C H A P T E R O U T L I N E
(continued)
Common Peroneal Nerve 479
Posterior Cutaneous Nerve of the
Thigh 479
Obturator Nerve 479
Fascial Compartments of the Leg 479
Interosseous Membrane 479
Retinacula of the Ankle 479
The Front of the Leg 481
Skin 481
Contents of the Anterior Fascial
Compartment of the Leg 481
Contents of the Lateral Fascial
Compartment of the Leg 486
The Back of the Leg 487
Skin 487
Contents of the Posterior Fascial
Compartment of the Leg 487
The Region of the Ankle 490
Anterior Aspect of the Ankle 490
Posterior Aspect of the Ankle 490
The Foot 490
The Sole of the Foot 490
The Dorsum of the Foot 498
Joints of the Lower Limb 500
Knee Joint 500
Proximal Tibiofibular Joint 504
Distal Tibiofibular Joint 504
Ankle Joint 505
Tarsal Joints 507
Tarsometatarsal and Intermetatarsal
Joints 508
Metatarsophalangeal and
Interphalangeal Joints 508
The Foot as a Functional Unit 508
The Foot as a Weight Bearer
and a Lever 508
Radiographic Anatomy 512
Radiographic Appearances of the Lower
Limb 512
Surface Anatomy 512
Gluteal Region 513
Inguinal Region 513
Femoral Triangle 520
Adductor Canal 520
Knee Region 520
Tibia 521
Ankle Region and Foot 521
C H A P T E R O B J E C T I V E S
The basic anatomy of the vascular supply, lymphatic drainage,
is given. Emphasis is placed on the functions of the muscles, and
A general description of the bones, joints, and actions of muscles
surgery, or an emergency department.
■
■
Lower limb problems are some of the most common dealt with
by health professionals, whether working in general practice,
■
■
Arthritis, varicose veins, vascular deficiencies, fractures,
dislocations, sprains, lacerations, knee effusions, leg pain,
ankle injuries, and peripheral nerve injuries are just a few of the
conditions that physicians see.
■
■
The anatomy of the lower limb is discussed in relation to com-
mon clinical conditions.
■
■
only the briefest coverage of their attachments is provided.
■
■
and distribution of the nerves is reviewed.
natomy
asic
B
a
The primary function of the lower limbs is to support the
nerves (anterior rami).
branches of the iliohypogastric (L1) and 12th thoracic
The upper lateral quadrant is supplied by the lateral
three sacral nerves.
rami of the upper three lumbar nerves and the upper
The upper medial quadrant is supplied by the posterior
posterior and anterior rami of spinal nerves, as follows:
(Figs. 10.1 and 10.2) are derived from
cutaneous nerves
The
layer of superficial fascia.
region is largely made up of the gluteal muscles and a thick
the iliac crest and inferiorly by the fold of the buttock. The
The gluteal region, or buttock, is bounded superiorly by
its own distinct nerve and blood supply.
having its own muscles that perform group functions and
and the leg are compartmentalized, each compartment
thigh, the knee, the leg, the ankle, and the foot. The thigh
The lower limbs are divided into the gluteal region, the
stable and can bear the weight of the body.
each other at the symphysis pubis, the lower limbs are very
the trunk at the strong sacroiliac joints and anteriorly with
Because the two hip bones articulate posteriorly with
ized for locomotion.
standing, walking, and running; they have become special
weight of the body and to provide a stable foundation in
-
Organization of the Lower Limb
The Gluteal Region
The Skin of the Buttock
■
■
■
■
Basic Anatomy
437
posterior rami of
upper three
lumbar nerves
posterior rami of
upper three
sacral nerves
sural nerve
branches of
saphenous nerve
medial calcaneal
nerve
medial plantar
nerve
lateral plantar
nerve
sural nerve
sural communicating
branch of common
peroneal nerve
posterior cutaneous
nerve of thigh
branches of lateral
cutaneous nerve
of thigh
branches of
posterior cutaneous
nerve of thigh
branches of lateral
cutaneous nerve
of thigh
lateral branches of
iliohypogastric (LI) nerve
lateral branch of
12th thoracic nerve
lateral cutaneous
nerve of calf
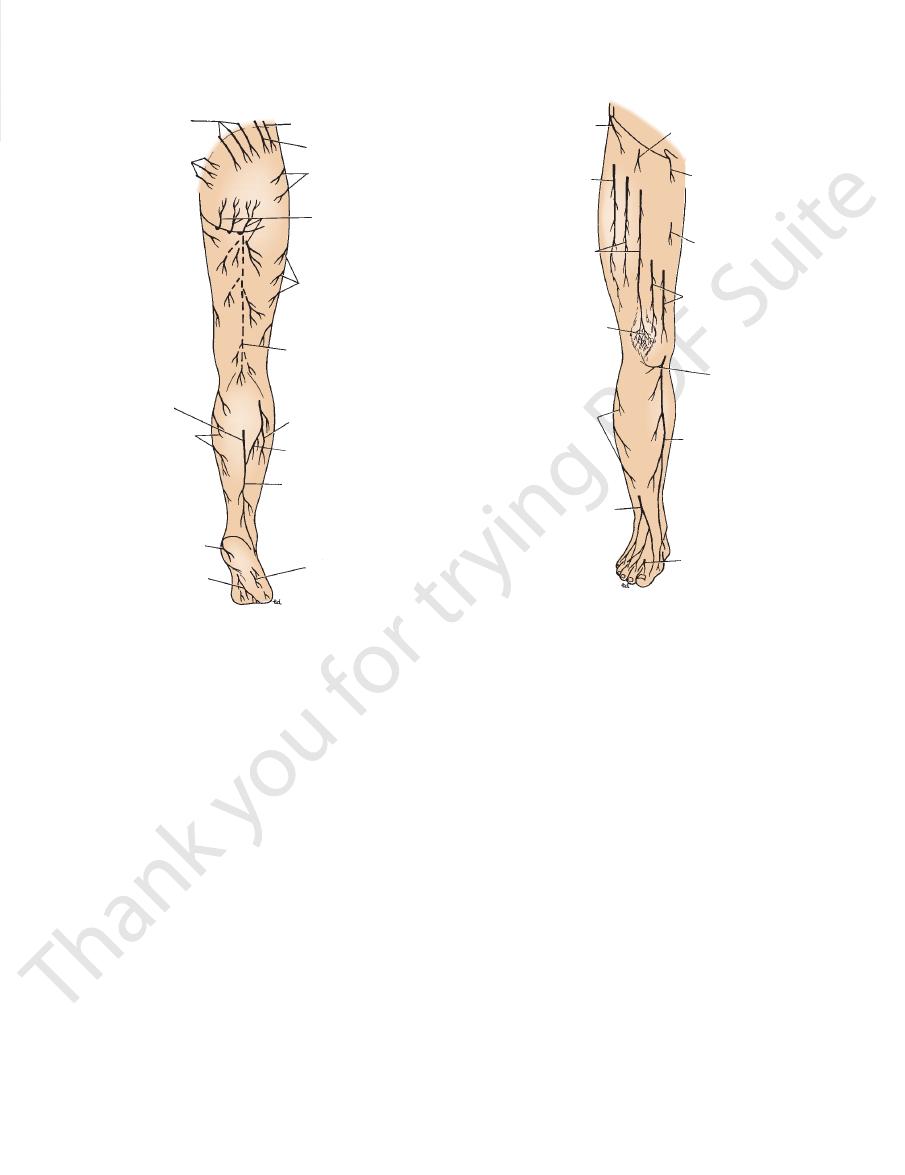
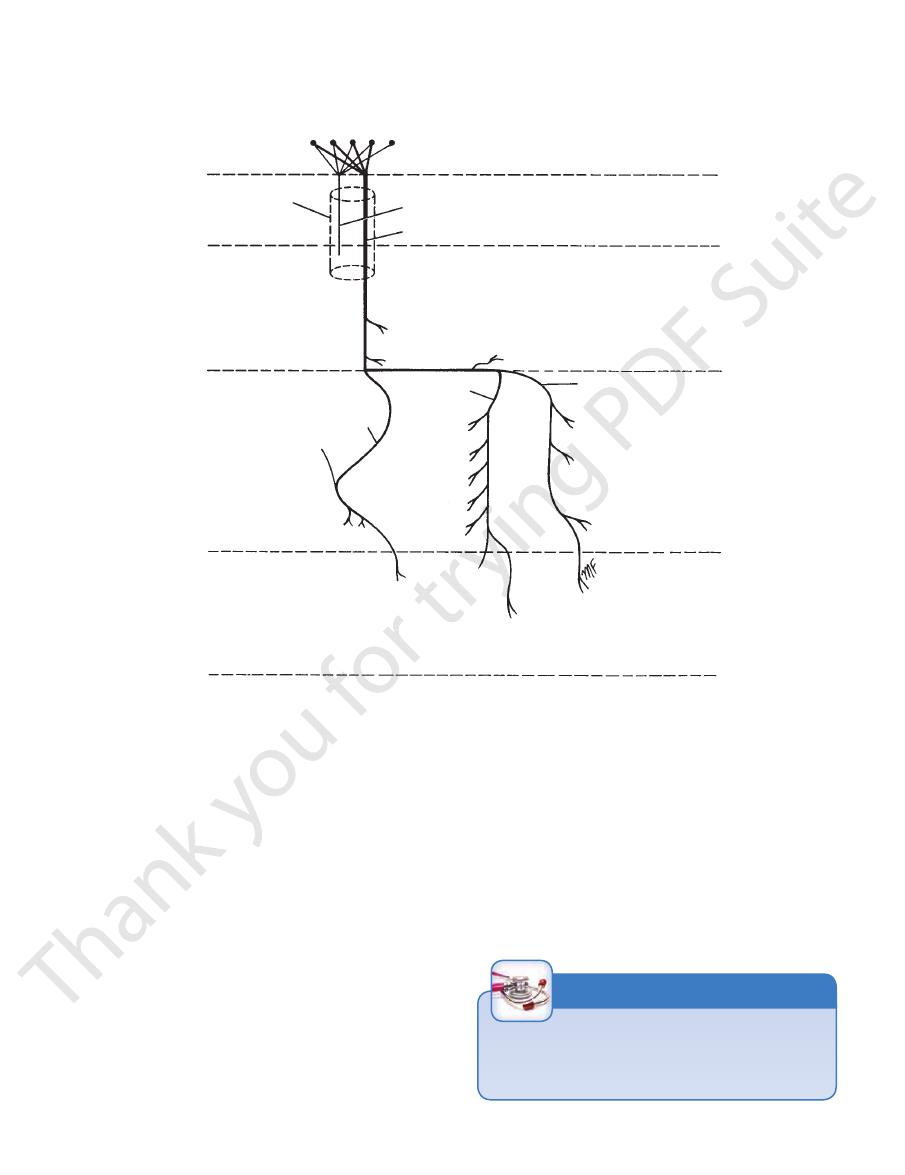
FIGURE 10.1
Cutaneous nerves of the posterior surface of
the right lower limb.
lateral cutaneous
branch of 12th
thoracic nerve
lateral cutaneous
nerve of thigh
intermediate
cutaneous nerve
of thigh
patellar plexus
of nerves
lateral sural
cutaneous nerve
superficial peroneal
nerve
deep peroneal
nerve
saphenous nerve
infrapatellar branch
of saphenous nerve
medial cutaneous
nerve of thigh
obturator nerve
ilioinguinal nerve
femoral branch of
genitofemoral nerve
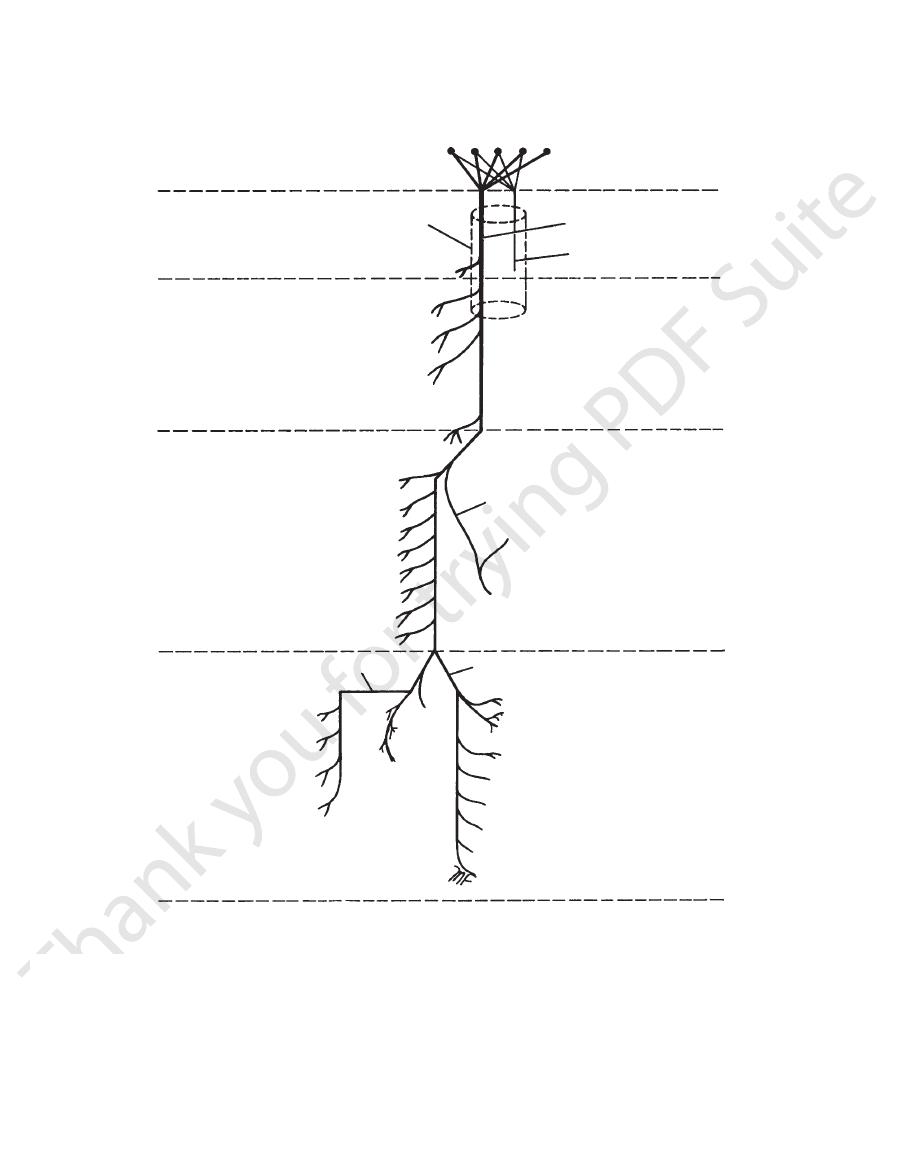
FIGURE 10.2
Cutaneous nerves of the anterior surface of
gluteus maximus.
muscle and receives the greater part of the insertion of the
The iliotibial tract forms a sheath for the tensor fasciae latae
the iliac crest and below to the lateral condyle of the tibia.
(Fig. 10.6). This is attached above to the tubercle of
tract
iliotibial
cia is thickened to form a strong, wide band, the
to the iliac crest. On the lateral surface of the thigh, the fas
ers the outer surface of the gluteus medius and is attached
the gluteus maximus, it continues as a single layer that cov
to enclose the gluteus maximus muscle (Fig. 10.5). Above
of the thigh. In the gluteal region, it splits
or
deep fas
is continuous below with the
deep fascia
The
the prominence of the buttock.
impregnated with large quantities of fat. It contributes to
is thick, especially in women, and is
superficial fascia
The
superficial inguinal nodes (Figs. 10.3 and 10.4).
drain into the lateral group of the
lymph vessels
The
sacral and coccygeal nerves.
the buttocks is supplied by small branches of the lower
The skin over the coccyx in the floor of the cleft between
anterior rami).
the posterior cutaneous nerve of the thigh (S1, 2, and 3,
The lower medial quadrant is supplied by branches from
rior rami).
the lateral cutaneous nerve of the thigh (L2 and 3, ante
The lower lateral quadrant is supplied by branches from
the right lower limb.
■
■
-
■
■
Fascia of the Buttock
-
cia,
fascia lata,
-
-
Bones of the Gluteal Region
Hip Bone
The ilium, ischium, and pubis form the hip bone (Figs. 10.7
posterior
a similar prominence, the
inferior iliac spine;
anterior
anterior superior iliac spine is a prominence, the
2 in. (5 cm) behind the anterior superior spine. Below the
lies about
iliac tubercle
The
terior superior iliac spine.
pos
and behind at the
anterior superior iliac spine
through the skin along its entire length; it ends in front at
(Fig. 10.8). This can be felt
iliac crest
bone, possesses the
which is the upper flattened part of the
ilium,
The
the hip bone in the gluteal region are as follows.
The important features found on the outer surface of
bony pelvis is considered on page 241.
pubis. The detailed structure of the internal aspect of the
articulate with one another anteriorly at the symphysis
and form the anterolateral walls of the pelvis; they also
hip bones articulate with the sacrum at the sacroiliac joints
and 10.8). They meet one another at the acetabulum. The
the
-
438
CHAPTER 10
The Lower Limb
deep fascia
of thigh
(fascia lata)
femoral
sheath
femoral vein
femoral artery
saphenous
opening
falciform
margin
great saphenous
vein
attachment of membranous
layer of superficial fascia
horizontal group of
superficial inguinal
lymph nodes
femoral artery
vertical group of superficial inguinal lymph nodes
great saphenous
vein
superficial external
pudendal vessels
superficial epigastric vessels
superficial circumflex iliac vessels
A
B
inguinal ligament
fascia
h
a lata)
ral
h
ein
tery
nous
ng
orm
gin
great saphenous
attachment of membranous
layer of superficial fascia
horizontal group of
superficial inguinal
lymph nodes
femoral artery
gg
ve
v
u
su
u
pu
g
superficial epi
x
superficial circumflex
inguinal ligament
inguinal ligament
femoral canal
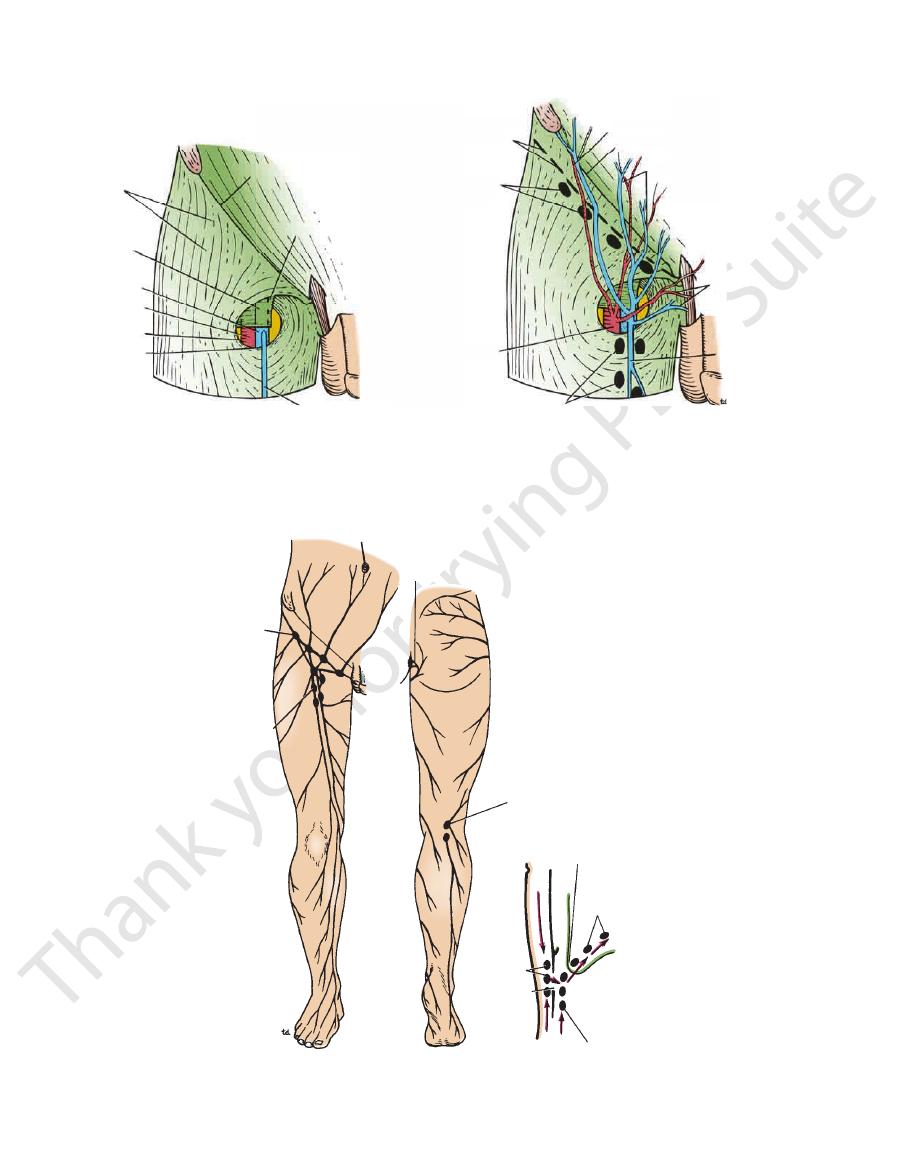
FIGURE 10.3
A, B.
superficial fascia to the deep fascia, about a fingerbreadth below the inguinal ligament.
in the deep fascia and its relationship to the femoral sheath. Note also the line of attachment of the membranous layer of
Superficial veins, arteries, and lymph nodes over the right femoral triangle. Note the saphenous opening
umbilicus
lymph from lower half
of anal canal
iliac crest
popliteal lymph nodes
femoral canal
external iliac nodes
deep inguinal nodes
saphenous
opening
vertical group of
superficial
inguinal
lymph nodes
horizontal group
of superficial
inguinal
lymph nodes
superficial
inguinal
nodes
FIGURE 10.4
Lymph drainage for the superficial tissues of the right lower limb and the abdominal walls below the level of
the femoral canal.
ous opening in the deep fascia. Note also that all lymph from these nodes ultimately drains into the external iliac nodes via
the umbilicus. Note the arrangement of the superficial and deep inguinal lymph nodes and their relationship to the saphen-
Basic Anatomy
(Fig. 10.8).
acetabular fossa
called the
cartilage. The floor of the acetabulum is nonarticular and is
ited to a horseshoe-shaped area and is covered with hyaline
(Fig. 10.8). The articular surface of the acetabulum is lim
acetabular notch
ulum is deficient and is marked by the
(Figs. 10.8 and 10.9). The inferior margin of the acetab
almost spherical head of the femur to form the hip joint
which articulates with the
acetabulum,
sion, called the
On the outer surface of the hip bone is a deep depres
(Figs. 10.7 and 10.8).
pubic tubercle
ends laterally as the
forms the upper border of the body of the pubis, and it
pubic crest
(see page 245). The
obturator membrane
The obturator foramen in life is filled in by
tor foramen.
obtura
inferior ramus joins the ischial ramus below the
joins the ilium and ischium at the acetabulum, and the
the superior ramus
symphysis pubis;
line anteriorly at the
the two pubic bones articulate with each other in the mid
(Fig. 10.8). The bodies of
inferior ramus
ramus,
superior
body,
can be divided into a
The
sacrospinous and sacrotuberous ligaments (see page 245).
by the presence of the
lesser sciatic foramina
greater
The greater and lesser sciatic notches are converted into
posterior aspect of the lower part of the body of the bone.
forms the
ischial tuberosity
The
lesser sciatic notches.
greater
border of the ischium and intervenes between the
projects from the posterior
ischial spine
10.7 and 10.8). The
(Figs.
ramus
and a lower thinner part, the
body,
part, the
is L shaped, possessing an upper thicker
ischium
The
(Figs. 10.7
greater sciatic notch
possesses a large notch, the
iliac spine. Above and behind the acetabulum, the ilium
is located below the posterior superior
inferior iliac spine,
439
and 10.8).
and
and
pubis
a
and an
-
-
the
-
-
-
In the anatomic position, the front of the
sis
symphy
femur are shown in Figures 10.10 and 10.11.
The important muscles and ligaments attached to the
medial epicondyle.
10.11). The adductor tubercle is continuous with the
(Fig.
lateral epicondyles
medial
condyles are the
take part in the formation of the knee joint. Above the
by an articular surface for the patella. The two condyles
The anterior surfaces of the condyles are joined
notch.
intercondylar
condyles, separated posteriorly by the
medial
lateral
The lower end of the femur has
(Fig. 10.11).
popliteal surface
area on its posterior surface called the
broader toward its distal end and forms a flat, triangular
ment of the gluteus maximus muscle. The shaft becomes
for the attach
gluteal tuberosity
greater trochanter is the
On the posterior surface of the shaft below the
lar ridge.
lateral supracondy
becomes continuous below with the
on the medial condyle (Fig. 10.11). The lateral margin
cle
adductor tuber
to the
medial supracondylar ridge
above and below. The medial margin continues below as
muscular septa. The margins of the linea aspera diverge
(Fig. 10.11), to which are attached muscles and inter
linea aspera
anterior surface but posteriorly has a ridge, the
of the femur is smooth and rounded on its
The
(Fig. 10.11).
tubercle
quadrate
posteriorly, on which is the
trochanteric crest
inter
ofemoral ligament is attached, and a prominent
anteriorly, where the ili
intertrochanteric line
are the
(Figs. 10.10 and 10.11). Connecting the two trochanters
nences situated at the junction of the neck and the shaft
are large emi
lesser trochanters
greater
The
axis of the shaft. The size of this angle can be altered by
of about 125° (slightly less in the female) with the long
downward, backward, and laterally and makes an angle
which connects the head to the shaft, passes
neck,
The
ment and enters the bone at the fovea.
femur from the obturator artery is conveyed along this liga
of the head. Part of the blood supply to the head of the
for the attachment of the ligament
fovea capitis,
called the
(Fig. 10.9). In the center of the head is a small depression,
with the acetabulum of the hip bone to form the hip joint
forms about two thirds of a sphere and articulates
head
greater and lesser trochanters (Figs. 10.10 and 10.11). The
The upper end of the femur has a head, a neck, and
form the knee joint.
the hip joint and below with the tibia and the patella to
The femur articulates above with the acetabulum to form
Femur
outer surface of the hip bone are shown in Figure 10.8.
The important muscles and ligaments attached to the
downward.
anterior surface of the sacrum is directed forward and
symphysis pubis faces upward and backward and the
vertical plane. This means that the pelvic surface of the
pubis and the anterior superior iliac spines lie in the same
-
disease.
and
-
-
-
shaft
-
the
-
-
-
and
and
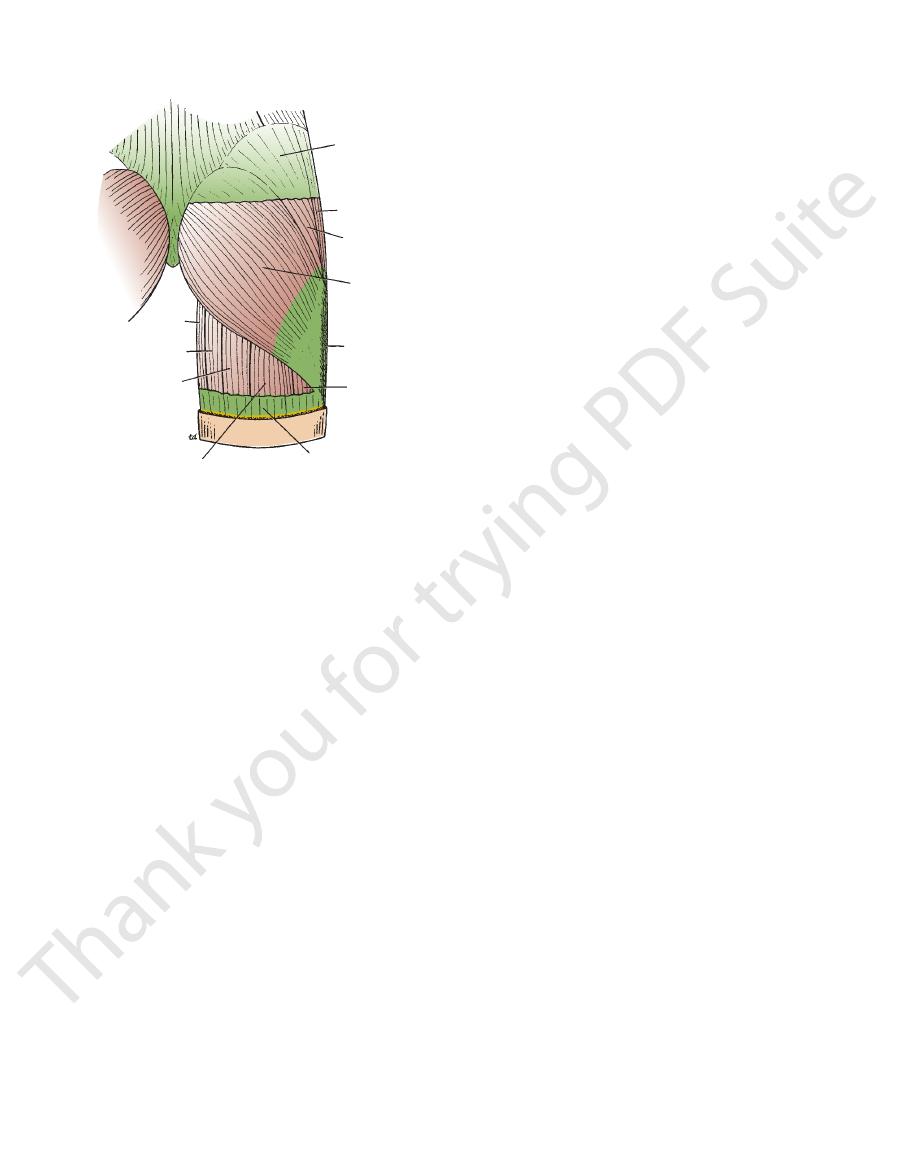
deep fascia
tensor fasciae latae
gluteus medius
iliotibial tract
vastus lateralis
deep fascia (fascia lata)
long head of biceps
semitendinosus
adductor magnus
gracilis
gluteus maximus
FIGURE 10.5
Right gluteus maximus muscle.
440
CHAPTER 10
The Lower Limb
anterior superior iliac spine
lateral cutaneous nerve of thigh
sartorius
femoral nerve
lateral femoral
circumflex artery
intermediate cutaneous nerve
of thigh
nerve to vastus medialis
vastus intermedius
vastus lateralis
vastus medialis
shaft of femur
iliotibial tract
rectus femoris
ligamentum patellae
saphenous nerve
saphenous nerve
femoral artery
gracilis
adductor magnus
adductor longus
medial cutaneous nerve of thigh
pectineus
spermatic cord
deep external pudendal artery
pubic tubercle
inguinal ligament
femoral canal
femoral sheath
femoral vein
psoas
iliacus
profunda femoris artery
tensor fasciae latae
medial femoral
circumflex artery
femoral artery
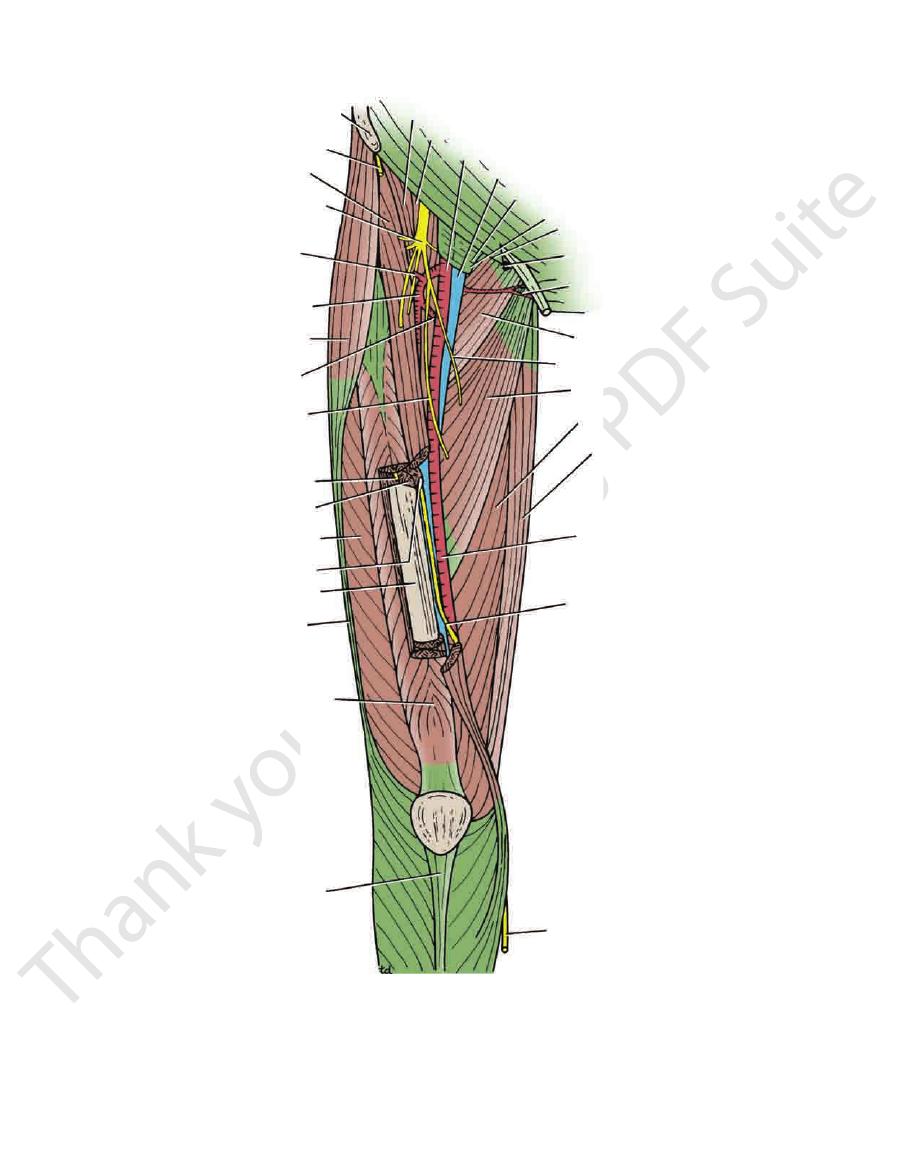
FIGURE 10.6
Femoral triangle and adductor (subsartorial) canal in the right lower limb.
Basic Anatomy
441
iliac crest
rough surface for attachment of
interosseous ligament
posterior superior
iliac spine
auricular surface
posterior inferior iliac spine
greater sciatic notch
ischial spine
lesser sciatic notch
obturator membrane
ischial tuberosity
ischial ramus
inferior ramus of pubis
obturator canal
pubic crest
pubic tubercle
body of pubis
superior ramus
of pubis
iliopectineal line
anterior inferior
iliac spine
anterior superior
iliac spine
iliac fossa
ilium
tubercle of ilium
line of fusion of bones
acetabulum
obturator foramen
ischium
A
B
pubis
posterior superior
iliac spine
auricular surface
posterior inferior iliac spine
greater sciatic notch
ischial spine
lesser sciatic notch
obturator membrane
ischial tuberosity
al
ramus
ne
ferior
or
fossa
ilium
tu
line of fusion of bones
ac
obt
ischium
p
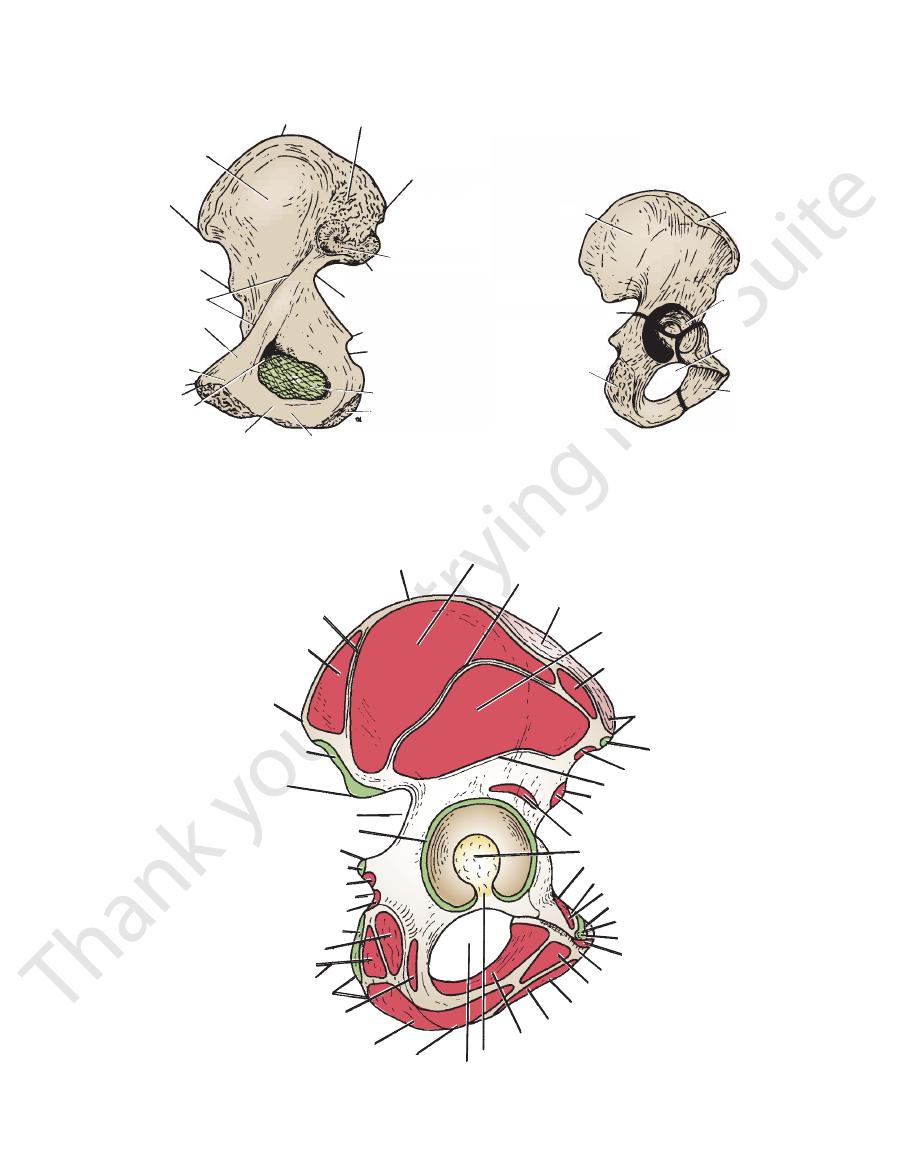
FIGURE 10.7
Medial surface (
(the ilium, the ischium, and the pubis).
) of the right hip bone. Note the lines of fusion between the three bones
) and lateral surface (
A
B
iliac crest
posterior gluteal line
gluteus maximus
posterior inferior
iliac spine
sacrotuberous ligament
posterior superior
iliac spine
greater sciatic notch
capsule
ischial spine
sacrospinous ligament
gemellus superior
lesser sciatic notch
gemellus inferior
sacrotuberous ligament
semimembranosus
semitendinosus
biceps femoris
ischial tuberosity
quadratus femoris
adductor magnus
ramus of ischium
obturator foramen
acetabular notch
obturator externus
gracilis
inferior ramus of pubis
adductor brevis
body of pubis
adductor longus
pubic tubercle
inguinal ligament
pubic crest
pectineus
superior ramus of pubis
pectineal line
acetabular fossa
reflected head of rectus femoris
anterior inferior iliac spine
inferior gluteal line
sartorius
inguinal ligament
anterior superior
iliac spine
tensor fasciae latae
gluteus minimus
iliac tubercle
middle gluteal line
gluteus medius
straight head of rectus femoris
FIGURE 10.8
xternal surface of the right hip bone.
Muscles and ligaments attached to the e
442
CHAPTER 10
The Lower Limb
gluteus maximus
gemellus superior
gemellus inferior
semitendinosus
biceps femoris
adductor magnus
semimembranosus
psoas
iliacus
pectineus
adductor magnus
adductor longus
vastus medialis
vastus lateralis
adductor brevis
vastus intermedius
gluteus maximus
quadratus femoris
obturator externus
gluteus medius
rectus femoris
sartorius
tensor fasciae latae
gluteus minimus
gluteus medius
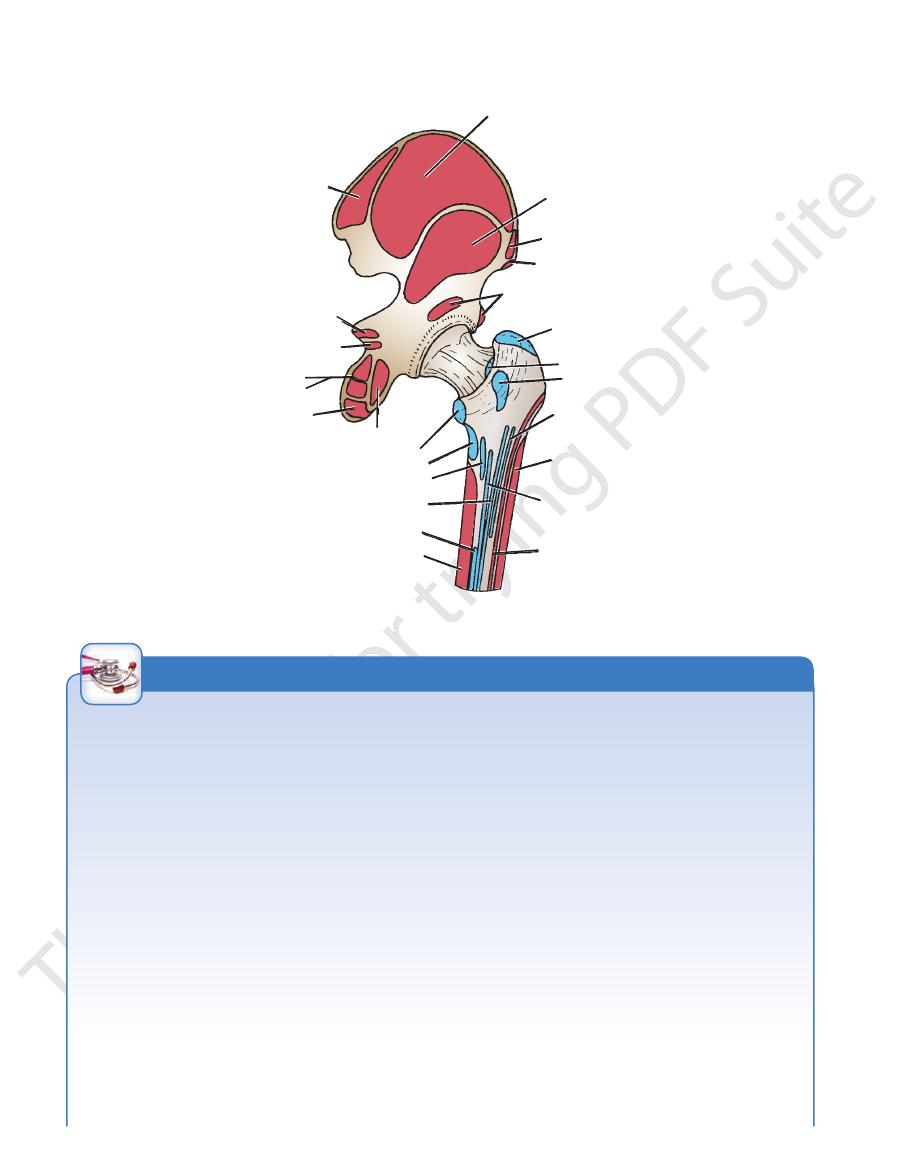
FIGURE 10.9
xternal surface of the right hip bone and the posterior surface of the femur.
Muscles attached to the e
Tenderness of the Head of the Femur and Arthritis of
the Hip Joint
The head of the femur—that is, that part that is not intra-
Fractures of the neck of the femur are common and are of two
of the neck of the femur and in slipping of the femoral epiphysis.
and it occurs in fractures
in this angle is referred to as
The neck of the femur is inclined at an angle with the shaft; the
Fractures of the femoral neck interfere with or completely inter
synovial membrane. As long as the epiphyseal cartilage remains,
explains why avascular necrosis of the head can occur after
just inferior to the inguinal ligament and just lateral to the pulsat
acetabular—can be palpated on the anterior aspect of the thigh
-
ing femoral artery. Tenderness over the head of the femur usu-
ally indicates the presence of arthritis of the hip joint.
Blood Supply to the Femoral Head and Neck
Fractures
Anatomic knowledge of the blood supply to the femoral head
fractures of the neck of the femur. In the young, the epiphysis
of the head is supplied by a small branch of the obturator artery,
which passes to the head along the ligament of the femoral
head. The upper part of the neck of the femur receives a profuse
blood supply from the medial femoral circumflex artery. These
branches pierce the capsule and ascend the neck deep to the
no communication occurs between the two sources of blood. In
the adult, after the epiphyseal cartilage disappears, an anasto-
mosis between the two sources of blood supply is established.
-
rupt the blood supply from the root of the femoral neck to the
femoral head. The scant blood flow along the small artery that
accompanies the round ligament may be insufficient to sustain
the viability of the femoral head, and ischemic necrosis gradually
takes place.
The Neck of the Femur and Coxa Valga and Coxa Vara
angle is about 160° in the young child and about 125° in the adult.
An increase in this angle is referred to as coxa valga, and it
occurs, for example, in cases of congenital dislocation of the hip.
In this condition, adduction of the hip joint is limited. A decrease
coxa vara,
In this condition, abduction of the hip joint is limited. Shenton’s
line is a useful means of assessing the angle of the femoral neck
on a radiograph of the hip region (see Fig. 10.72).
Fractures of the Femur
types, subcapital and trochanteric. The subcapital fracture
occurs in the elderly and is usually produced by a minor trip or
stumble. Subcapital femoral neck fractures are particularly com-
mon in women after menopause. This gender predisposition is
because of a thinning of the cortical and trabecular bone caused
C L I N I C A L N O T E S
(continued)
Basic Anatomy
443
neck
piriformis
greater trochanter
gluteus minimus
iliofemoral ligament
vastus lateralis
intertrochanteric line
vastus intermedius
patellar surface
lateral
ligament
medial ligament
capsule of knee joint
articularis genus
vastus medialis
lesser trochanter
psoas
pubofemoral ligament
capsule of hip joint
fovea capitis
ligament of head
head
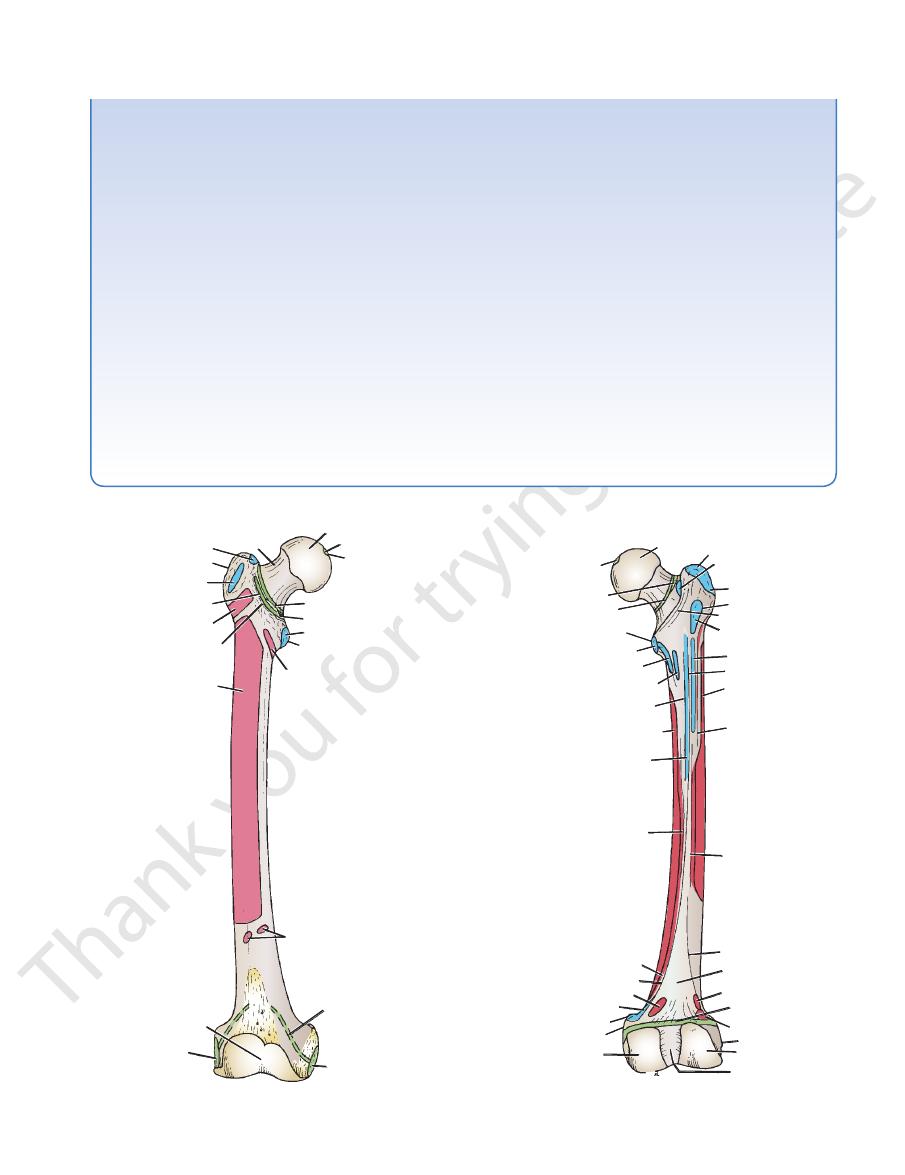
FIGURE 10.10
Muscles and ligaments attached to the ante
rior surface of the right femur.
-
ischiofemoral
ligament
capsule of hip joint
lesser trochanter
psoas
iliacus
pectineus
adductor brevis
vastus medialis
linea aspera
adductor longus
site of hiatus of
adductor magnus
medial supracondylar ridge
gastrocnemius (medial head)
adductor magnus
adductor tubercle
medial condyle
intercondylar notch
lateral condyle
lateral epicondyle
gastrocnemius
(lateral head)
capsule of knee joint
plantaris
popliteal surface
lateral supracondylar
ridge
biceps femoris
(short head)
vastus lateralis
vastus intermedius
adductor magnus
gluteus maximus
quadratus femoris
quadrate tubercle
gluteus medius
obturator externus
greater trochanter
head
intertrochanteric crest
medial epicondyle
ligament of
head of femur
FIGURE 10.11
Muscles and ligaments attached to the poste
siderable displacement occurs. The strong muscles of the thigh
rior surface of the right femur.
-
by estrogen deficiency. Avascular necrosis of the head is a
common complication. If the fragments are not impacted, con-
(Fig. 10.12), including the rectus femoris, the adductor muscles,
correct length before manipulation and operative therapy to
ferent actions of the muscles of the leg is necessary to under
From these accounts, it is clear that knowledge of the dif
ment is smaller and is rotated backward by the gastrocnemius
tures of the middle third of the shaft. However, the distal frag
distal fragment is also rotated backward by the pull of the two
ment is adducted by the adductor muscles, pulled upward by the
gemelli, and the quadratus femoris (Fig. 10.13). The lower frag
femur, the proximal fragment is flexed by the iliopsoas; abducted
bone fragments are not impacted, the pull of the strong muscles
capsular, and both fragments have a profuse blood supply. If the
commonly occur in the young and
and the quadratus femoris rotate the distal fragment laterally, as
and the hamstring muscles, pull the distal fragment upward, so
that the leg is shortened (as measured from the anterior superior
iliac spine to the adductor tubercle or medial malleolus). The glu-
teus maximus, the piriformis, the obturator internus, the gemelli,
seen by the toes pointing laterally.
Trochanteric fractures
middle aged as a result of direct trauma. The fracture line is extra-
will produce shortening and lateral rotation of the leg, as previ-
ously explained.
Fractures of the shaft of the femur usually occur in young and
healthy persons. In fractures of the upper third of the shaft of the
by the gluteus medius and minimus; and laterally rotated by
the gluteus maximus, the piriformis, the obturator internus, the
-
hamstrings and quadriceps, and laterally rotated by the adduc-
tors and the weight of the foot (Fig. 10.13).
In fractures of the middle third of the shaft of the femur,
the distal fragment is pulled upward by the hamstrings and the
quadriceps (Fig. 10.13), resulting in considerable shortening. The
heads of the gastrocnemius (Fig. 10.13).
In fractures of the distal third of the shaft of the femur, the
same displacement of the distal fragment occurs as seen in frac-
-
muscle (Fig. 10.13) to a greater degree and may exert pressure
on the popliteal artery and interfere with the blood flow through
the leg and foot.
-
-
stand the displacement of the fragments of a fractured femur.
Considerable traction on the distal fragment is usually required
to overcome the powerful muscles and restore the limb to its
bring the proximal and distal fragments into correct alignment.
444
CHAPTER 10
The Lower Limb
GAST
QDF
GAST
AM
QDF
HAM
GM
PI
GE
QF
AM
GME
GMI
IP
A
B
C
popliteal
artery
HAM
OI
type 3
GM
PI
OI
GE
QF
A
B
type 1
type 2
type 4
RF
AM
HS
RF
AM
A
A
HS
H
H
FIGURE 10.12
A.
muscles; HS, hamstring muscles.
gluteus maximus; PI, piriformis; OI, obturator internus; GE, gemelli; QF, quadratus femoris; RF, rectus femoris; AM, adductor
powerful muscles. Note in particular the outward rotation of the leg so that the foot characteristically points laterally. GM,
Displacement of the lower bone fragment caused by the pull of the
Fractures of the neck of the femur. B.
FIGURE 10.13
Fractures of the shaft of the femur.
tus femoris; AM, adductor muscles; QDF, quadriceps femoris; HAM, hamstrings; GAST, gastrocnemius.
gluteus medius; GMI, gluteus minimus; GM, gluteus maximus; PI, piriformis; OI, obturator internus; GE, gemelli; QF, quadra
fragment caused by the pull of the gastrocnemius muscle, threatening the integrity of the popliteal artery. IP, iliopsoas; GME,
Lower third of the femoral shaft. Note the excessive displacement of the lower
caused by the gastrocnemius muscle.
Middle third of the femoral shaft. Note the posterior displacement of the lower fragment
pull of the powerful muscles.
Upper third of the femoral shaft. Note the displacement caused by the
A.
B.
C.
-
Basic Anatomy
Posterior cutaneous nerve of the thigh
Sciatic nerve
Piriformis
The following structures exit the foramen (Fig. 10.15):
pelvis into the gluteal region.
and sacrospinous ligaments. It provides an exit from the
greater sciatic notch of the hip bone and the sacrotuberous
The greater sciatic foramen (see Fig. 6.11) is formed by the
Greater Sciatic Foramen
greater sciatic foramen and the lesser sciatic foramen.
The two important foramina in the gluteal region are the
to the spine of the ischium (Fig. 10.14; see Fig. 6.1).
The sacrospinous ligament connects the back of the sacrum
Sacrospinous Ligament
sacrum to the ischial tuberosity (Fig. 10.14; see Fig. 6.1).
The sacrotuberous ligament connects the back of the
Sacrotuberous Ligament
the sacroiliac joint by the weight of the vertebral column.
ligaments is to stabilize the sacrum and prevent its rotation at
rotuberous and sacrospinous ligaments. The function of these
The two important ligaments in the gluteal region are the sac
445
Ligaments of the Gluteal Region
-
Foramina of the Gluteal Region
■
■
■
■
■
■
posterior superior iliac spine
superior gluteal nerve
piriformis
sacrotuberous ligament
inferior gluteal artery
coccyx
sacrospinous ligament
internal pudendal artery
pudendal nerve
body of pubis
nerve to quadratus femoris
ischial tuberosity
adductor magnus
medial femoral circumflex artery
posterior cutaneous nerve of thigh
sciatic nerve
iliopsoas tendon
quadratus femoris
obturator externus
greater trochanter
gemellus inferior
obturator internus
gemellus superior
ischial spine
tensor fasciae latae
inferior gluteal nerve
straight
reflected
head of
rectus femoris
gluteus minimus
iliac crest
superior gluteal artery
nerve to obturator
internus
FIGURE 10.14
Deep structures in the right gluteal region; the gluteus maximus and the gluteus medius muscles have been
completely removed.
446
CHAPTER 10
The Lower Limb
posterior superior iliac spine
sacrotuberous ligament
superior gluteal artery
inferior gluteal artery
and nerve
spine of ischium
nerve to
obturator internus
pudendal nerve
sacrospinous ligament
internal pudendal artery
coccyx
ischiorectal fossa
anus
fat
semimembranosus
gracilis
nerve to hamstrings
adductor magnus
semitendinosus
biceps femoris
gluteus maximus
sciatic nerve
iliotibial tract
adductor magnus
quadratus femoris
posterior cutaneous nerve
of thigh
greater trochanter
gemellus superior
piriformis
superior gluteal nerve
tensor fasciae latae
gluteus minimus
superior gluteal artery
gluteus medius
iliac crest
gemellus inferior
oburator internus
FIGURE 10.15
Structures in the right gluteal region. The greater part of the gluteus maximus and part of the gluteus medius
extended position.
gluteus maximus muscle in maintaining the knee in the
to its insertion in the iliotibial tract and thus assists the
The tensor fasciae latae runs downward and backward
largely responsible for the prominence of the buttock.
the body. It lies superficial in the gluteal region and is
The gluteus maximus (Fig. 10.5) is the largest muscle in
Note the following:
and described in Table 10.1.
The muscles are shown in Figures 10.5, 10.14, and 10.15
superior and inferior gemelli, and the quadratus femoris.
fasciae latae, the piriformis, the obturator internus, the
mus, the gluteus medius, the gluteus minimus, the tensor
The muscles of the gluteal region include the gluteus maxi
Internal pudendal artery and vein
Pudendal nerve
Nerve to obturator internus
Tendon of obturator internus muscle
(Fig. 10.14):
The following structures pass through the foramen
the perineum below the pelvic floor.
the greater sciatic foramen above the pelvic floor to enter
nerves and blood vessels that have left the pelvis through
the perineum from the gluteal region. Its presence enables
and sacrospinous ligaments. It provides an entrance into
lesser sciatic notch of the hip bone and the sacrotuberous
The lesser sciatic foramen (see Fig. 6.11) is formed by the
Lesser Sciatic Foramen
Internal pudendal artery and vein
Superior and inferior gluteal arteries and veins
Pudendal nerve
Nerves to the obturator internus and quadratus femoris
Superior and inferior gluteal nerves
have been removed.
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
Muscles of the Gluteal Region
-
■
■
■
■
Basic Anatomy
447
Muscles of the Gluteal Region
T A B L E 1 0 . 1
Tensor fasciae
Muscle
Origin
Insertion
Nerve Supply
Nerve Root
a
Action
Gluteus
maximus
Outer surface of
ilium, sacrum,
coccyx,
sacrotuberous
ligament
Iliotibial tract and
gluteal tuberosity
of femur
Inferior gluteal
nerve
L5; S1, 2
Extends and
laterally rotates
hip joint; through
iliotibial tract,
it extends knee
joint
Gluteus medius
Outer surface of
ilium
Lateral surface of
greater trochanter
of femur
Superior
gluteal nerve
L5; S1
Abducts thigh at hip
joint; tilts pelvis
when walking to
permit opposite
leg to clear
ground
Gluteus minimus
Outer surface of
ilium
Anterior surface of
greater trochanter
of femur
Superior gluteal
nerve
L5; S1
Abducts thigh at hip
joint; tilts pelvis
when walking to
permit opposite
leg to clear
ground
latae
Iliac crest
Iliotibial tract
Superior gluteal
nerve
L4; 5
Assists gluteus
maximus in
extending the
knee joint
Piriformis
Anterior surface
of sacrum
Upper border of
greater trochanter
of femur
1st and 2nd
sacral nerves
L5; S1, 2
Lateral rotator of
thigh at hip joint
Obturator
internus
Inner surface
of obturator
membrane
Upper border of
greater trochanter
of femur
Sacral plexus
L5; S1
Lateral rotator of
thigh at hip joint
Gemellus
superior
Spine of ischium
Upper border of
greater trochanter
of femur
Sacral plexus
L5; S1
Lateral rotator of
thigh at hip joint
Gemellus
inferior
Ischial tuberosity
Upper border of
greater trochanter
of femur
Sacral plexus
L5; S1
Lateral rotator of
thigh at hip joint
Quadratus
femoris
Lateral border
of ischial
tuberosity
Quadrate tubercle of
femur
Sacral plexus
L5; S1
Lateral rotator of
thigh at hip joint
a
The predominant nerve root supply is indicated by boldface type.
448
CHAPTER 10
the vastus lateralis, and overlying the ischial tuberosity.
greater trochanter, between the tendon of insertion and
maximus: between the tendon of insertion and the
Three bursae are usually associated with the gluteus
is inserted into the greater trochanter of the femur.
tendon is joined by the superior and inferior gemelli and
lesser sciatic foramen to enter the gluteal region. The
within the pelvis at its origin. It emerges through the
The obturator internus is a fan-shaped muscle that lies
gluteal vessels and nerves (Fig. 10.15).
the superior gluteal vessels and nerves from the inferior
to enter the gluteal region. Its position serves to separate
its origin. It emerges through the greater sciatic foramen
The piriformis (Fig. 10.15) lies partly within the pelvis at
The Lower Limb
■
■
■
■
■
■
ciculi that can be easily separated without damage. The great
Gluteus Maximus and Intramuscular Injections
The gluteus maximus is a large, thick muscle with coarse fas-
thickness of this muscle makes it ideal for intramuscular injec-
tions. To avoid injury to the underlying sciatic nerve, the injec-
tion should be given well forward on the upper outer quadrant
of the buttock.
Gluteus Maximus and Bursitis
Bursitis, or inflammation of a bursa, can be caused by acute
or chronic trauma. An inflamed bursa becomes distended with
excessive amounts of fluid and can be extremely painful. The
bursae associated with the gluteus maximus are prone to
inflammation.
C L I N I C A L N O T E S
seriously interferes with the ability of the patient to tilt the pel
ments of the spinal cord. They are supplied by the superior
Gluteus Medius and Minimus and Poliomyelitis
The gluteus medius and minimus muscles may be paralyzed
when poliomyelitis involves the lower lumbar and sacral seg-
gluteal nerve (L4 and 5 and S1). Paralysis of these muscles
-
vis when walking.
C L I N I C A L N O T E S
Nerves of the Gluteal Region
pelvic surface.
rator internus supplies the obturator internus muscle on its
supplies structures in the perineum. The nerve to the obtu
in the ischiorectal fossa (see page 309). The pudendal nerve
the pelvis through the lesser sciatic foramen; they then lie
with the internal pudendal artery and immediately re-enter
formis (Figs. 10.14 and 10.15). They cross the ischial spine
lower part of the greater sciatic foramen, below the piri
nerve to the obturator internus leave the pelvis through the
Branches of the sacral plexus, the pudendal nerve, and
Obturator Internus
Pudendal Nerve and the Nerve to the
the quadratus femoris and the inferior gemellus.
greater sciatic foramen (Fig. 10.15). It ends by supplying
femoris leaves the pelvis through the lower part of the
A branch of the sacral plexus, the nerve to the quadratus
Nerve to the Quadratus Femoris
It supplies the gluteus maximus muscle.
atic foramen below the piriformis (Figs. 10.14 and 10.15).
leaves the pelvis through the lower part of the greater sci
The inferior gluteal nerve, a branch of the sacral plexus,
Inferior Gluteal Nerve
both, and ends by supplying the tensor fasciae latae.
ward between the gluteus medius and minimus, supplies
atic foramen above the piriformis (Fig. 10.15). It runs for
leaves the pelvis through the upper part of the greater sci
The superior gluteal nerve, a branch of the sacral plexus,
Superior Gluteal Nerve
upper part of the leg (Fig. 10.1)
to the back of the thigh and the
Cutaneous branches
or labium majus
to the skin of the back of the scrotum
Perineal branch
quadrant of the buttock (Fig. 10.1)
to the skin over the lower medial
Gluteal branches
Branches
thigh beneath the deep fascia. In the popliteal fossa, it sup
surface of the sciatic nerve and runs down the back of the
muscle (Fig. 10.14). It passes downward on the posterior
part of the greater sciatic foramen below the piriformis
sacral plexus, enters the gluteal region through the lower
The posterior cutaneous nerve of the thigh, a branch of the
Posterior Cutaneous Nerve of the Thigh
region.
The sciatic nerve usually gives no branches in the gluteal
region by passing above or through the piriformis muscle.
sciatic nerve high in the pelvis and appears in the gluteal
Occasionally, the common peroneal nerve leaves the
biceps femoris to enter the back of the thigh (see page 466).
the buttock region by passing deep to the long head of the
ous nerve of the thigh and the gluteus maximus. It leaves
(Fig. 10.15). It is related posteriorly to the posterior cutane
femoris to reach the back of the adductor magnus muscle
obturator internus, the inferior gemellus, and the quadratus
on the root of the ischial spine, the superior gemellus, the
cle and curves downward and laterally, lying successively
and 10.17). The nerve appears below the piriformis mus
mon peroneal nerves bound together with fascia (Figs. 10.16
largest nerve in the body and consists of the tibial and com
the greater sciatic foramen (Figs. 10.14 and 10.15). It is the
2, and 3), emerges from the pelvis through the lower part of
The sciatic nerve, a branch of the sacral plexus (L4 and 5; S1,
Sciatic Nerve
-
-
-
-
plies the skin.
■
■
■
■
■
■
-
-
-
-
-
Basic Anatomy
449
L4 L5 S1 S2 S3
sciatic nerve
pelvis
sacral plexus
sciatic nerve
gluteal region
tibial nerve
common peroneal nerve
back of thigh
biceps femoris (short head)
lateral cutaneous nerve of calf
knee joint
lower leg
skin of lateral side of leg
sural
communicating
branch
deep peroneal
nerve
tibialis
anterior
extensor
hallucis longus
peroneus tertius
ankle joint
superficial peroneal nerve
peroneus longus
skin of leg
foot
skin of lateral
side of foot
and little toe
extensor
digitorum
brevis
skin of cleft
between first
and second toes
skin of dorsum of foot
extensor digitorum
longus
peroneus brevis
FIGURE 10.16
Summary of the origin of the sciatic nerve and the main branches of the common peroneal nerve.
the first perforating artery, a branch of the profunda artery.
ral circumflex artery, the lateral femoral circumflex artery, and
the anastomosis: the inferior gluteal artery, the medial femo
and the femoral arteries. The following arteries take part in
anastomosis, provides a connection between the internal iliac
trochanter of the femur and, together with the trochanteric
The cruciate anastomosis is situated at the level of the lesser
The Cruciate Anastomosis
circumflex artery, and the lateral femoral circumflex artery.
gluteal artery, the inferior gluteal artery, the medial femoral
following arteries take part in the anastomosis: the superior
along the femoral neck beneath the capsule (Fig. 10.18). The
supply to the head of the femur. The nutrient arteries pass
The trochanteric anastomosis provides the main blood
The Trochanteric Anastomosis
region.
ous branches that are distributed throughout the gluteal
formis (Figs. 10.14 and 10.15). It divides into numer
lower part of the greater sciatic foramen, below the piri
iliac artery and enters the gluteal region through the
The inferior gluteal artery is a branch of the internal
Inferior Gluteal Artery
distributed throughout the gluteal region.
(Figs. 10.14 and 10.15). It divides into branches that are
part of the greater sciatic foramen above the piriformis
iliac artery and enters the gluteal region through the upper
The superior gluteal artery is a branch from the internal
Superior Gluteal Artery
Arteries of the Gluteal Region
-
-
-
Arterial Anastomoses and Femoral Artery Occlusion
The importance of the trochanteric and cruciate anastomoses
in femoral artery occlusion is discussed on page 524.
C L I N I C A L N O T E S
450
CHAPTER 10
The Lower Limb
sciatic nerve
L4 L5 S1 S2 S3
pelvis
sacral plexus
gluteal region
sciatic nerve
hip joint
tibial nerve
common peroneal nerve
back of thigh
semitendinosus
biceps femoris
(long head)
semimembranosus
adductor magnus
(hamstring part)
lower leg
knee joint
gastrocnemius
soleus
plantaris
popliteus
tibialis posterior
flexor digitorum longus
flexor hallucis longus
skin of ankle
ankle joint
sural nerve
sole of foot
medial plantar nerve
adductor hallucis
flexor digitorum brevis
flexor hallucis brevis
first lumbrical
joints
of foot
skin of sole
of foot
lateral plantar nerve
skin of sole
of foot
flexor digitorum accessorius
abductor digiti minimi
flexor digiti minimi brevis
second, third, fourth lumbricals
abductor hallucis
all interossei
FIGURE 10.17
Summary of the origin of the sciatic nerve and the main branches of the tibial nerve.
a branch of the
lateral cutaneous nerve of the thigh,
The
Cutaneous Nerves
The Front and Medial Aspects
of the Thigh
Skin of the Thigh
lumbar plexus (L2 and 3), enters the thigh behind the lateral
the cremaster muscle (see page 222).
small area of skin (Fig. 10.2). The genital branch supplies
behind the middle of the inguinal ligament and supplies a
branch of the lumbar plexus (L1 and 2), enters the thigh
femoral branch of the genitofemoral nerve,
The
skin of the lower lateral quadrant of the buttock (Fig. 10.1).
the lateral aspect of the thigh and knee. It also supplies the
into anterior and posterior branches, it supplies the skin of
end of the inguinal ligament (Fig. 10.2). Having divided
a