500
CHAPTER 10
the condyles of the tibia and their cartilaginous menisci
Above are the rounded condyles of the femur; below are
Articulation
Note that the fibula is not directly involved in the joint.
between the patella and the patellar surface of the femur.
the corresponding condyles of the tibia, and a gliding joint,
between the medial and lateral condyles of the femur and
in the body. Basically, it consists of two condylar joints
The knee joint is the largest and most complicated joint
The hip joint is fully described on page 467.
articular branches to the joints of the foot.
sor digitorum brevis muscle. Both terminal branches give
ond toes (Fig. 10.60). The lateral branch supplies the exten
supplies the skin of the adjacent sides of the big and sec
terminal, medial, and lateral branches. The medial branch
of the dorsalis pedis artery (see page 485). It divides into
The Lower Limb
-
-
Joints of the Lower Limb
Knee Joint
(Fig. 10.35); in front is the articulation between the lower
tellar bursa
suprapa
beneath the quadriceps tendon, forming the
permitting the synovial membrane to pouch upward
the joint. On the front of the joint, the capsule is absent,
surfaces and surrounds the sides and posterior aspect of
The capsule is attached to the margins of the articular
vial joint of the plane gliding variety.
possible. The joint between the patella and femur is a syno
the hinge variety, but some degree of rotatory movement is
The joint between the femur and tibia is a synovial joint of
Type
tibial plateaus
referred to clinically as the medial and lateral
faces of the medial and lateral condyles of the tibia are often
covered with hyaline cartilage. Note that the articular sur
The articular surfaces of the femur, tibia, and patella are
end of the femur and the patella.
-
.
-
Capsule
-
(Fig.
h side of the patella, the
10.35). On eac
above to the lateral condyle of the femur and below to the
is cordlike and is attached
lateral collateral ligament
The
the common tendon of the quadriceps femoris muscle.
10.35). It is, in fact, a continuation of the central portion of
der of the patella and below to the tuberosity of the tibia (Fig.
is attached above to the lower bor
ligamentum patellae
The
Extracapsular Ligaments
capsule and those that lie within the capsule.
The ligaments may be divided into those that lie outside the
Ligaments
permits the tendon of the popliteus to emerge (Fig. 10.35).
An opening in the capsule behind the lateral tibial condyle
(Fig. 10.35).
oblique popliteal ligament
muscle called the
is strengthened by an expansion of the semimembranous
vastus lateralis and medialis. Behind the joint, the capsule
capsule is strengthened by expansions from the tendons of
-
head of the fibula (Fig. 10.35). The tendon of the popliteus
and below to the medial surface of the shaft of the tibia
attached above to the medial condyle of the femur
medial collateral ligament
The
meniscus (Fig. 10.61).
muscle intervenes between the ligament and the lateral
is a flat band and is
(Fig. 10.35).
popliteal bursa
popliteus, forming the
longed downward on the deep surface of the tendon of the
At the back of the joint, the synovial membrane is pro
muscle (Fig. 10.35).
articularis genus
called the
ment of a small portion of the vastus intermedius muscle,
. This is held in position by the attach
suprapatellar bursa
cle for three fingerbreadths above the patella, forming the
which extends up beneath the quadriceps femoris mus
10.61). On the front and above the joint, it forms a pouch,
to the margins of the articular surfaces (Figs. 10.35 and
The synovial membrane lines the capsule and is attached
Synovial Membrane
it is relatively immobile.
meniscus is also attached to the medial collateral ligament,
tibia by anterior and posterior horns. Because the medial
Each meniscus is attached to the upper surface of the
cushions between the two bones.
to receive the convex femoral condyles; they also serve as
tion is to deepen the articular surfaces of the tibial condyles
surfaces are in contact with the tibial condyles. Their func
faces are in contact with the femoral condyles. The lower
forms a free edge (Figs. 10.35 and 10.61). The upper sur
capsule, and the inner border is thin and concave and
tilage. The peripheral border is thick and attached to the
The menisci are C-shaped sheets of fibrocar
Menisci
being pulled posteriorly.
With the knee joint flexed, the PCL prevents the tibia from
prevents anterior displacement of the femur on the tibia.
medial femoral condyle (Figs. 10.35 and 10.61). The PCL
be attached to the anterior part of the lateral surface of the
of the tibia and passes upward, forward, and medially to
ament (PCL) is attached to the posterior intercondylar area
The posterior cruciate lig
Posterior Cruciate Ligament
from being pulled anteriorly.
tibia. With the knee joint flexed, the ACL prevents the tibia
ACL prevents posterior displacement of the femur on the
the lateral femoral condyle (Figs. 10.35 and 10.61). The
be attached to the posterior part of the medial surface of
of the tibia and passes upward, backward, and laterally, to
ment (ACL) is attached to the anterior intercondylar area
The anterior cruciate liga
Anterior Cruciate Ligament
tibia throughout the joint’s range of movement.
ligaments are the main bond between the femur and the
to their tibial attachments (Fig. 10.61). These important
10.35). They are named anterior and posterior, according
ments that cross each other within the joint cavity (Fig.
are two strong intracapsular liga
cruciate ligaments
The
Intracapsular Ligaments
strengthens the posterior aspect of the capsule (Fig. 10.35).
sion derived from the semimembranosus muscle. It
is a tendinous expan
oblique popliteal ligament
The
(Fig. 10.61).
meniscus
It is firmly attached to the edge of the medial
-
-
-
-
-
-
-
-
-
-
. A bursa is
osed
interp

Basic Anatomy
501
infrapatellar pad of fat
infrapatellar fold
of synovial membrane
alar fold
anterior cruciate
ligament
medial
collateral
ligament
medial
meniscus
sartorius
gracilis
saphenous nerve
great saphenous vein
semimembranosus
semitendinosus
oblique popliteal ligament
gastrocnemius (medial head)
small saphenous vein
tibial nerve
popliteal artery
gastrocnemius (lateral head)
posterior cruciate ligament
popliteal vein
plantaris
common peroneal nerve
deep fascia
biceps femoris
popliteus
tendon
lateral collateral
ligament
lateral
meniscus
capsule
synovial membrane
transverse ligament
ligamentum patellae
prepatellar bursa
FIGURE 10.61
Relations of the right knee joint.
ceps muscle and communicates with the joint cavity
lies beneath the quadri
suprapatellar bursa
The
Anterior Bursae
may communicate with the joint.
membranosus bursa
semi
always communicate with the joint, and the
bursa
popliteal
suprapatellar bursa
behind the joint. The
Four are situated in front of the joint and six are found
found wherever skin, muscle, or tendon rubs against bone.
Numerous bursae are related to the knee joint. They are
Bursae Related to the Knee Joint
(Fig. 10.61).
alar folds
borders of the fold are termed the
the free
infrapatellar fold;
mentum patellae to form the
is reflected backward from the posterior surface of the liga
In the anterior part of the joint, the synovial membrane
behind the synovial cavity and are not bathed in synovial fluid.
ligaments (Fig. 10.61). As a result, the cruciate ligaments lie
posterior part of the capsule around the front of the cruciate
The synovial membrane is reflected forward from the
quently communicates with the synovial cavity of the joint.
and it fre
semimembranosus bursa,
this is termed the
medial femoral condyle and the semimembranosus tendon;
between the medial head of the gastrocnemius and the
-
-
and the
-
■
■
-
(Fig. 10.35). It is described above.
communicate with the joint cavity. It was described
insertion of the semimembranosus muscle and may
is found related to the
semimembranosus bursa
The
cavity. It was described previously.
don of the popliteus and communicates with the joint
is found in association with the ten
popliteal bursa
The
Posterior Bursae
tum patellae and the tibia (Fig. 10.35).
lies between the ligamen
deep infrapatellar bursa
The
part of the ligamentum patellae (Fig. 10.35).
neous tissue between the skin and the front of the lower
lies in the subcuta
superficial infrapatellar bursa
The
(Figs. 10.35 and 10.61).
patella and the upper part of the ligamentum patellae
between the skin and the front of the lower half of the
lies in the subcutaneous tissue
prepatellar bursa
The
■
■
■
■
-
■
■
-
■
■
-
■
■
previously.
nerves supply the knee joint.
The femoral, obturator, common peroneal, and tibial
Nerve Supply
medial head of origin of the gastrocnemius muscle.
of origin of the gastrocnemius muscle; and beneath the
pass to their insertion on the tibia; beneath the lateral head
the sartorius, gracilis, and semitendinosus muscles as they
of insertion of the biceps femoris; related to the tendons of
The remaining four bursae are found related to the tendon
502
CHAPTER 10
sus muscles, assisted by the gracilis, sartorius, and popliteus
The biceps femoris, semitendinosus, and semimembrano
The following muscles produce movements of the knee joint.
especially the cruciate ligaments, are slack in this position.
on the femur. This is possible because the major ligaments,
the tibia can also be moved passively forward and backward
erable range of rotation is possible. In the flexed position,
When the knee joint is flexed to a right angle, a consid
being pulled backward also.
popliteus to the lateral meniscus results in that structure
ing contour of the femoral condyles. The attachment of the
again, the menisci have to adapt their shape to the chang
muscle, which laterally rotates the femur on the tibia. Once
ing or untwisting process is accomplished by the popliteus
permit movements between the joint surfaces. This unlock
tial that the major ligaments be untwisted and slackened to
Before flexion of the knee joint can occur, it is essen
The extended knee is said to be in the locked position.
rubber cushions between the femoral and tibial condyles.
rigid structure; the cartilaginous menisci are compressed like
ligaments of the joint, and the knee becomes a mechanically
the femur results in a twisting and tightening of all the major
medial rotation of
assumes the position of full extension,
The knee joint can flex, extend, and rotate. As the knee joint
Movements
The Lower Limb
1
-
-
-
-
Flexion
-
(Fig. 10.61)
Biceps femoris and common peroneal nerve
Laterally:
cles (Fig. 10.61)
Sartorius, gracilis, and semitendinosus mus
Medially:
taris (Fig. 10.61)
oris, the two heads of the gastrocnemius, and the plan
semimembranosus, the semitendinosus, the biceps fem
form the boundaries of the popliteal fossa, namely, the
peroneal nerves; lymph nodes; and the muscles that
The popliteal vessels; tibial and common
Posteriorly:
The prepatellar bursa (Fig. 10.61)
Anteriorly:
Important Relations
knee joint.
especially the quadriceps femoris, after injury to the
otherapist to build up the strength of these muscles,
cles is the most important, and it is the job of the physi
of the ligaments. Of these factors, the tone of the mus
the strong muscles acting on the joint and the strength
The stability of the knee joint depends on the tone of
The biceps femoris produces lateral rotation.
Lateral Rotation
rotation.
The sartorius, gracilis, and semitendinosus produce medial
Medial Rotation
limited by the tension of all the major ligaments of the joint.
The quadriceps femoris produces extension. Extension is
of the back of the leg with the thigh.
muscles, produce flexion. Flexion is limited by the contact
may be laterally rotated on the femur to lock the knee joint.
lize the knee joint. However, if the foot is raised off the ground, the tibia
is standing, the femur is medially rotated on the tibia to lock and stabi
Note that when the foot is firmly planted on the ground when a person
1
-
Extension
-
-
■
■
■
■
-
-
■
■
-
■
■
Strength of the Knee Joint
ligament in the body, for which surgery is performed. The condi
Tears of the ACL
Forced adduction of the tibia on the femur can result in injury
whereas sprains of the medial collateral ligament result in ten
femoral or tibial attachments. It is useful to remember that tears
of insertion of the vastus lateralis and medialis, respectively.
aged, the large synovial cavity becomes distended with fluid. The
the quadriceps femoris; provided that this is well developed, it is
muscles acting on the joint. The most important muscle group is
ligaments that bind the femur to the tibia and on the tone of the
The strength of the knee joint depends on the strength of the
capable of stabilizing the knee in the presence of torn ligaments.
Knee Injury and the Synovial Membrane
The synovial membrane of the knee joint is extensive, and if the
articular surfaces, menisci, or ligaments of the joint are dam-
wide communication between the suprapatellar bursa and the
joint cavity results in this structure becoming distended also. The
swelling of the knee extends three or four fingerbreadths above
the patella and laterally and medially beneath the aponeuroses
Ligamentous Injury of the Knee Joint
Four ligaments—the medial collateral ligament, the lateral col-
lateral ligament, the ACL, and the PCL—are commonly injured
in the knee. Sprains or tears occur depending on the degree of
force applied.
Medial Collateral Ligament
Forced abduction of the tibia on the femur can result in partial
tearing of the medial collateral ligament, which can occur at its
of the menisci result in localized tenderness on the joint line,
-
derness over the femoral or tibial attachments of the ligament.
Lateral Collateral Ligament
to the lateral collateral ligament (less common than medial liga-
ment injury).
Cruciate Ligaments
Injury to the cruciate ligaments can occur when excessive force
is applied to the knee joint.
are common. It is the most frequently injured
-
tion is more common in women and this may be explained by the
different alignment of the thigh on the leg in women associated
with the wider pelvis. There is also an increased risk in women
during the preovulatory phase of the menstrual cycle, possibly
C L I N I C A L N O T E S
(continued)
Basic Anatomy
503
due to the influence of the female sex hormones.
such as the cruciate ligaments and the menisci, for diagnostic
This technique permits the direct visualization of structures,
into the synovial cavity of the knee joint through a small incision.
Arthroscopy involves the introduction of a lighted instrument
wedged between the articular surfaces, further movement is
length (Fig. 10.63). When the torn part of the meniscus becomes
being subjected to a severe grinding force, and it splits along its
sudden movement between the condyles results in the meniscus
position between the femoral and tibial condyles (Fig. 10.62A). A
the femur, and the medial meniscus is pulled into an abnormal
taking the weight of the body. The tibia is usually abducted on
is rotated on the femur, with the knee joint partially flexed and
injury occurs when the femur is rotated on the tibia, or the tibia
eral ligament of the knee joint, which restricts its mobility. The
probably because of its strong attachment to the medial collat
damaged much more frequently than the lateral, and this is
Injuries of the menisci are common. The medial meniscus is
however, the capsule of the joint and the collateral ligaments be
on the quadriceps femoris muscle is begun at once. Should,
immobilized in slight flexion in a cast, and active physiotherapy
torn cruciate ligaments is not always attempted. The knee is
integrity of the collateral ligaments, operative repair of isolated
largely on the tone of the quadriceps femoris muscle and the
(Fig. 10.62). Because the stability of the knee joint depends
tibia can be made to move excessively backward on the femur
on the femur; with rupture of the posterior cruciate ligament, the
ligament shows that the tibia can be pulled excessively forward
len. Examination of patients with a ruptured anterior cruciate
commonly torn, or the capsule may be damaged. The joint cavity
damage to other knee structures; the collateral ligaments are
Injury to the cruciate ligaments is always accompanied by
Tears of the
PCL are rare.
quickly fills with blood (hemarthrosis) so that the joint is swol-
torn in addition, early operative repair is essential.
Meniscal Injury of the Knee Joint
-
impossible, and the joint is said to “lock.”
Injury to the lateral meniscus is less common, probably
because it is not attached to the lateral collateral ligament of
the knee joint and is consequently more mobile. The popliteus
muscle sends a few of its fibers into the lateral meniscus, and
these can pull the meniscus into a more favorable position dur-
ing sudden movements of the knee joint.
Pneumoarthrography
Air can be injected into the synovial cavity of the knee joint so
that soft tissues can be studied. This technique is based on
the fact that air is less radiopaque than structures such as the
medial and lateral menisci, so their outline can be visualized on
a radiograph (Fig. 10.76).
Arthroscopy
purposes.
cruciate ligament
ruptured posterior
cruciate ligament
ruptured anterior
cruciate ligament
test for posterior
cruciate ligament
r anterior
foot on ground
of fall
direction of impact
direction
medial
meniscus
test fo
A
B
C
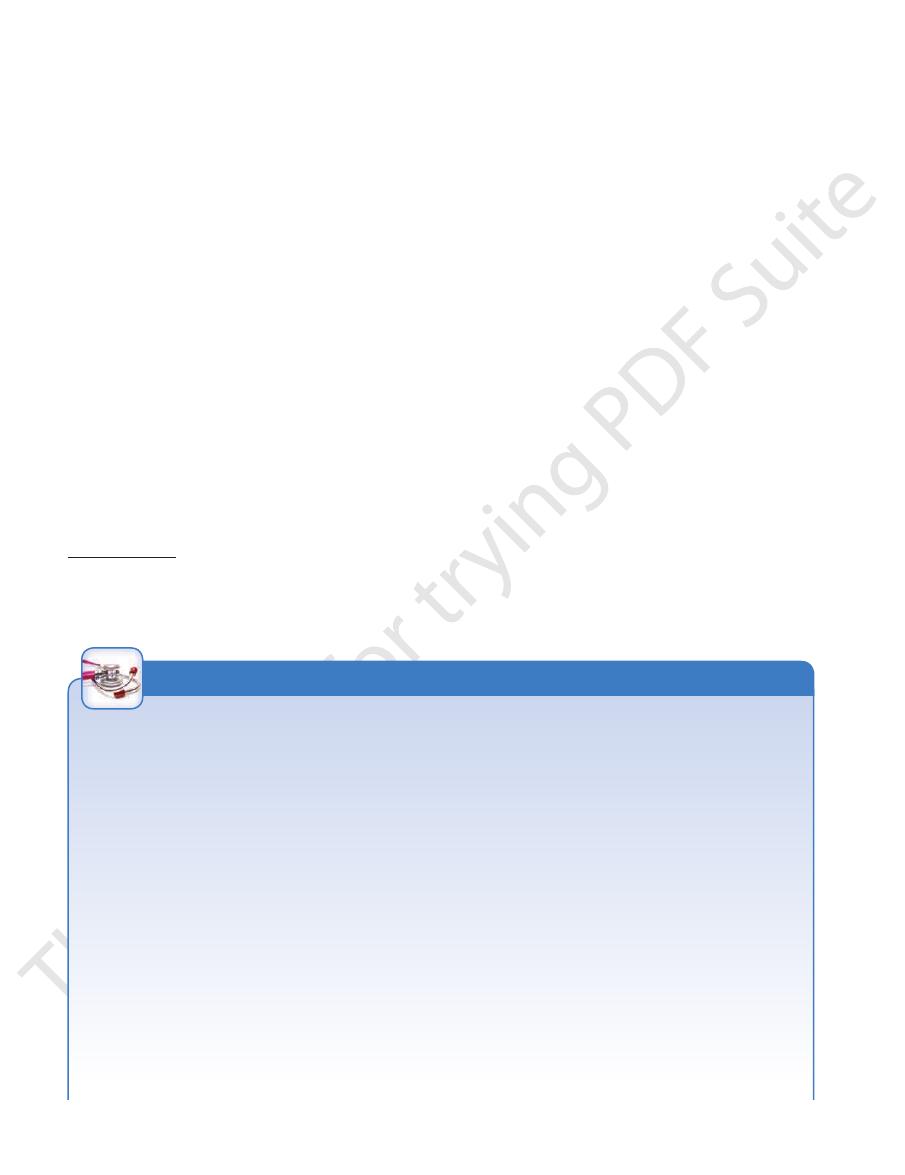
FIGURE 10.62
posterior cruciate ligament (PCL).
Test for integrity of the
Test for integrity of the anterior cruciate ligament (ACL).
ground between the femur and the tibia.
of the tibia on the femur, and the medial meniscus is pulled into an abnormal position. The cartilaginous meniscus is then
right knee joint is semiflexed and that medial rotation of the femur on the tibia occurs. The impact causes forced abduction
Mechanism involved in damage to the medial meniscus of the knee joint from playing football. Note that the
A.
B.
C.

504
CHAPTER 10
The Lower Limb
B
C
medial meniscus
A
D
FIGURE 10.63
Tears of the medial meniscus of the knee
10.65). The opposed bony surfaces are roughened.
of the tibia and the lower end of the fibula (Figs. 10.64 and
Articulation is between the fibular notch at the lower end
Articulation
Distal Tibiofibular Joint
movements at the ankle joint.
A small amount of gliding movement takes place during
Movements
The common peroneal nerve supplies the joint.
Nerve Supply
the margins of the articular surfaces.
The synovial membrane lines the capsule and is attached to
Synovial Membrane
the tibia and fibula together, also greatly strengthens the joint.
which connects the shafts of
interosseous membrane,
The
strengthen the capsule.
posterior ligaments
Anterior
Ligaments
gins of the articular surfaces.
The capsule surrounds the joint and is attached to the mar
This is a synovial, plane, gliding joint.
Type
flattened and covered by hyaline cartilage.
the head of the fibula (Fig. 10.35). The articular surfaces are
Articulation is between the lateral condyle of the tibia and
Articulation
Proximal Tibiofibular Joint
Tear of the anterior portion of
Tear of the posterior
torn from its peripheral attachment.
The meniscus is
Complete bucket handle tear.
joint. A.
B.
C.
portion of the meniscus. D.
the meniscus.
Capsule
-
and
posterior ligament of distal tibiofi
posterior talofibular ligament
calcaneofibular ligament
anterior talofi
anterior ligament of distal tibiofi
fibula
tuberosity of navicular
calcaneonavicular
tibia
medial malleolus
medial (deltoid) ligament
calcaneum
sustentaculum tali
plantar
ligament
talus
tibia
bular joint
talus
bular ligament
bifurcated ligament
dorsal tarsal ligaments
cuboid
dorsal tarsometatarsal ligaments
calcaneum
lateral malleolus
bular joint
A
B
FIGURE 10.64
The right ankle joint as seen from the medial aspect (A) and the lateral aspect (B).

Basic Anatomy
505
calcaneofibular ligament
peroneus brevis
lateral plantar vessels and ner
flexor digitorum brevis
flexor digitorum longus
tibialis posterior
posterior tubercle of talus
posterior talofi
calcaneofibular ligament
inferior transverse ligament
posterior tibiofibular ligament
tibia
interosseous membrane
fibula
lateral malleolus
calcaneum
sustentaculum tali
bular ligament
medial tubercle of talus
medial (deltoid) ligament
capsule
medial malleolus
tibia
medial malleolus
medial (deltoid) ligament
medial plantar vessels and nerve
abductor hallucis
quadratus plantae
abductor digiti minimi
ve
peroneus longus
lateral malleolus
talus
interosseous membrane
fibula
A
B
flexor hallucis longus
sustentaculum tali
FIGURE 10.65
The right ankle joint as seen from the posterior aspect
near their articular margins.
The capsule encloses the joint and is attached to the bones
The ankle is a synovial hinge joint.
Type
covered with hyaline cartilage.
the body of the talus fits snugly. The articular surfaces are
the lower end of the tibia, deepens the socket into which
between the lateral malleolus and the posterior border of
The inferior transverse tibiofibular ligament, which runs
malleoli, and the body of the talus (Figs. 10.64 and 10.65).
Articulation is between the lower end of the tibia, the two
Articulation
rounding tendons make this joint strong and stable.
of the bones and the strength of the ligaments and the sur
move on a transverse axis in a hingelike manner. The shape
upper part of the body of the talus. The talus is able to
lower ends of the tibia and fibula, into which is fitted the
The ankle joint consists of a deep socket formed by the
ments at the ankle joint.
A small amount of movement takes place during move
Movements
Deep peroneal and tibial nerves supply the joint.
Nerve Supply
terior border of the lower end of the tibia.
surface of the upper part of the lateral malleolus to the pos
runs from the medial
inferior transverse ligament
The
and behind the interosseous ligament.
fibrous tissue connecting the two bones together in front
are flat bands of
posterior ligaments
anterior
The
and fibula together, also greatly strengthens the joint.
which connects the shafts of the tibia
osseous membrane,
inter
fibrous tissue that binds the two bones together. The
is a strong, thick band of
interosseous ligament
The
Ligaments
There is no capsule.
The distal tibiofibular joint is a fibrous joint.
Type
(A) and in coronal section (B).
Capsule
-
and
-
-
Ankle Joint
-
Capsule
506
CHAPTER 10
The Lower Limb
Ankle Joint Stability
transversely. Overinversion (without rotation), in which the talus
by forced overeversion (without rotation), in which the talus
still farther, its rotary movement results in its violent contact with
off the tip of the medial malleolus. If the talus is forced to move
fracture spirally. If the force continues, the talus moves laterally,
by forced external rotation and overeversion of the foot. The
Fracture dislocations of the ankle are common and are caused
deep mortise formed by the lower end of the tibia and the medial
The ankle joint is a hinge joint possessing great stability. The
and lateral malleoli securely holds the talus in position.
Acute Sprains of the “Lateral Ankle”
Acute sprains of the lateral ankle are usually caused by exces-
sive inversion of the foot with plantar flexion of the ankle. The
anterior talofibular ligament and the calcaneofibular ligament
are partially torn, giving rise to great pain and local swelling.
Acute Sprains of the “Medial Ankle”
Acute sprains of the medial ankle are similar to but less com-
mon than those of the lateral ankle. They may occur to the medial
or deltoid ligament as a result of excessive eversion. The great
strength of the medial ligament usually results in the ligament
pulling off the tip of the medial malleolus.
Fracture Dislocations of the Ankle Joint
talus is externally rotated forcibly against the lateral malleolus of
the fibula. The torsion effect on the lateral malleolus causes it to
and the medial ligament of the ankle joint becomes taut and pulls
the posterior inferior margin of the tibia, which shears off.
Other less common types of fracture dislocation are caused
presses the lateral malleolus laterally and causes it to fracture
presses against the medial malleolus, produces a vertical frac-
ture through the base of the medial malleolus.
C L I N I C A L N O T E S
Ligaments
tial position for major thrusting movements in walking,
the stability of the ankle joint when the foot is in the ini
distal tibiofibular joint. This arrangement greatly increases
them to separate slightly and tighten the ligaments of the
forced between the medial and lateral malleoli, causing
wider anterior part of the articular surface of the talus is
Note that during dorsiflexion of the ankle joint, the
talofibular ligament.
the anterior fibers of the medial ligament, and the anterior
gus. It is limited by the tension of the opposing muscles,
posterior, flexor digitorum longus, and flexor hallucis lon
soleus, plantaris, peroneus longus, peroneus brevis, tibialis
is performed by the gastrocnemius,
Plantar flexion
the calcaneofibular ligament.
calcaneus, the posterior fibers of the medial ligament, and
peroneus tertius. It is limited by the tension of the tendo
extensor hallucis longus, extensor digitorum longus, and
is performed by the tibialis anterior,
Dorsiflexion
at the ankle joint
inversion and eversion take place at the tarsal joints and
(toes pointing downward) are possible. The movements of
Dorsiflexion (toes pointing upward) and plantar flexion
Movements
Deep peroneal and tibial nerves supply the ankle joint.
Nerve Supply
The synovial membrane lines the capsule.
Synovial Membrane
talus.
from the lateral malleolus to the posterior tubercle of the
(Fig. 10.64) runs
posterior talofibular ligament
The
the lateral surface of the calcaneum.
the tip of the lateral malleolus downward and backward to
(Fig. 10.64) runs from
calcaneofibular ligament
The
talus.
from the lateral malleolus to the lateral surface of the
(Fig. 10.64) runs
anterior talofibular ligament
The
and consists of three bands.
is weaker than the medial ligament
lateral ligament
The
navicular bone.
calcaneonavicular ligament, and the tuberosity of the
side of the talus, the sustentaculum tali, the plantar
the talus; the superficial fibers are attached to the medial
nonarticular area on the medial surface of the body of
(Fig. 10.65). Below, the deep fibers are attached to the
attached by its apex to the tip of the medial malleolus
is strong and is
deltoid, ligament
or
medial,
The
not
.
-
-
running, and jumping.
longus (Fig. 10.48)
rior tibial vessels, the tibial nerve, and the flexor hallucis
tibialis posterior, the flexor digitorum longus, the poste
The
Posteromedially (behind the medial malleolus):
peroneus longus and brevis (Fig. 10.46)
The
Posterolaterally (behind the lateral malleolus):
The tendo calcaneus and plantaris (Fig.
Posteriorly:
tertius (Fig. 10.48)
nerve, the extensor digitorum longus, and the peroneus
longus, the anterior tibial vessels, the deep peroneal
The tibialis anterior, the extensor hallucis
Anteriorly:
Important Relations
possible.
small amounts of rotation, abduction, and adduction are
the ligaments of the distal tibiofibular joint are less taut and
Note also that when the ankle joint is fully plantar flexed,
■
■
■
■
10.48)
■
■
■
■
-
Basic Anatomy
is con
joint cavity
by dorsal and plantar ligaments. The
is strengthened
capsule
vial joint of the gliding variety. The
navicular bone and the three cuneiform bones. It is a syno
between the
articulation
The cuneonavicular joint is the
Cuneonavicular Joint
extensor digitorum longus also assist.
brevis, and peroneus tertius; the lateral tendons of the
Eversion is performed by the peroneus longus, peroneus
digitorum longus; the tibialis posterior also assists.
sor hallucis longus, and the medial tendons of extensor
Inversion is performed by the tibialis anterior, the exten
movement of inversion is more extensive than eversion.
the foot so that the sole faces in the lateral direction. The
is the opposite movement of
Eversion
sole faces medially.
is the movement of the foot so that the
Inversion
joints.
of the foot take place at the subtalar and transverse tarsal
The important movements of inversion and eversion
sal joints
transverse tar
or
midtarsal
are together referred to as the
The talocalcaneonavicular and the calcaneocuboid joints
and Calcaneocuboid Joints
Movements in the Subtalar, Talocalcaneonavicular,
The synovial membrane lines the capsule.
Synovial Membrane
bone (Fig. 10.59).
of the calcaneum and to the adjoining part of the cuboid
that is attached to the anterior tubercle on the undersurface
is a wide, strong ligament
short plantar ligament
The
into a tunnel.
the groove for the peroneus longus tendon, converting it
fourth, and fifth metatarsal bones in front. It bridges over
to the undersurface of the cuboid and the bases of the third,
attached to the undersurface of the calcaneum behind and
the lower surface of the joint (Figs. 10.58 and 10.59). It is
is a strong ligament on
long plantar ligament
The
the navicular bone.
of the cuboid, and the medial limb to the upper surface of
calcaneum. The lateral limb is attached to the upper surface
is attached to the upper surface of the anterior part of the
surface of the joint (Fig. 10.64). It is Y shaped, and the stem
is a strong ligament on the upper
bifurcated ligament
The
Ligaments
The capsule encloses the joint.
The calcaneocuboid joint is synovial, of the plane variety.
Type
articular surfaces are covered with hyaline cartilage.
and the posterior surface of the cuboid (Fig. 10.37). The
Articulation is between the anterior end of the calcaneum
Articulation
Calcaneocuboid Joint
Gliding and rotatory movements are possible.
Movements
The synovial membrane lines the capsule.
Synovial Membrane
cartilage and supports the head of the talus.
The superior surface of the ligament is covered with fibro
the inferior surface and tuberosity of the navicular bone.
runs from the anterior margin of the sustentaculum tali to
is strong and
plantar calcaneonavicular ligament
The
Ligaments
The capsule incompletely encloses the joint.
The joint is a synovial joint.
Type
faces are covered with hyaline cartilage.
concave surface of the navicular bone. The articular sur
upper surface of the sustentaculum tali, and the posterior
Articulation is between the rounded head of the talus, the
Articulation
navicular bone (Fig. 10.37).
between the talus and the calcaneum and also involves the
The talocalcaneonavicular joint is the anterior joint
Talocalcaneonavicular Joint
Gliding and rotatory movements are possible.
Movements
The synovial membrane lines the capsule.
Synovial Membrane
tali and below to the sulcus calcanei.
between the two bones. It is attached above to the sulcus
(Fig. 10.65) is strong and is the main bond of union
interosseous (talocalcaneal) ligament
the capsule. The
strengthen
lateral (talocalcaneal) ligaments
Medial
Ligaments
gins of the articular areas of the two bones.
The capsule encloses the joint and is attached to the mar
These joints are synovial, of the plane variety.
Type
ered with hyaline cartilage.
the calcaneum (Fig. 10.37). The articular surfaces are cov
the talus and the facet on the middle of the upper surface of
Articulation is between the inferior surface of the body of
Articulation
and the calcaneum.
The subtalar joint is the posterior joint between the talus
Subtalar Joint
Tarsal Joints
507
-
Capsule
-
and
-
Capsule
-
Capsule
-
.
-
-
and 4th metatarsal bones.
sal joints, between the bases of the 2nd and 3rd and the 3rd
joints and also with the cuneometatarsal and intermetatar
tinuous with those of the intercuneiform and cuneocuboid
-
-
508
CHAPTER 10
third, as in the hand.
take place from the midline of the second digit and not the
toes, performed by the interossei muscles, are minimal and
The movements of abduction and adduction of the
verse ligaments connect the joints of the five toes.
resemble those of the hand (see page 412). The deep trans
The metatarsophalangeal and interphalangeal joints closely
sal joint of the big toe has a separate joint cavity.
sal, plantar, and interosseous ligaments. The tarsometatar
joints of the plane variety. The bones are connected by dor
The tarsometatarsal and intermetatarsal joints are synovial
Tarsometatarsal and Intermetatarsal
ligaments.
bones are connected by dorsal, plantar, and interosseous
continuous with that of the cuneonavicular joint. The
vial joints of the plane variety. Their joint cavities are
The intercuneiform and cuneocuboid joints are syno
Intercuneiform and Cuneocuboid Joints
ous ligaments.
the two bones connected by dorsal, plantar, and interosse
The cuboideonavicular joint is usually a fibrous joint, with
Cuboideonavicular Joint
The Lower Limb
-
-
Joints
-
-
Metatarsophalangeal and
Interphalangeal Joints
-
Later, osteoarthritic changes occur in the metatarsophalan
which is a lateral deviation of the great toe
Metatarsophalangeal Joint of the Big Toe
Hallux valgus,
at the metatarsophalangeal joint, is a common condition. Its
incidence is greater in women than in men and is associated
with badly fitting shoes. It is often accompanied by the pres-
ence of a short 1st metatarsal bone. Once the deformity is
established, it is progressively worsened by the pull of the
flexor hallucis longus and extensor hallucis longus muscles.
-
geal joint, which then becomes stiff and painful; the condition
is then known as hallux rigidus.
C L I N I C A L N O T E S
The Foot as a Functional Unit
assist the forward propulsive action of the gastrocnemius
and toes (i.e., the takeoff point of the foot) and greatly
exert their action on the bones of the forepart of the foot
long flexor muscles and the small muscles of the foot can
able and can adapt itself to uneven surfaces. Moreover, the
the lever is segmented with multiple joints, the foot is pli
activities of the gastrocnemius and soleus muscles. Because
forward propulsive action would depend entirely on the
the foot could not adapt itself to uneven surfaces, and the
pulsion (Fig. 10.66). However, with such an arrangement,
body weight and serve well as a rigid lever for forward pro
bone instead of a series of small bones, it could sustain the
walking and running. If the foot possessed a single strong
weight and to serve as a lever to propel the body forward in
The foot has two important functions: to support the body
The Foot as a Weight Bearer
and a Lever
-
-
and soleus muscles (Fig. 10.66).
the following engineering methods used for its support
Examination of the design of any stone bridge reveals
Mechanisms of Arch Support
bones (Fig. 10.67).
atarsal bones and the cuboid and the three cuneiform
This consists of the bases of the met
Transverse arch:
(Fig. 10.67).
neum, the cuboid, and the 4th and 5th metatarsal bones
This consists of the calca
Lateral longitudinal arch:
bones, and the first three metatarsal bones (Fig. 10.63).
neum, the talus, the navicular bone, the three cuneiform
This consists of the calca
Medial longitudinal arch:
graph of the foot shows the bones that form the arches.
An examination of an articulated foot or a lateral radio
The Bones of the Arches
metatarsals.
of the first metatarsal and the heads of the remaining four
in front, namely, the two sesamoid bones under the head
the heel behind and six points of contact with the ground
body weight on standing is distributed through a foot via
From this description, it can be understood that the
the two feet are placed together, a complete dome is formed.
likened to a half-dome, so that when the medial borders of
its summit on the foot’s medial border. The foot has been
an arch, with its base on the lateral border of the foot and
the cuboid and cuneiform bones. This is, in fact, only half
transverse arch involves the bases of the five metatarsals and
the presence of the low-lying lateral longitudinal arch. The
5th metatarsal head and least between these areas because of
the lateral margin of the foot is greatest at the heel and the
longitudinal arch. The pressure exerted on the ground by
arched above the ground because of the important medial
gin of the foot, from the heel to the 1st metatarsal head, is
are in contact with the ground (Fig. 10.67). The medial mar
the metatarsal heads, and the pads of the distal phalanges
that the heel, the lateral margin of the foot, the pad under
made with the person in the standing position, one can see
On examination of the imprint of a wet foot on the floor
a large amount of subcutaneous fat on the sole of the foot.
child, the foot appears to be flat because of the presence of
(Fig. 10.67). In the young
transverse arches
and
medial longitudinal, lateral longi
are present at birth: the
in the form of an arch. The foot has three such arches, which
A segmented structure can hold up weight only if it is built
The Arches of the Foot
-
tudinal,
-
-
■
■
-
■
■
-
■
■
-
(Fig. 10.68):
with the thin edge of the wedge lying inferiorly. This
porting the arch is to make the stones wedge shaped,
The most effective way of sup
The shape of the stones:
■
■
-