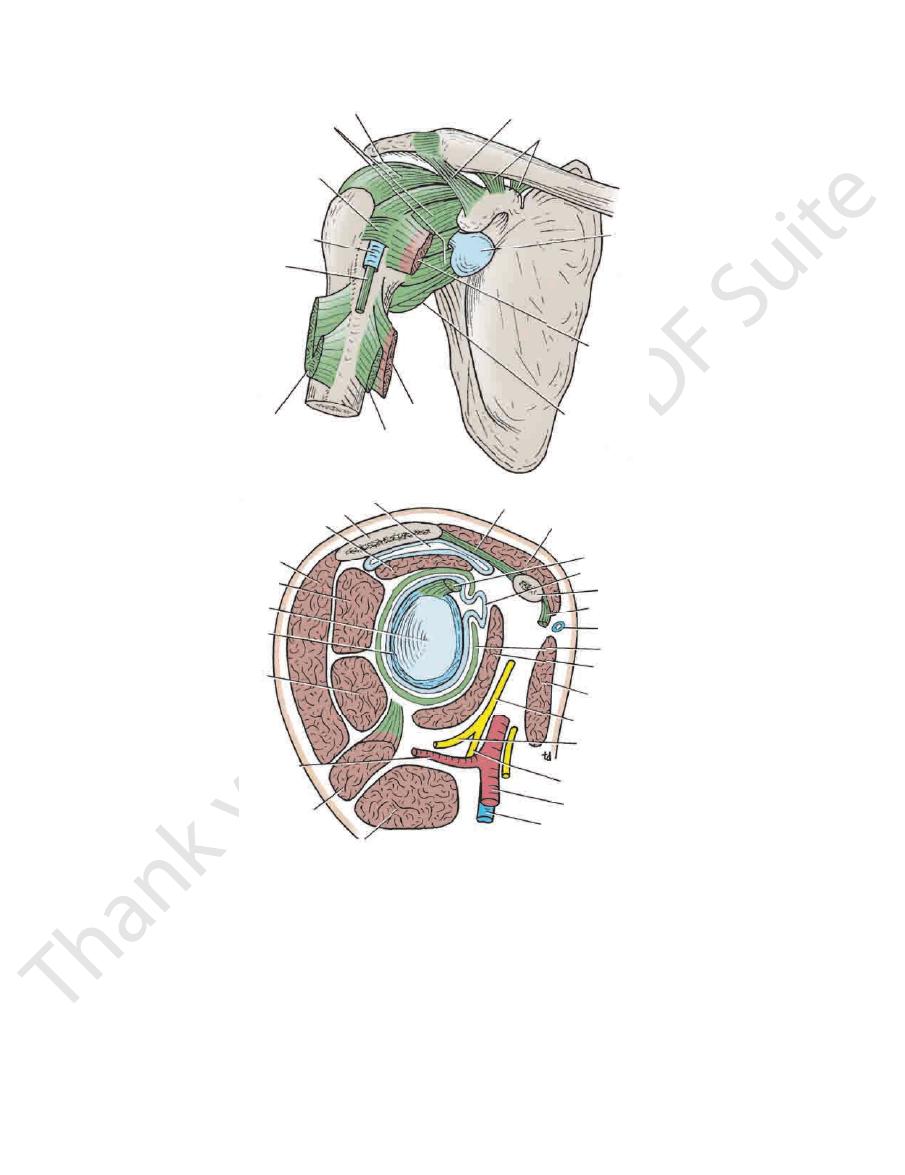
coracohumeral ligament
capsule of shoulder joint
transverse humeral ligament
synovial sheath
tendon of long
head of biceps
pectoralis major tendon
latissimus dorsi
teres major
capsule of shoulder joint
subscapularis
subacromial bursa
coracoclavicular ligament
coracoacromial ligament
A
subscapularis bursa
acromion
supraspinatus
deltoid
infraspinatus
glenoid fossa
glenoid labrum
teres minor
posterior circumflex
humeral artery
long head of triceps
teres major
axillary vein
axillary artery
radial nerve
axillary nerve
posterior cord of brachial plexus
pectoralis major
subscapularis
capsule
cephalic vein
short head of biceps
coracoid process
subscapularis bursa
long head of biceps
deltoid
B
coracoacromial ligament
FIGURE 9.34
Shoulder joint and its relations.
Sagittal section.
Anterior view.
A.
B.
366
CHAPTER 9
The Upper Limb
acromium
subacromial bursa
part of rotator cuff
supraspinatus
capsule
synovial membrane
glenoid labrum
glenoid fossa
scapula
synovial membrane
capsule
axillary nerve
teres major
long head of triceps
quadrangular space
posterior
axillary
vessels
surgical
neck of
humerus
long head of biceps
deltoid
FIGURE 9.35
Interior of the shoulder joint.
extension
flexion
adduction
abduction
lateral rotation
medial rotation
circumduction
FIGURE 9.36
The movements possible at the shoulder joint. Pure glenohumeral abduction is possible only as much as about
120°; further movement of the upper limb above the level of the shoulder requires rotation of the scapula (see text).
Basic Anatomy
through the joint and emerges beneath the transverse
The tendon of the long head of the biceps muscle passes
lary nerve, and the posterior circumflex humeral vessels
The long head of the triceps muscle, the axil
Inferiorly:
bursa, coracoacromial ligament, and deltoid muscle
The supraspinatus muscle, subacromial
Superiorly:
The infraspinatus and teres minor muscles
Posteriorly:
367
■
■
■
■
■
■
-
ligament.
intercostobrachial nerves
(T1) and the
the arm
medial cutaneous nerve of
of the arm is supplied by the
(C5 and 6). The skin of the armpit and the medial side
a branch of the radial nerve
cutaneous nerve of the arm,
lower lateral
the arm below the deltoid is supplied by the
lary nerve (C5 and 6). The skin over the lateral surface of
a branch of the axil
lateral cutaneous nerve of the arm,
upper
over the lower half of the deltoid is supplied by the
(C3 and 4). The skin
supraclavicular nerves
is from the
point of the shoulder to halfway down the deltoid muscle
The sensory nerve supply (Fig. 9.38) to the skin over the
Superficial Sensory Nerves
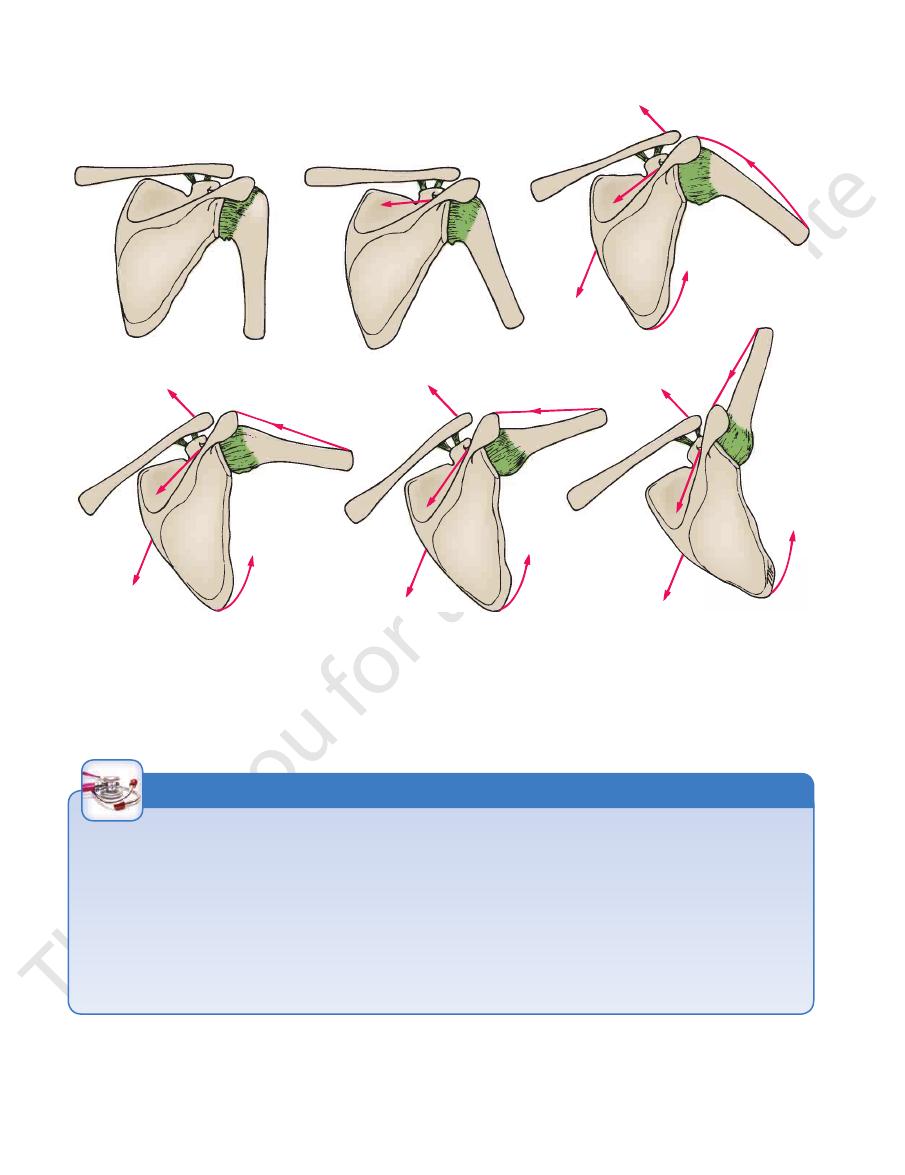
these movements.
shows the direction of pull of the muscles responsible for
summarizes the movements of abduction of the arm and
head is accomplished by rotating the scapula. Figure 9.37
of the acromion. Further elevation of the arm above the
ity of the humerus comes into contact with the lateral edge
At about 120° of abduction of the arm, the greater tuberos
joint and a 1° abduction occurs by rotation of the scapula.
abduction of the arm, a 2° abduction occurs in the shoulder
as well as movement at the shoulder joint. For every 3° of
Abduction of the arm involves rotation of the scapula
clavicular ligament.
of rotation may be considered to pass through the coraco
so that the position of the glenoid fossa is altered, the axis
tone of muscles. When the scapula rotates on the chest wall
cle by the strong coracoclavicular ligament assisted by the
The scapula and upper limb are suspended from the clavi
The Scapular–Humeral Mechanism
-
-
-
The Upper Arm
Skin
-
(T2). The
skin of the back of the arm (Fig. 9.38) is supplied by
the
the radial nerve (C8).
a branch of
posterior cutaneous nerve of the arm,
Stability of the Shoulder Joint
example, diseases of the spinal cord and vertebral column and
Injury to the shoulder joint is followed by pain, limitation of
nerve. The joint is sensitive to pain, pressure, excessive traction,
displacement of the humerus can also stretch and damage the
of skin sensation over the lower half of the deltoid. Downward
nerve, as indicated by paralysis of the deltoid muscle and loss
into the quadrangular space can cause damage to the axillary
muscle. A subglenoid displacement of the head of the humerus
the humerus is no longer bulging laterally beneath the deltoid
shoulder is seen to be lost because the greater tuberosity of
with shoulder dislocation, the rounded appearance of the
violence to the front of the joint. On inspection of the patient
Posterior dislocations are rare and are usually caused by direct
tendons of these muscles are fused to the underlying capsule of
of the short muscles that bind the upper end of the humerus to
ble structure. Its strength almost entirely depends on the tone
The shallowness of the glenoid fossa of the scapula and the lack
of support provided by weak ligaments make this joint an unsta-
the scapula—namely, the subscapularis in front, the supraspi-
natus above, and the infraspinatus and teres minor behind. The
the shoulder joint. Together, these tendons form the rotator cuff.
The least supported part of the joint lies in the inferior loca-
tion, where it is unprotected by muscles.
Dislocations of the Shoulder Joint
The shoulder joint is the most commonly dislocated large joint.
Anterior Inferior Dislocation
Sudden violence applied to the humerus with the joint fully
abducted tilts the humeral head downward onto the inferior
weak part of the capsule, which tears, and the humeral head
comes to lie inferior to the glenoid fossa. During this move-
ment, the acromion has acted as a fulcrum. The strong flexors
and adductors of the shoulder joint now usually pull the humeral
head forward and upward into the subcoracoid position.
Posterior Dislocations
radial nerve.
Shoulder Pain
The synovial membrane, capsule, and ligaments of the shoulder
joint are innervated by the axillary nerve and the suprascapular
and distention. The muscles surrounding the joint undergo reflex
spasm in response to pain originating in the joint, which in turn
serves to immobilize the joint and thus reduce the pain.
movement, and muscle atrophy owing to disuse. It is important
to appreciate that pain in the shoulder region can be caused by
disease elsewhere and that the shoulder joint may be normal; for
the pressure of a cervical rib (see page XXX) can cause shoul-
der pain. Irritation of the diaphragmatic pleura or peritoneum
can produce referred pain via the phrenic and supraclavicular
nerves.
C L I N I C A L N O T E S
368
CHAPTER 9
The Upper Limb
1
T
D
S
T
3
SA
T
D
S
T
5
SA
S
2
T
D
S
T
4
SA
T
D
S
SA
T
6
S
FIGURE 9.37
Movements of abduction of the shoulder joint and rotation of the scapula and the muscles producing these
SA, serratus anterior.
mion. Elevation of the arm above the head is accomplished by rotating the scapula. S, supraspinatus; D, deltoid; T, trapezius;
rotation of the scapula. At about 120° of abduction, the greater tuberosity of the humerus hits the lateral edge of the acro
movements. Note that for every 3° of abduction of the arm, a 2° abduction occurs in the shoulder joint, and 1° occurs by
-
Dermatomes and Cutaneous Nerves
The skin over the point of the shoulder and halfway down the
of the same segment, pass to the skin in two or more different
upper limb; the C7 dermatome is situated on the middle finger;
cal segments C3 to 6 are located along the lateral margin of the
upper limb. It is seen that the dermatomes for the upper cervi
It may be necessary for a physician to test the integrity of the
spinal cord segments of C3 through T1. The diagrams in Figures
1.23 and 1.24 show the arrangement of the dermatomes of the
-
and the dermatomes for C8, T1, and T2 are along the medial mar-
gin of the limb. The nerve fibers from a particular segment of the
spinal cord, although they exit from the cord in a spinal nerve
cutaneous nerves.
lateral surface of the deltoid muscle is supplied by the supracla-
vicular nerves (C3 and 4). Pain may be referred to this region as a
result of inflammatory lesions involving the diaphragmatic pleura
or peritoneum. The afferent stimuli reach the spinal cord via the
phrenic nerves (C3, 4, and 5). Pleurisy, peritonitis, subphrenic
abscess, or gallbladder disease may therefore be responsible
for shoulder pain.
C L I N I C A L N O T E S