
Basic Anatomy
which crosses in front of the
branch of the median nerve,
palmar cutaneous
9.38 and 9.55) is derived from the
supply to the skin of the palm (Figs.
sensory nerve
The
so improve the grip of the palm in holding a rounded object.
rugate the skin at the base of the hypothenar eminence and
superficial branch of the ulnar nerve. Its function is to cor
and is inserted into the skin of the palm. It is supplied by the
arises from the flexor retinaculum and palmar aponeurosis
(Fig. 9.55) is a small muscle that
palmaris brevis
The
the site of joints. Sweat glands are present in large numbers.
sites of skin movement, which are not necessarily placed at
fibrous bands. The skin shows many flexure creases at the
bound down to the underlying deep fascia by numerous
The skin of the palm of the hand is thick and hairless. It is
pollicis brevis (Fig. 9.65).
the tendons of the abductor pollicis longus and extensor
between the lateral collateral ligament of the wrist joint and
The radial artery reaches the back of the hand by passing
extends above and below the retinaculum.
compartment is provided with a synovial sheath, which
that contain the tendons of the extensor muscles. Each
underlying radius and ulna and form six compartments
Beneath the extensor retinaculum, fibrous septa pass to the
common compartment.
have separate synovial sheaths but share a
vis tendons
extensor pollicis bre
Abductor pollicis longus
lateral part of the posterior surface of the radius.
share a common synovial sheath and are situated on the
brevis tendons
Extensor carpi radialis longus
medial side of the dorsal tubercle of the radius.
winds around the
Extensor pollicis longus tendon
397
■
■
■
■
and
■
■
and the
-
The Palm of the Hand
Skin
-
Muscles of the Posterior Fascial Compartment of the Forearm
T A B L E 9 . 8
Muscle
Origin
Insertion
Nerve Supply
Nerve Roots
a
Action
Extensor carpi
radialis brevis
Lateral epicondyle of
humerus
Posterior surface
of base of third
metacarpal bone
Deep branch of
radial nerve
C7, 8
Extends and abducts
hand at wrist joint
Extensor
digitorum
Lateral epicondyle of
humerus
Middle and distal
phalanges of
medial four
fingers
Deep branch of
radial nerve
C7, 8
Extends fingers and hand
(see text for details)
Extensor digiti
minimi
Lateral epicondyle of
humerus
Extensor expansion
of little finger
Deep branch of
radial nerve
C7, 8
Extends metacarpal
phalangeal joint of little
finger
Extensor carpi
ulnaris
Lateral epicondyle of
humerus
Base of 5th
metacarpal bone
Deep branch of
radial nerve
C7, 8
Extends and adducts
hand at wrist joint
Anconeus
Lateral epicondyle of
humerus
Lateral surface
of olecranon
process of ulna
Radial nerve
C7, 8; T1
Extends elbow joint
Supinator
Lateral epicondyle of
humerus, anular
ligament of proximal
radioulnar joint, and
ulna
Neck and shaft of
radius
Deep branch of
radial nerve
C5, 6
Supination of forearm
Abductor pollicis
longus
Posterior surface of
shafts of radius and
ulna
Base of first
metacarpal bone
Deep branch of
radial nerve
C7, 8
Abducts and extends
thumb
Extensor pollicis
brevis
Posterior surface of
shaft of radius
Base of proximal
phalanx of thumb
Deep branch of
radial nerve
C7, 8
Extends
metacarpophalangeal
joints of thumb
Extensor pollicis
longus
Posterior surface of
shaft of ulna
Base of distal
phalanx of thumb
Deep branch of
radial nerve
C7, 8
Extends distal phalanx of
thumb
Extensor indicis
Posterior surface of
shaft of ulna
Extensor expansion
of index finger
Deep branch of
radial nerve
C7, 8
Extends
metacarpophalangeal
joint of index finger
a
The predominant nerve root supply is indicated by boldface type.
398
CHAPTER 9
cialis and the flexor carpi radialis muscles (Fig. 9.54).
space between the flexor digitorum superfi
restricted
The median nerve passes beneath the flexor retinaculum
through the lateral part of the tunnel in its own synovial
The tendon of the flexor pollicis longus muscle runs
the tendons to enter them from the lateral side.
the lateral side (Fig. 9.54). This allows the arterial supply to
and profundus invaginate a common synovial sheath from
All eight tendons of the flexor digitorum superficialis
tendons.
cle are on the same plane and lie behind the superficialis
The tendons of the flexor digitorum profundus mus
become arranged on the same plane (Fig. 9.62).
der of the flexor retinaculum, the four tendons diverge and
of those to the index and little fingers. At the lower bor
rows, those to the middle and ring fingers lying in front
superficialis muscle are arranged in anterior and posterior
nerve. The four separate tendons of the flexor digitorum
through the tunnel and are accompanied by the median
The long flexor tendons to the fingers and thumb pass
by the flexor retinaculum (Fig. 9.54).
forms a bony gutter. The gutter is converted into a tunnel
The carpus is deeply concave on its anterior surface and
The Carpal Tunnel
and to protect the underlying tendons.
attachment to the overlying skin and so improve the grip
The function of the palmar aponeurosis is to give firm
page 404).
take part in the formation of the palmar fascial spaces (see
borders, fibrous septa pass posteriorly into the palm and
the hypothenar and thenar muscles. From each of these
rosis are continuous with the thinner deep fascia covering
The medial and lateral borders of the palmar aponeu
the deep transverse ligaments.
tendons and finally fuse with the fibrous flexor sheath and
deep band divides into two, which diverge around the flexor
the other passing deeply to the root of the finger; here each
into two bands, one passing superficially to the skin and
at the bases of the fingers into four slips. Each slip divides
gus tendon (Fig. 9.55). The base of the aponeurosis divides
retinaculum and receives the insertion of the palmaris lon
aponeurosis is attached to the distal border of the flexor
tral area of the palm (Fig. 9.55). The apex of the palmar
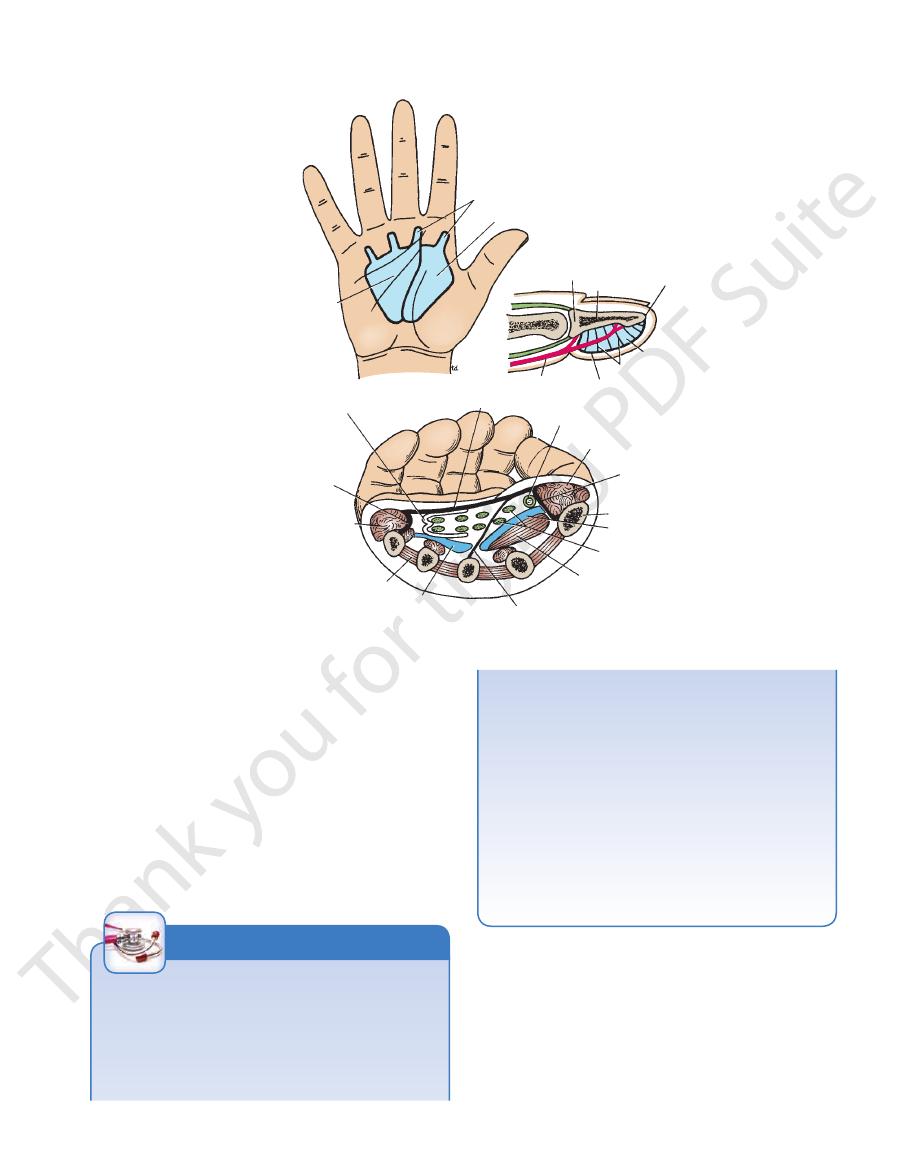
The palmar aponeurosis is triangular and occupies the cen
palmar aponeurosis.
(described on page XXX) and the
flexor retinaculum
The deep fascia of the wrist and palm is thickened to form
(Fig. 9.38).
superficial branch of the radial nerve
or the
lateral cutaneous nerve of the forearm
plied by the
The skin over the base of the thenar eminence is sup
(Fig. 9.54) and supplies the medial part of the palm.
latter nerve also crosses in front of the flexor retinaculum
palmar cutaneous branch of the ulnar nerve;
flexor retinaculum and supplies the lateral part of the palm,
The Upper Limb
and the
the
-
Deep Fascia
the
The Palmar Aponeurosis
-
-
-
-
-
sheath.
in a
-
Carpal Tunnel Syndrome
The carpal tunnel, formed by the concave anterior surface
of the carpal bones and closed by the flexor retinaculum, is
tightly packed with the long flexor tendons of the fingers, with
their surrounding synovial sheaths, and the median nerve
(Fig.
vial sheaths of the flexor tendons or arthritic changes in the
median nerve within the tunnel. The exact cause of the com
of the thenar muscles. It is produced by compression of the
a burning pain
9.54). Clinically, the syndrome consists of
or “pins and needles” along the distribution of the median
nerve to the lateral three and a half fingers and weakness
-
pression is difficult to determine, but thickening of the syno-
carpal bones are thought to be responsible in many cases.
As you would expect, no paresthesia occurs over the thenar
eminence because this area of skin is supplied by the palmar
cutaneous branch of the median nerve, which passes super-
ficially to the flexor retinaculum. The condition is dramatically
relieved by decompressing the tunnel by making a longitudinal
incision through the flexor retinaculum.
C L I N I C A L N O T E S
native treatment of injection of the enzyme collagenase into
are actually extended by the pressure of the fingers against
joints. The distal interphalangeal joints are not involved and
fingers results in flexion of the proximal interphalangeal
long-standing cases, the pull on the fibrous sheaths of these
condition involves the little finger in the same manner. In
palm, flexing it at the metacarpophalangeal joint. Later, the
near the root of the ring finger and draws that finger into the
tion and may eventually disable the hand. It commonly starts
Dupuytren’s Contracture
Dupuytren’s contracture is a localized thickening and con-
tracture of the palmar aponeurosis, which limits hand func-
the palm.
Surgical division of the fibrous bands followed by physio-
therapy to the hand is the usual form of treatment. The alter-
the contracted bands of fibrous tissue has been shown to
significantly reduce the contractures and improve mobility.
C L I N I C A L N O T E S
Fibrous Flexor Sheaths
the base of the distal phalanx. The sheath and the bones form a
whereas the distal end of the sheath is closed and is attached to
ges (Fig. 9.66). The proximal end of the fibrous sheath is open,
strong fibrous sheath that is attached to the sides of the phalan
acarpal to the base of the distal phalanx, is provided with a
The anterior surface of each finger, from the head of the met-
-
blind tunnel in which the flexor
ns of the finger lie.
tendo
Basic Anatomy
mesentery and convey blood vessels to the tendons.
rior surface of the phalanges (Fig. 9.63). They resemble a
synovial membrane that connect the tendons to the ante
are small vascular folds of
brevia
vincula longa
The
of subjects.
at the level of the wrist in about 50%
ulnar bursa)
cialis and profundus tendons (sometimes referred to as
cates with the common synovial sheath of the superfi
communi
radial bursa)
(sometimes referred to as the
The synovial sheath of the flexor pollicis longus
retinaculum and the fibrous flexor sheaths.
smoothly, with a minimum of friction, beneath the flexor
the thumb. These sheaths allow the long tendons to move
gus tendon has its own synovial sheath that passes into
as they enter the fingers. The flexor pollicis lon
sheaths
digital synovial
the middle, and the ring fingers acquire
and the distal ends of the long flexor tendons of the index,
of the sheath stops abruptly on the middle of the palm,
ruption on the tendons of the little finger. The lateral part
part of this common sheath extends distally without inter
vial sheath from the lateral side (Fig. 9.54). The medial
cialis and profundus muscles invaginate a common syno
In the hand, the tendons of the flexor digitorum superfi
lax over the joints.
The fibrous sheath is thick over the phalanges but thin and
flexor digitorum superficialis and profundus (Fig. 9.66).
medial fingers, the tunnel is occupied by the tendons of the
don of the flexor pollicis longus. In the case of the four
In the thumb, the osteofibrous tunnel contains the ten
399
-
Synovial Flexor Sheaths
-
-
-
-
-
-
the
and
-
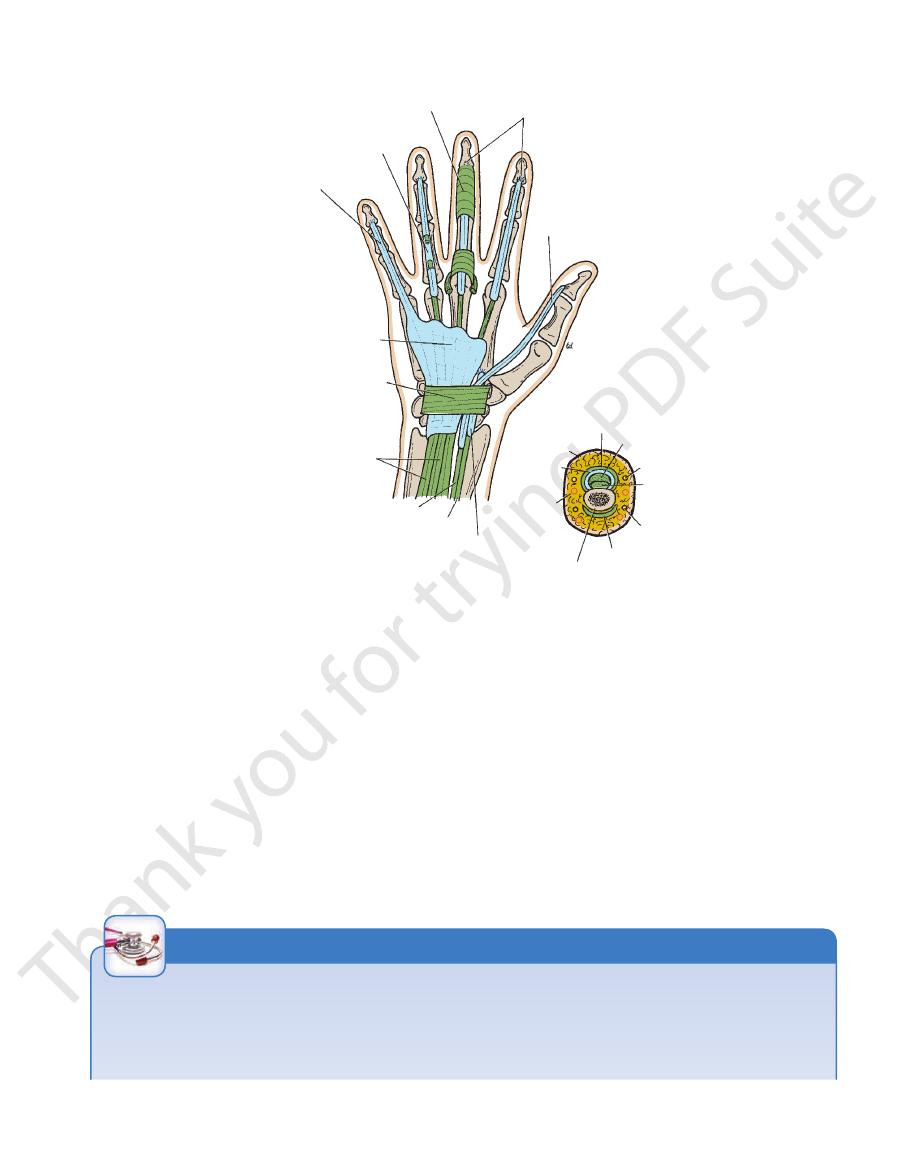
fibrous flexor sheath
digital synovial sheath opened
to show flexor tendons
digital synovial sheath
common flexor synovial sheath (ulnar bursa)
flexor retinaculum
flexor digitorum superficialis
flexor pollicis longus
flexor carpi radialis
synovial sheath for flexor carpi radialis
digital artery
synovial
sheath
skin
fibrous flexor sheath
flexor digitorum superficialis
palmar digital nerve
flexor digitorum profundus
dorsal digital nerve
dorsal extensor expansion
proximal phalanx
synovial sheath for flexor pollicis
longus (radial bursa)
insertion of flexor digitorum profundus
FIGURE 9.66
or synovial sheaths. Cross section of a finger is also
Anterior view of the palm of the hand showing the flex
shown.
Tenosynovitis of the Synovial Sheaths of the Flexor
with pus; the finger is held semiflexed and is swollen. Any
point of a needle or thorn. Rarely, the sheath may become
Tendons
Tenosynovitis is an infection of a synovial sheath. It most com-
monly results from the introduction of bacteria into a sheath
through a small penetrating wound, such as that made by the
infected by extension of a pulp-space infection.
Infection of a digital sheath results in distention of the sheath
attempt to extend the finger is accompanied by extreme pain
C L I N I C A L N O T E S
(continued)
400
CHAPTER 9
phalanx (Fig. 9.63).
inserted into the anterior surface of the base of the distal
of the superficialis tendon, continues downward, to be
digitorum profundus, having passed through the division
borders of the middle phalanx. Each tendon of the flexor
at once into two further slips, which are attached to the
superficialis tendon, having united again, divides almost
partial decussation of the fibers takes place (Fig. 9.63). The
tendon and meet on its deep or posterior surface, where
divides into two halves, which pass around the profundus
the fibrous flexor sheath; opposite the proximal phalanx it
Each tendon of the flexor digitorum superficialis enters
Insertion of the Long Flexor Tendons
The Upper Limb
The situation can be relieved surgically by incising the fibrous
fibrous flexor sheath anterior to the metacarpophalangeal
the long flexor tendons that catches on a narrowing of the
It is caused by the presence of a localized swelling of one of
ping when a patient is asked to flex and extend the fingers.
Trigger Finger
In trigger finger, there is a palpable and even audible snap-
joint. It may take place either in flexion or in extension. A simi-
lar condition occurring in the thumb is called trigger thumb.
flexor sheath.
C L I N I C A L N O T E S
Small Muscles of the Hand
are described in Table 9.9.
muscles are seen in Figures 9.55, 9.67, 9.68, and 9.69 and
the thumb, and the short muscles of the little finger. The
interossei muscles, the short muscles of
muscles, the eight
The small muscles of the hand include the four lumbrical
1
because the distended sheath is stretched. As the inflammatory
cula longa and brevia (Fig. 9.63). Rupture or later severe scarring
process continues, the pressure within the sheath rises and may
compress the blood supply to the tendons that travel in the vin-
of the tendons may follow.
A further increase in pressure can cause the sheath to rupture
at its proximal end. Anatomically, the digital sheath of the index
finger is related to the thenar space, whereas that of the ring
finger is related to the midpalmar space. The sheath for the
It restores the thumb to its anatomic position, which is flush
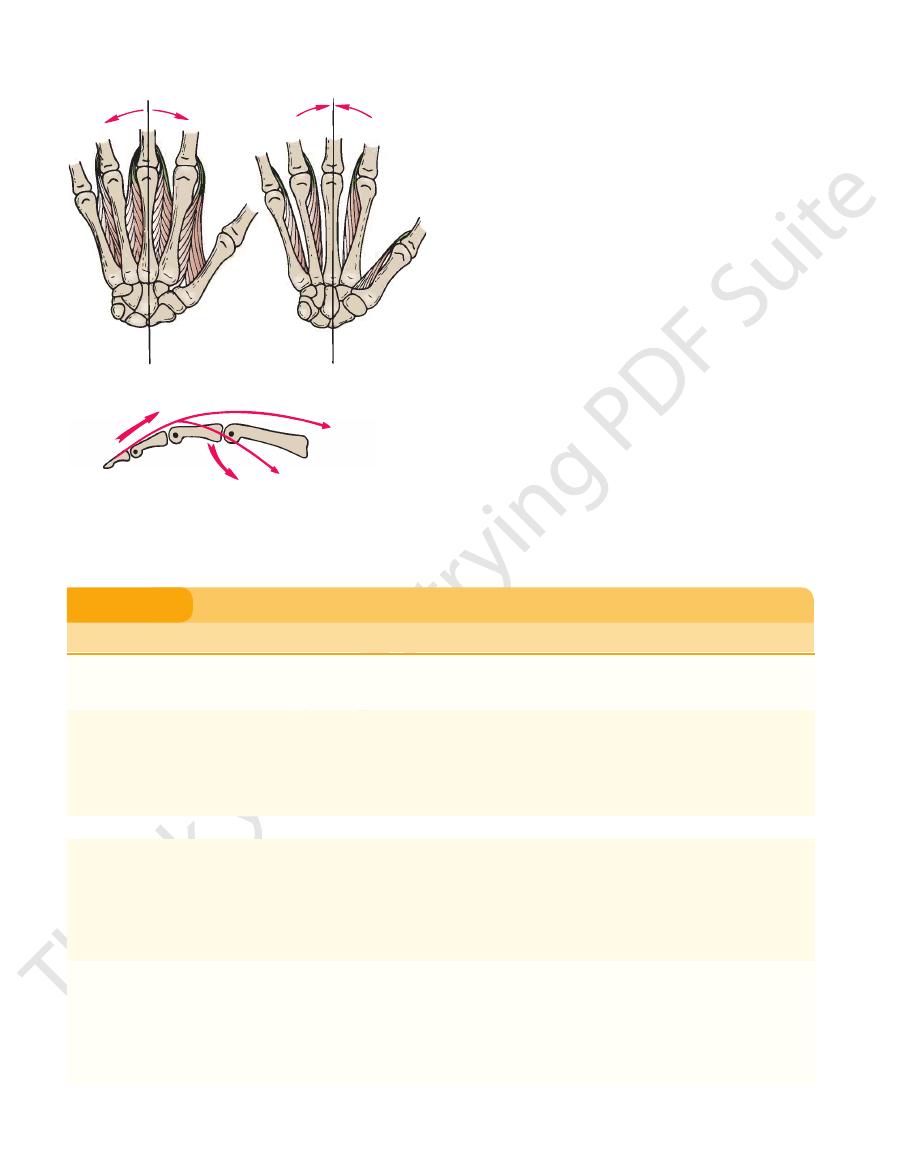
of the abducted thumb in the anteroposterior plane.
This movement can be defined as a movement backward
Adduction of the Thumb
pophalangeal joint.
takes place at the carpometacarpal joint and the metacar
forward of the thumb in the anteroposterior plane. It
Abduction of the thumb may be defined as a movement
Abduction of the Thumb
metacarpal bone at the carpometacarpal joint.
a small amount of abduction and medial rotation of the
the carpometacarpal and metacarpophalangeal joints and
up objects. This complex movement involves a flexion of
form one claw in the pincer-like action used for picking
gers. It is an important muscle and enables the thumb to
contact with the palmar surface of the tips of the other fin
the palmar surface of the tip of the thumb may come into
the thumb medially and forward across the palm so that
It should be noted that the opponens pollicis muscle pulls
Opposition of the Thumb
thenar eminence.
three of these muscles form the
the adductor pollicis (Figs. 9.59, 9.62, and 9.67). The first
brevis, the flexor pollicis brevis, the opponens pollicis, and
The short muscles of the thumb are the abductor pollicis
of the forearm between the flexor digitorum profundus ante
Should such an infection be neglected, pus may burst through
These relationships explain how infection can extend from the
middle finger is related to both the thenar and midpalmar spaces.
digital synovial sheaths and involve the palmar fascial spaces.
In the case of infection of the digital sheaths of the little fin-
ger and thumb, the ulnar and radial bursae are quickly involved.
the proximal ends of these bursae and enter the fascial space
-
riorly and the pronator quadratus and the interosseous mem-
brane posteriorly. This fascial space in the forearm is commonly
referred to clinically as the space of Parona.
Short Muscles of the Thumb
-
-
with the palm. The adductor pollicis is the muscle that, in
pincers grip of the thumb. Adduction of the thumb occurs
pollicis muscles, is largely responsible for the power of the
association with the flexor pollicis longus and the opponens
at the carpometacarpal and at the
ophalangeal
metacarp
The opponens digiti minimi muscle is only capable of rotat
Opposition of the Little Finger
(Figs 9.59, 9.62, and 9.67).
nence
hypothenar emi
digiti minimi, which together form the
minimi, the flexor digiti minimi brevis, and the opponens
The short muscles of the little finger are the abductor digiti
joint.
Short Muscles of the Little Finger
-
-
ing the fifth metacarpal bone to a slight degree.
ver,
Howe
mar muscles. Some authors describe only three palmar interossei
1
There are eight interossei, consisting of four dorsal and four pal-
and state that the first palmar interosseous is in reality a second
head to the flexor pollicis brevis: others believe that it is part of the
adductor pollicis muscle.
Basic Anatomy
401
second dorsal interosseous
third palmar interosseous
third dorsal interosseous
fourth dorsal interosseous
fourth palmar interosseous
deep palmar arch
opponens digiti minimi
abductor digiti minimi
ulnar artery and nerve
flexor retinaculum
flexor carpi radialis
radial artery
first palmar interosseous
flexor pollicis brevis
sesamoid bones
adductor pollicis
first dorsal interosseous
second palmar interosseous
abductor pollicis longus
abductor pollicis brevis
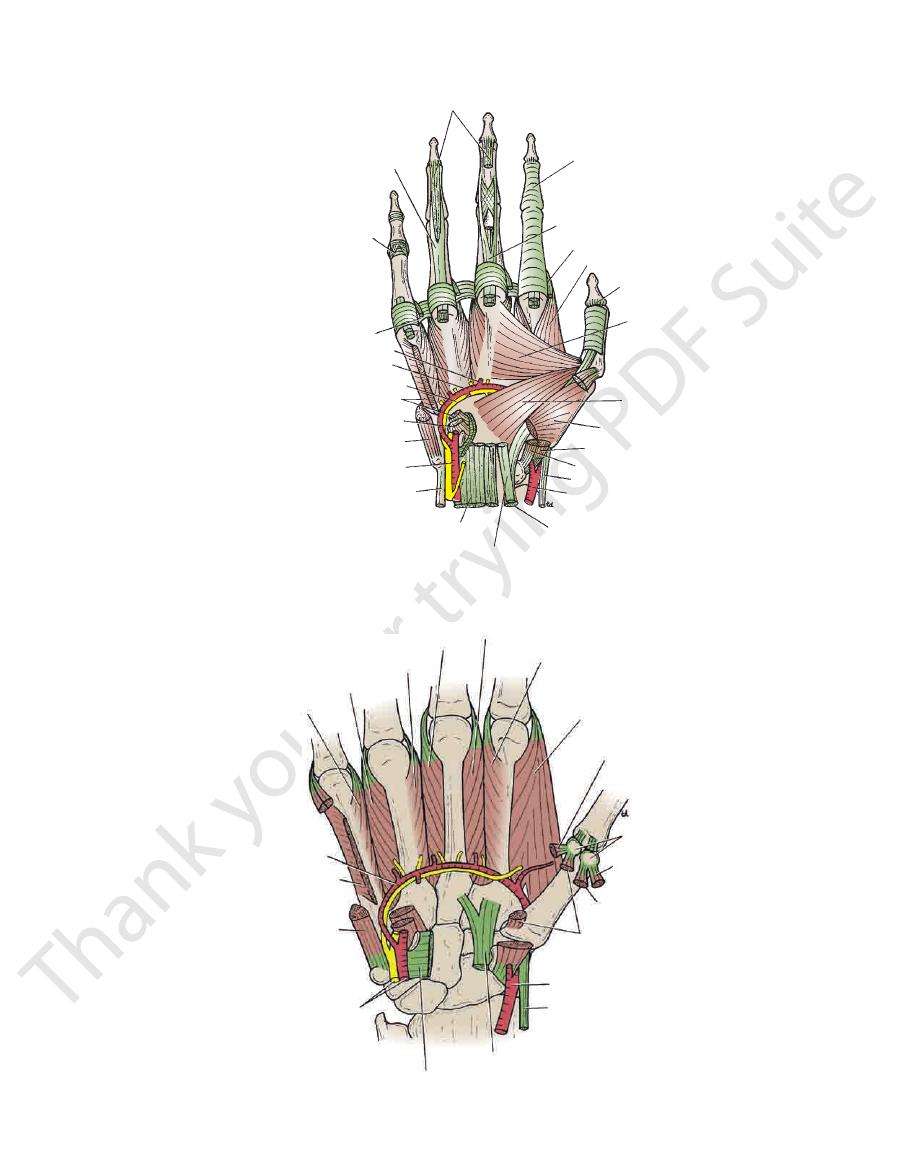
FIGURE 9.68
Anterior view of the palm of the hand showing the deep palmar arch and the deep terminal branch of the ulnar
nerve. The interossei are also shown.
flexor digitorum profundus
flexor digitorum superficialis
palmar ligament of joint
deep transverse palmar ligament
palmar metacarpal artery
deep palmar arch
deep branch of ulnar nerve
opponens digiti minimi
flexor digiti minimi
abductor digiti minimi
ulnar artery and nerve
flexor carpi ulnaris
flexor digitorum profundus
flexor carpi radialis
flexor pollicis longus
radial artery
abductor pollicis longus
opponens pollicis
oblique head of
adductor pollicis
transverse head of
adductor pollicis
flexor pollicis longus
first dorsal interosseous
first lumbrical
flexor digitorum superficialis
fibrous flexor sheath
flexor pollicis brevis
abductor pollicis brevis
FIGURE 9.67
xor tendons have been removed from the palm, but their
Anterior view of the palm of the hand. The long fle
method of insertion into the fingers is shown.
402
CHAPTER 9
The Upper Limb
interosseous
extensor digitorum
palmar interossei
dorsal interossei
FIGURE 9.69
Origins and insertion of the palmar and the
also shown.
dorsal interossei muscles. The actions of these muscles are
Small Muscles of the Hand
T A B L E 9 . 9
radial artery to complete the deep palmar arch (Figs. 9.67
digiti minimi and the flexor digiti minimi, and joins the
of the flexor retinaculum, passes between the abductor
arises in front
deep branch of the ulnar artery
The
and pass to the fingers (Fig. 9.62).
arise from the convexity of the arch
digital arteries
Four
of the fully extended thumb.
of the arch lies across the palm, level with the distal border
side by one of the branches of the radial artery. The curve
long flexor tendons. The arch is completed on the lateral
laterally behind the palmar aponeurosis and in front of the
the ulnar artery (Fig. 9.62). On entering the palm, it curves
is a direct continuation of
superficial palmar arch
The
palmar arch.
branch and then continues into the palm as the superficial
the pisiform bone (Fig. 9.62). The artery gives off a deep
retinaculum on the lateral side of the ulnar nerve and
The ulnar artery enters the hand anterior to the flexor
Ulnar Artery
acarpal bone forward and cupping the palm.
carpal joint of the little finger, thereby pulling the fifth met
it assists the flexor digiti minimi in flexing the carpometa
expansion of each
dorsal extensor
little fingers and
index, ring, and
of thumb and
Proximal phalanges
Tendons of flexor
Muscle
Origin
Insertion
Nerve Supply
Nerve Roots
a
Action
Palmaris brevis
Flexor retinaculum,
palmar
aponeurosis
Skin of palm
Superficial branch
of ulnar nerve
C8; T1
Corrugates skin to
improve grip of palm
Lumbricals (4)
digitorum
profundus
Extensor expansion
of medial four
fingers
1st and 2nd,
(i.e., lateral two)
median nerve;
3rd and 4th
deep branch of
ulnar nerve
C8; T1
Flex
metacarpophalangeal
joints and extend
interphalangeal joints
of fingers except
thumb
Interossei (8)
Palmar (4)
First arises from base
of 1st metacarpal;
remaining three
from anterior
surface of shafts
of 2nd, 4th, and 5th
metacarpals
finger (Fig. 9.69)
Deep branch of
ulnar nerve
C8; T1
Palmar interossei adduct
fingers toward center
of third finger
Dorsal (4)
Contiguous sides
of shafts of
metacarpal bones
Proximal phalanges
of index,
middle, and
ring fingers and
dorsal extensor
expansion
(Fig. 9.69)
Deep branch of
ulnar nerve
C8; T1
Dorsal interossei abduct
fingers from center
of third finger; both
palmar and dorsal flex
metacarpophalangeal
joints and extend
interphalangeal joints
(continued)
-
-
Arteries of the Palm
and 9.68).

Basic Anatomy
lateral axillary nodes.
drain into the
and some
infraclavicular nodes,
vein; they drain into the
the hand ascends in vessels that accompany the cephalic
The lymph from the lateral side of
lateral axillary nodes.
and then ascend to drain into the
supratrochlear nodes
vessels that accompany the basilic vein; they drain into the
The lymph from the medial side of the hand ascends in
on the dorsum of the hand.
or pass around the medial and lateral borders to join vessels
that is drained by vessels that ascend in front of the forearm
sum of the hand. Lymph vessels on the palm form a plexus
reach the webs. From here, the vessels ascend onto the dor
The lymph vessels of the fingers pass along their borders to
Lymph Drainage of the Palm
ing corresponding tributaries.
nied by superficial and deep palmar venous arches, receiv
Superficial and deep palmar arterial arches are accompa
Veins of the Palm
sides of the thumb.
which divides into two and supplies the lateral and medial
arteria princeps pollicis,
side of the index finger, and the
which supplies the lateral
arteria radialis indicis,
off the
Immediately on entering the palm, the radial artery gives
Branches of the Radial Artery in the Palm
mar arch.
inferiorly, to join the digital branches of the superficial pal
take part in the anastomosis around the wrist joint, and
The deep palmar arch sends branches superiorly, which
the extended thumb.
curve of the arch lies at a level with the proximal border of
the medial side by the deep branch of the ulnar artery. The
and the interosseous muscles. The arch is completed on
long flexor tendons and in front of the metacarpal bones
radial artery (Fig. 9.68). It curves medially beneath the
is a direct continuation of the
deep palmar arch
The
arch (Figs. 9.67 and 9.68).
of the adductor pollicis and continues as the deep palmar
it curves medially between the oblique and transverse heads
interosseous muscle (see page 406). On entering the palm,
ond metacarpal bones and the two heads of the first dorsal
ing forward between the proximal ends of the first and sec
The radial artery leaves the dorsum of the hand by turn
Radial Artery
403
-
-
-
-
-
-
Small Muscles of the Hand (continued)
T A B L E 9 . 9
Muscle
Origin
Insertion
Nerve Supply
Nerve Roots
a
Action
Short Muscles of Thumb
Abductor pollicis
brevis
Scaphoid, trapezium,
flexor retinaculum
Base of proximal
phalanx of thumb
Median nerve
C8; T1
Abduction of thumb
Flexor pollicis
brevis
Flexor retinaculum
Base of proximal
phalanx of thumb
Median nerve
C8; T1
Flexes
metacarpophalangeal
joint of thumb
Opponens
pollicis
Flexor retinaculum
Shaft of metacarpal
bone of thumb
Median nerve
C8; T1
Pulls thumb medially and
forward across palm
Adductor pollicis
Oblique head; 2nd
and 3rd metacarpal
bones; transverse
head; 3rd
metacarpal bone
Base of proximal
phalanx of thumb
Deep branch of
ulnar nerve
C8; T1
Adduction of thumb
Short Muscles of Little Finger
Abductor digiti
minimi
Pisiform bone
Base of proximal
phalanx of little
finger
Deep branch of
ulnar nerve
C8; T1
Abducts little finger
Flexor digiti
minimi
Flexor retinaculum
Base of proximal
phalanx of little
finger
Deep branch of
ulnar nerve
C8; T1
Flexes little finger
Opponens digiti
minimi
Flexor retinaculum
Medial border fifth
metacarpal bone
Deep branch of
ulnar nerve
C8; T1
Pulls 5th metacarpal
forward as in cupping
the palm
a
The predominant nerve root supply is indicated by boldface type.
404
CHAPTER 9
of the
palmar cutaneous branch
Note also that the
plies the second lumbrical muscle.
dorsal aspect of each finger. One of these branches also sup
the lateral three and a half fingers and the distal half of the
supply the palmar aspect of
cutaneous branches
The
pollicis) and the 1st lumbrical muscle.
pollicis brevis, the flexor pollicis brevis, and the opponens
supplies the muscles of the thenar eminence (the abductor
one fingerbreadth distal to the tubercle of the scaphoid; it
the lower border of the flexor retinaculum and lies about
takes a recurrent course around
muscular branch
The
immediately divides into lateral and medial branches.
It
carpal tunnel.
the flexor retinaculum and through the
behind
The median nerve enters the palm by passing
Median Nerve
The Upper Limb
Nerves of the Palm
-
median nerve given off in the front of the forearm (Fig. 9.55)
one of the palmar spaces.
with connective tissue. Proximally, it is continuous with
the tendon of each lumbrical muscle and is normally filled
is a potential space surrounding
lumbrical canal
The
bones (Fig. 9.70).
of the interossei and the third, fourth, and fifth metacarpal
dons to the middle, ring, and little fingers. It lies in front
lumbrical muscles and lies posterior to the long flexor ten
contains the 2nd, 3rd, and 4th
midpalmar space
The
(Fig. 9.70).
index finger and in front of the adductor pollicis muscle
cle and lies posterior to the long flexor tendons to the
contains the first lumbrical mus
thenar space
The
canals (Fig. 9.70).
two spaces are continuous with the appropriate lumbrical
forearm by the walls of the carpal tunnel. Distally, the
the thenar and midpalmar spaces are closed off from the
which lies medial to the septum (Fig. 9.70). Proximally,
midpalmar space,
taining the thenar muscles), and the
must not be confused with the fascial compartment con
which lies lateral to the septum (and
thenar space,
middle fingers. This second septum divides the palm into
passes between the long flexor tendons of the index and
the third metacarpal bone (Fig. 9.70). Usually, the septum
tum passes obliquely backward to the anterior border of
border of the palmar aponeurosis, a second fibrous sep
compartment is unimportant clinically. From the lateral
partment containing the three hypothenar muscles; this
bone (Fig. 9.70). Medial to this septum is a fascial com
is attached to the anterior border of the 5th metacarpal
its medial border, a fibrous septum passes backward and
lower border of the flexor retinaculum (Fig. 9.55). From
The triangular palmar aponeurosis fans out from the
infection in the palm.
important clinically because they may limit the spread of
filled with loose connective tissue. Their boundaries are
Normally, the fascial spaces of the palm are potential spaces
medial part of the palm (Fig. 9.38).
retinaculum (Fig. 9.54) and supplies the skin over the
to the flexor
anterior
off in the front of the forearm crosses
of the ulnar nerve given
palmar cutaneous branch
The
licis muscle.
4th lumbrical muscles, and both heads of the adductor pol
It supplies all the palmar and dorsal interossei, the 3rd and
the flexor digiti minimi, and the opponens digiti minimi.
hypothenar eminence, namely, the abductor digiti minimi,
to the three muscles of the
muscular branches
It gives off
front of the metacarpal bones and interosseous muscles.
arch. The nerve lies behind the long flexor tendons and in
passes laterally within the concavity of the deep palmar
around the lower border of the hook of the hamate, and
(Fig. 9.67). It pierces the opponens digiti minimi, winds
the abductor digiti minimi and the flexor digiti minimi
The deep branch of the ulnar nerve runs backward between
Deep Branch of the Ulnar Nerve
finger.
It also supplies the distal half of the dorsal aspect of each
the adjacent sides of the little and ring fingers (Fig. 9.62).
the palmar aspect of the medial side of the little finger and
to
cutaneous branches
to the palmaris brevis and
branch
muscular
The nerve gives off the following branches: a
and symptoms.
may be compressed at this site, giving rise to clinical signs
the superficial part of the flexor retinaculum. The nerve
created by fibrous tissue derived from
tunnel of Guyon,
nerve and artery may lie in a fibro-osseous tunnel, the
and 9.62). The ulnar artery is on its lateral side. Here, the
pisiform bone and the hook of the hamate (Figs. 9.55
the palm, lying in the subcutaneous tissue between the
The superficial branch of the ulnar nerve descends into
Superficial Branch of the Ulnar Nerve
divides into a superficial and a deep terminal branch.
bone (Figs. 9.55 and 9.62). As it crosses the retinaculum, it
retinaculum alongside the lateral border of the pisiform
to the flexor
anterior
The ulnar nerve enters the palm
Ulnar Nerve
skin over the lateral part of the palm (Fig. 9.38).
to the flexor retinaculum and supplies the
anterior
crosses
-
Fascial Spaces of the Palm
-
-
the
-
-
-
Fascial Spaces of the Palm and Infection
The fascial spaces of the palm (Fig. 9.70) are clinically impor-
tant because they can become infected and distended with
pus as a result of the spread of infection in acute suppura-
tive tenosynovitis; rarely, they can become infected after pen-
etrating wounds such as falling on a dirty nail.
C L I N I C A L N O T E S
Basic Anatomy
405
midpalmar space
lumbrical canals
thenar space
epiphysis
diaphysis
periosteum
pulp space
fibrous septa
deep fascia
digital artery
synovial sheath surrounding tendons of
flexor digitorum superficialis and profundus
medial fibrous septum
muscles of hypothenar eminence
interossei
midpalmar space
oblique fibrous septum
transverse head of adductor pollicis
long flexor tendons to index finger
thenar space
metacarpal bone
lateral fibrous septum
muscles of thenar eminence
synovial sheath surrounding flexor pollicis longus
palmar aponeurosis
FIGURE 9.70
Palmar and pulp fascial spaces.
periosteum of the terminal phalanx just distal to the
The deep fascia of the pulp of each finger fuses with the
Pulp Space of the Fingers
insertion of the long flexor tendons and closes off a fascial
Through the pulp space, which is filled with fat, runs
septa, which pass from the deep fascia to the periosteum.
pulp space is subdivided by the presence of numerous
(Fig. 9.70). Each
pulp space
compartment known as the
the terminal branch of the digital artery that supplies
the diaphysis of the terminal phalanx. The epiphysis of
the distal phalanx receives its blood supply proximal to
the pulp space.
Pulp-Space Infection (Felon)
ally introduced into the space by pinpricks or sewing needles.
most often in the thumb and index finger. Bacteria are usu
Infection of such a space is common and serious, occurring
situated in front of the terminal phalanx of each finger (Fig. 9.70).
The pulp space of the fingers is a closed fascial compartment
-
C L I N I C A L N O T E S
Because each space is subdivided into numerous smaller com
ulnar nerve.
radial nerve and the posterior cutaneous branch of the
of the hand is derived from the superficial branch of the
to the skin on the dorsum
sensory nerve supply
The
mobile on the underlying tendons and bones.
The skin on the dorsum of the hand is thin, hairy, and freely
proximally located epiphysis of this bone is saved because it
the blood vessels could result in necrosis of the diaphysis. The
of the phalanx passes through the pulp space, and pressure on
phalanx can occur. In children, the blood supply to the diaphysis
infection is left without decompression, infection of the terminal
causes the pressure in the pulp space to quickly rise. If the
mulation of inflammatory exudate within these compartments
-
partments by fibrous septa, it is easily understood that the accu-
receives its arterial supply just proximal to the pulp space.
The close relationship of the proximal end of the pulp
space to the digital synovial sheath accounts for the involve-
ment of the sheath in the infectious process when the pulp-
space infection has been neglected.
The Dorsum of the Hand
Skin
406
CHAPTER 9
supplies the medial third of the dorsum of the hand
tendon, descends over the extensor retinaculum, and
winds around the ulna deep to the flexor carpi ulnaris
posterior cutaneous branch of the ulnar nerve
The
finger.
the ulnar nerve, also supplies the lateral side of the ring
variation. Frequently, a dorsal digital nerve, a branch of
hand and fingers supplied by the radial nerve is subject to
side of the ring finger. The area of skin on the back of the
the thumb, the index and middle fingers, and the lateral
It divides into several dorsal digital nerves that supply
lateral two thirds of the dorsum of the hand (Fig. 9.38).
descends over the extensor retinaculum, and supplies the
around the radius deep to the brachioradialis tendon,
winds
superficial branch of the radial nerve
The
The Upper Limb
(Fig. 9.38). It divides into several dorsal digital nerves
cal muscle on the lateral side (Fig. 9.63).
side and farther distally receives the tendon of the lumbri
insertion of the corresponding interosseous muscle on each
The dorsal extensor expansion receives the tendon of
(Fig. 9.63).
verge to be inserted into the base of the distal phalanx
which con
two lateral parts,
the middle phalanx, and
which is inserted into the base of
central part,
parts: a
phalangeal joint, the extensor expansion splits into three
(Figs. 9.56 and 9.57). Near the proximal inter
expansion
extensor
tendon joins the fascial expansion called the
On the posterior surface of each finger, the extensor
digiti minimi (Fig. 9.55).
joined on its medial side by the two tendons of the extensor
of the extensor indicis, and the tendon to the little finger is
to the index finger is joined on its medial side by the tendon
proximal to the heads of the metacarpal bones. The tendon
connect the tendons to the little, ring, and middle fingers,
of the dorsum of the hand. Strong oblique fibrous bands
which occupies the whole width
subfascial space,
roof of a
embedded in the deep fascia, and together they form the
sum of the hand (Figs. 9.56 and 9.57). The tendons are
under the extensor retinaculum and fan out over the dor
The four tendons of the extensor digitorum emerge from
Insertion of the Long Extensor Tendons
seous spaces.
cates with the deep veins of the palm through the interos
arch, which receives digital veins and freely communi
part of the blood from the whole hand drains into the
medial side, into the basilic vein (Fig. 9.100). The greater
on the lateral side into the cephalic vein and, on the
proximal to the metacarpophalangeal joints and drains
The dorsal venous arch lies in the subcutaneous tissue
Dorsal Venous Arch (or Network)
supply from palmar digital nerves.
remainder of the dorsum of each finger receives its nerve
nerves do not extend far beyond the proximal phalanx. The
The dorsal digital branches of the radial and ulnar
the little fingers.
that supply the medial side of the ring and the sides of
-
-
-
-
-
-
Mallet Finger
flexed when the extensor tendon is taut. The last 20° of active
Avulsion of the insertion of one of the extensor tendons into
the distal phalanges can occur if the distal phalanx is forcibly
extension is lost, resulting in a condition known as mallet
finger
extension of the distal interphalangeal joint. This injury can
to its insertion into the base of the middle phalanx results in
(Fig. 9.71).
Boutonnière Deformity
Avulsion of the central slip of the extensor tendon proximal
a characteristic deformity (Fig. 9.71C). The deformity results
from flexing of the proximal interphalangeal joint and hyper-
result from direct end-on trauma to the finger, direct trauma
over the back of the proximal interphalangeal joint, or lacera-
tion of the dorsum of the finger.
C L I N I C A L N O T E S
The Radial Artery on the Dorsum
ligament of the joint (Fig. 9.65). On reaching the dorsum
longus and extensor pollicis brevis, and lies on the lateral
wrist joint, beneath the tendons of the abductor pollicis
The radial artery winds around the lateral margin of the
of the Hand
of the hand, the artery descends beneath the
n of
tendo
the extensor pollicis longus to reach the
al between
interv
the
two heads of the first dorsal interosseous
re,
muscle; he
the margins of the olecranon fossa of the humerus and
, it is attached above to
Posteriorly
head of the radius.
ulna and to the anular ligament, which surrounds the
and below to the margin of the coronoid process of the
sae and to the front of the medial and lateral epicondyles
along the upper margins of the coronoid and radial fos
, it is attached above to the humerus
Capsule: Anteriorly
Synovial hinge joint
Type:
surfaces are covered with hyaline cartilage.
ulna and the head of the radius (Fig. 9.72). The articular
capitulum of the humerus and the trochlear notch of the
This occurs between the trochlea and
Articulation:
and the shoulder joint are fully described on pages 362
The sternoclavicular joint, the acromioclavicular joint,
(Fig. 9.65).
Dorsal digital arteries pass to the thumb and index finger
take part in the anastomosis around the wrist joint.
Branches of the radial artery on the dorsum of the
(see page 403).
the artery turns forward to enter the palm of the hand
hand
Joints of the Upper Limb
and 364.
Elbow Joint
■
■
■
■
■
■
-