
Basic Anatomy
467
peroneal nerves (Figs. 10.29 and 10.31). Occasionally, the
The synovial membrane lines the capsule and is
membrane (Fig. 10.18).
notch. It lies within the joint and is ensheathed by synovial
the transverse ligament and the margins of the acetabular
on the head of the femur (fovea capitis) and by its base to
angular (Fig. 10.18). It is attached by its apex to the pit
is flat and tri
ligament of the head of the femur
The
through which the blood vessels and nerves enter the joint.
10.18). The ligament converts the notch into a tunnel
acetabular labrum as it bridges the acetabular notch (Fig.
is formed by the
transverse acetabular ligament
The
limits extension.
and are attached to the greater trochanter. This ligament
margin (Fig. 10.32). The fibers pass upward and laterally
attached to the body of the ischium near the acetabular
is spiral shaped and is
ischiofemoral ligament
The
extension and abduction.
part of the intertrochanteric line. This ligament limits
of the pubis, and the apex is attached below to the lower
The base of the ligament is attached to the superior ramus
is triangular (Fig. 10.32).
pubofemoral ligament
The
extension during standing.
teric line of the femur. This strong ligament prevents over
attached to the upper and lower parts of the intertrochan
inferior iliac spine above; below, the two limbs of the Y are
ligament (Fig. 10.32). Its base is attached to the anterior
is a strong, inverted Y-shaped
iliofemoral ligament
The
These blood vessels supply the head and neck of the femur.
retinacula.
reflected upward along the neck as bands called
front, some of its fibers, accompanied by blood vessels, are
behind. At its attachment to the intertrochanteric line in
halfway along the posterior aspect of the neck of the bone
to the intertrochanteric line of the femur in front and
ular labrum medially (Fig. 10.18). Laterally, it is attached
The capsule encloses the joint and is attached to the acetab
The hip joint is a synovial ball-and-socket joint.
Type
The articular surfaces are covered with hyaline cartilage.
(Fig. 10.18).
transverse acetabular ligament
notch and is here called the
The labrum bridges across the acetabular
tabular labrum.
ace
by the presence of a fibrocartilaginous rim called the
The cavity of the acetabulum is deepened
acetabular notch.
lum is horseshoe shaped and is deficient inferiorly at the
hip bone (Fig. 10.18). The articular surface of the acetabu
head of the femur and the cup-shaped acetabulum of the
The hip joint is the articulation between the hemispherical
run medially to supply the muscles (Figs. 10.29 and 10.31).
arise from the tibial component of the sciatic nerve and
hamstring part of the adductor magnus. These branches
ris, the semitendinosus, the semimembranosus, and the
to the long head of the biceps femo
Muscular branches
course is described on page 479.
fossa on the lateral side of the tibial nerve. Its further
sciatic nerve (Figs. 10.29 and 10.31), enters the popliteal
a terminal branch of the
common peroneal nerve,
The
Its further course is described on page 479.
(Figs. 10.17, 10.29, and 10.31), enters the popliteal fossa.
a terminal branch of the sciatic nerve
tibial nerve,
The
Branches
even inside the pelvis.
level—in the upper part of the thigh, the gluteal region, or
sciatic nerve divides into its two terminal parts at a higher
■
■
■
■
■
■
-
Hip Joint
Articulation
-
-
Capsule
-
Ligaments
-
-
-
Synovial Membrane
attached to
the articular surfaces (Fig. 10.18).
the margins of
the joint capsule. It ensheathes the ligament of the head of
It covers the portion of the neck of the femur that lies within
anterior inferior
iliac spine
opening for bursa
superior ramus of pubis
pubofemoral
ligament
intertrochanteric
line
iliofemoral ligament
capsule
A
ischium
iliofemoral ligament
ischiofemoral
ligament
intertrochanteric
crest
area of loose attachment
of capsule
B
FIGURE 10.32
Anterior aspect (A) and posterior aspect (B) of the right hip joint.
468
CHAPTER 10
ing movements take place:
tion is limited by the ischiofemoral ligament. The follow
iliofemoral and pubofemoral ligaments, and medial rota
the femur. Lateral rotation is limited by the tension in the
site limb and by the tension in the ligament of the head of
ament, and adduction is limited by contact with the oppo
Abduction is limited by the tension of the pubofemoral lig
the iliofemoral, pubofemoral, and ischiofemoral ligaments.
ward to the anatomic position, is limited by the tension of
Extension, which is the movement of the flexed thigh back
limited by the tension of the hamstring group of muscles.
rior abdominal wall. When the knee is extended, flexion is
surface of the thigh coming into contact with the ante
When the knee is flexed, flexion is limited by the anterior
ing part in the articulation and on the strong ligaments.
of the joint depends largely on the shape of the bones tak
The hip joint has a wide range of movements. The strength
quadratus femoris supply the area.
Femoral, obturator, and sciatic nerves and the nerve to the
beneath the psoas tendon (Figs. 10.32
psoas bursa
forms the
between the pubofemoral and iliofemoral ligaments, and
protrudes through a gap in the anterior wall of the capsule,
tabular fossa. A pouch of synovial membrane frequently
the femur and covers the pad of fat contained in the ace
The Lower Limb
-
and 10.33).
Nerve Supply
Movements
-
-
-
-
-
-
-
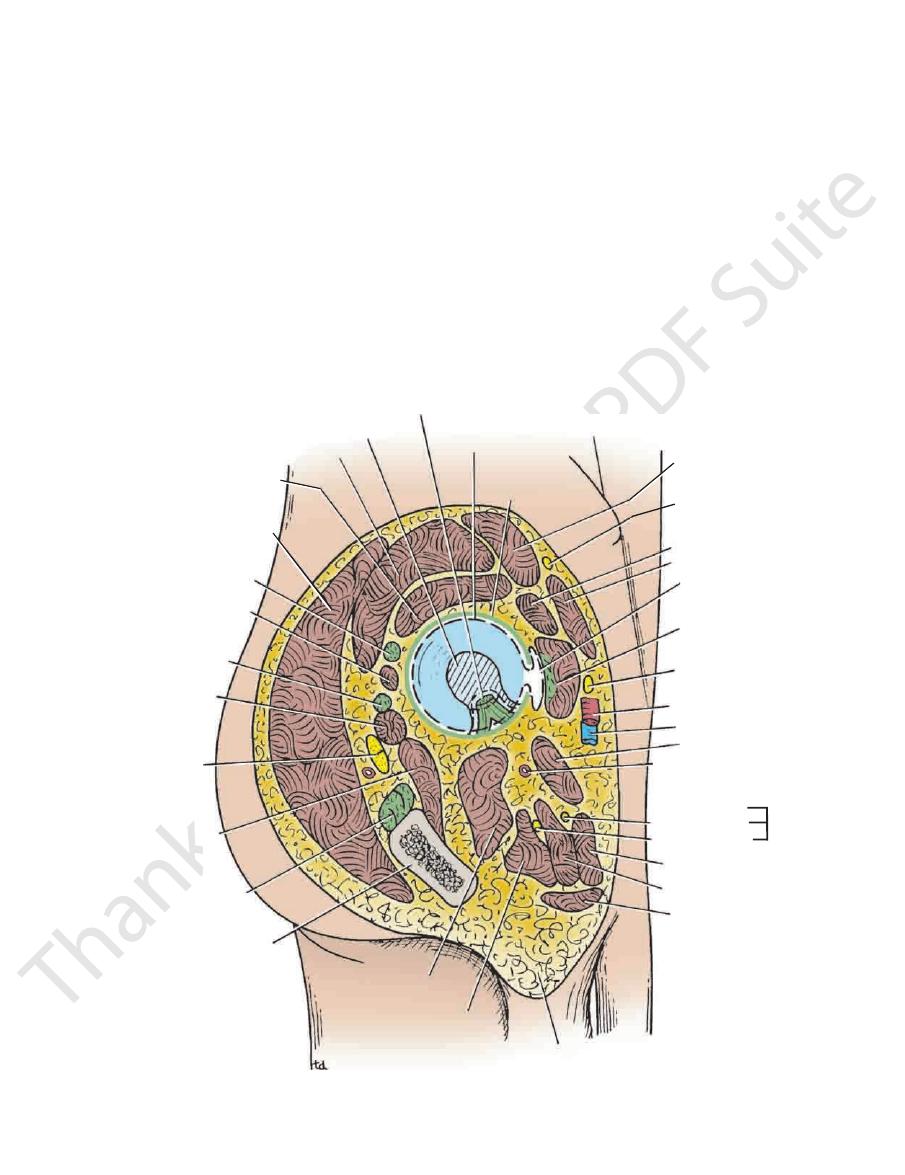
ligament of femoral head
synovial pad of fat
gluteus medius
gluteus
minimus
gluteus
maximus
piriformis
gemellus superior
obturator internus
gemellus inferior
sciatic nerve
quadratus femoris
hamstrings
ischium
obturator externus
adductor magnus
root of scrotum
gracilis
adductor brevis
adductor longus
posterior division
anterior division
obturator nerve
medial circumflex
femoral artery
pectineus
femoral vein
femoral artery
femoral nerve
iliopsoas
bursa
sartorius
rectus femoris
lateral cutaneous
nerve of thigh
tensor fasciae
latae
anterior superior iliac spine
capsule
synovial membrane
anterior
posterior
FIGURE 10.33
Structures surrounding the right hip joint.
Basic Anatomy
Adduction
and piriformis.
minimus, assisted by the sartorius, tensor fasciae latae,
is performed by the gluteus medius and
Abduction
muscles.
is performed by the gluteus maximus and the hamstring
(a backward movement of the flexed thigh)
Extension
and sartorius and also by the adductor muscles.
is performed by the iliopsoas, rectus femoris,
Flexion
469
■
■
■
■
■
■
■
■
is performed by the adductor longus and
is
brev
and the adductor fibers of the adductor magnus. These
muscles are assisted by the pectineus and the gracilis.
fasciae latae.
the gluteus medius and gluteus minimus and the tensor
is performed by the anterior fibers of
Medial rotation
and quadratus femoris, assisted by the gluteus maximus.
tor internus and externus, superior and inferior gemelli,
is performed by the piriformis, obtura
Lateral rotation
■
■
-
■
■
Referred Pain from the Hip Joint
(posterior dislocation). The close relation of the sciatic nerve to
tabulum, and it comes to rest on the gluteal surface of the ilium
The head of the femur is displaced posteriorly out of the ace
it can lodge, rides up out of the acetabulum onto the gluteal
the head of the femur, having no stable platform under which
upper lip of the acetabulum fails to develop adequately, and
ments. In congenital dislocation of the hip (see page 512), the
The stability of the hip joint depends on the ball-and-socket
The femoral nerve not only supplies the hip joint but, via the
intermediate and medial cutaneous nerves of the thigh, also sup-
plies the skin of the front and medial sides of the thigh. It is not
surprising, therefore, for pain originating in the hip joint to be
referred to the front and medial side of the thigh. The posterior
division of the obturator nerve supplies both the hip and knee
joints. This would explain why hip joint disease sometimes gives
rise to pain in the knee joint.
Congenital Dislocation of the Hip
arrangement of the articular surfaces and the strong liga-
surface of the ilium.
Traumatic Dislocation of the Hip
Traumatic dislocation of the hip is rare because of its strength; it
is usually caused by motor vehicle accidents. However, should it
occur, it usually does so when the joint is flexed and adducted.
-
the posterior surface of the joint makes it prone to injury in pos-
terior dislocations.
Hip Joint Stability and Trendelenburg’s Sign
The stability of the hip joint when a person stands on one leg with
the foot of the opposite leg raised above the ground depends on
three factors:
■
■
The gluteus medius and minimus must be functioning
ion, adduction, and external rotation and is produced initially by
reflex spasm of the surrounding muscles. The deformity is flex
supplies both joints). The stiffness is caused by the pain and
the adult, causes pain, stiffness, and deformity. The pain may be
the most common disease of the hip joint in
increased amount of synovial fluid secreted. The hip joint is par
or she will show the characteristic “dipping” gait. In patients
will sink below the horizontal. If the patient is asked to walk, he
Trendelenburg’s sign, and the unsupported side of the pelvis
the opposite leg clear off the ground, will exhibit a positive
tion of the hip, when asked to stand on the right leg and raise
clear of the ground before it is thrust forward in taking the
at the hip joint and moved forward—that is, the leg is raised
on one side and then on the other, allowing the leg to be flexed
other. By this means, he or she is able to raise the pelvis first
gluteus medius and minimus, first on one side and then on the
Normally, when walking, a person alternately contracts the
downward on the opposite, unsupported side. The patient is then
The neck of the femur must be intact and must have a normal
normally.
■
■
The head of the femur must be located normally within the
acetabulum.
■
■
angle with the shaft of the femur.
If any one of these factors is defective, then the pelvis will sink
said to exhibit a positive Trendelenburg’s sign (Fig. 10.34).
forward step. A patient with a right-sided congenital disloca-
with bilateral congenital dislocation of the hip, the gait is typi-
cally “waddling” in nature.
Arthritis of the Hip Joint
A patient with an inflamed hip joint will place the femur in the
position that gives minimum discomfort—that is, the position in
which the joint cavity has the greatest capacity to contain the
-
tially flexed, abducted, and externally rotated.
Osteoarthritis,
in the hip joint itself or referred to the knee (the obturator nerve
-
muscle spasm and later by muscle contracture.
C L I N I C A L N O T E S
■
Superiorly:
the sciatic nerve (Fig. 10.32).
the quadratus femoris muscles separate the joint from
The obturator internus, the gemelli, and
Posteriorly:
ral vessels and nerve from the joint (Fig. 10.33).
muscles. The iliopsoas and pectineus separate the femo
Iliopsoas, pectineus, and rectus femoris
Anteriorly:
Important Relations
than the medial rotators.
flexor group, and the lateral rotators are more powerful
The extensor group of muscles is more powerful than the
movements.
is a combination of the previous
Circumduction
■
■
■
-
■
■
■
■
Piriformis and gluteus minimus (Fig. 10.33).
Obturator externus tendon (Fig. 10.33).
Inferiorly:
■
■