GIT DRUGS
DR. JAMAL
1
GIT DRUGS
OVERVIEW
The four common medical conditions involving the gastrointestinal (GI)
tract:
1) Peptic ulcers and gastroesophageal reflux disease (GERD)
2) Antiemetic
3) Diarrhea
4) Constipation.
DRUGS USED TO TREAT PEPTIC ULCER
DISEASE AND
GASTROESOPHAGEAL REFLUX DISEASE
The major causative factors for these diseases are:
1. Infection with gram-negative Helicobacter pylori,
2. Use of nonsteroidal anti-inflammatory drugs (NSAIDs).
Treatment approaches include
1) Eradicating the H. pylori infection,
2) Reducing secretion of gastric acid with the use of PPIs (proton pump
inhibitors) or H
2
-receptor antagonists, and/or
3) Providing agents that protect the gastric mucosa from damage, such as
misoprostol and sucralfate.
A. Antimicrobial agents
Optimal therapy for patients with peptic ulcer disease (both duodenal and
gastric ulcers) who are infected with H. pylori requires antimicrobial
treatment.
Eradication of H. pylori results in rapid healing of active peptic ulcers
and low recurrence rates.
Successful eradication of H. pylori (80–90 percent) is possible with
various combinations of antimicrobial drugs; currently, either triple
therapy or quadruple therapy is administered for a 2-week course. This
usually results in a 90% or greater eradication rate.
Triple therapy
Quadruple therapy
1. PPI
1. PPI
2. metronidazole or amoxicillin
2. metronidazole
3. clarithromycin
3. tetracycline
4. ------
4. bismuth subsalicylate
GIT DRUGS
DR. JAMAL
2
L Treatment with a single antimicrobial drug is less effective, results in
antimicrobial resistance, and is absolutely not recommended.
L Switching antibiotics is also not recommended (that is, do not
substitute amoxicillin for ampicillin, erythromycin for clarithromycin, or
doxycycline for tetracycline).
B. H2-receptor antagonists
Physiology: Gastric acid secretion by parietal cells of the gastric mucosa
is stimulated by acetylcholine, histamine, and gastrin. The receptor-
mediated binding of acetylcholine, histamine, or gastrin results in the
activation of protein kinases, which in turn stimulates the H
+
/K
+
–
adenosine triphosphatase (ATPase) proton pump to secrete hydrogen ions
in exchange for K
+
into the lumen of the stomach.
Drugs of the group:
a. Cimetidine (TEGAMET
®
) is the prototype histamine H
2
-receptor
antagonist. However, its utility is limited by its adverse effect
profile and drug–drug interactions.
b. Ranitidine (ZANTAK
®
)
c. Famotidine
d. Nizatidine
Mechanism of action: They act selectively on H
2
receptors in the
stomach, blood vessels, and other sites, but they have no effect on H
1
receptors &they potently inhibit (greater than 90 percent) basal, food-
stimulated, and nocturnal secretion of gastric acid after a single dose.
Therapeutic uses: The use of these agents has decreased with the advent
of PPIs.
a. Peptic ulcers
b. Acute stress ulcers
c. Gastroesophageal reflux disease
Pharmacokinetics
: After oral administration, the H2 antagonists
distribute widely throughout the body (including into breast milk and
across the placenta) and are excreted mainly in urine. Cimetidine,
ranitidine, and famotidine are also available in intravenous formulations.
The half-life of all of these agents may be increased in patients with renal
dysfunction, and dosage adjustments are needed.
Adverse effects of cimetidine
GIT DRUGS
DR. JAMAL
3
1) Cimetidine can have endocrine effects because it acts as a
nonsteroidal antiandrogen. These effects include gynecomastia and
galactorrhea (continuous release/discharge of milk).
2) Central nervous system effects (such as confusion and altered
mentation) occur primarily in elderly patients and after intravenous
administration.
3) Cimetidine inhibits several cytochrome P450 isoenzymes and can
interfere with the metabolism of many other drugs, such as
warfarin, phenytoin, and clopidogrel
C. PPIs: Inhibitors of the H+/K+-ATPase proton
pump
Drugs of the group:
• Omeprazole is the first of a class of drugs
• Esomeprazole
• Lansoprazole
• Dexlansoprazole
• Pantoprazole
• Rabeprazole
Mechanism of Actions: These agents are prodrugs which transported to
the parietal cell canaliculus. There, it is converted to the active form,
which reacts with a cysteine residue of the H+/K+-ATPase, forming a
stable covalent bond and suppress the secretion of hydrogen ions into the
gastric lumen.
At standard doses, all PPIs inhibit both basal and stimulated gastric acid
secretion by more than 90 percent.
Therapeutic uses:
• Stress ulcer treatment and prophylaxis.
• Active duodenal ulcer.
• Reduce the risk of bleeding from an ulcer caused by aspirin and
other NSAIDs.
• Long-term treatment of pathologic hypersecretory conditions (for
example, Zollinger-Ellison syndrome).
• Treating erosive esophagitis.
• Treatment of GERD.
• Used with antimicrobial regimens to eradicate H. pylori.
J For maximum effect, PPIs should be taken 30 to 60 minutes before
breakfast or the largest meal of the day.
J If an H
2
-receptor antagonist is also needed, it should be taken well
after the PPI for best effect because the H
2
antagonists will reduce the

GIT DRUGS
DR. JAMAL
4
activity of the proton pump, and PPIs require active pumps to be
effective.
Pharmacokinetics: All of these agents are effective orally. [Note: Some
are also available for intravenous injection.]
Metabolites of these agents are excreted in urine and feces.
Adverse effects:
• Nausea, diarrhea and GI disturbance
• Headache
• Increase the risk of fractures especially those patients taking the
PPIs for one year or greater.
• Decrease the effectiveness of clopidogrel (Plavix).
• Prolonged therapy with agents that suppress gastric acid, such as
the PPIs and H
2
antagonists, may result in low vitamin B
12
,
because acid is required for its absorption in a complex with
intrinsic factor.
• Elevated gastric pH may also impair the absorption of calcium
carbonate. (Treat with calcium citrate - not affected by gastric pH).
D. Prostaglandins
Prostaglandin E, produced by the gastric mucosa, inhibits secretion of
HCl and stimulates secretion of mucus and bicarbonate (cytoprotective
effect).
Misoprostol (analog of prostaglandin E
1
), is less effective than H
2
antagonists and the PPIs.
Side effects
• Misoprostol produces uterine contractions, and is contraindicated
during pregnancy.
• Dose related diarrhea and nausea are the most common adverse
effects and limit the use of this agent.
E. Antacids
Antacids are weak bases that react with gastric acid to form water and a
salt to diminish gastric acidity.
Drugs of the group
• Aluminum hydroxide or magnesium hydroxide, are commonly used
either alone or in combination.
• Calcium carbonate reacts with HCl to form CO
2
and CaCl
2
and is a
commonly used preparation.
• Sodium bicarbonate [NaHCO
3
] can produce transient metabolic
alkalosis because of systemic absorption ; therefore, this antacid is
not recommended for long-term use.
Therapeutic uses:
• Symptomatic relief of peptic ulcer disease and GERD
GIT DRUGS
DR. JAMAL
5
• Promote healing of duodenal ulcers.
• Calcium carbonate preparations are also used as calcium
supplements for the treatment of osteoporosis.
3. Adverse effects:
• Aluminum hydroxide tends to cause constipation, whereas
magnesium hydroxide tends to produce diarrhea. Preparations that
combine these agents aid in normalizing bowel function.
• The
aluminum-containing
antacids
can
lead
to
hypophosphatemia.
• In addition to the potential for systemic alkalosis, sodium
bicarbonate liberates CO
2
, causing belching and flatulence.
• Absorption of the cations from antacids (Mg
2+
, Al
3+
, Ca
2+
) lead to
accumulation of these ions in patients with renal impairment.
• The sodium content of antacids can be an important consideration
in patients with hypertension or congestive heart failure.
F. Mucosal protective agents
1. Sucralfate:
This is a complex of aluminum hydroxide and sulfated sucrose
MOA:
• It binds to proteins of both normal and necrotic mucosa & creates a
physical barrier.
• Little of the drug is absorbed systemically.
Uses:
• Sucralfate is effective for the treatment of duodenal ulcers and
prevention of stress ulcers, but its use is limited due to the need for
multiple daily dosing and drug–drug interactions.
• Because it requires an acidic pH for activation, sucralfate should
not be administered with PPIs, H
2
antagonists, or antacids.
• This agent does not prevent NSAID-induced ulcers, and it does not
heal gastric ulcers.
2. Bismuth subsalicylate: This agent is used as a component of
quadruple therapy to heal peptic ulcers
.
Action:
• It has antimicrobial action
• Inhibit the activity of pepsin
• Increase secretion of mucus
• Interact with glycoproteins in necrotic mucosal tissue to coat and
protect the ulcer crater
GIT DRUGS
DR. JAMAL
6
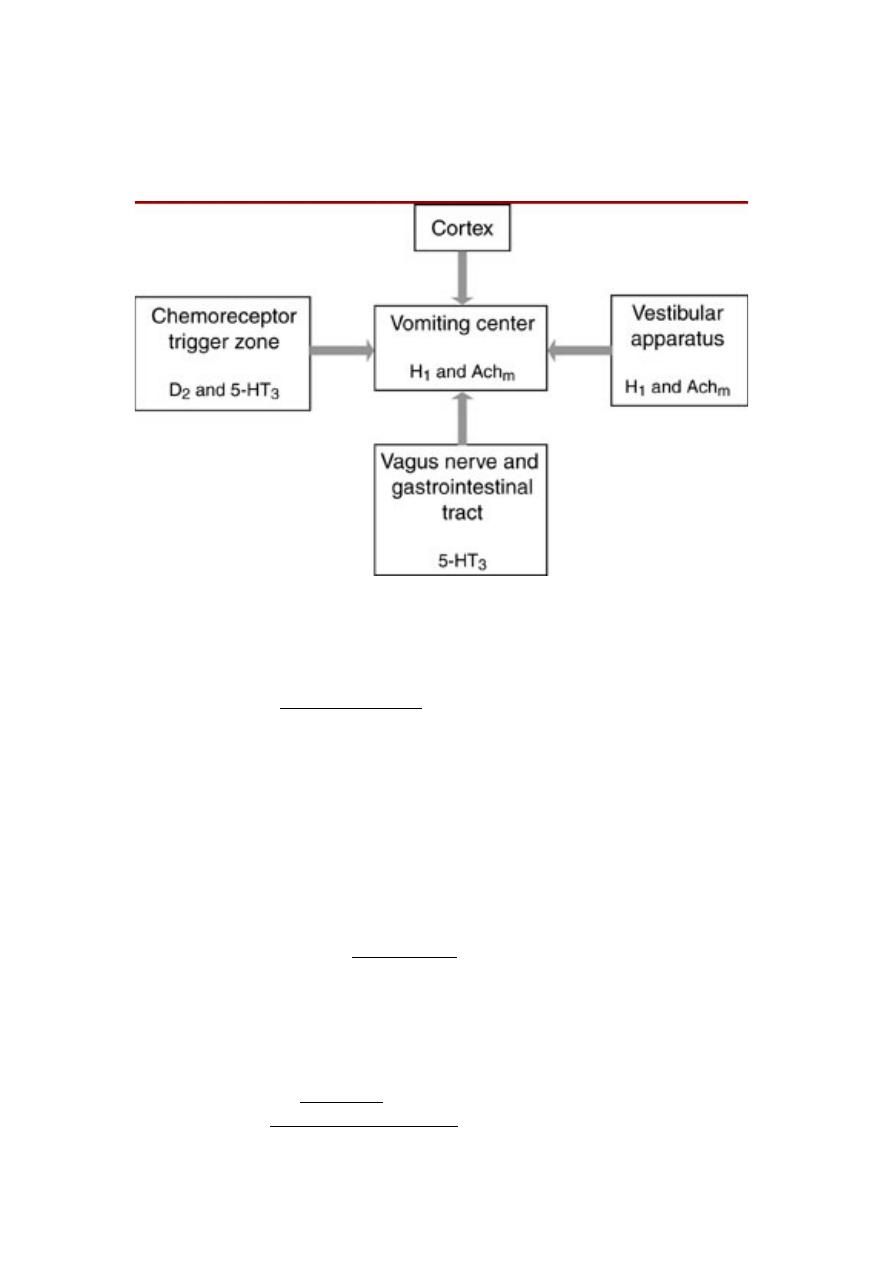
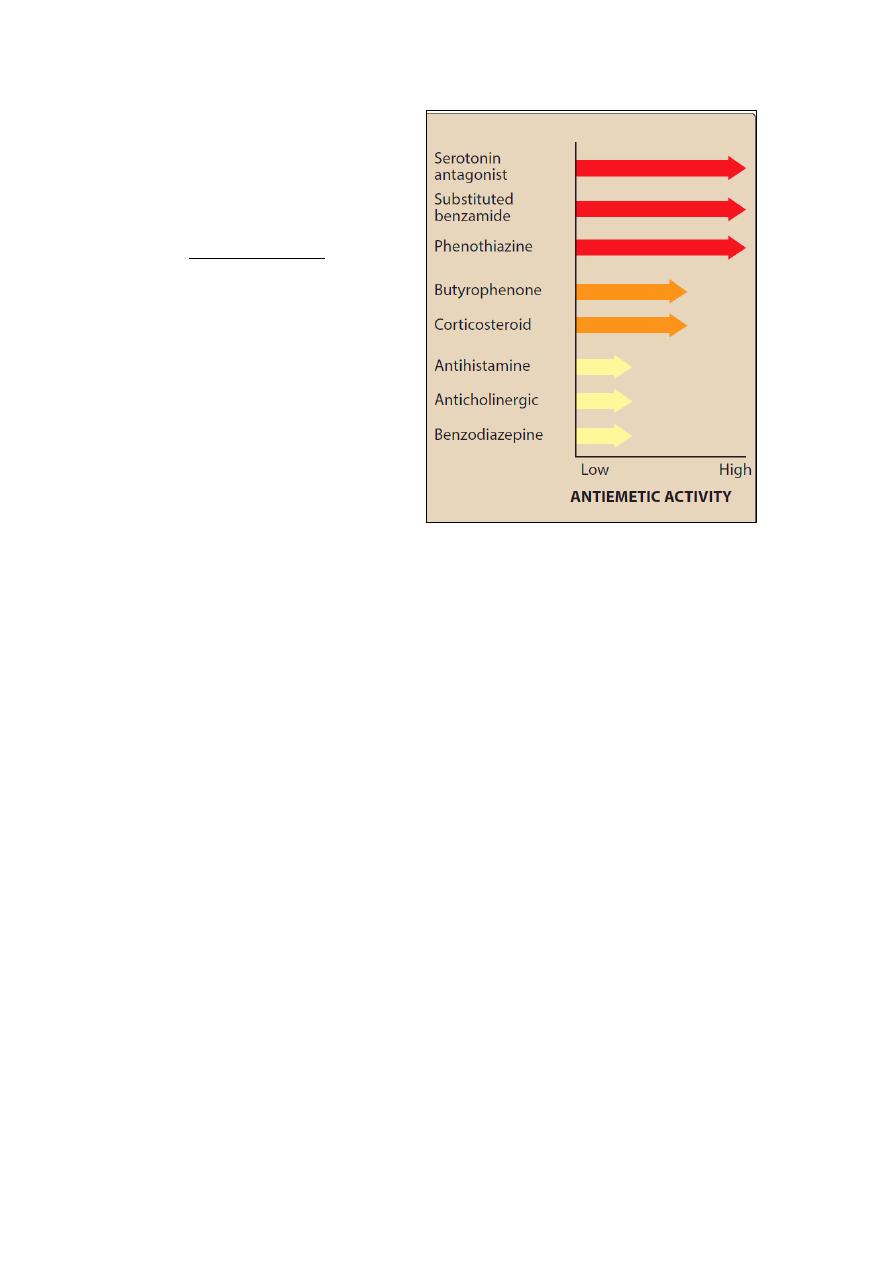
G. ANTIEMETIC DRUGS
Pathophysiology of vomiting:
1. Phenothiazines
:
• Action: blocking dopamine 2 receptors
• Example: prochlorperazine (
Stemetil)
• Side effects: hypotension, restlessness, extrapyramidal symptoms
and sedation.
2. 5-HT3 receptor blockers
:
They are potent antiemetics with
longer duration of action (can be administered as a single dose).
• Action: Selectively block 5-HT
3
receptors in the periphery
(visceral vagal afferent fibers) and in the brain (chemoreceptor
trigger zone).
• They include: ondansetron, granisetron, palonosetron, and
dolasetron
• Pharmacokinetics: These agents are extensively metabolized by
the liver, with being an active metabolite of dolasetron. (
Therefore,
doses of these agents should be adjusted in patients with hepatic
insufficiency
). Elimination is through the urine.
• Side effect: Headache
is common. Electrocardiographic changes,
such as a prolonged QT interval, can occur with dolasetron.
GIT DRUGS
DR. JAMAL
7
3. Substituted benzamides
:
• It is commonly used as a
prokinetic drug (increase
the GIT motility).
• Example:
metoclopramide (plasil).
• Action: Antagonize D
2
receptors in CTZ
• Side
effects:
Antidopaminergic
side
effects,
including
sedation, diarrhea, and
extrapyramidal
symptoms, limit its high-
dose use.
4. Butyrophenones
:
• Example:
Droperidol
and haloperidol
• Action: By blocking dopamine receptors.
• Side effects: Prolong the QT interval, and current practice
reserves it for patients whose response to other agents is
inadequate.
5. Benzodiazepines
: The antiemetic potency of lorazepam and
alprazolam is low. Their beneficial effects may be due to their sedative,
anxiolytic, and amnesic properties. These same properties make
benzodiazepines useful in treating anticipatory vomiting.
6.
Corticosteroids:
Dexamethasone and methylprednisolone, used
alone, are mildly to moderately effective. Their antiemetic mechanism is
not known.
7. Substance P (neurokinin-1 receptor blocker):
• Aprepitant belongs to a new family of antiemetic agents. It targets
the neurokinin receptor in the brain and blocks the actions of the
natural substance.
• Aprepitant is usually administered orally with dexamethasone and
palonosetron.
• It undergoes extensive metabolism.
• Constipation and fatigue appear to be the major side effects.
• Aprepitant is only indicated for highly or moderately emetogenic
chemotherapy regimens.
8. Combination regimens:
Antiemetic drugs are often combined to
increase antiemetic activity or decrease toxicity.
GIT DRUGS
DR. JAMAL
8
H. ANTIDIARRHEALS
Increased motility of the gastrointestinal tract and decreased absorption of
fluid are major factors in diarrhea. Antidiarrheal drugs used to treat acute
diarrhea include antimotility agents, adsorbents, and drugs that modify
fluid and electrolyte transport.
A. Antimotility agents
• Two drugs that are widely used to control diarrhea are
diphenoxylate and loperamide.
• Both are analogs of meperidine and have opioid-like actions on the
gut. They activate presynaptic opioid receptors in the enteric
nervous system to inhibit acetylcholine release and decrease
peristalsis.
• At the usual doses, they lack analgesic effects.
• Side effects include drowsiness, abdominal cramps, and dizziness.
• Because these drugs can contribute to toxic megacolon, they
should not be used in young children or in patients with severe
colitis.
B. Adsorbents
• Adsorbent agents, such as aluminum hydroxide and methylcellulose
are used to control diarrhea.
• Presumably, these agents act by adsorbing intestinal toxins or
microorganisms and/or by coating or protecting the intestinal
mucosa.
• They are much less effective than antimotility agents and they can
interfere with the absorption of other drugs.
C. Agents that modify fluid and electrolyte transport Bismuth
subsalicylate, used for traveler’s diarrhea, decreases fluid secretion in the
bowel. Its action may be due to its salicylate component as well as its
coating action. Adverse effects may include black tongue and black
stools.
I. LAXATIVES
Laxatives are commonly used for constipation.
L Laxatives increase the potential for loss of pharmacologic effect of
poorly absorbed, delayed-acting, and extended-release oral preparations
by accelerating their transit through the intestines.
L They may also cause electrolyte imbalances when used chronically.
L All of these drugs, except for the chloride channel activator
lubiprostone, have a risk of dependency for the user.
These drugs can be classified on the basis of their mechanism of action.
A. Irritants and stimulants

GIT DRUGS
DR. JAMAL
9
1. Senna: This agent is a widely used stimulant laxative. Taken orally,
senna causes evacuation of the bowels within 8 to 10 hours. It also causes
water and electrolyte secretion into the bowel.
2. Bisacodyl: Available as suppositories and enteric-coated tablets,
bisacodyl is a potent stimulant of the colon. It acts directly on nerve fibers
in the mucosa of the colon.
Adverse effects include abdominal cramps and the potential for atonic
colon with prolonged use.
Milk and drugs that may increase the gastric pH, such as antacids, PPIs,
and H
2
-receptor antagonists, should not be taken at the same time as the
enteric-coated tablets. These agents may cause the enteric coating to
dissolve prematurely in the stomach, resulting in stomach irritation and
pain.
3. Castor oil: This agent is broken down in the small intestine to
ricinoleic acid, which is very irritating to the stomach and promptly
increases peristalsis. Pregnant patients should avoid castor oil because it
may stimulate uterine contractions.
B. Bulk laxatives
The bulk laxatives include hydrophilic colloids (from indigestible parts of
fruits and vegetables). They form gels in the large intestine, causing water
retention and intestinal distension, thereby increasing peristaltic activity.
Similar actions are produced by methylcellulose, psyllium seeds, and
bran. They should be used cautiously in patients who are immobile
because of their potential for causing intestinal obstruction.
C. Saline and osmotic laxatives
Saline cathartics, such as magnesium citrate, magnesium hydroxide, and
sodium phosphate are nonabsorbable salts that hold water in the intestine
by osmosis. This distends the bowel, increasing intestinal activity and
producing defecation in a few hours.
Electrolyte solutions containing polyethylene glycol (PEG) are used as
colonic lavage solutions to prepare the gut for radiologic or endoscopic
procedures.
Lactulose is a semisynthetic disaccharide sugar that also acts as an
osmotic laxative. It is a product that cannot be hydrolyzed by intestinal
enzymes. Oral doses are degraded in the colon by colonic bacteria into
acids. This increases osmotic pressure, causing fluid accumulation, colon
distension, soft stools, and defecation.
D. Stool softeners (emollient laxatives or surfactants)
Surface-active agents that become emulsified with the stool produce
softer feces and ease passage. These include docusate sodium, docusate
calcium, and docusate potassium. They may take days to become
effective and are often used for prophylaxis rather than acute treatment.
E. Lubricant laxatives

GIT DRUGS
DR. JAMAL
10
Mineral oil and glycerin suppositories are considered to be lubricants and
act by facilitating the passage of hard stools. Mineral oil should be taken
orally in an upright position to avoid its aspiration.
F. Chloride channel activators
Lubiprostone, currently the only agent in this class, works by activating
chloride channels to increase fluid secretion in the intestinal lumen.
This eases the passage of stools and causes little change in electrolyte
balances. It is used in the treatment of chronic constipation, particularly
because studies do not appear to show tolerance or dependency with this
drug. Also, drug–drug interactions appear minimal because metabolism
occurs quickly in the stomach and jejunum. Nausea is a relatively
common side effect with lubiprostone.