
Approach
to
FEVER
Dr.Bilal Natiq Nuaman
C.A.B.M. ,F.I.B.M.S. ,D.I.M. ,M.B.Ch.B.
2015-2016

Th
e
rmor
e
g
u
la
t
ion
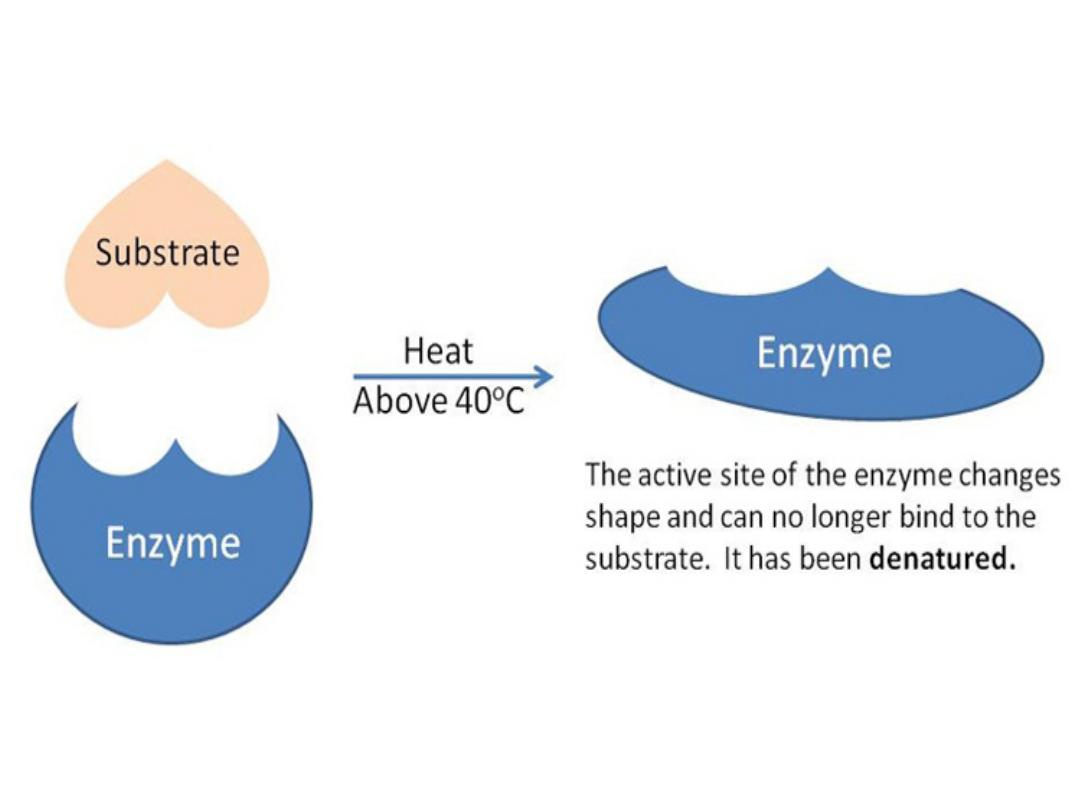
• Because Temperature affects how the enzymes work in your
body , People should maintain a normal body temperature of
about 37°C despite wide variations in both their metabolic
activity and the temperature of their environment.
Almost all enzymes have an "optimal" temperature. For
example, most human derived enzymes will function best at
around 37 ° C .If it gets too hot or cold the enzymes might
denature and lose the shape of their active site, which means
the substrate may no longer fit and this decreases the rate of
the chemical reactions.
•
•
HO
M
EO
S
TASIS
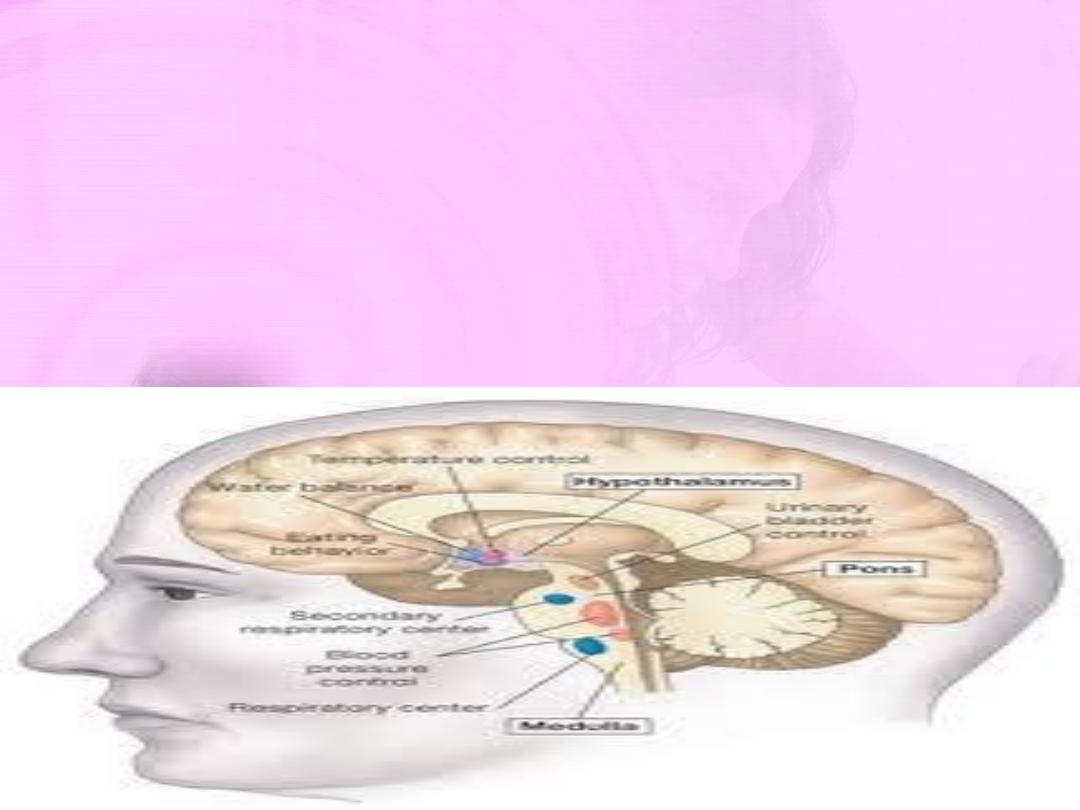
The body keeps its core temperature constant at about 37 C by
physiological adjustments controlled by the hypothalamus
(Thermostat Center) where there are neurons sensitive to
changes in skin and blood temperatures. The temperature-
regulating centers are found in the Preoptic Area (the anterior
portion of the hypothalamus).

Nor
m
al
F
e
a
t
ur
e
s
of Body
Temperature
1-the mean oral temperature is
36
.
8°
±
0
.
4°C
2-The normal diurnal variation is typically
0
.
5°C
(6 A.M. readings < 6 P.M. readings by 0.5
°C)
Fever is an elevation of body temperature
that exceeds the normal daily variation and
occurs in conjunction with an increase in the
hypotha-lamic set point (e.g., from 37
°
C to
39
°
C).
FEVER:
an A.M. temperature of >37.2°C (>98.9°F) or
a
P.M. temperature of >37. 7°C (>99. 9°F)

induce host cells, such as blood leukocytes and tissue
called Endogenous pyrogens (
e.g.,
interleukin-1).
higher level through the action of prostaglandin
raise body temperature (chill);
thermostatic set point;
(defervescence-sweating)
and
return
of
body
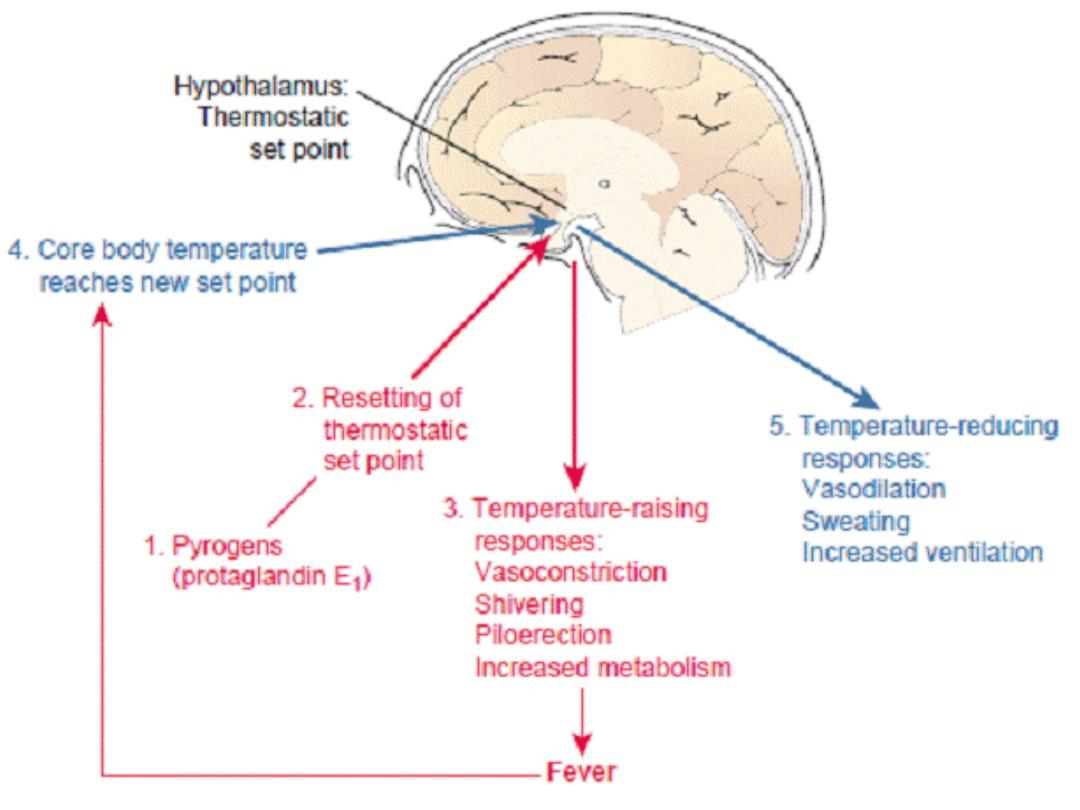
Mechanisms of fever
• (1) Exogenous pyrogens (micro-organism , toxin …)
macrophages, to produce fever-producing mediators
• (2) resetting of hypothalamus thermostatic set point to a
E2.(prodrome);
• (3) generation of hypothalamic mediated responses that
• (4) development of fever with elevation of body to new
• (5) production of temperature lowering responses
temperature to a lower level.

• 1-It enhance immune function;
• 2-Inhibits growth of some microbial agents:
Benefits
o
f fever
• Increases motility and activity of the white blood cells
(T cells and B cells ).
• Stimulates the interferon production .
• Increase phagocytic activity
• Many of the microbial agents that cause infection grow
best at normal body temperatures, and their growth is
inhibited by temperatures in the fever range

• Dehydration occurs because of sweating.
Metabolic effects:
•
• Increased need for oxygen (13 % for every 1 ˚ C increase
• Increases the heart rate (10 /min. for every 1 ˚ C increase
• Increases the respiration rate (4/min. for every 1 ˚ C
• Increased use of body proteins as an energy source
• With prolonged fever, there is increased breakdown of
• Precipitates febrile convulsions
Adver
s
e
effec
t
s
of fever
• Increased need for oxygen (13 % for every 1 ˚ C increas
in body temp.).
• Increases the heart rate (10 /min. for every 1 ˚ C increas
in body temp.).
• Increases the respiration rate (4/min. for every 1 ˚
increase in body temp.).
• Increased use of body proteins as an energy so
(catabolism)
• With prolonged fever, there is increased breakdown
endogenous fat stores .(metabolic acidosis)

Diagnostic Fea
t
ures
of
Fev
e
r
Ø
R
e
l
a
tive
bradycard
i
a
:(rising of HR <5 /min. for each 1˚C rise )
Causes : Typhoid,Brucellosis,Leptospirosis,and Factitious fever
Ø
R
e
l
a
tive
tachycardia
(rising of HR >15/min. for each 1˚C rise )
Causes :Myocarditis, rheumatic fever
Ø
R
e
versed di
u
rnal
patte
r
n
:(AM Temp. >PM Temp.)
Causes: Typhoid , disseminated TB
Ø
Fa
i
l
u
re
to
h
ave fever
Cause: Elderly,CRF,Corticosteroid
compon
e
nts
of
fe
v
er
1
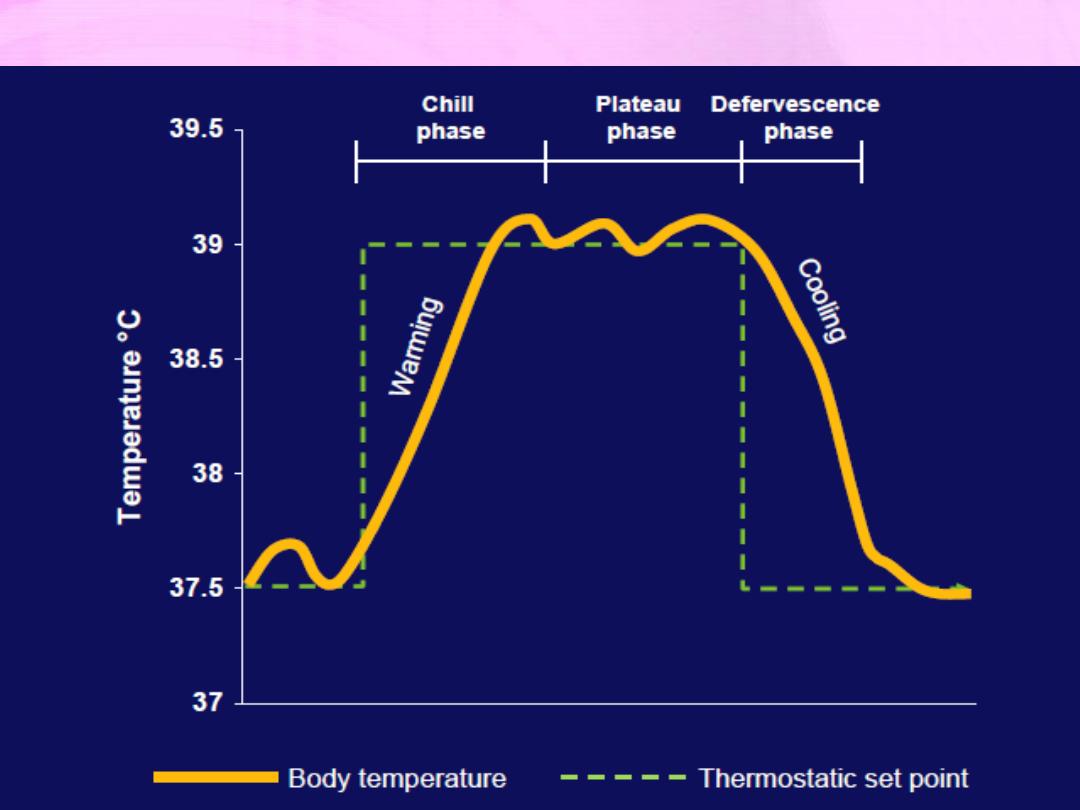
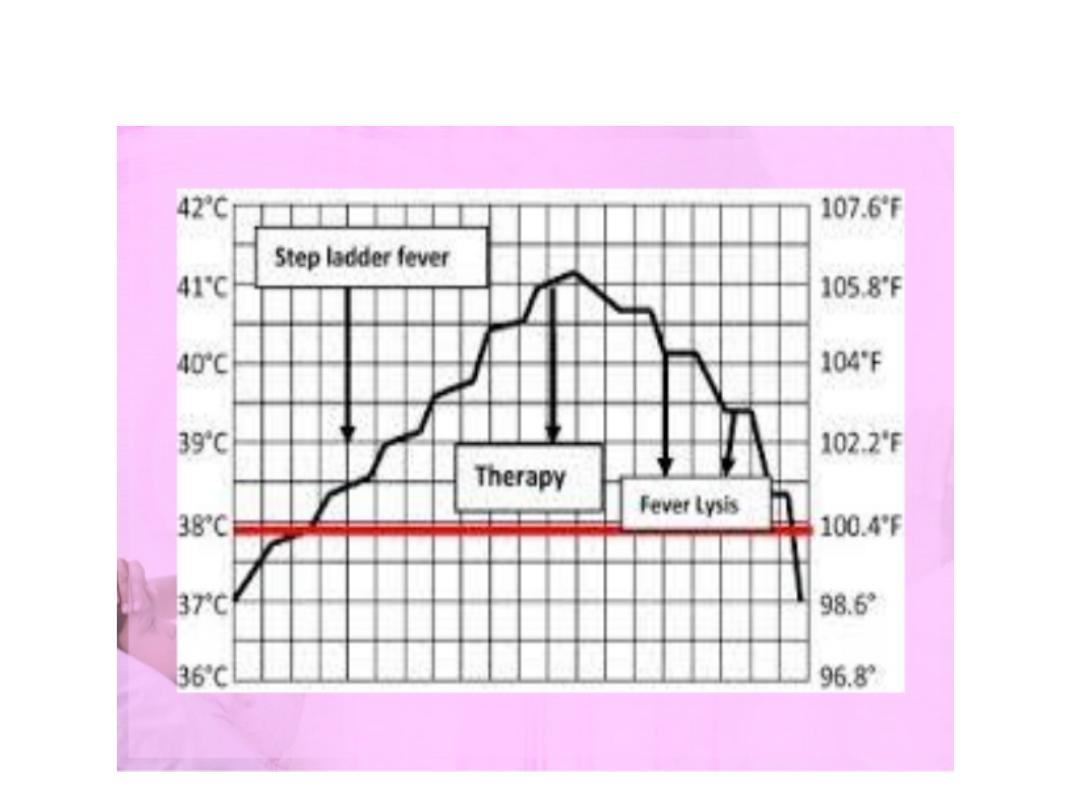
-Ons
e
t of fever : (warming – c
h
ill p
h
a
s
e)
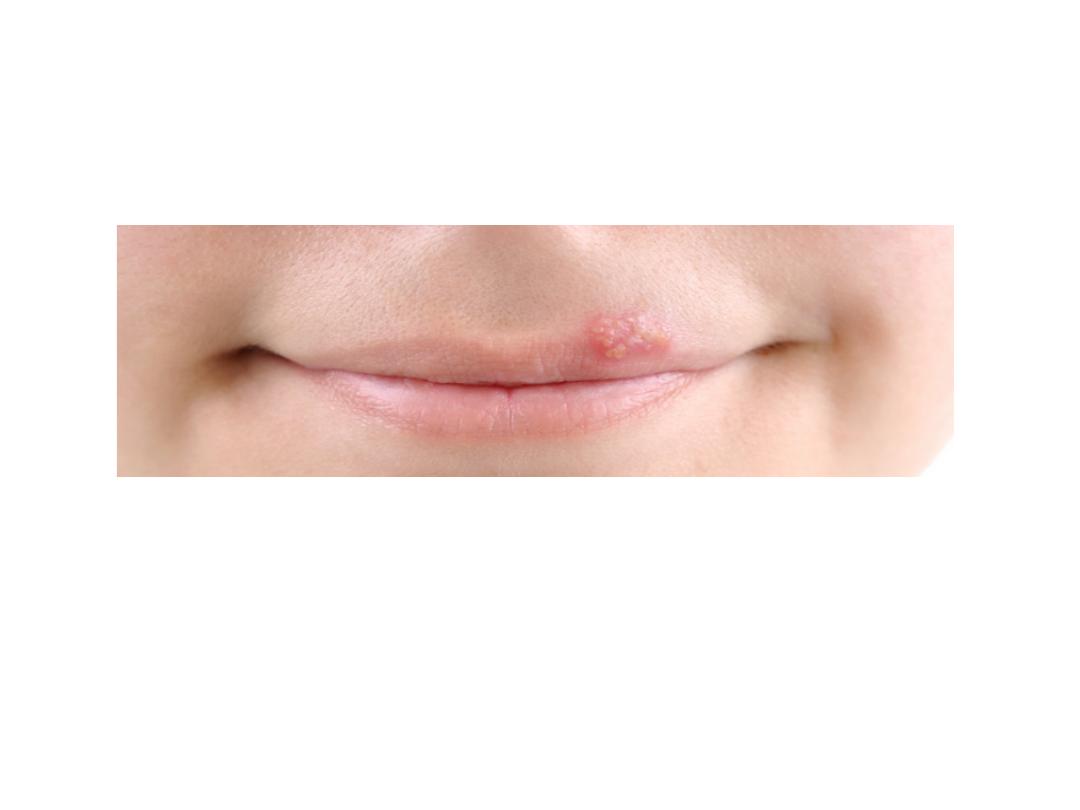
Sudden rise : pneumonia,malaria,meningitis (associated with oral
herpes simplex).
Gradual rise : typhoid fever (step-ladder) .

2
-
Ma
i
n
(pat
t
er
n-
plateau
ph
a
se)
v
Co
n
t
i
nuo
u
s
: fever does not fluctuate more than 1˚C during
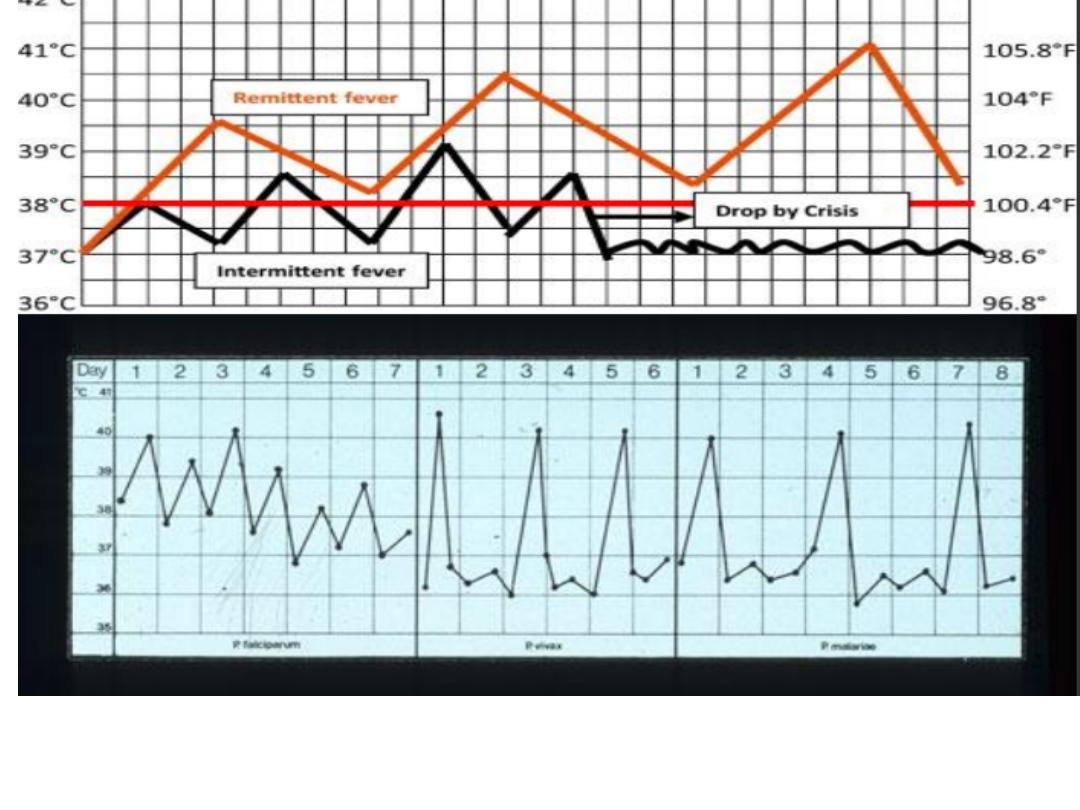
v
R
e
mi
t
e
n
t
: daily fluctuations exceed 2˚C but at no time touches
It is associated with viral upper respiratory tract, legionella, and
v
In
t
erm
i
t
t
ent
: fever reaches normal level
ü
Quotidian :wn. Paroxysms of fever occur daily(P.Falciparum)
ü
Tertian : wn. Paroxysms of fever on alternate days(P.Vivax
ü
Quartan :every 72 hrs (P.Malaiae)
24hrs, but at no time touches the normal.e.g.pneumonia,
typhoid fever, urinary tract infection, brucellosis
the normal.
mycoplasma,Ovale)
infections

3-End of fever :
Crisis
(sudden reduction ){associated with sweating}
e.g. pneumonia
L
y
sis
( gradual reduction)
e.g. Typhoid
• 1- History taking
Low grade : temp.<38.5 , not associated with rigor (but chills ) ,
High grade : temp.>38.5 , associated with rigor and sweating , not
Rigors
.
•
severe shivering, implies a rapid rise in body temperature. Can
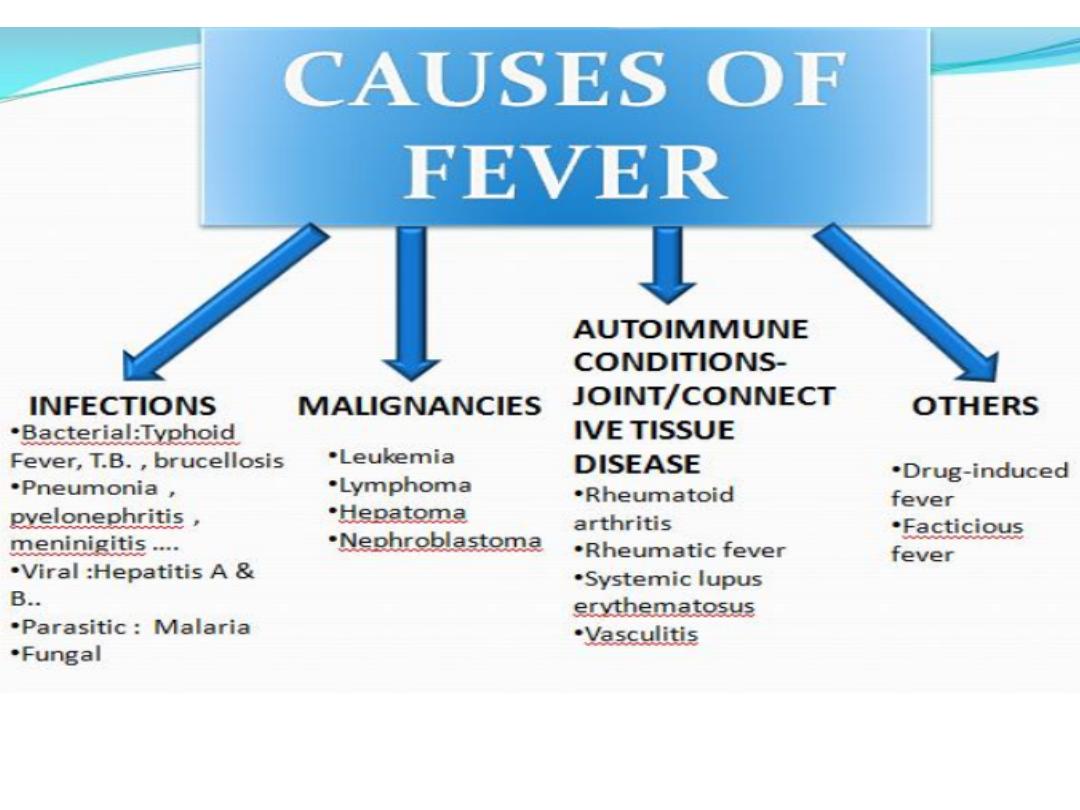
• 1) brucellosis , malaria
, pye
l
on
e
phritis
,
Pneumonia
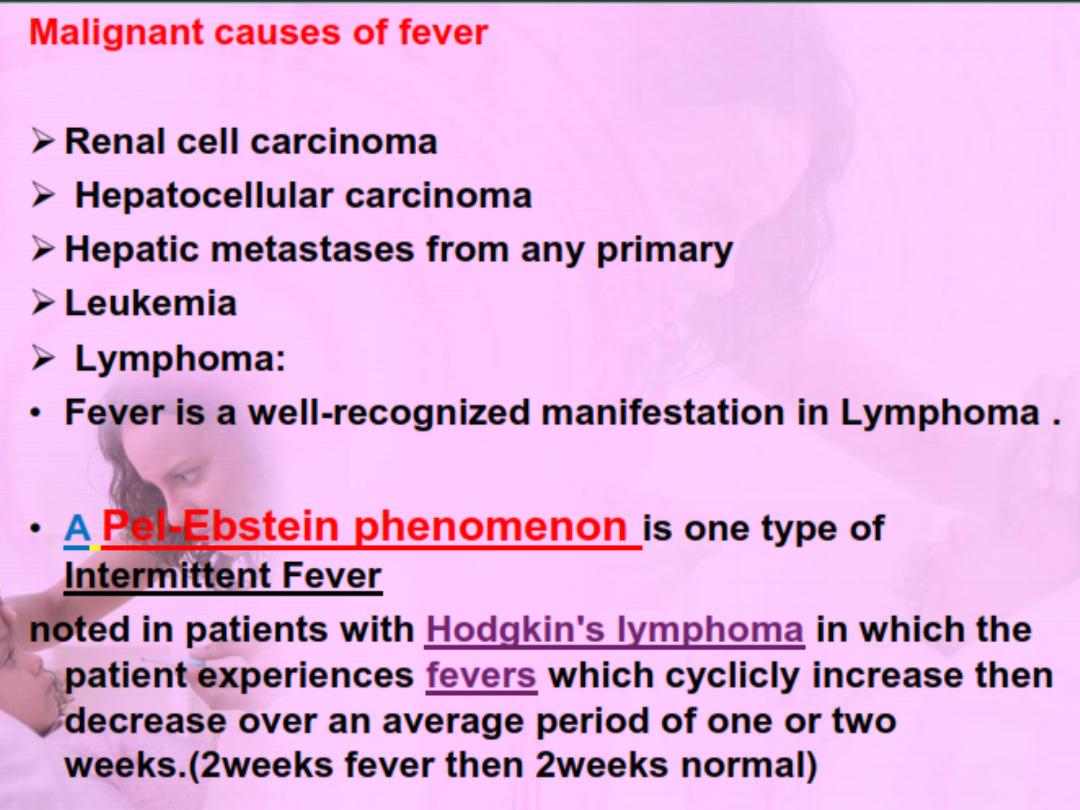
3) lymphoma
Ap
p
roach
to patient
with fever
1)Onset (sudden vs. gradual)
2) grade (High vs. low grade)
relieved by antipyretics or sponging , not interfere with usual
activity .
relieved by antipyretics or sponging , interfere with usual
activity.
profound chills accompanied by chattering of the teeth and
be produced by :
2) abscess ,cholangitis ,
septic
arthritis

3)Duration of the fever
4)Fever pattern (Remittent fever, Intermittent, continuous fever)
6)Severity
7)Relieving and aggravating factors
8)Treatment received or/and outcome
5)Timing (through out the day, at night, day time)
interfere with sleep , interfere with usual activity
Drug and allergy History
Ø
Drug fever is a disorder characterized by a febrile response
absence of underlying conditions that can be responsible for
of other causes is that it disappears once the offending drug is
fevers.
often suspected in patients with otherwise unexplained
cardiac drugs
Ø
Blood transfusion.
Immunization and vaccinations .
Ø
coinciding temporally with the administration of a drug in the
the fever. A key feature that differentiates drug fever from fever
discontinued. Drug fever tends to be a diagnosis of exclusion,
causes :
antibiotics (penicillin) ,anticonvulsants(phenytoin) , and some

• Smoking history - amount, duration & type
Alcohol history - amount, duration &type
Occupation, social & education background, family social
•
•
• Home conditions-Water supply, Sanitation status in his home &
• Animals / birds in his/her house- exposure to birds (psittacosis)
• Consumption of unpasteurized milk or milk products
Personal and Social History
support& financial situation, Social class.
surrounding, Geographic area of living, fresh-water swimming.
or animals (,avian flu , toxoplasmosis, brucellosis, rabies….)
(tuberculosis, brucellosis and Q fever).

• Sexual History- Unprotected exposure to sexual partner with
• Illicit drug usage- injections and sharing of needles (HIV,
Travel History
Travel to an area known to be endemic for certain disease:
If the patient has been in an endemic area
Malaria, Typhoid fever, Viral hepatitis .
STD, HIV,syphilis…
hepatitis B &C, infective endocarditis), site of injection (e.g
Femoral vein-septic arthritis, ilio-psoas abscess)
• Name of the area, duration of stay
• Onset of illness- (incubation period)
The most common diagnoses :


FEVER AND MUCUS MEMBRANE RASH
(ENANTHEM)
•
K
o
pl
i
k's
spots in
measles
•
Forchhe
i
mer
spots
in
rubella

T
h
a
n
k
y
o
u