
CHEST PAIN
DR.Bilal Na*q Nuaman
CABM,FICMS,DIM,MBChB
2015
Chest pain—broadly defined as any discomfort in the
anterior thorax occurring above the epigastrium and below
the mandible—can be one of the most challenging problem
managed
by
the
physicians.
The
typical
pa*ents’
concern
with
the
first
bout
of
chest
pain
is their apprehension of the onset of cardiac pathology, such
as
ischemic
heart
disease
(IHD).
Chest
discomfort
is
among
the
most
common
reasons
for
which pa*ents present for medical aQen*on at either an
emergency department (ED) or an outpa*ent clinic.
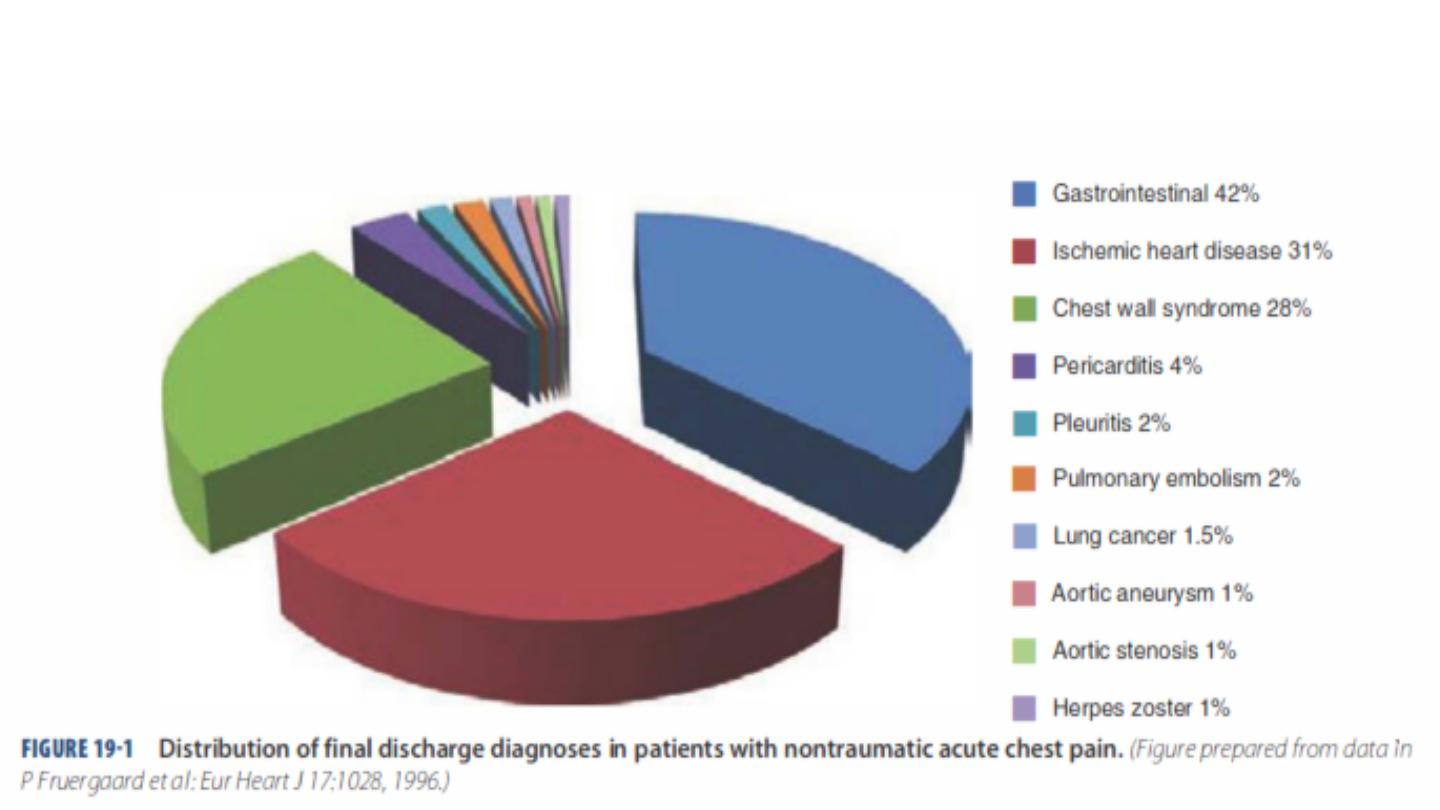
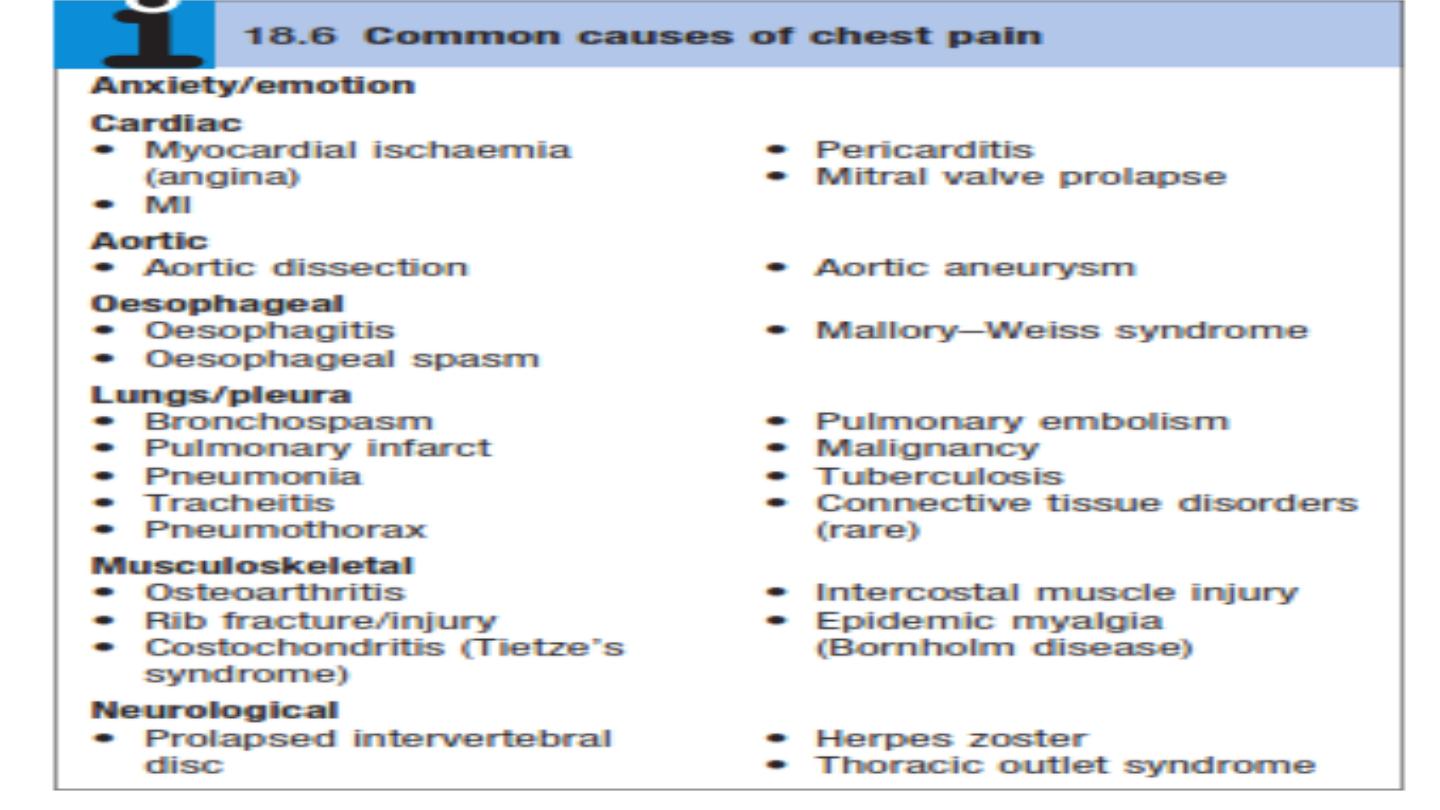
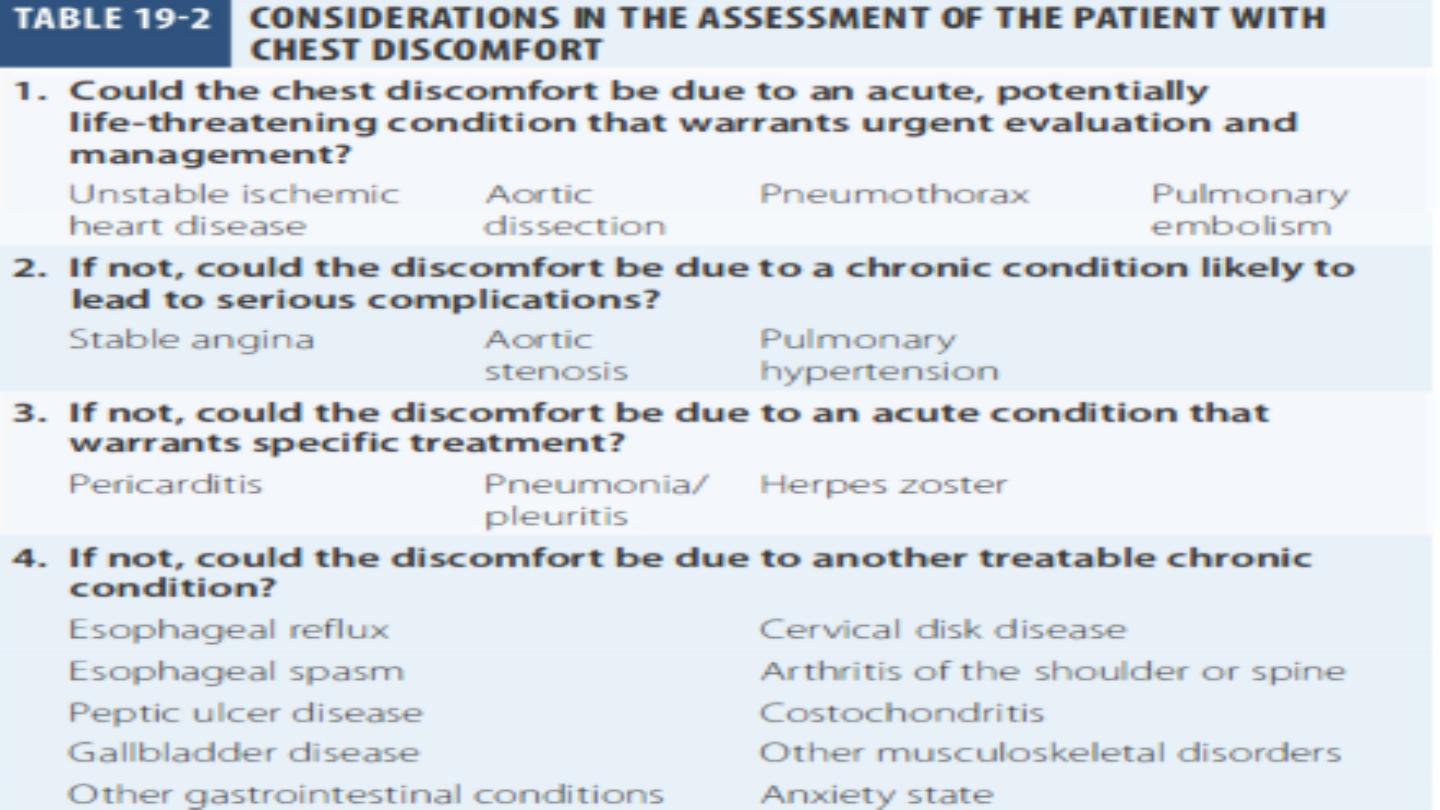
CAUSES OF CHEST PAIN

It
is
helpful
to
frame
the
ini*al
diagnos*c
assessment
and
triage of pa*ents with acute chest discomfort around three
categories:
(1) Ischemic
heart
disease;
(2) other
cardiopulmonary
causes
(pericardial
disease,
aor*c
emergencies, and pulmonary condi*ons); and
(3) non-‐cardiopulmonary causes
.

Ischemic
Vs
Non Ischemic
Chest
Pain
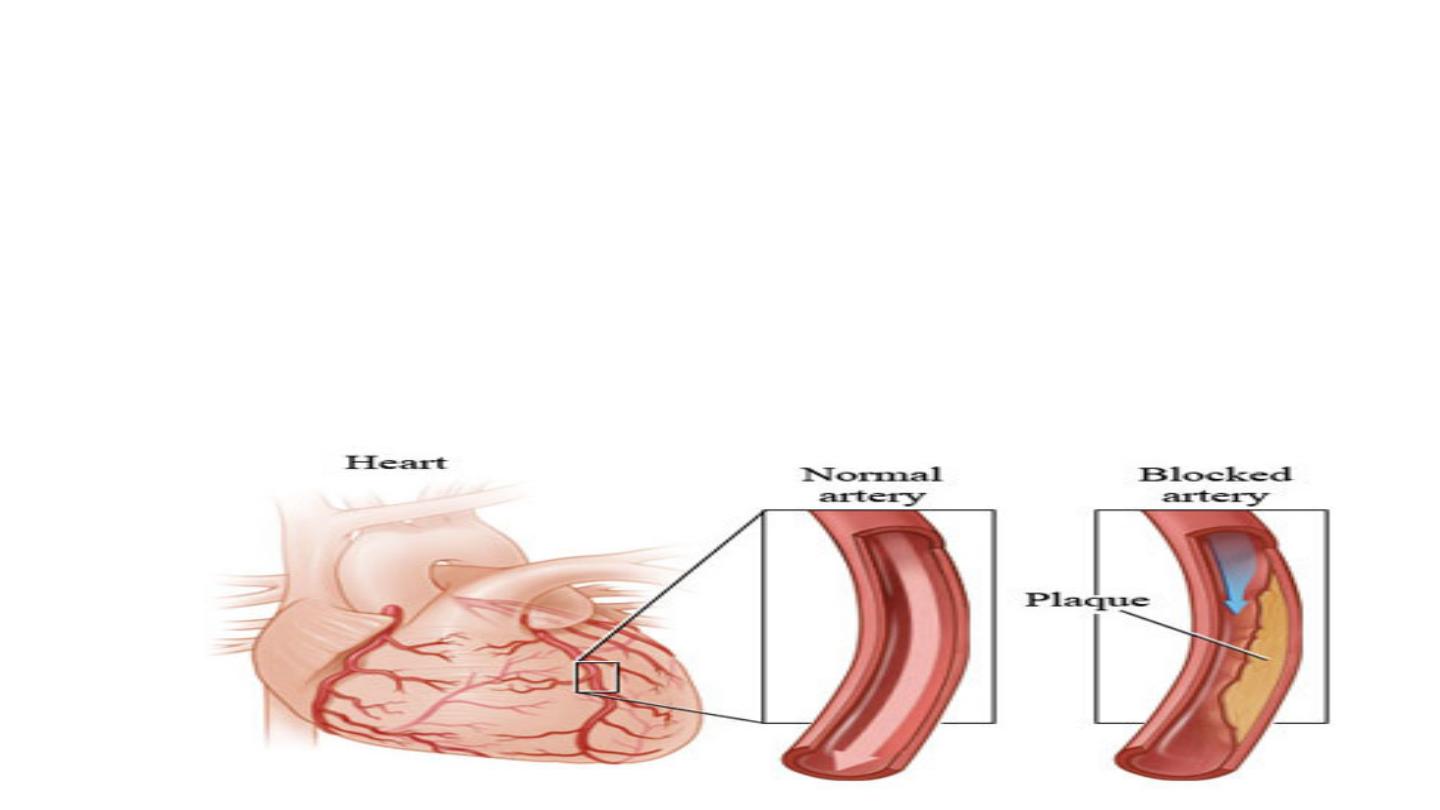
•
Chest pain due to ischemic heart disease (IHD) may manifest as:
Angina
pectoris
:2-‐10
min.,
relieved
by
rest
,
not
associated
with
vomiDng
Myocardial
infarcDon
:>30
min.,
not
relieved
by
rest
,
associated
with
vomiDng

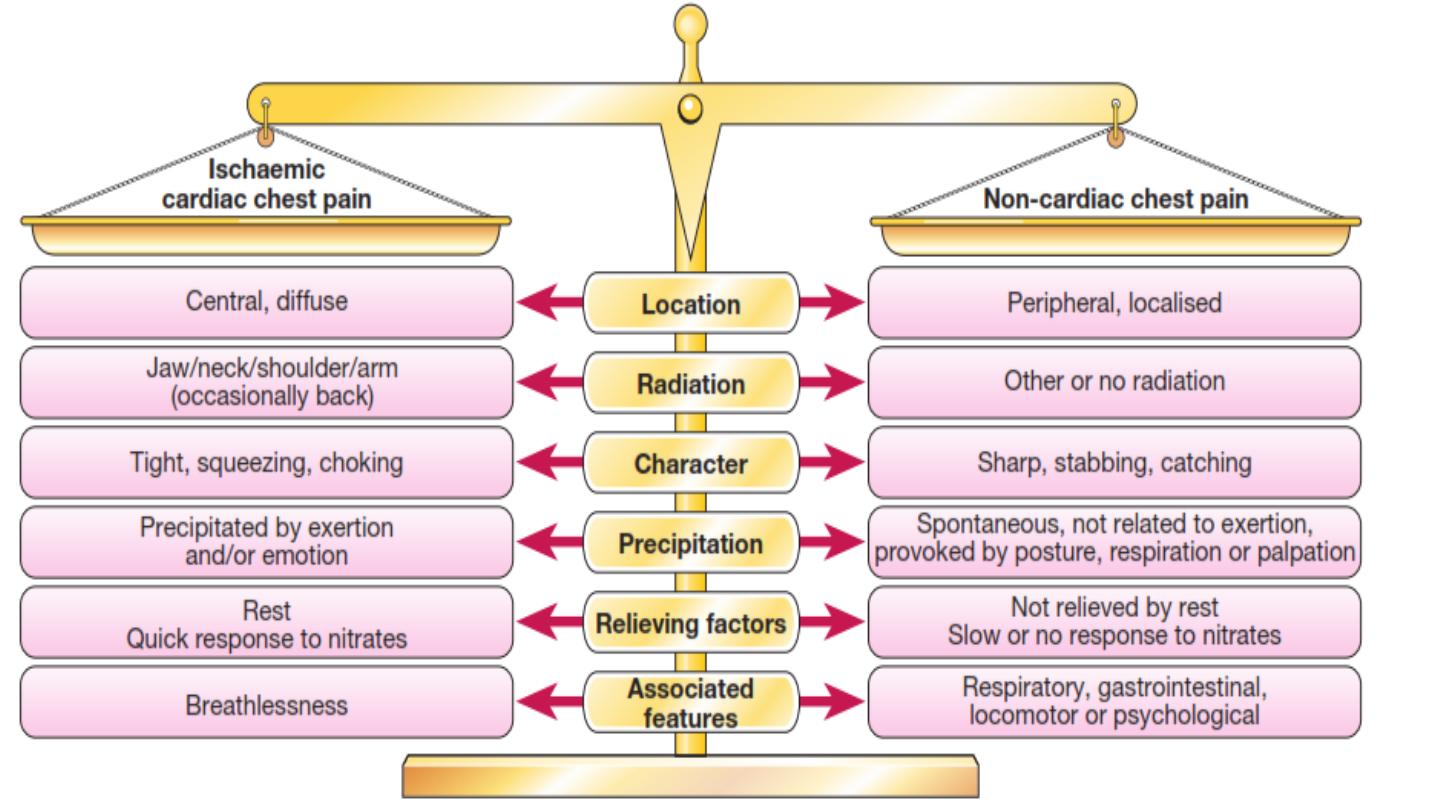
Characteristics of cardiac pain
•
Onset.
The pain of MI typically takes several minutes or even
longer to develop; similarly, angina builds up gradually in
proporDon to the intensity of exerDon.
The pain of aorDc dissecDon, massive pulmonary embolism or
pneumothorax is usually very sudden or instantaneous in
onset.

•
Site.
Cardiac pain is typically located in the Centre of the
chest because of the derivaDon of the nerve supply to the
heart and mediasDnum.
•
Radia-on.
Ischemic cardiac pain may radiate to the neck,
jaw, and upper or even lower arms. Occasionally, cardiac
pain may be experienced only at the sites of radiaDon or in
the back.
Pain situated over the leN anterior chest and radiaDng
laterally is unlikely to be due to cardiac ischemia and may
have many causes, including pleural or lung disorders,
musculoskeletal problems and anxiety.

•
Character.
Cardiac pain is typically
dull, constric-ng, or
'heavy’, and is usually described as squeezing, crushing,
burning
but not sharp, stabbing, pricking
.
They
typically
use
characterisDc
hand
gestures
(e.g.
Open
hand or clenched fist) when describing ischemic pain(
Levine's
sign)
.

Levine's sign
•
Provoca-on.
Anginal pain occurs during (not aNer) exerDon
and is promptly relieved (in less than 5 minutes) by rest. The
pain may also be precipitated or exacerbated by emoDon but
tends to occur more readily during exerDon, aNer a large
meal or in a cold wind.
In
contrast,
pleural or pericardial pain
is usually described as
a ‘sharp’ or ‘catching’ sensaDon that is exacerbated by
breathing,
coughing
or
movement.
Pain
associated
with
a
specific
movement
(bending,
stretching, turning) is likely to be
musculoskeletal
in origin.

•
Relief of chest discomfort
within min-‐utes aNer administraDon of
nitroglycerin is suggesDve of myocardial ischemia.
Esophageal
spasm
may
also
be
relieved
promptly
with
nitroglycerin.
Pain
that
occurs
aNer
rather
than
during
exerDon
is
usually
musculoskeletal or psychological
in origin.

•
Associated features
. The pain of MI, massive pulmonary
embolism or aorDc dissecDon is oNen accompanied by
autonomic disturbance, including sweaDng, nausea and
vomiDng.
Breathlessness, due to pulmonary congesDon arising from
transient ischemic leN ventricular dysfuncDon, is oNen a
prominent and occasionally the dominant feature of MI or
angina
(angina equivalent)
. Breathlessness may also
accompany any of the respiratory causes of chest pain and
can be associated with cough, wheeze or other respiratory
symptoms.
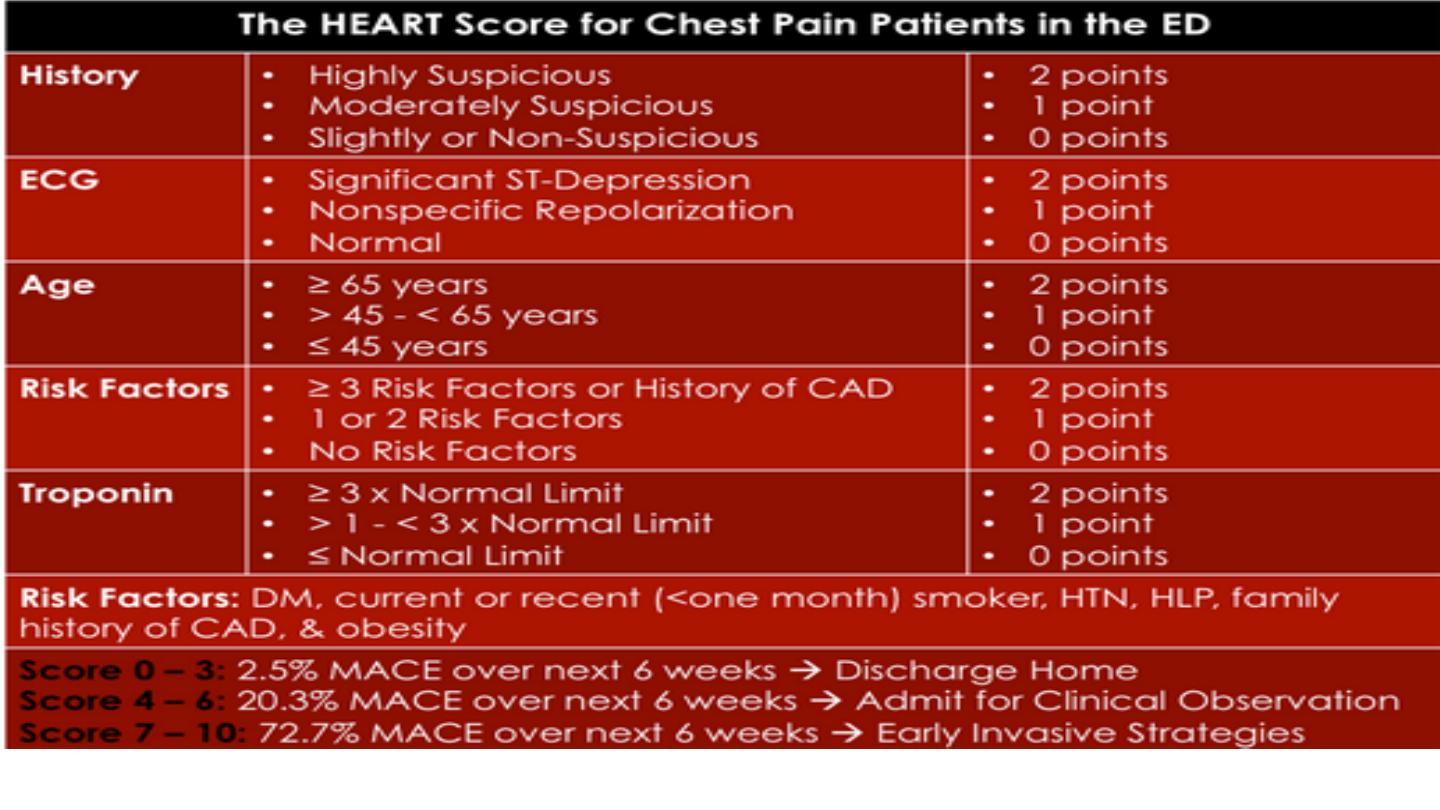
Major adverse cardiac events (MACE)

DIFFERENTIAL DIAGNOSIS
•
Acute, sudden and severe chest pain described as tearing that is
maximal at onset and radiates to interscapular area raises the
possibility of
aor*c dissec*on
.
Important diagnosDc feature is the inequality in the pulses, e.g.
caroDd, radial and femoral, and a blood pressure differenDal of greater
than 20 mm Hg

•
Severe chest pain, retrosternal, accompanied by dyspnea, cough, and
hemoptysis developing in a paDent who has been immobilized or
bedridden is suggesDve of
pulmonary embolism
•
Chest discomfort due to
pericardi*s
is typically retrosternal,
aggravated by coughing, deep respiraDon, or change in posiDon;
worse in supine, and relieved in si\ng upright and leaning forward
•
The pain of
esophageal spasm
is commonly an intense, squeezing
discomfort that is retrosternal in locaDon and, like angina, may be
relieved by nitroglycerin
•
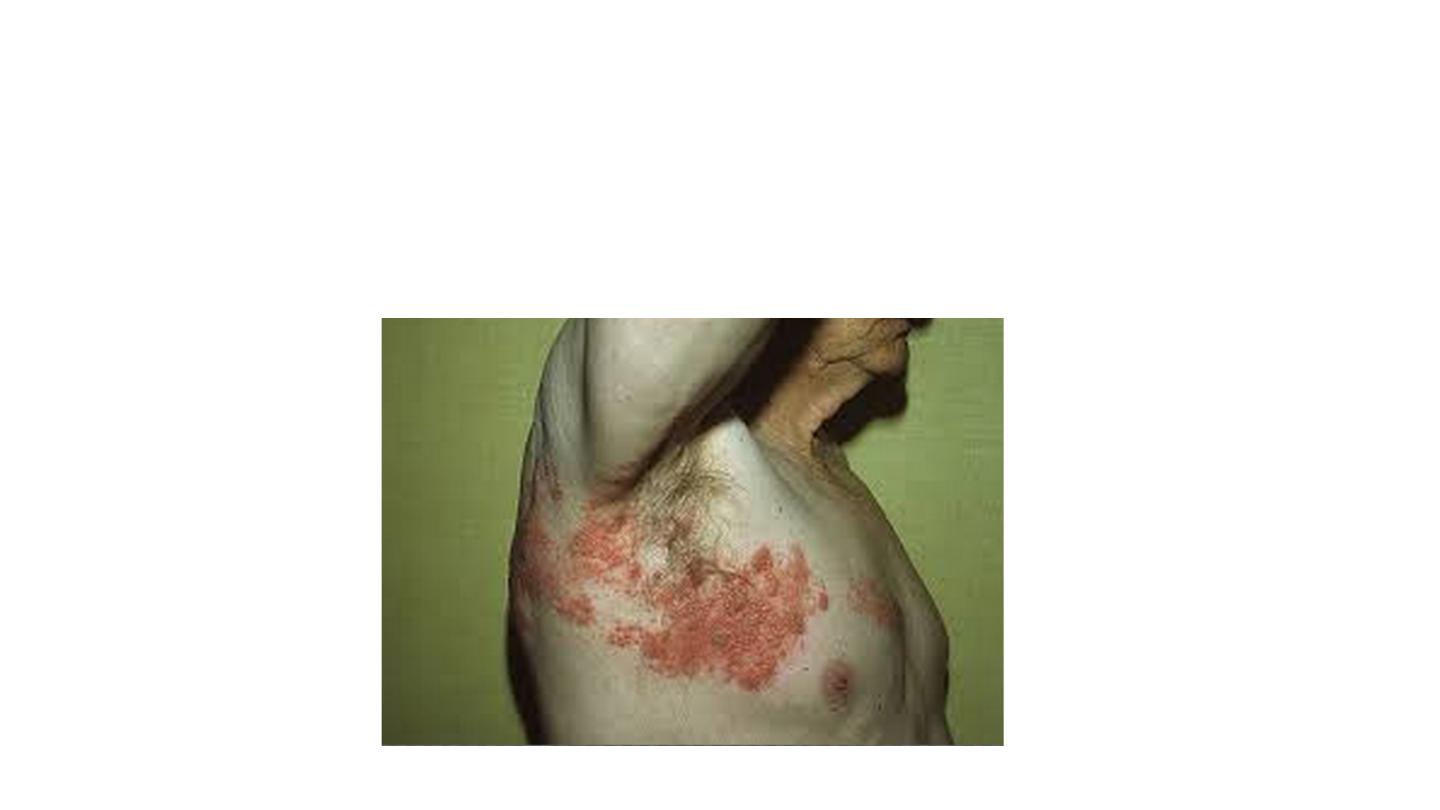
Pain in a dermatomal distribuDon can also be caused by
herpes
zoster
•
Stable angina NON ischemic chest pain
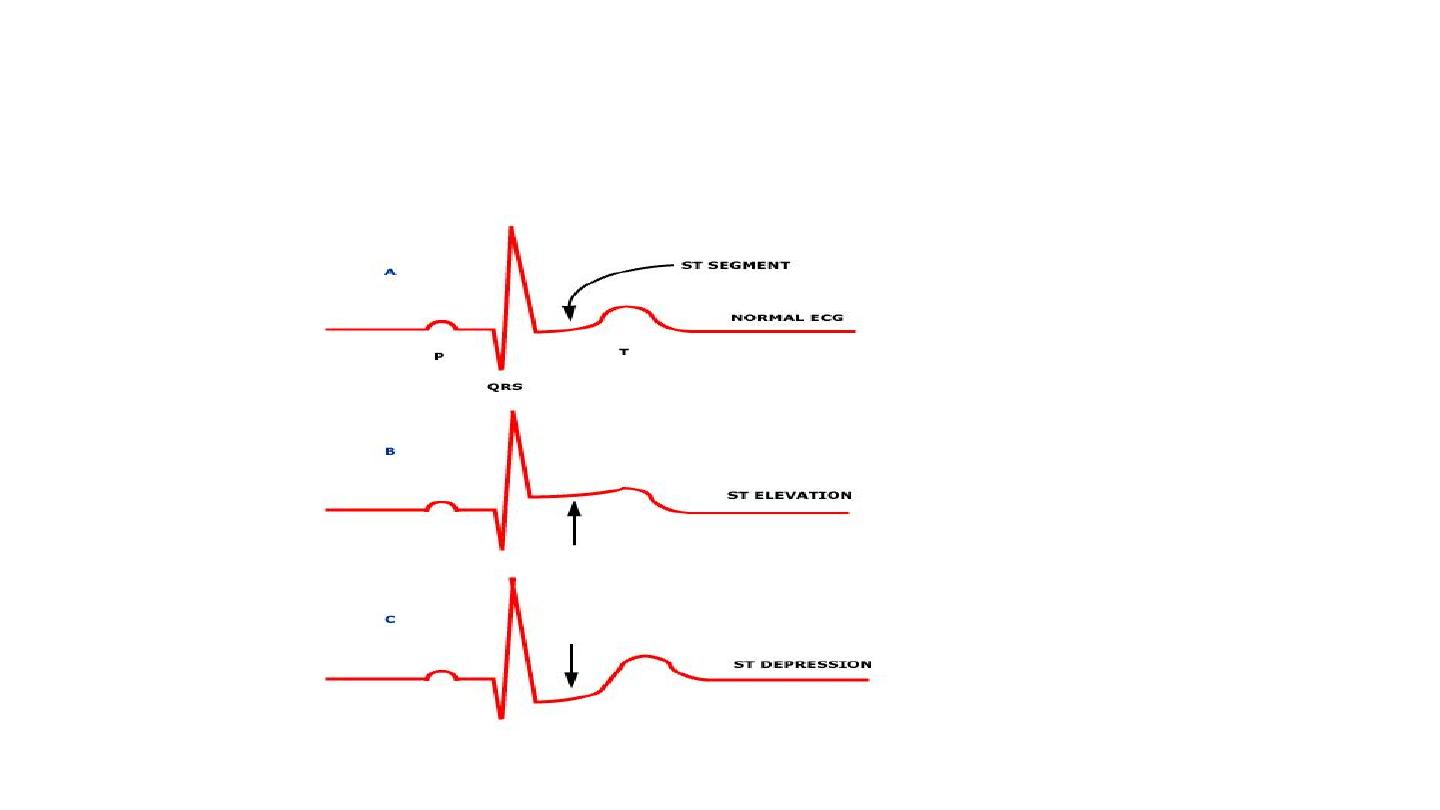
ECG
50%
DIAGNOSTIC
TREADMILL TEST
75%
DIAGNOSTIC
CORONARY
ANGIOGRAPHY
DIAGNOSTIC
95%
CXR
PULMONARY
CAUSES
ABDOMINAL U/
S , OGD
ABDOMINAL
CAUSES
ECHO
EXCLUDE
VALVE LESION

THANK YOU