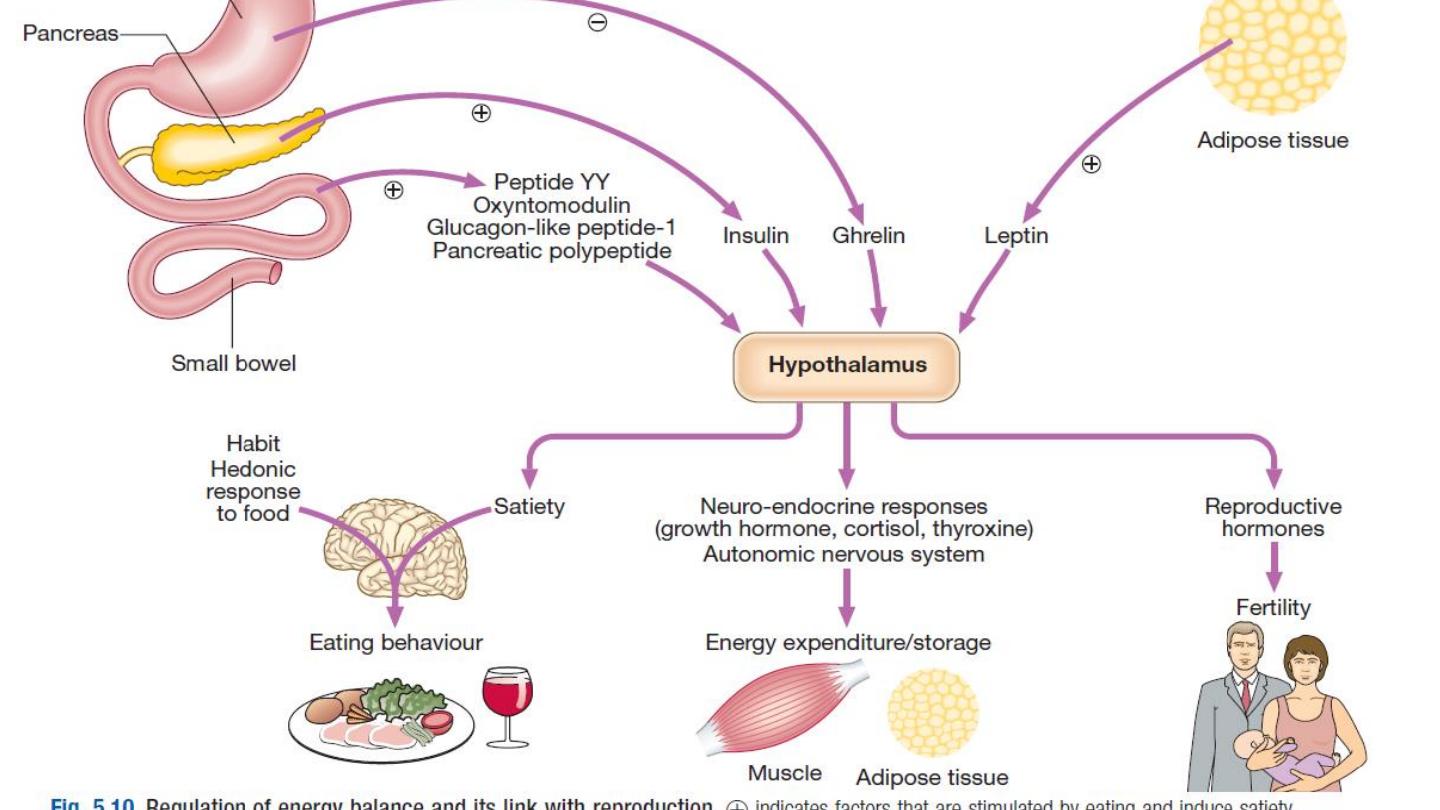
Nutrients
the
diet can be classified into ‘
macronutrients
’,
which are eaten in relatively large amounts to
provide fuel for energy, and ‘
micronutrients
’ (e.g.
vitaminsand minerals), which do not contribute to
energy balance but are required in small amounts
because they are not synthesised in the body.

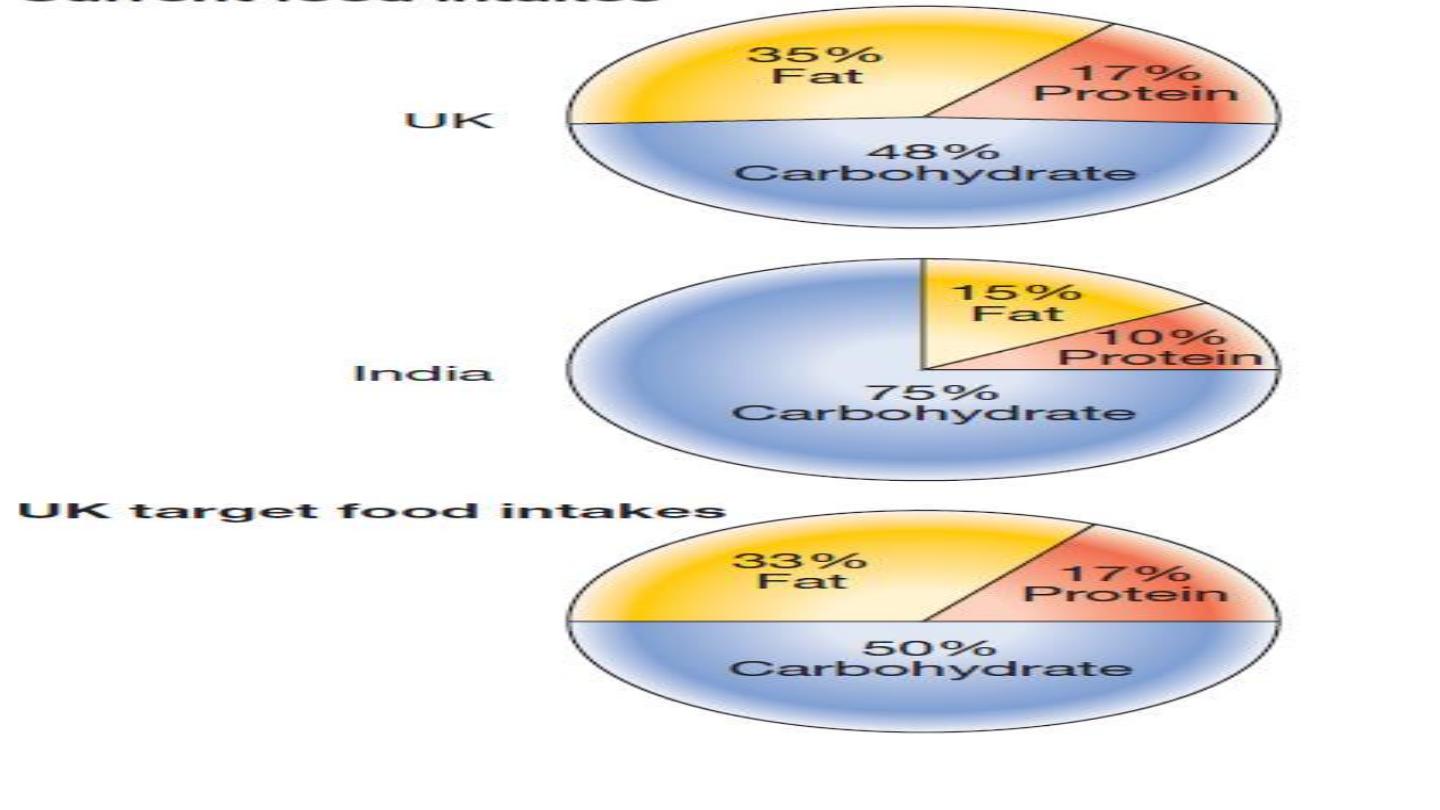
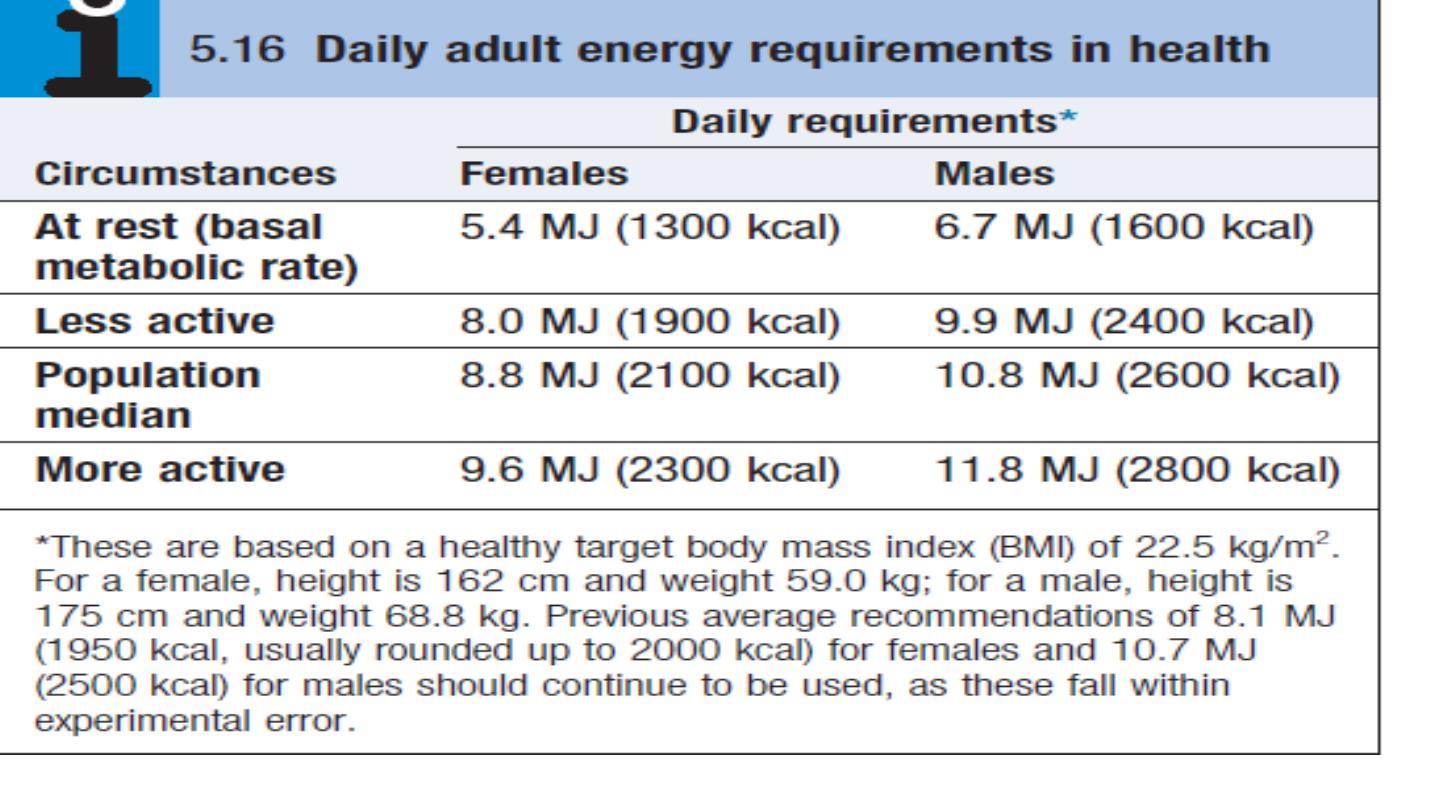
Energy intake is determined by the ‘macronutrient’
content of food. Carbohydrates, fat, protein and alcohol
provide fuel for
oxidation in the mitochondria
to
generate
energy (as adenosine triphosphate (
ATP)
. The
energy provided by each of these elements differs:
•
carbohydrates
(16 kJ/g)
•
fat
(37 kJ/g)
•
protein
(17 kJ/g)
•
alcohol
(29 kJ/g).

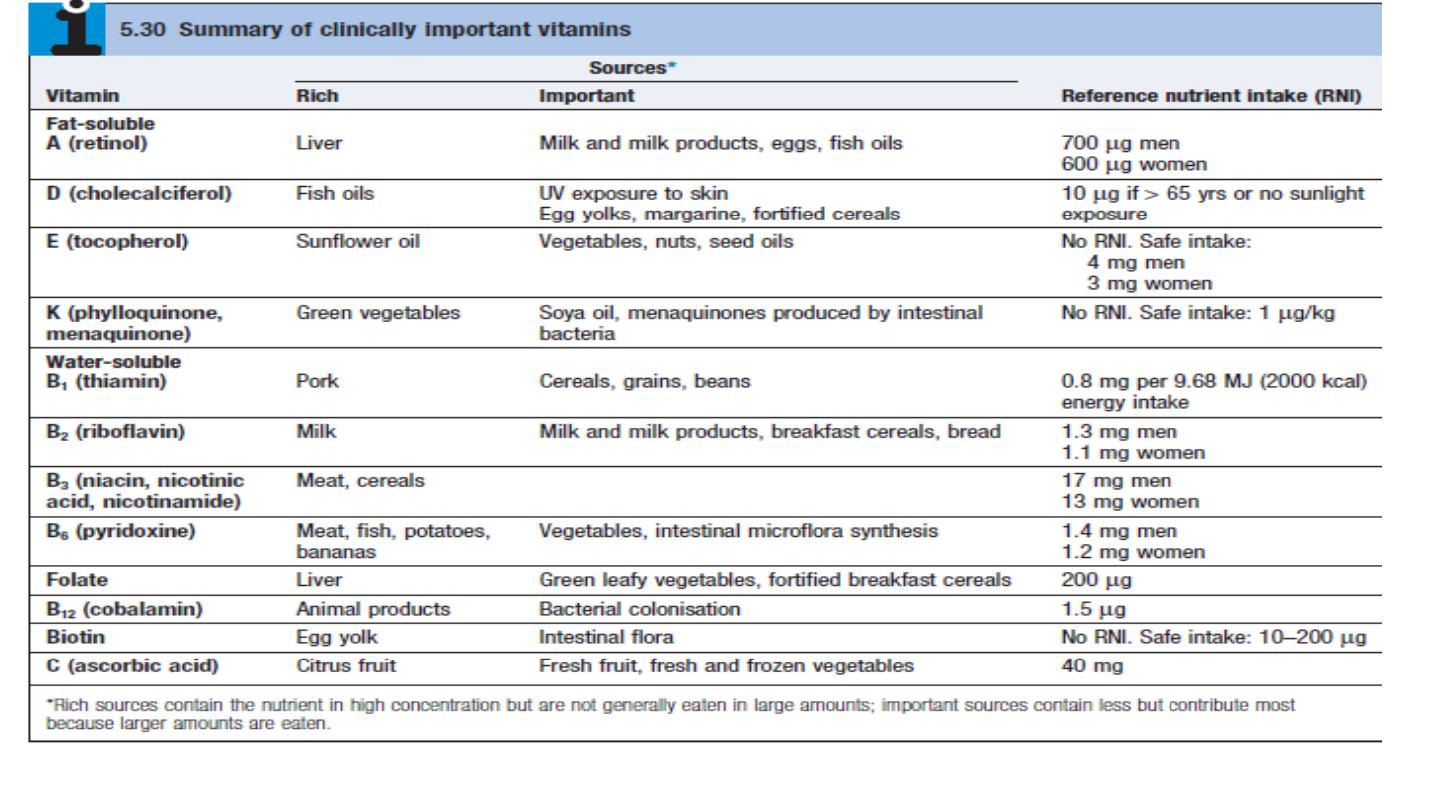
Vitamins
are organic substances with key
roles in certain
metabolic pathways, and are categorised into
those that
are fat-soluble (vitamins A, D, E and K) and those
that
are water-soluble (vitamins of the B complex
group and
vitamin C).
Vitamin A (retinol)
Pre-formed retinol is found only in foods of animalorigin. Vitamin A can also be derived from
carotenes,
which are present
in green and coloured vegetables and some fruits
. Carotenes provide most of
the total
vitamin A in the UK, and constitute the only supply invegans. Retinol is converted to several
other important
molecules:
•
11-cis retinaldehyde
is part of the photoreceptor complex in rods of the retina
.
•
Retinoic acid induces
differentiation of epithelial
cells by binding to specific nuclear receptors, which
induce responsive genes. In vitamin A deficiency,
mucus-secreting cells are replaced by keratinproducing
cells.
• Retinoids are necessary for normal growth, fetal
development, fertility, haematopoiesis and immune
function.
Globally
, the most important consequence of
vitamin A deficiency is irreversible blindness in young
children.
Asia is most notably affected and the problem
is being addressed through widespread vitamin Asupplementation
programmes. Adults are not usually at
risk because liver stores can supply vitamin A when
foods containing vitamin A are unavailable
.

Early deficiency causes impaired adaptation to thedark (
night
blindness
). Keratinisation of the cornea
(
xerophthalmia
) gives rise to characteristic
Bitot’s spots
, and progresses to
keratomalacia
, with corneal ulceration,
scarring and irreversible blindness ).
Incountries where vitamin A deficiency is endemic, pregnant women should be advised to eat dark-green, leafy
vegetables and yellow fruits (to build up stores of retinol in the fetal liver), and infants should be fed the same.
WHO is according high priority to prevention in communities where xerophthalmia occurs, giving single
prophylactic oral doses of 60 mg retinyl palmitate (providing200 000 U retinol) to pre-school children.
Thisalso reduces mortality from gastroenteritis and respiratory
infections.


Repeated moderate or
high doses
of retinol can cause
liver damage
,
hyperostosis
and
teratogenicity
.
Women
in countries where deficiency is
not endemic
are therefore
advised not to take vitamin A supplements in pregnancy
.
Retinol intake may also be restricted in those at
risk of osteoporosis.
Acute overdose leads to nausea and
headache, increased intracranial pressure and skin
desquamation.
Excessive intake of carotene can cause pigmentation
of the skin (
hypercarotenosis
); this gradually
fades when intake is reduced.
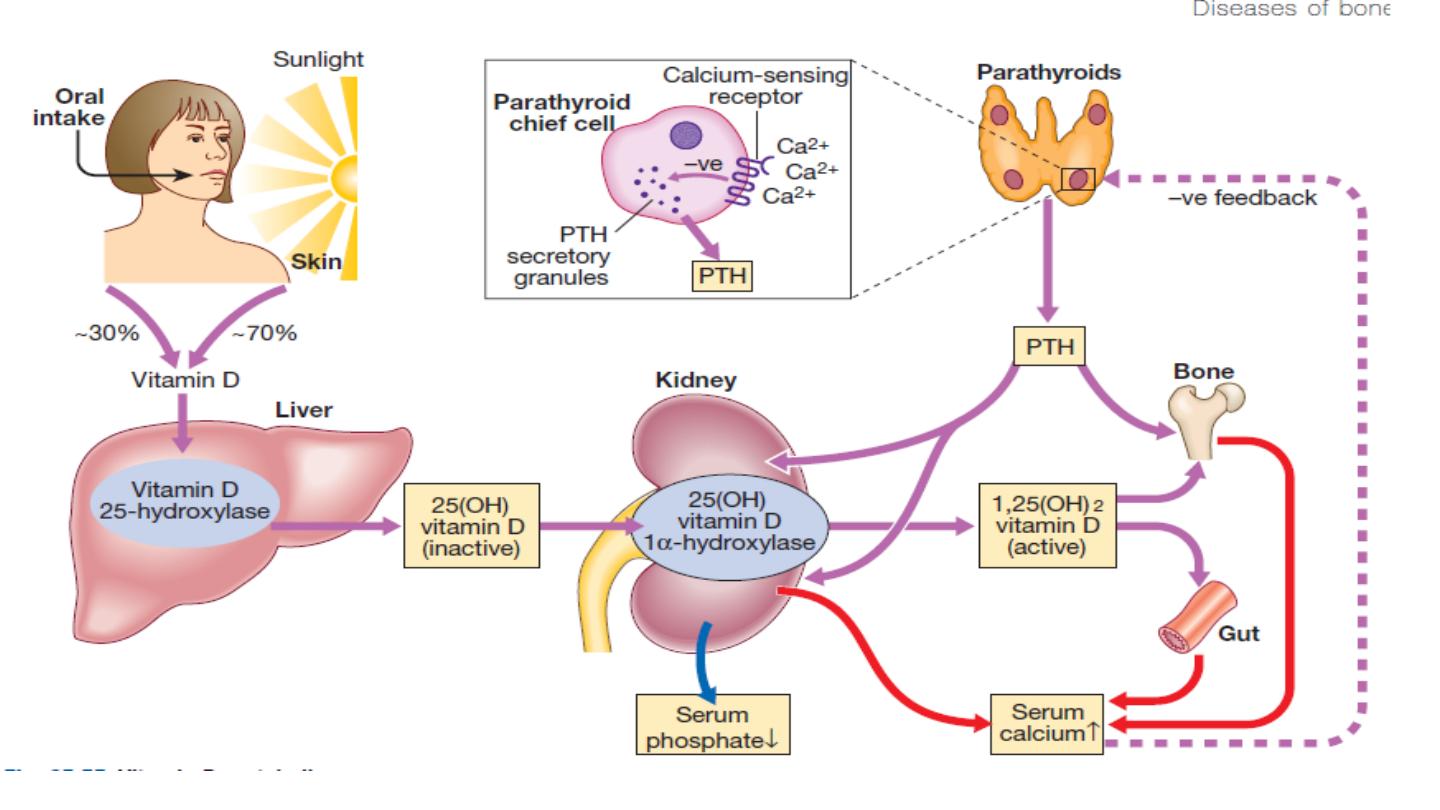
The natural form of vitamin D
, cholecalciferol or
vitaminD
3
, is formed in the skin by the action of UV light on
7-dehydrocholesterol, a metabolite of cholesterol. Fewfoods contain vitamin D naturally and skin exposure to
sunlight is the main source. Moving away from theequator, the intensity of UV light decreases, so that at
a latitude above 50
° (including northern Europe),
vitamin D is not synthesised in winter, and even above
30
° there is seasonal variation.
The body store accumulated
during the summer is consumed during the winter.
Vitamin D is converted in the liver to 25-hydroxy vitamin
D (25(OH)D), which is further hydroxylated in thekidneys to 1,25-dihydroxy-vitamin D (1,25 (OH)
2
D), the
active form of the vitamin
1,25(OH)
2
D activates specific intracellular receptorswhich influence calcium metabolism, bone mineralisation
and tissue differentiation. The synthetic form
, ergocalciferol, or vitamin D
2
, is considered to be less potent
than the endogenous D
3
.

The effects of vitamin D deficiency (calcium
deficiency,
rickets and
osteomalacia
) are described on An
analogue of vitamin D (calcipotriol) is used for
treatment of skin conditions such as psoriasis.
Excessive
doses of cholecalciferol, ergocalciferol or the
hydroxylated
metabolites cause hypercalcaemia

-
Vitamihasn E
αtocopherol. many direct metabolic
actions:
• It prevents
oxidation of polyunsaturated
fatty acids
in cell membranes by free radicals.
1
helps maintain cell membrane structure
.
2
DNA synthesis
and cell signalling.
3
anti-inflammatory and immunesystems
.

Human deficiency is rare and has only been
described
in premature infants and in malabsorption. It can
cause a mild
haemolytic anaemia, ataxia
and
scotomas. visual
Vitamin K
is supplied in the diet mainly as
vitamin K
1
Gla(phylloquinone
) in the UK, or as vitamin
K
2
(menaquinone)
from fermented products in parts of Asia. Vitamin
K
2
is also synthesised by bacteria in the colon
. Vitamin
K is a co-factor
for carboxylation reactions
: in particular,
the production of
γ-carboxyglutamate (gla).
residues are found in four of the coagulation factor proteins
(II, VII, IX and X; , conferring their capacity
to bind to phospholipid surfaces in the presence of
calcium
. Other important gla proteins are osteocalcin
and matrix gla protein, which are important in bone
mineralisation

Vitamin K deficiency leads to
delayed coagulation
and bleeding.
In obstructive jaundice,
dietary vitamin K
is not absorbed and it is essential to administer the
vitamin in parenteral
form before surgery.
Warfarin and
related anticoagulants act by antagonising
vitamin K. Vitamin K is given routinely to newborn
babies to prevent haemorrhagic disease.
Symptoms of
excess have been reported only in infants, with synthetic
preparations linked to haemolysis and liver damage
Water-soluble vitamins
Thiamin (vitamin B1 )
Thiamin is widely distributed in foods of both vegetableand
animal origin. Thiamin pyrophosphate (TPP) isa co-factor for
enzyme reactions involved in themetabolism of macronutrients
(carbohydrate, fat andalcohol), including
• decarboxylation of pyruvate to acetyl-co-enzyme A,
which bridges between glycolysis and the
tricarboxylic acid (Krebs) cycle
• transketolase activity in the hexose monophosphate
shunt pathway
• decarboxylation of α-ketoglutarate to succinate in
the Krebs cycle.

In thiamin deficiency, cells cannot metabolise
glucoseaerobically to generate energy as
ATP. Neuronal cellsare most vulnerable,
since they depend almost exclusivelyon
glucose for energy requirements
.
Impaired
glucose oxidation
also causes an
accumulation ofpyruvic and lactic acids,
which produce vasodilatationand increased
cardiac output
.
Deficiency
– beri-beri
In the developed world, thiamin deficiency is
mainlyencountered in chronic
alcoholics. Poor diet,
impairedabsorption, storage
and phosphorylation of
thiamin inthe liver, and the increased requirements for
thiamin to metabolise ethanol all contribute. In the
developingworld, deficiency usually arises as a
consequence of adiet based on polished rice. The body
has very limitedstores of thiamin, so deficiency is manifest
after only
1month
on a thiamin-free diet. There are two
forms of thedisease in adults:
•
Dry (or neurological) beri-beri
manifests with chronic
peripheral neuropathy and with wrist and/or foot
drop, and may cause
Korsakoff’s psychosis
and
Wernicke’s encephalopathy
•
Wet (or cardiac) beri-beri
causes generalised oedema
due to biventricular heart failure with pulmonary
congestion.
In dry beri-beri, response to thiamin administration
is not uniformly good. However
,
multivitamin therapy
seems to produce some improvement, suggesting
that other vitamin deficiencies may be involved.
Wernicke’s encephalopathy and wet beri-beri should
be treated without delay with intravenous vitamin B
and C mixture (‘Pabrinex’,
Korsakoff’s psychosis
is irreversible and does not respond to thiamin
A rare but important effect of chronic alcohol misuse
is
the Wernicke
–Korsakoff syndrome
. This organic brain
disorder results from damage to the mamillary bodies,
dorsomedial nuclei of the thalamus and adjacent areas
of periventricular grey matter caused by a deficiency of
thiamin (vitamin B
1
), which most commonly results
from long-standing heavy drinking and an inadequate
diet. It can also arise from malabsorption or even protracted
vomiting. Without prompt treatment (see below),
the acute presentation of Wernicke’s encephalopathy
(nystagmus, ophthalmoplegia, ataxia and confusion
)
can progress to the irreversible deficits of
Korsakoff’s
syndrome (severe short-term memory deficits and
confabulation, and also reduced red blood cell transketolase).
In those who die in the acute stage, microscopic
examination of the brain shows hyperaemia,
petechial haemorrhages and astrocytic prolifera
Riboflavin (vitamin B
2
)
Riboflavin is required for the
flavin co-factors
involved
in oxidation
–reduction reactions. It is widely
distributed
in
animal and vegetable foods
. Levels are low in staple
cereals but germination increases its content. It is
destroyed under alkaline conditions
by heat and by
exposure to sunlight.
Deficiency is rare in developed countries. It mainly
affects the tongue and lips and manifests as
glossitis,
angular stomatitis
and
cheilosis.
The genitals may be
affected, as well as the skin areas rich in sebaceous
glands, causing
nasolabial or facial dyssebacea
.
Rapid

Niacin (vitamin B
3
)
Niacin encompasses
nicotinic acid and nicotinamide
. Nicotinamide is an essential part of the two
pyridinenucleotides,
nicotinamide adenine dinucleotide (NAD
) and
nicotinamide adenine dinucleotide phosphate
(NADP),
which play a key role as hydrogen acceptors and donors for many enzymes. Niacin can be synthesised
in the body in limited amounts from the aminoacid tryptophan
.
Deficiency
– pellagra
Pellagra was formerly endemic among poor people whosubsisted chiefly on maize, which contains niacytin, a
form of niacin that the body is unable to utilise. Pellagracan develop in
only 8 weeks
in individuals eating
diets
that are very deficient in niacin and tryptophanremains a problem in parts of Africa
, and is occasionally
seen in
alcoholics
and in patients with
chronic smallintestinal disease
in developed countries.
Pellagra canoccur in
Hartnup’s disease
, a genetic disorder characterisedby impaired absorption of several
amino acids, including tryptophan.
It is also seen occasionally in
carcinoid syndrome
, when tryptophan is consumed
in the excessive production of
5-hydroxytryptamine(5-HT).
Pellagra has been called the disease of the
three D
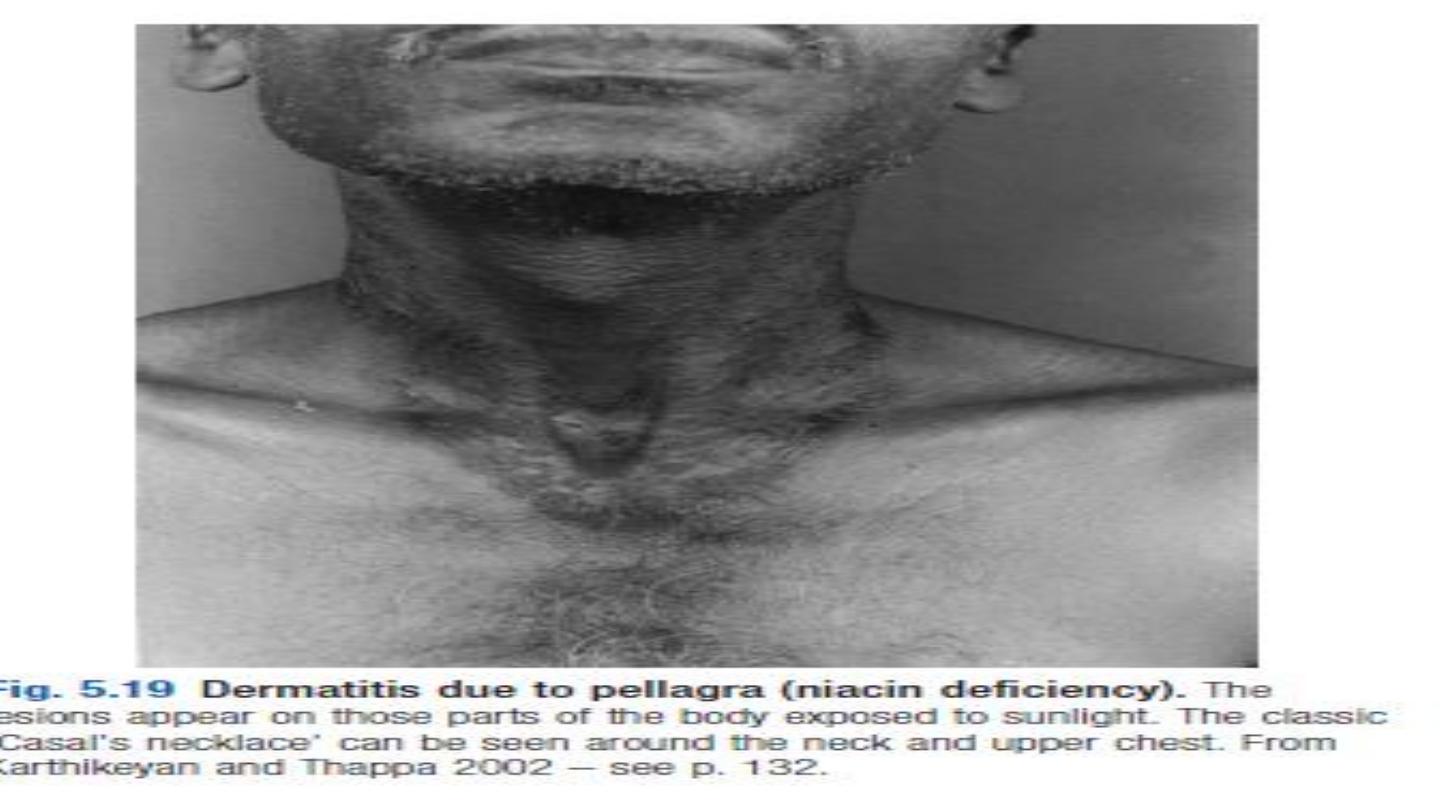

•
Dermatitis
.
Characteristically, there is erythema resembling severe
sunburn, appearing symmetrically over the parts of the body exposed to
sunlight, particularly the limbs and especially on the neck, but not the
face (
Casal’s necklace,
The skin lesions may progress tovesiculation, cracking, exudation and
secondaryinfection.
•
Diarrhoea
. This is often associated with anorexia, nausea, glossitis
and dysphagia, reflecting thepresence of a non-infective inflammation
thatextends throughout the gastrointestinal tract.
•
Dementia
. In severe deficiency, delirium occursacutely and dementia
develops in chronic cases
.

Toxicity
Excessive intakes of niacin may lead to
reversible
hepatotoxicity
.
Nicotinic acid is a lipid-lowering agent,
but at doses above 200 mg a day gives
rise to vasodilatory symptoms (‘
flushing
’
and/or
hypotension
)
Pyridoxine (vitamin B
6
)
Pyridoxine, pyridoxal and pyridoxamine are differentforms of vitamin B
6
that undergo phosphorylation to
produce pyridoxal 5-phosphate (PLP). PLP is theco-factor for a large number of enzymes involved in the
metabolism of amino acids. Vitamin B
6
is available inmost foods.
Deficiency is rare, although certain drugs, such
asisoniazid and penicillamine
, act as chemical antagonists
to pyridoxine.
Pyridoxine administration is effectivein isoniazid-induced
peripheral neuropathy
and some
cases of
sideroblastic anaemia
.
Large doses of vitaminB
6
have
an antiemetic effect in radiotherapy-induced
nausea
.
Although vitamin B
6
supplements have become popular in the treatment of nausea in pregnancy, carpal
tunnel syndrome and premenstrual syndrome, there is no convincing evidence of benefit.
Very high doses
ofvitamin B
6
taken for several months can cause a
sensorypolyneuropathy
.
Biotin
Biotin is a co-enzyme in the synthesis of
fatty
acids,
isoleucine and valine and is also involved in
gluconeogenesis
Deficiency results from consuming very large
quantities of raw egg whites
(> 30%
energy
intake)
because
the
avidin
they contain binds to and
inactivatesbiotin in the intestine. It may also be
seen after long periods of total parenteral
nutrition. The clinical features of deficiency include
scaly dermatitis, alopecia and paraesthesia
.
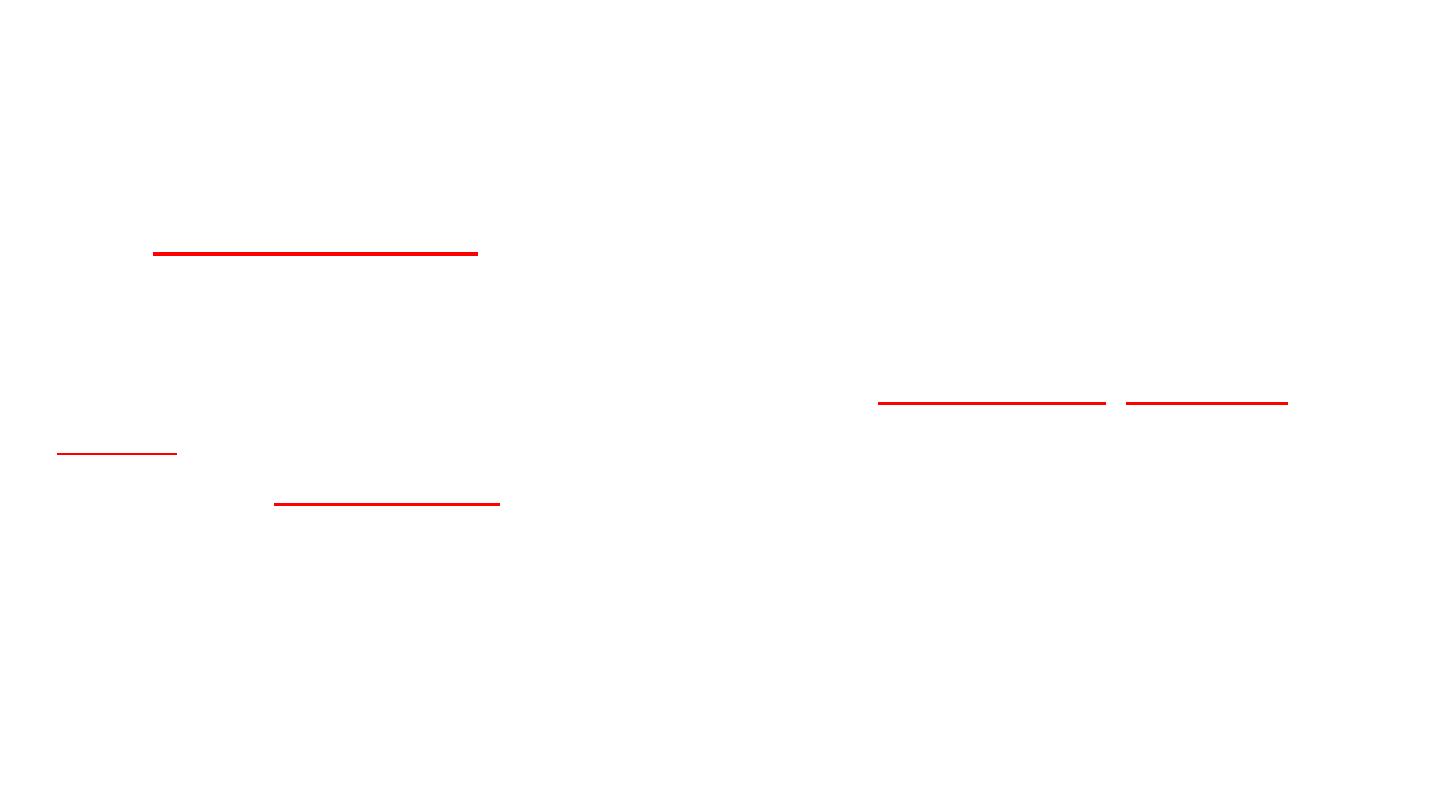
Folate (folic acid)
Folates exist in many forms. The main circulating formis
5-
methyltetrahydrofolate.
Folic acid is the stable synthetic form. Folate works
as a methyl donor for cellular methylationand protein synthesis. It is
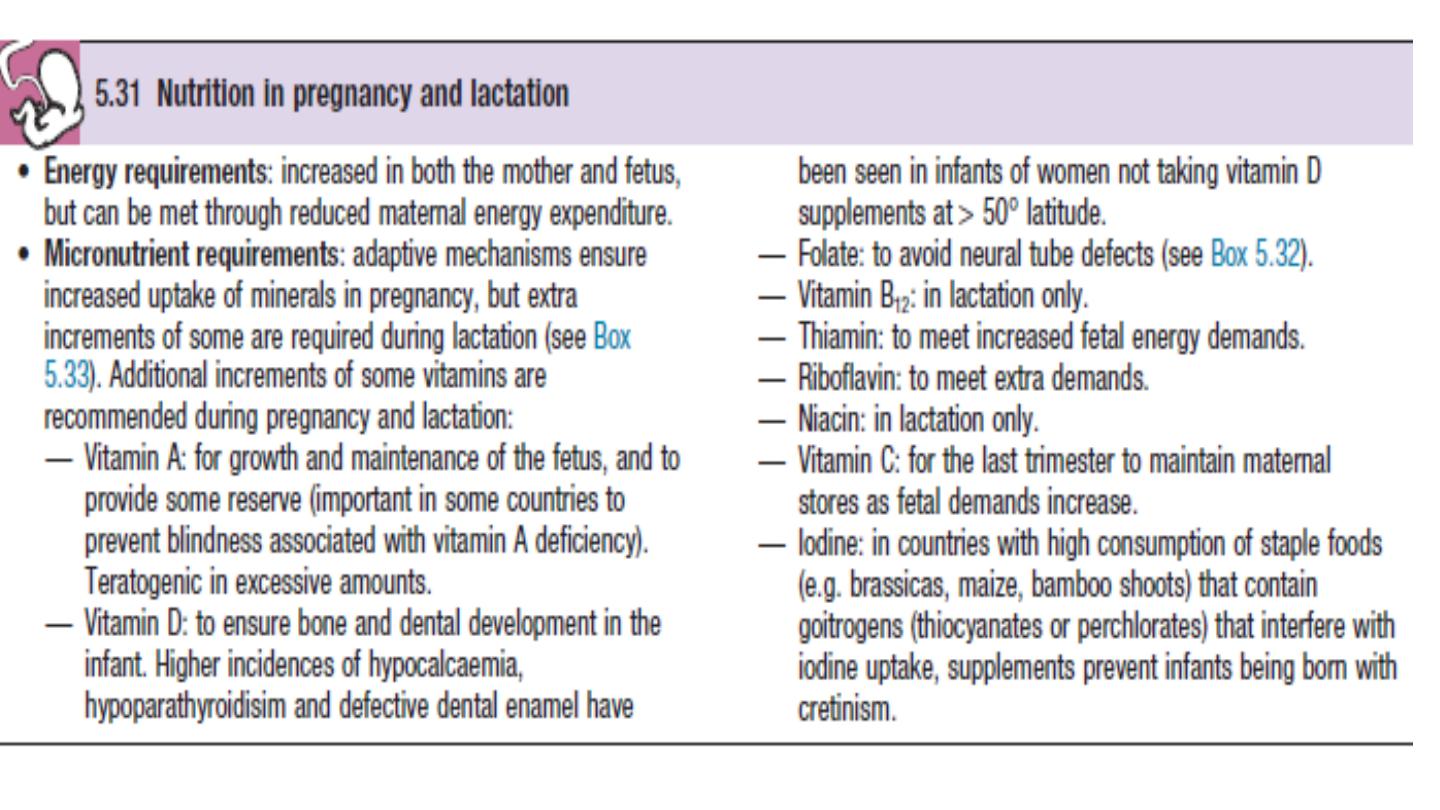
directly involved in DNAand RNA synthesis, and requirements increase
during embryonic development
Folate deficiency may cause three major birth defects
(
spina bifida, anencephaly and encephalocele
) resulting
from imperfect closure of the neural tube, which
takesplace 3
–4
weeks
after conception.
Departmentof Health advises that women who have experienced a
pregnancy affected by a neural tube defect should
take5 mg
of folic acid daily
from before conception andthroughout the first trimester
All
women planning a pregnancy are advised to include good sources of
folate in their diet, and to take folate supplements throughout the first
trimester. Liver is the richest source of folate but an alternative source
(e.g.
leafy vegetables
) is advised in early pregnancy because of the
high vitamin A content of liver
Folate deficiency also has been associated with
heart disease
,
dementia
and
cancer.
. There are now concerns that this may contribute to the increased
incidence of
colon cancer
through promotion of the growth of polyps.
Hydroxycobalamin (vitamin B
12
)
Vitamin B
12
is a co-factor in folate co-enzyme recyclingand nerve myelination. Vitamin B
12
and
folate are particularlyimportant in DNA synthesis in red blood cells
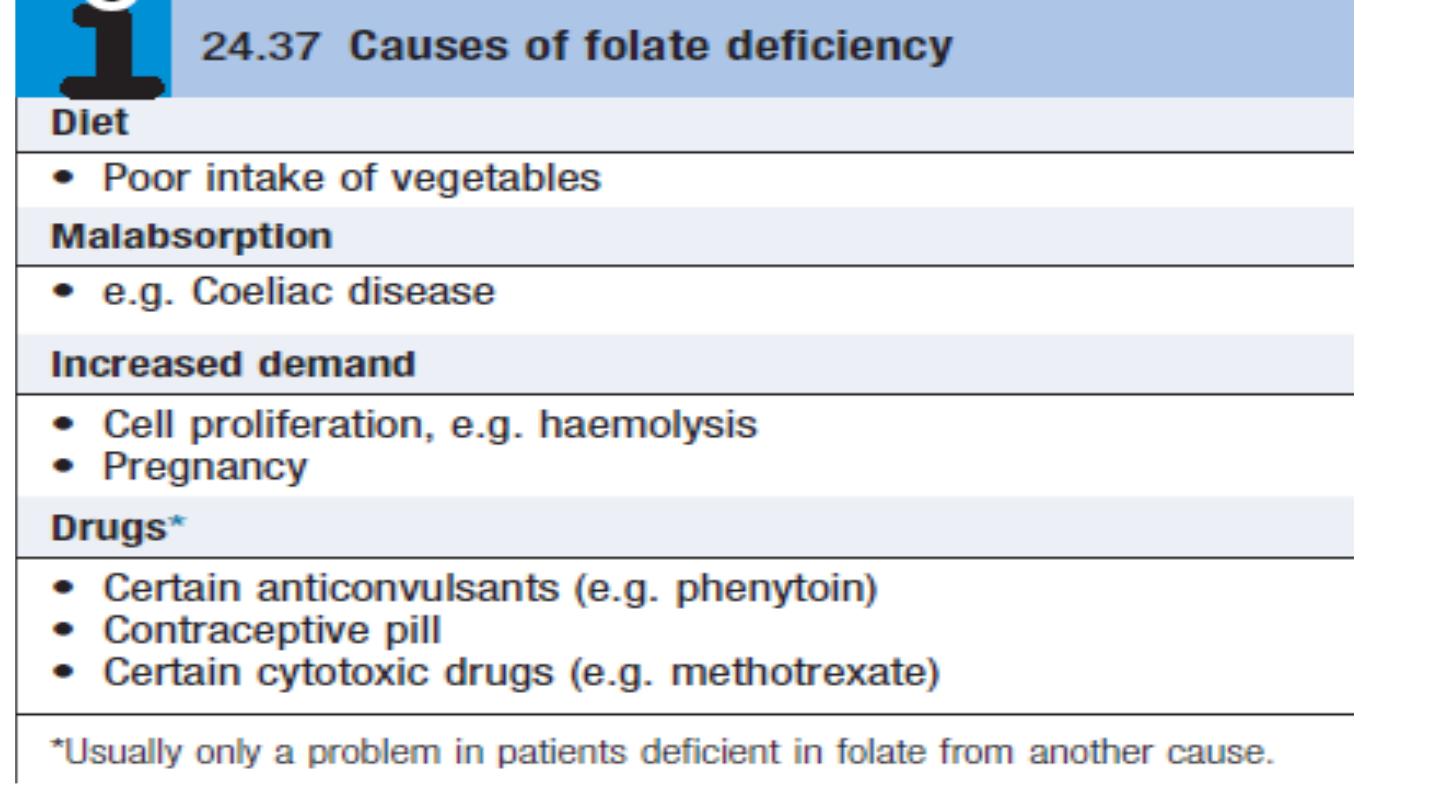
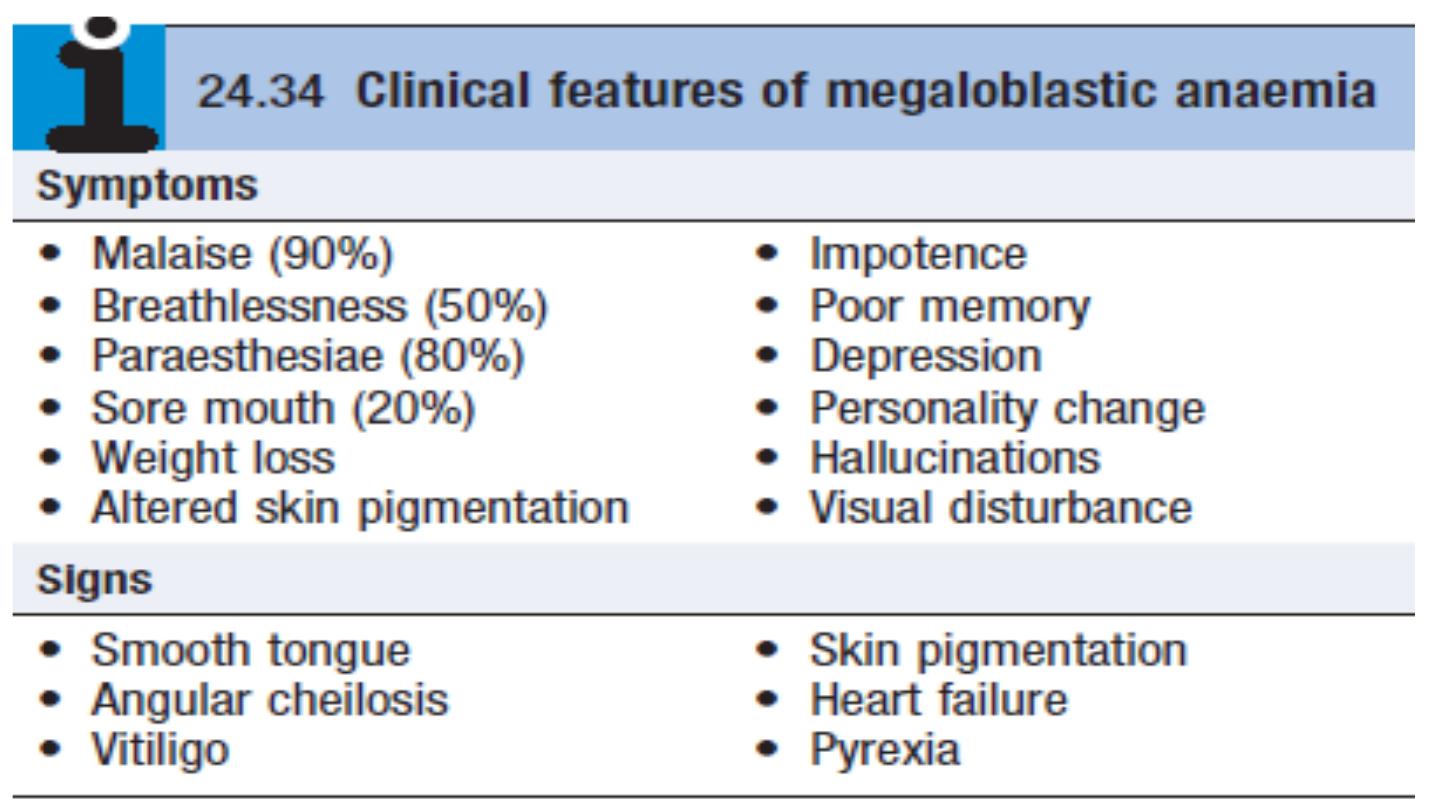
The haematological disorders (macrocytic ormegaloblastic anaemias) due to their deficiency
are discussedon . Vitamin B
12
, but not folate, is needed for the integrity of myelin, so that
vitamin B
12
deficiency is also associated with neurological disease
Neurological consequences of vitamin B
12
deficiency
.
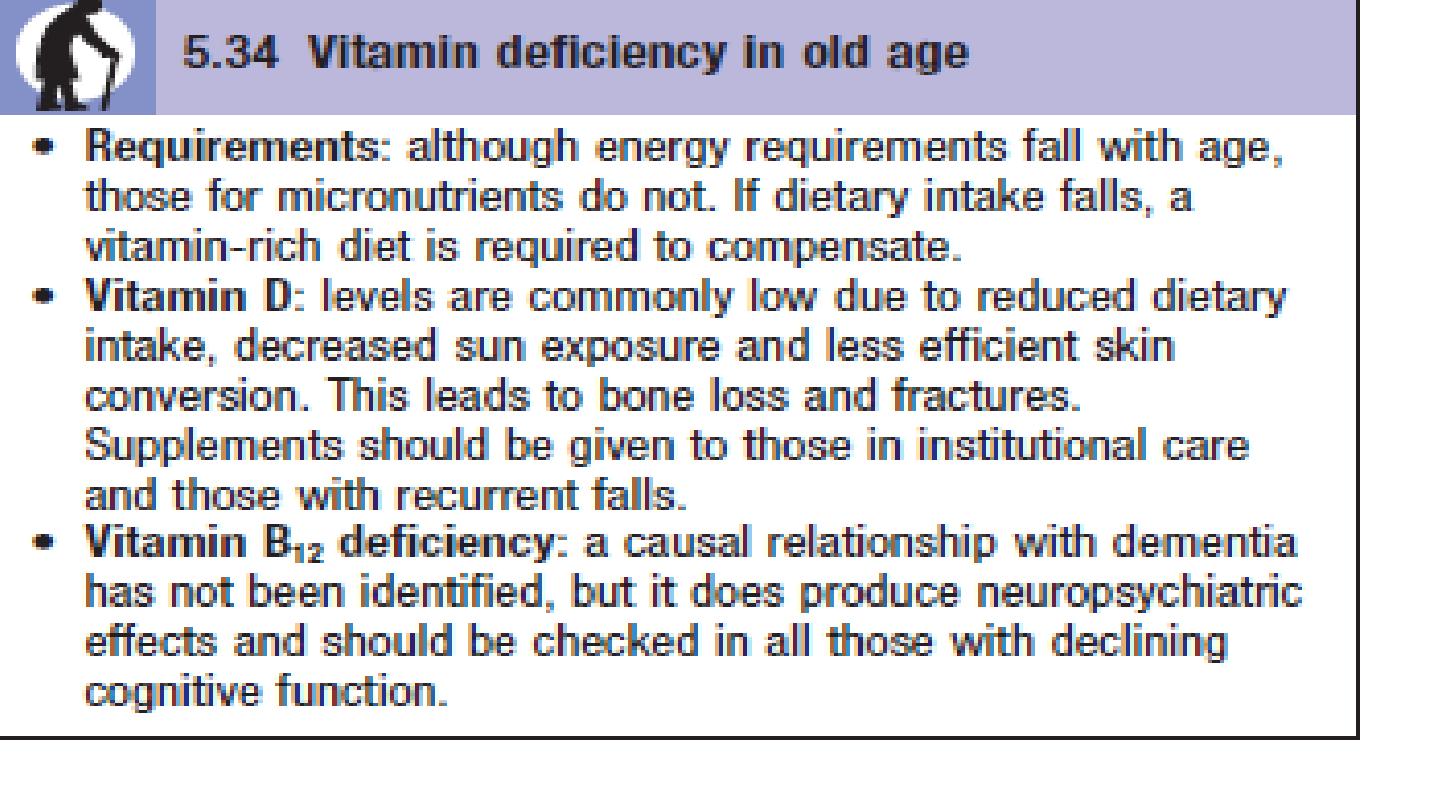
In older people and
chronic alcoholics
, vitamin B
12
deficiencyarises from
insufficient intake and/or frommalabsorption. Several drugs, including
neomycin, canrender vitamin B
12
inactive
.
Adequate intake of folatemaintains
erythropoiesis
and there is a concern
that fortification of foods with folate may mask underlyingvitamin B
12
deficiency. In severe deficiency there is insidious, diffuse and uneven
demyelination
. It may be clinically manifest
as peripheral neuropathy
or
spinalcord degeneration
affecting
both posterior and lateral columns
(‘
subacute combined degeneration of the spinal
cord’ or there may be cerebral
manifestations(resembling dementia) or optic
atrophy
.
Vitamin B
12
therapy improves symptoms in most cases
.

The average daily diet contains 5
–30 μg of vitamin B
12
,
mainly in
meat, fish, eggs and milk
– well in excess of
the 1
μg daily requirement. In the stomach, gastric
enzymes release vitamin B
12
from food and at
gastric pH
it
binds to a carrier protein termed R protein
. The gastric
parietal cells produce
intrinsic factor
, a vitamin B
12
-
binding protein which optimally binds vitamin B
12
at pH
8. As gastric emptying occurs, pancreatic secretion raises
the pH and vitamin B
12
released from the diet switches
from the R protein to intrinsic factor.
Bile also contains
vitamin B
12
which is available for reabsorption in the
intestine
. The vitamin B
12
–intrinsic factor complex binds
to specific receptors in the terminal ileum, and vitamin
B
12
is actively transported by the enterocytes to plasma

where it binds to transcobalamin II, a transport protein
produced by the liver, which carries it to the tissues for
utilisation.
The liver stores enough vitamin B12 for
3 years and this, together with the enterohepatic
circulation,
.
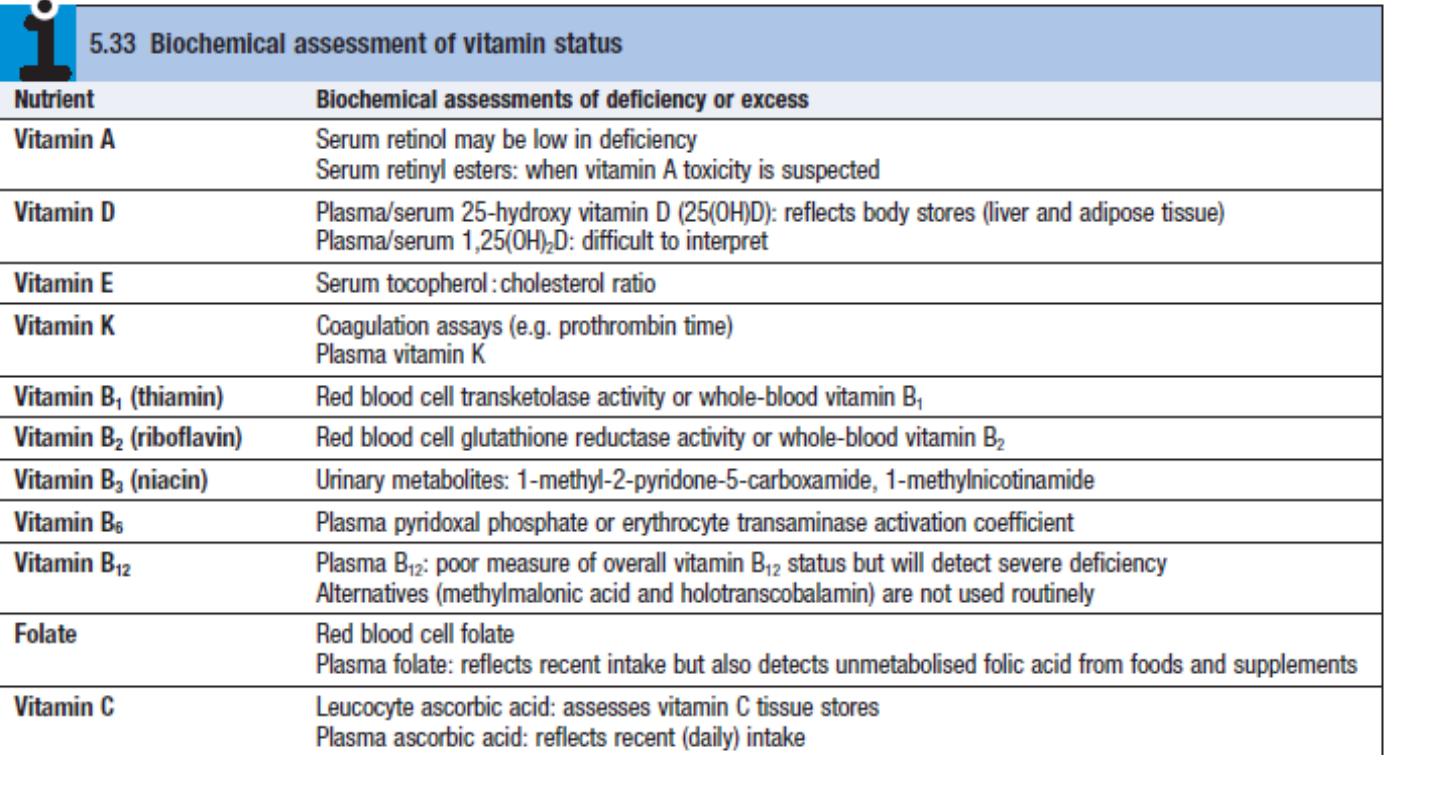
Blood levels of vitamin B12 provide a reasonable
indicationof tissue stores and are usually diagnostic of
deficiency. Levels of cobalamins
fall in normal pregnancy.
Reference ranges vary between laboratories but levels
below 150 ng/L are common and, in
the last trimester
,
.
Spuriously
low B12 values occur in women using the oral
contraceptive pill
and in patients with myeloma,.