Fifth stage
MedicineLec-1
د.خالد نافع
4/10/2016
HematologyHematopoietic system
Blood
Spleen
Kidneys
Bone marrow
Liver
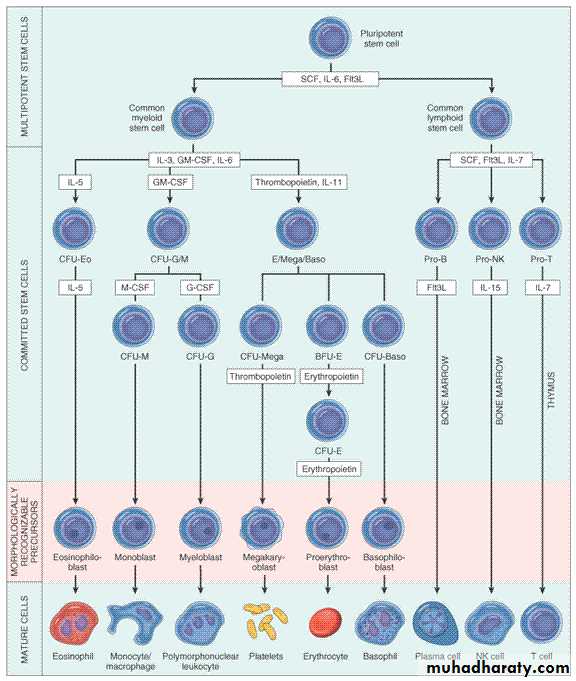
Cellular component
MARROW “DIFFERENTIATION”

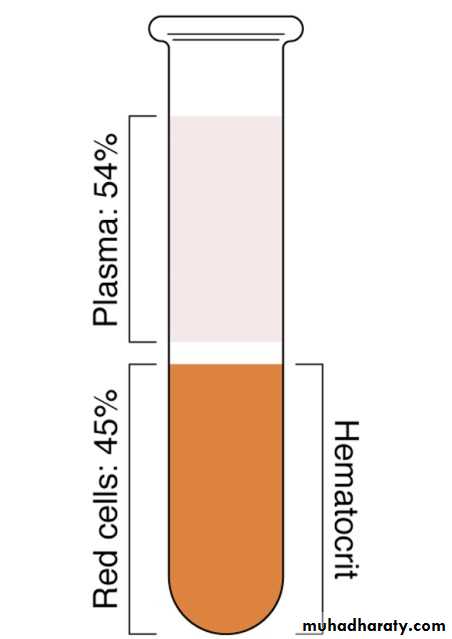
Components of Blood
PlasmaTransport mechanism
90-92% water.
6-7% proteins
2-3%
Fats
Carbohydrates (glucose)
Electrolytes
Gases (O2, CO2)
Chemical messengers
Red Blood Cells
Erythrocyte
Hemoglobin – O2 bearing molecule
Comprised of 4 subunits:
Globin (binds to 1 O2 molecule)
Heme (iron)
100% saturation = 4 globin subunits carrying O2
Each gram of hemoglobin = 1.34 ml O2
Red blood cell production
Erythropoiesis
Erythropoietin
Hemolysis
Sequestration
Laboratory analysis of red blood cells
Red blood cell count
Hematocrit
Hemoglobin
Platelets (Thrombocytes)
Megakaryocytes
Thrombopoietin
Thrombocytopenia
Thrombocytosis
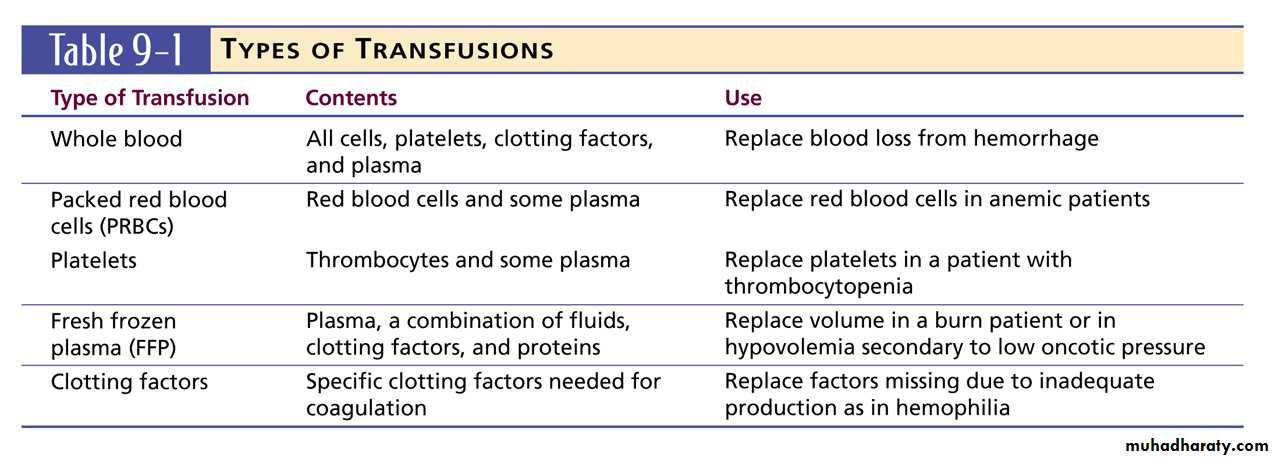
Blood Products and Blood Typing
Blood TypesAntigens
A, B, AB, O
Rh factor
Rh+ = ~85%
Rh- = ~15%
Diseases of Erythrocytes
Polycythemia
Overproduction of erythrocytes.Occurs in patients > 50 years old or with secondary dehydration.
Most deaths due to thrombosis
Results in bleeding abnormalities:
Epistaxis, spontaneous bruising, GI bleeding.
Management:
Follow general treatment guidelines.
Diseases of Leukocytes
LeukemiaCancer of hematopoietic cells
Initial presentation
Acutely ill, fatigued, febrile and weak, anemic.
Thrombocytopenia
Often have a secondary infection.
Management
Follow general treatment guidelines.
Utilize isolation techniques to limit risk of infection.
Lymphomas
Cancers of the lymphatic system
Hodgkin's
Non-Hodgkins
Presentation
Swelling of the lymph nodes
Fever, night sweats, anorexia, weight loss, fatigue, and pruritis
Management
Follow general treatment guidelines.
Utilize isolation techniques to limit risk of infection.
Leukopenia/Neutropenia
Too few white blood cells or neutrophils.
Follow general treatment guidelines and provide supportive care.
Leukocytosis
An increase in the number of circulating white blood cells, often due to infection.
Leukemoid reaction
Clotting Disorders
Thrombocytosis and Thrombocytopenia
Thrombocytosis
An abnormal increase in the number of platelets
Thrombocytopenia
An abnormal decrease in the number of platelets
Sequestration
Destruction (ITP)
Decreased production
Management
Provide supportive care and follow general treatment guidelines.
Hemophilia
Deficiency or absence of a blood clotting factor
Deficiency of factor VIII causes hemophilia A.
Deficiency of factor IX causes hemophilia B.
Deficiency is a sex-linked, inherited disorder.
Defective gene is carried on the X chromosome.
Signs & Symptoms
Numerous bruises, deep muscle bleeding, and joint bleeding.
PRINCIPLES OF HEMATOLOGICAL DIAGNOSIS
1.HISTORYI-Medical history
A.The present illness, focus on the following:
1.Bleeding.
2.Infection or symptoms related to enlargement of L.N , LIVER or the SPLEEN.
3.Non-specific symptoms related to ANAEMIA:Malaise , weakness, headache & weight loss.
B. Any exposure to drugs or chemical.
C. Review of systems; including the nervous system, is necessary as blood dyscrasia effect many, if not all, organ systems .
II- Family history; information about the health of other family members as well as the ethnic background .
2- PHYSICAL EXAMINATION
A- Thorough physical exam. Should focus on; SKIN, MOUTH ,MUCOUS MEMBRANE,& EYES.
JAUDICE
PALLOR
PETECHIAE & ECCYMOSIS.
ULCERS
B- Hepatomegaly, splenomegaly,enlarged or tender L.N ,soreness over the ribs or sternum & variety of neurological abnormalities.
ANAEMIA
A-Symptoms & signs pertaining to anaemia.
1-Non-specific symptoms include; fatigue, weakness, shortness of breath & symptoms of CHF
2-Signs include ; Pallor ,tachycardia , splenomegaly in minority of cases. Venous hum in severe anaemia ( Hb < 4 gm/dl).Functional systolic murmur.
B-SYMPTOMS & SIGNS Specific To IRON deficiency
1- Atrophic changes in the epithelium;a- oral lesions;
I- Angular cheilosis; soreness & cracking in the corners of the lips.
II-Atrophy of the tongue papillae with intermittent glossitis
III-Stomatitis ; inflammation & soreness of the tongue & mouth.
2-DYSPHAGIA.
3- Nail lesions; thinning & flattening of the nails progress to brittle & spoon-shaped nail ( koilonychia)
PLATELETS
NORMAL PLATELET COUNT 150-400X109/LPLATELET disorders; Defect in countTHROMBOCYTOPENIA
Defect in function THROMBOASTHENIA.
CLINICAL MANIFESTATIONS;
1-PETECHIAE.
2-PURPURA
3-ECCHYMOSIS(BRUSIES)
4- HAEMATOMA
Diagnostic Approaches to Anemia
Is the patient anemic ?
How severe is the anemia ?What type of anemia ?
Why is the patient anemic?
What should be done ?
1- IS THE PATIENT ANAEMIC
Visual diagnosis of anemia; observation of paler.Measurement of Hb & HCT
MCV = HCT/RBCs X 10 ( 85-95)
MCH = Hb/RBC X 10 (29-31)
MCHC= Hb/HCT X 10 ( 33% ± 2)
CLASSIFICATON OF ANAEMIA According To Cell Indices
*Normocytic: MCV 85-95flMCH 28-32pg
MCHC 27-35g/dl
*Macrocytic: MCV > 100
MCH > 34
MCHC 31-32
*Microcytic: MCV < 70
MCH < 25
MCHC < 28
2-How Severe Is The Anemia?
Severity of anemia depend on:
1. Hb level & HCT
2. Rapidity of onset
Mild ; Hb > 9g/dl
Moderate ; Hb 6-9g/dl
Severe ; Hb< 6g/dl
Compensatory Mechanism In ANAEMIA
1.Cardiac Output.
2. 2,3Diphosphoglycerate
3-WHAT TYPE OF ANAEMIA?
1- Is the anemia accompanied by alteration in WBC orPlatelet ?2-Is it the result of reduced red cell production or increased cell destruction?
* RETICULOCYTE COUNT ( corrected )
1.High = increase cell destruction.
2.LOW = reduce cell destruction.
Information Gained From Clinical Examinations
Pallor of mucosa; anaemiaEnlarged lymph node ; systemic disease
Hepatosplenomegaly; systemic disease, chronic hemolysis
Bruises; Bleeding disorder
Jaundice; Hemolysis
Simple Laboratory Test To Evaluate Anemia
Hb, PCV(HCT), MCHC.
WBC count & differential.
Peripheral Smear.
Reticulocyte count.
Urinalysis.
Occult Blood In Stool.
Serum Iron ,Total Iron Binding Capacity(TIBC).
Serum vitamin B12, Folic acid level.
Indirect bilirubin.
Haptoglobin leve.
Direct Coob`s test.
Sickle Cell Preparation.
Hb- electrophoresis.
Hb A2 %.
Hb F.
Osmotic Fragility.
Autohemolysis.
Red Cell Enzyme Assay.
Heinz bodies.
Acid lysis.
Platelet Count.
Bone Marrow Biopsy & Aspiration.
4- Why Is The Patient Anemic?
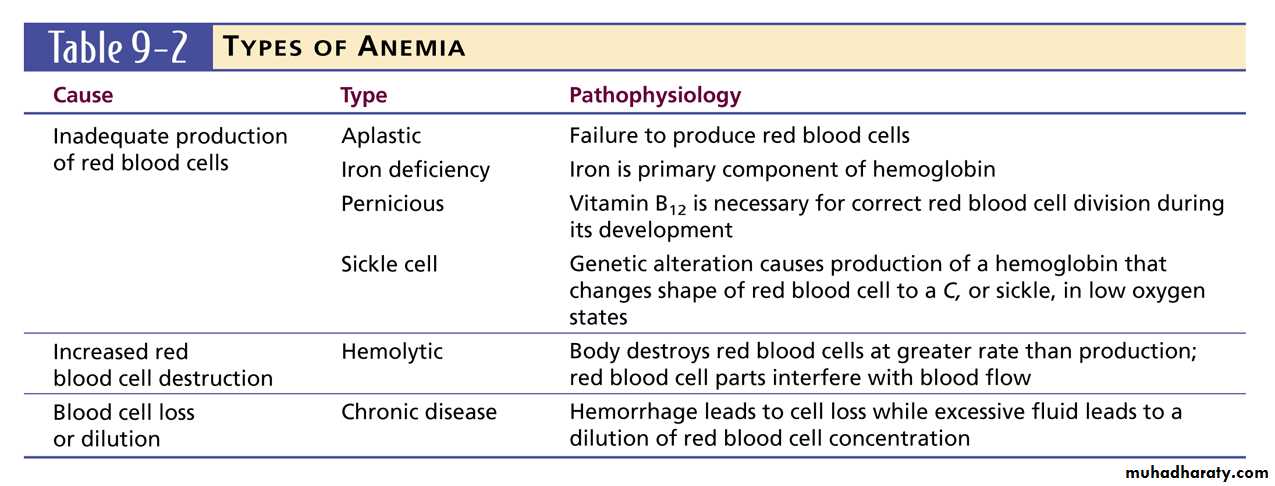
*Anemia due to decrease production of RBC
1-Lack of necessary nutrient;
a.Iron deficiency
b. Folic acid deficiency
c. Cobalamine deficiency
d.Combined deficiency
2-Bone Marrow defect;
* Generalized
a. Primary Aplastic Anemia. b. Replacement.
* Limited to RBC
a. Congenital b. Acquired
*Anemia Due to Excessive Destruction Of RBC
1.Formation of abnormal RBCA. Hb defect; Thalassemia.
B. Hereditary Spherocytosis.
C. Metabolic defect; Pyruvate kinase deficiency , other enzyme defect
2- Formation of RBC hypersensitive to hemolysis;
A. G6PD deficiency
B. Certain Hbpathies.
3- Presence of extracorpuscular factors
a. Immune hemolytic anemia
b. Cold agglutinin
c.Hemolytic uremic syndrome
d. Anemia of acute infection
e. Hypersplenism
f. Anemia of collagen disease.
5-What Should Be Done?
# Treatment of the cause, once recognized;
1- Available modality of treatment;
Iron, Folic acid , B12, B6, Steroid.
2- Splenectomy ; Indication
a. RBC coated by antibody.
b.Hereditary Spherocytosis.
c.Pyruvate Kinase deficiency.
3- Blood Transfusion ; Indication
a. Anaemia +CHF
b. Sickle cell anemia,Thalassemia
c. Failure of all logic approaches
d. Hb < 4 gm/dl.