Baghdad College of Medicine / 5
th
grade
Student’s Name :
Dr. Ahmed Khalaf
Lec. 1
Cleft lip & Cleft palate
Wed. 28 / 9 / 2016
DONE BY : Ali Kareem
مكتب اشو
ر لالستنساخ
2016 – 2017

Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
2
©Ali Kareem 2016-2017
Cleft lip and palate
Cleft lip and cleft palate are the second most frequently occurring of the major
congenital anomalies they occur in 1:750-1:1000 ,club foot being the most
common.
Racial and ethnic variations exist, with clefting occurring more commonly in
Asians and less frequently in Africans, while whites are intermediate in
occurrence.
Risk factors :
1- Medication: e.g. phyenytoin, steroid, diazepam, retinoic acid
2- Smoking.
3- Parental age especially father age, or both mother and father age over 30
years.
4- Family history: the risk increase with increase number of family who had
cleft lip. Most cases are sporadic (multifactorial), but may be X-linked, or
autosomal dominant e.g. Van der moude syndrome which is autosomal
dominant disorder with lower lip pits in association with different degree of
lip and palatal clefting Or associated with syndrome e.g. Down syndrome,
there are more than 150 syndromes described in which the clefting may be
a feature.
5- Folic acid and B6: intake during pregnancy may reduce cleft lip and cleft
palate.
6- low socioeconomic status : this is possibly related to inadequate nutrition.
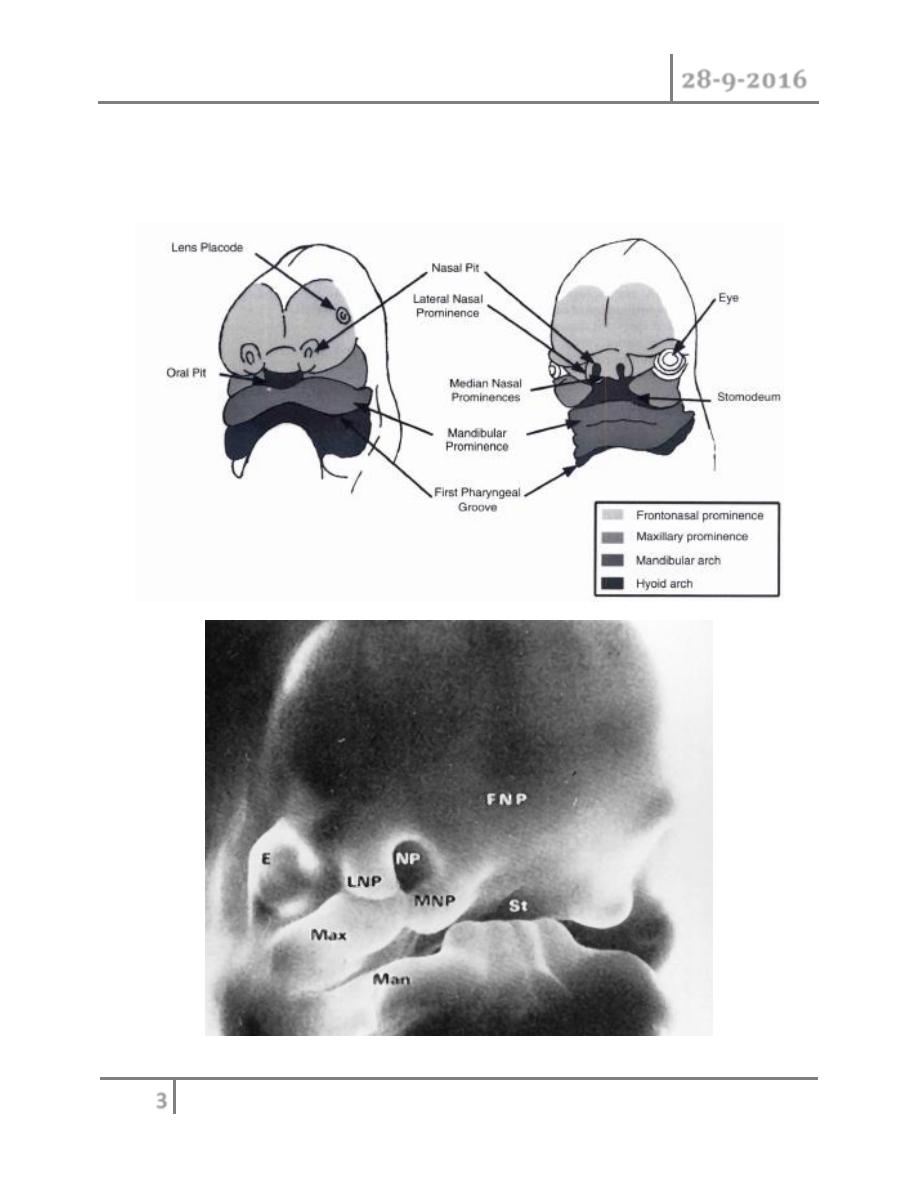
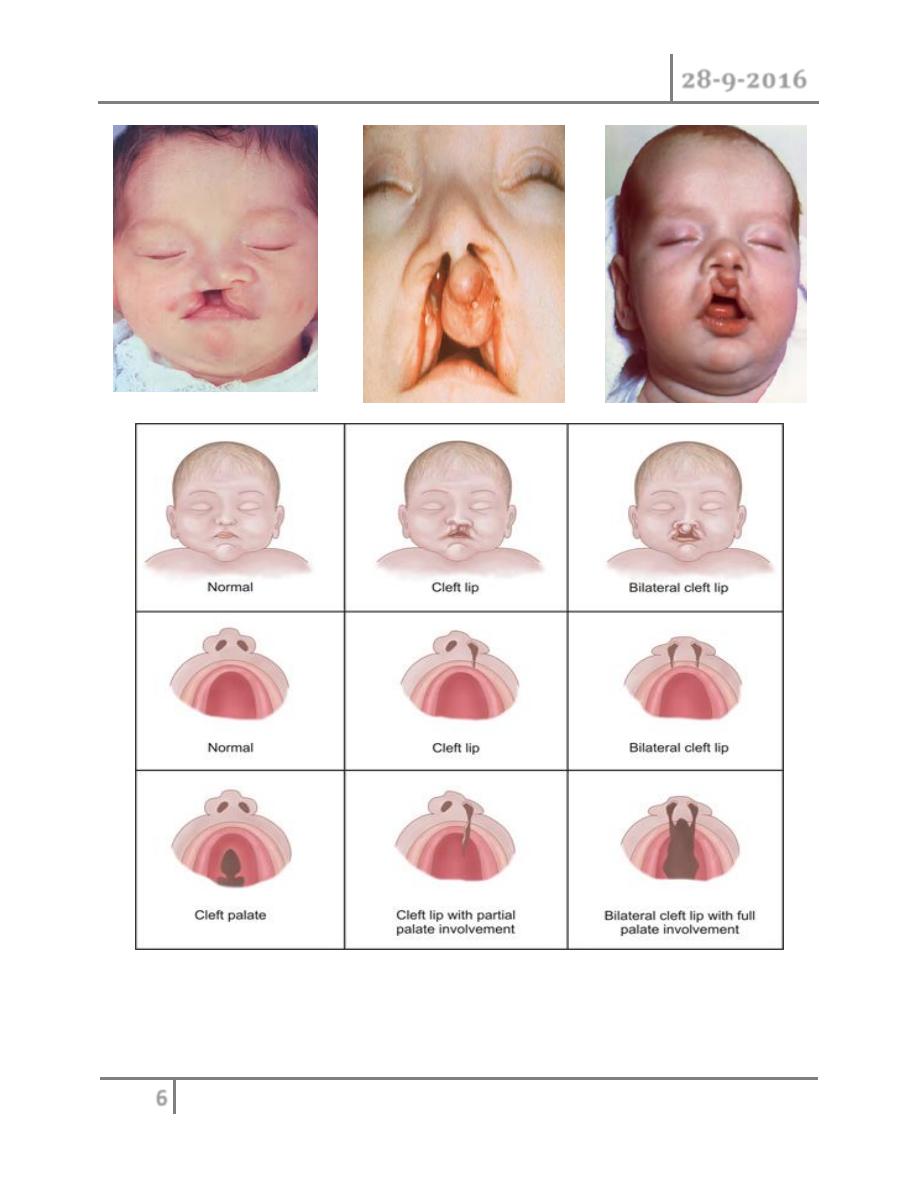
Cleft lip :
o The critical developmental period of lip and primary palate occur during 4-
6 weeks of gestation.
o Unilateral cleft lip result from failure of fusion of medial nasal prominence
and maxillary prominence on one side.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
3
©Ali Kareem 2016-2017
o Bilateral cleft lip result from failure of fusion of medial nasal prominence
with maxillary prominence on either site. Male to female ratio 2:1, left side
more common than right side.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
4
©Ali Kareem 2016-2017
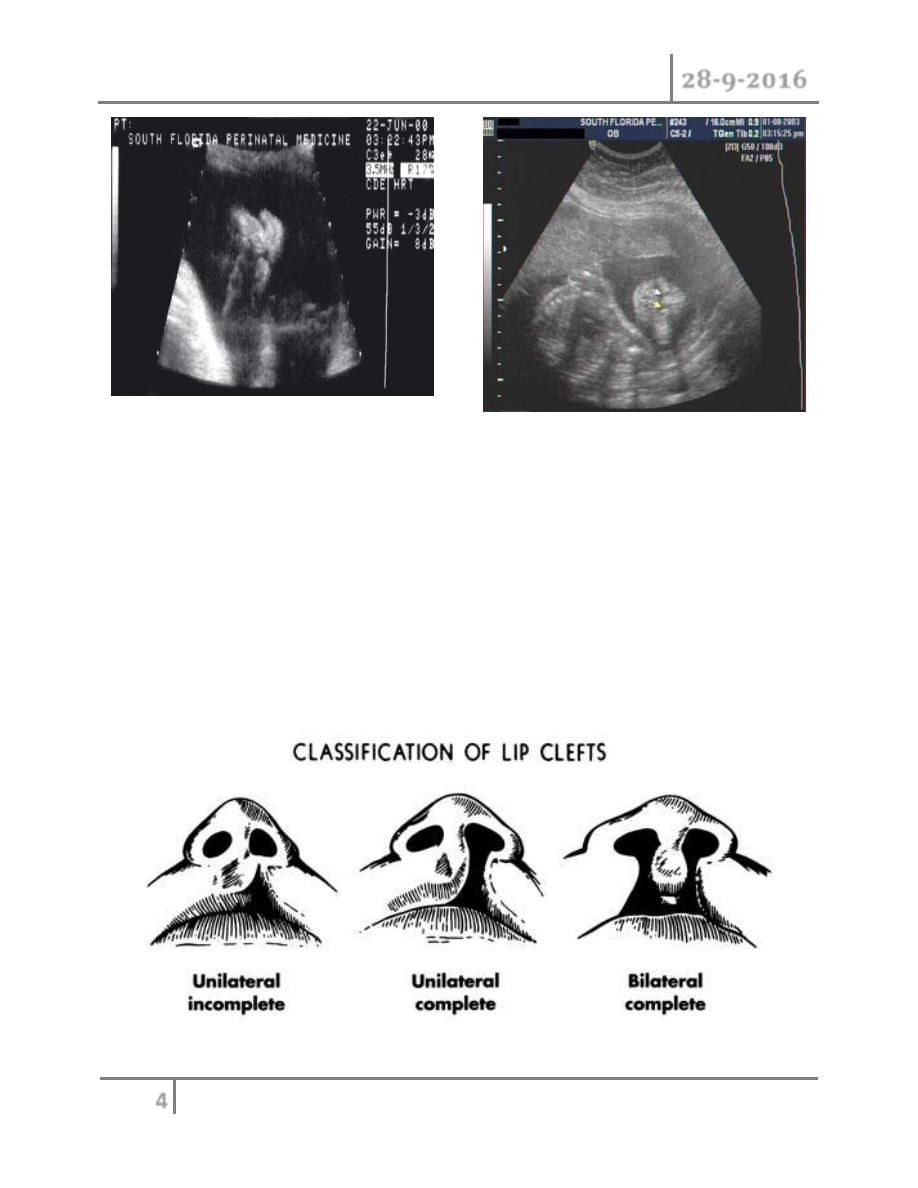
Classification of cleft lip:
1- according to extent of cleft lip:
o Microform cleft lip : furrow or scar through the vertical length of lip.
o Incomplete cleft lip : vertical separation of lip (skin, orbicularis
muscle and mucosa) with intact nasal sill.
o Complete cleft lip : vertical separation of the lip, nasal sill and
alveolus.
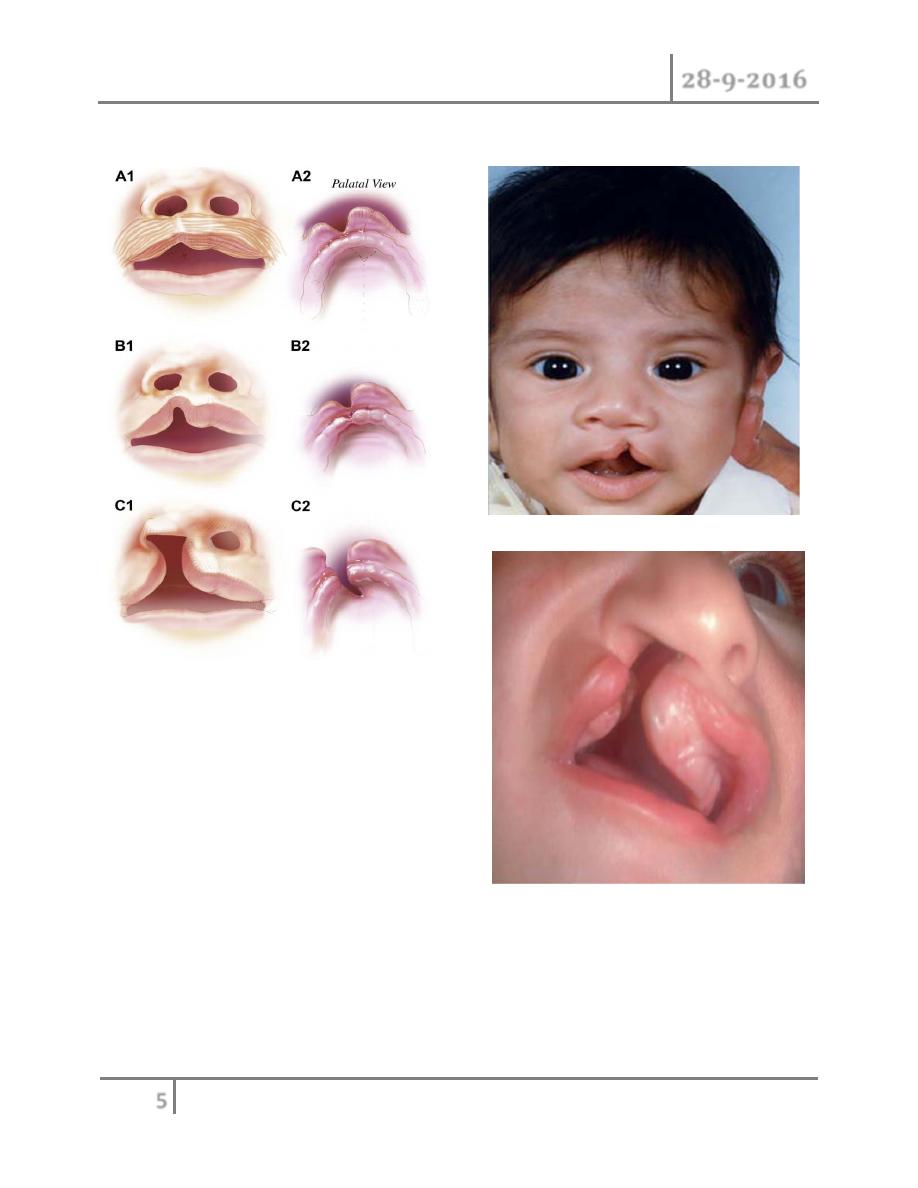
Unilateral cleft lip
Bilateral cleft lip and palate
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
5
©Ali Kareem 2016-2017
2- according to location of the cleft :
o Unilateral cleft lip.
o Bilateral cleft lip.
For both of above may be complete or incomplete or microform.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
6
©Ali Kareem 2016-2017
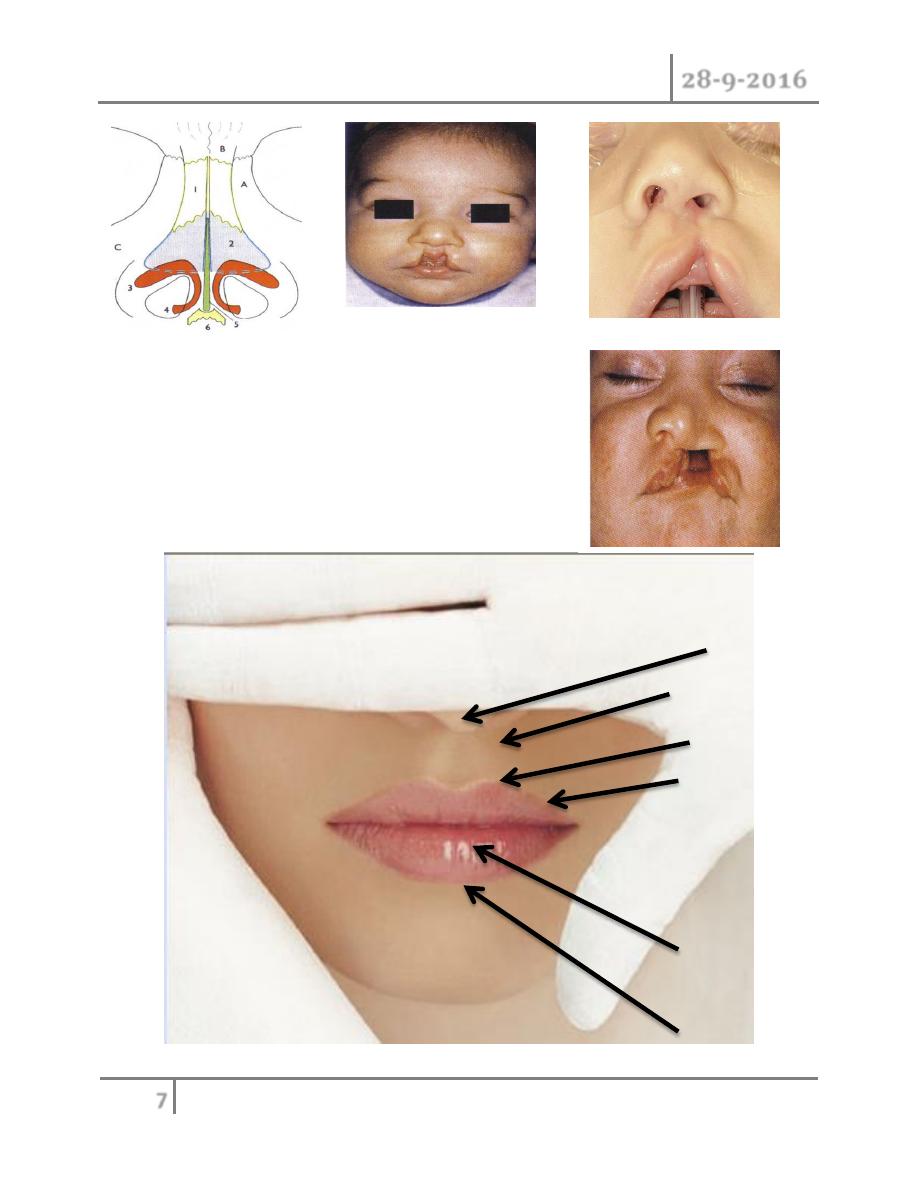
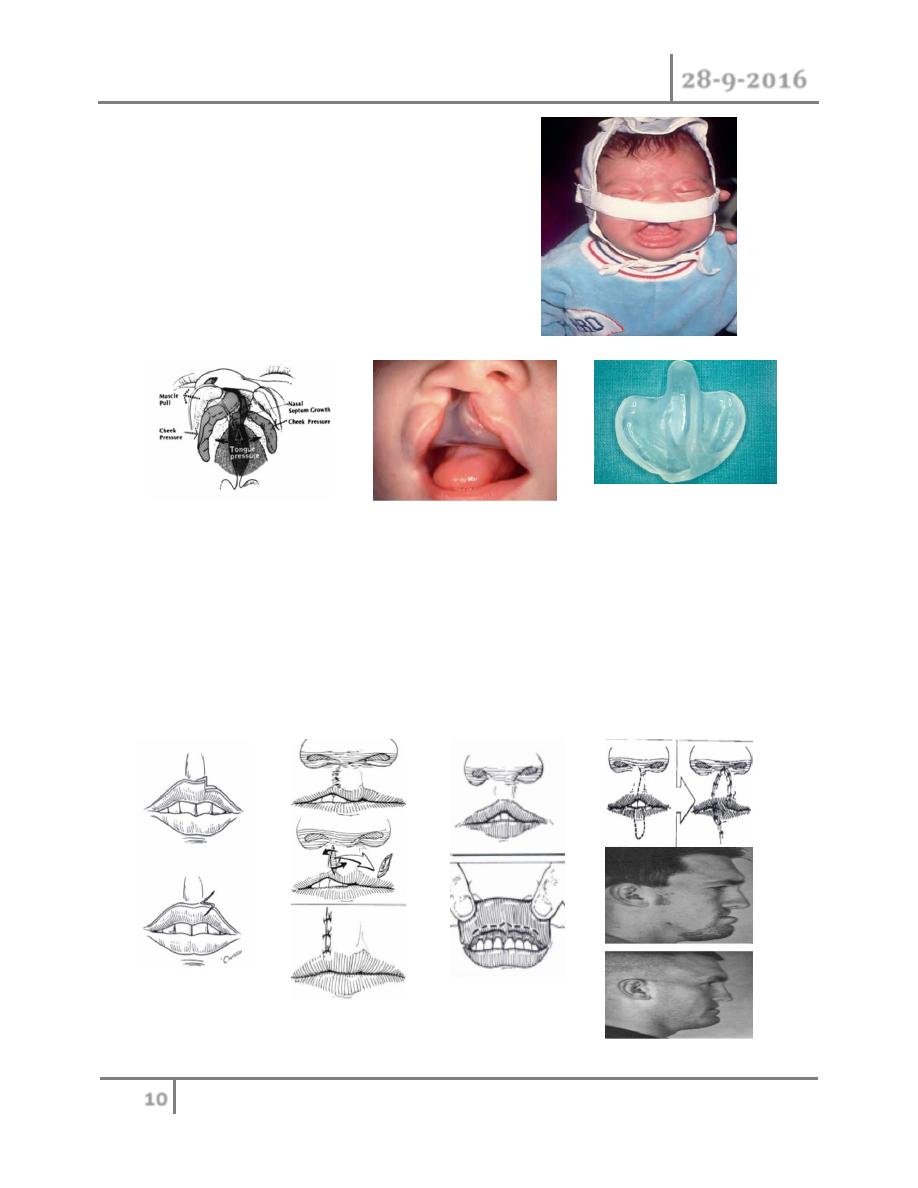
Cleft lip may be associated with nasal deformity, which could be mild, moderate or
severe nasal deformity.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
7
©Ali Kareem 2016-2017
Normal anatomy of lip :
1- Topographic landmark.
Columella
Philter columns
Cupid’s bow
Vermillion roll
Wet vermillion
Dry vermillion
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
8
©Ali Kareem 2016-2017
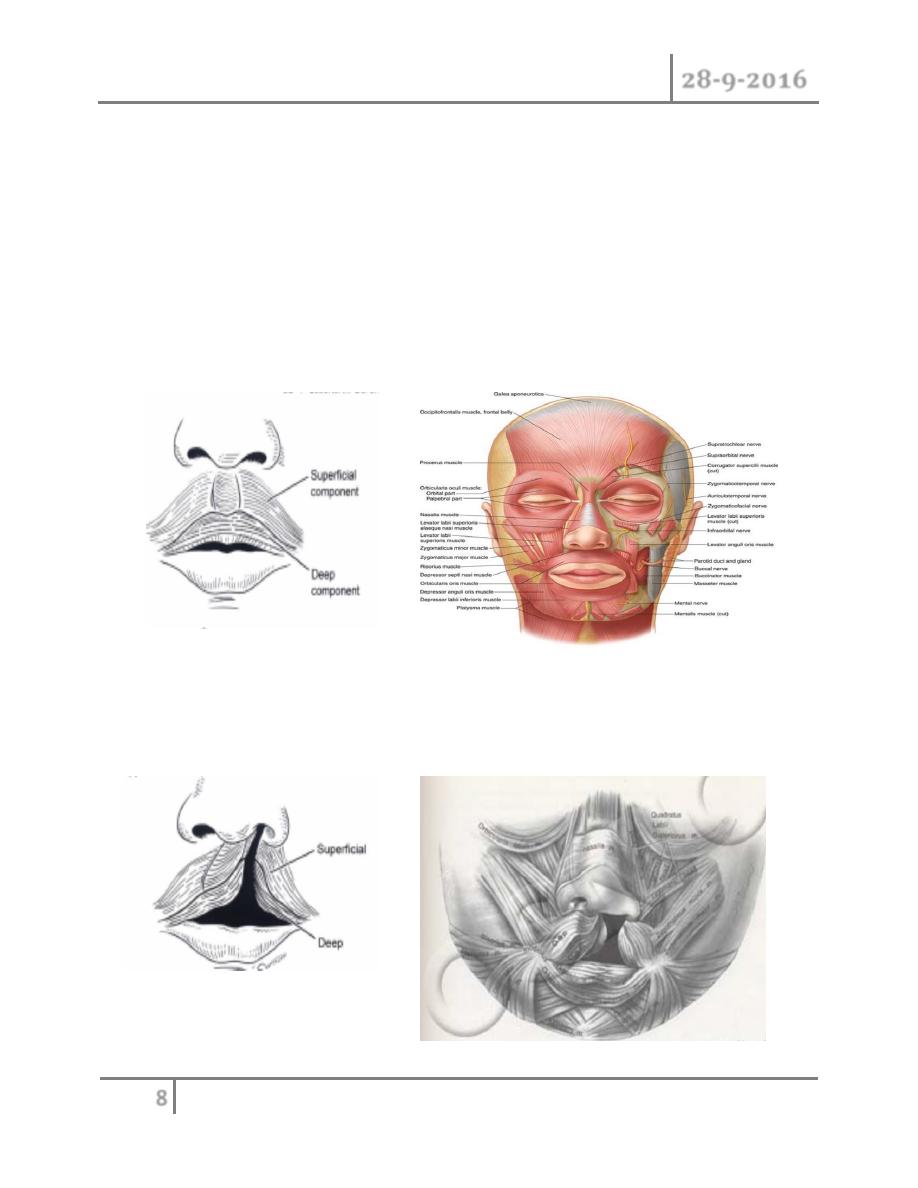
2- muscles:
o Orbicularis oris: function as sphincter (deep fibers) and for speech
(superficial fibers).
o Levator labii superoris: elevate the upper lip.
o Nasalis or depressor septi nasi muscle: depress the columella down
and elevate the upper lip.
3- Arterial blood supply: by labial artery bilaterally.
4- Sensory innervation: by maxillary branch of trigeminal nerve.
5- Motor innervation: by zygomatic and buccal branches of facial nerve.
Cleft lip anatomy :
1- Disruption of continuity, orientation and quality of muscles.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
9
©Ali Kareem 2016-2017
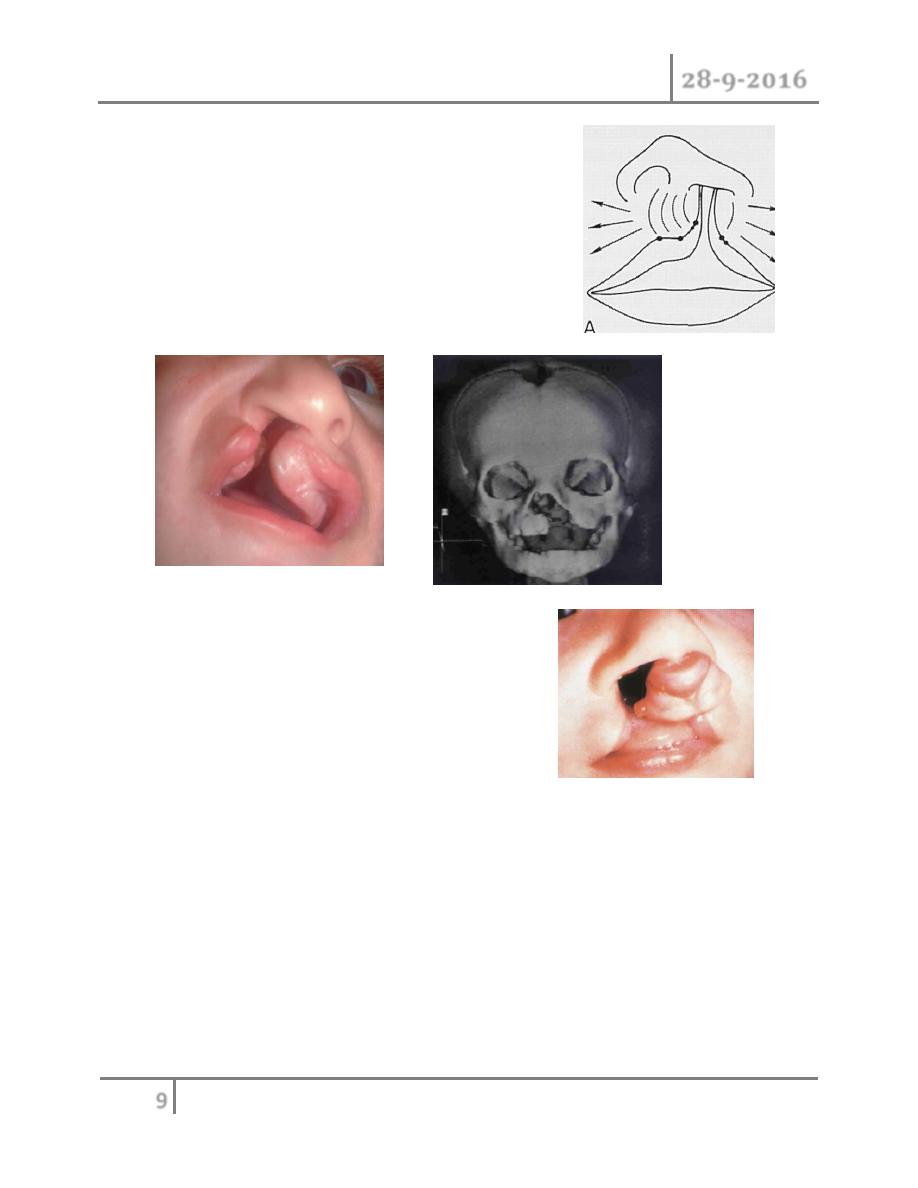
2- Cupid bow and lip rotated upward
on both the lateral –cleft side-as
well as medial side.
3- The alveolus and nostril floor are
open in complete cleft lip.
4- The premaxilla is rotated and protruding
especially in bilateral cleft lip.
Management :
o The parents should be reassured, and the newborn should evaluate for
associated anomalies, and the parents should inform about the stages and
operation that expected throughout the child lifetime.
o Time of repair: according to rules of ten:
o Should be 10 weeks old.
o Should be 10 pounds (4.5kg).
o Should be 10gm/dl hemoglobin level.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
10
©Ali Kareem 2016-2017
Preoperative measurement :
1- Elastic head cap: used in first week of
life especially for projected premaxill
in bilateral cleft lip.
2- Maxillary orthopedic: for collapsed
maxillary arches at (1-2) weeks of age.
Notes :
1- Initial lip procedure at (10-12 weeks) of age.
2- Columellar lengthening at (18 months) of age.
3- Time of revision should be complete at age (5-6 years) i.e. preschool age.
4- Final nasal deformity revision in adolescent.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
11
©Ali Kareem 2016-2017
Surgical treatment :
• Preoperative investigation: chest X-ray to exclude any chest infection,
bleeding profile to exclude any bleeding tendencies and Hb level.
Principal of repair :
1- Produce functional continuity of muscles.
2- Recreate symmetry.
3- Reconstruction Cupid bow.
4- Minimize scarring.
5- Treated the associated nasal deformity.
6- Should repair all layers of lip (skin, muscles, and mucos).
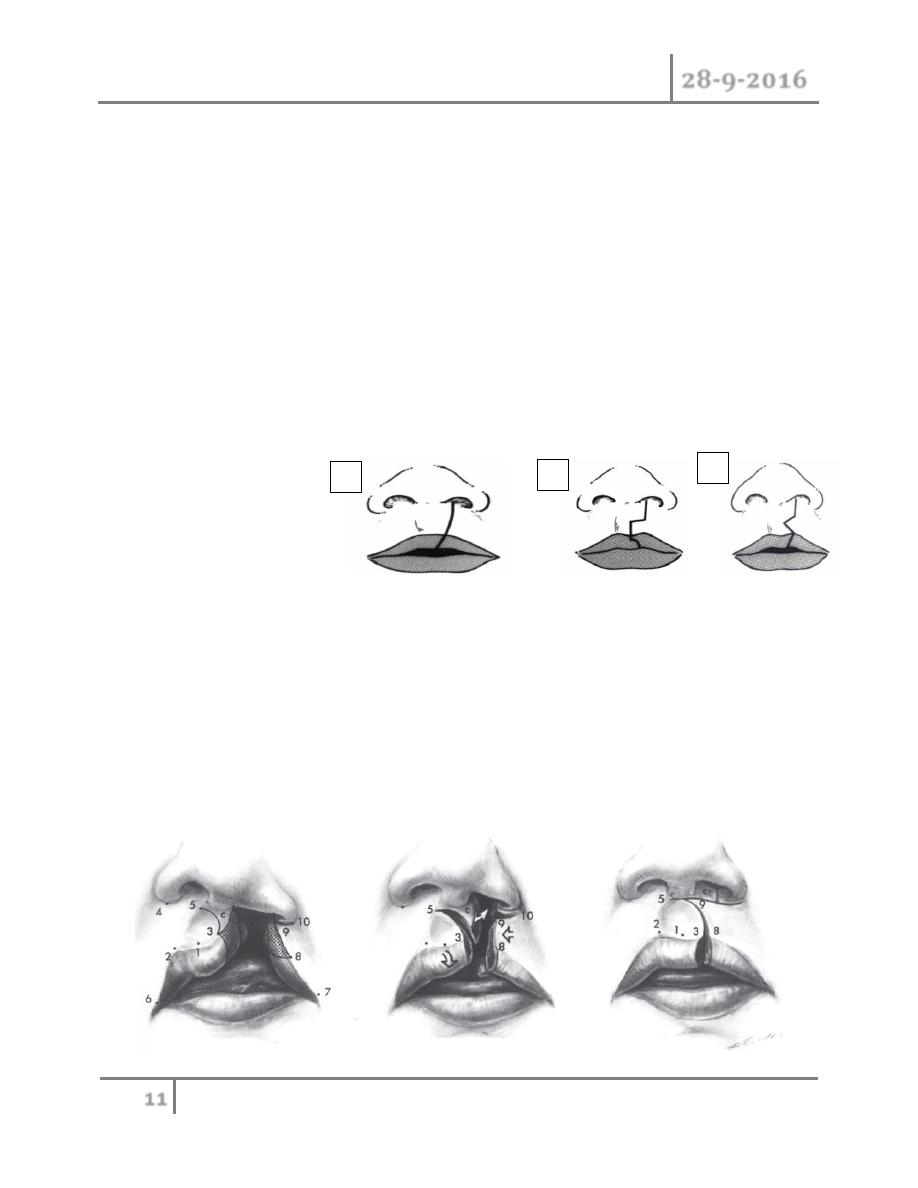
Methods of repair:
1- Straight line repair.
2- Lateral quadrilateral flap technique.
3- Lateral triangular flap technique.
4- Rotational advancement technique(Millard): most commonly used repair in
which the medial lip is rotated downward to fill the cleft defect, and lateral
lip is advanced to fill the defect that occur in place of medial lip ,with small
pennant shaped C-flap used either to create nasal sill or lengthened the
columella.
1
2
3
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
12
©Ali Kareem 2016-2017
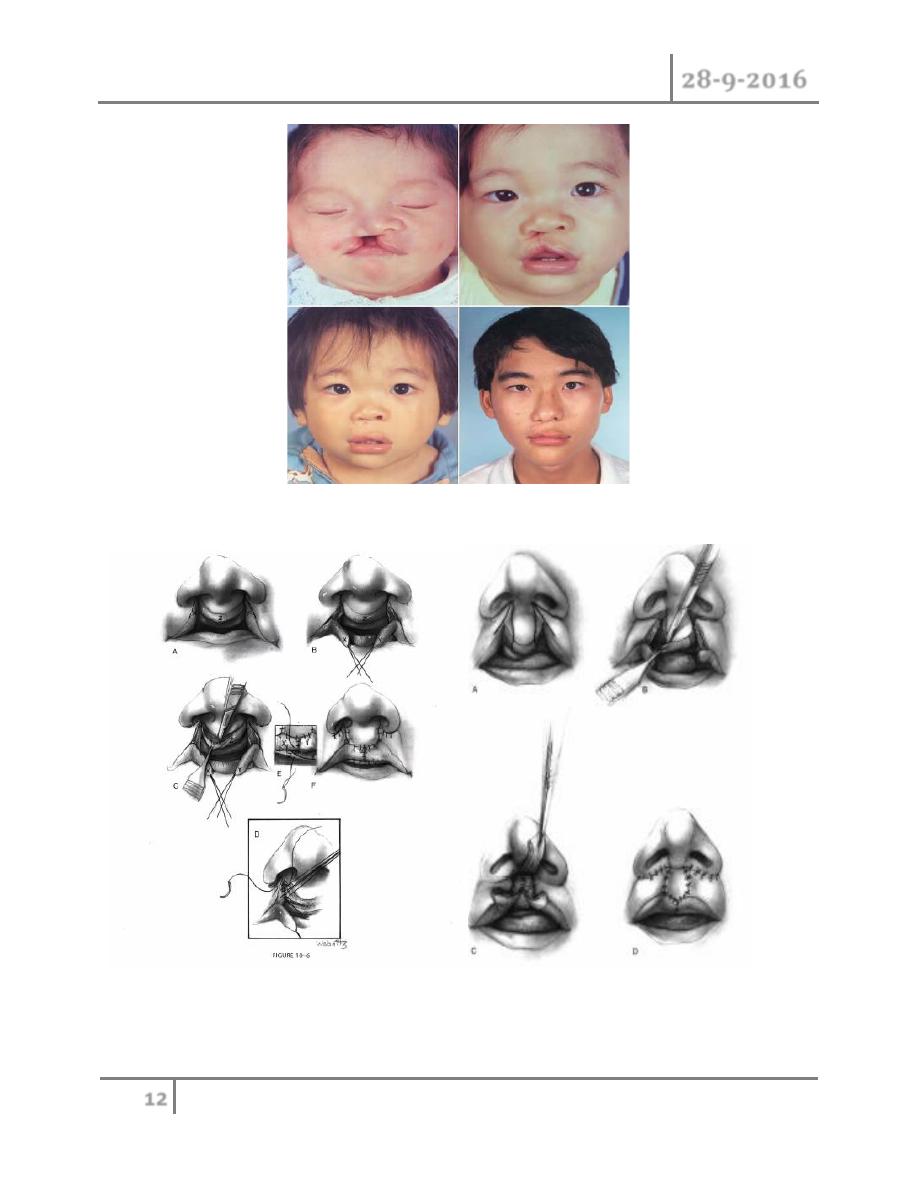
Repair of bilateral cleft lip
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
13
©Ali Kareem 2016-2017
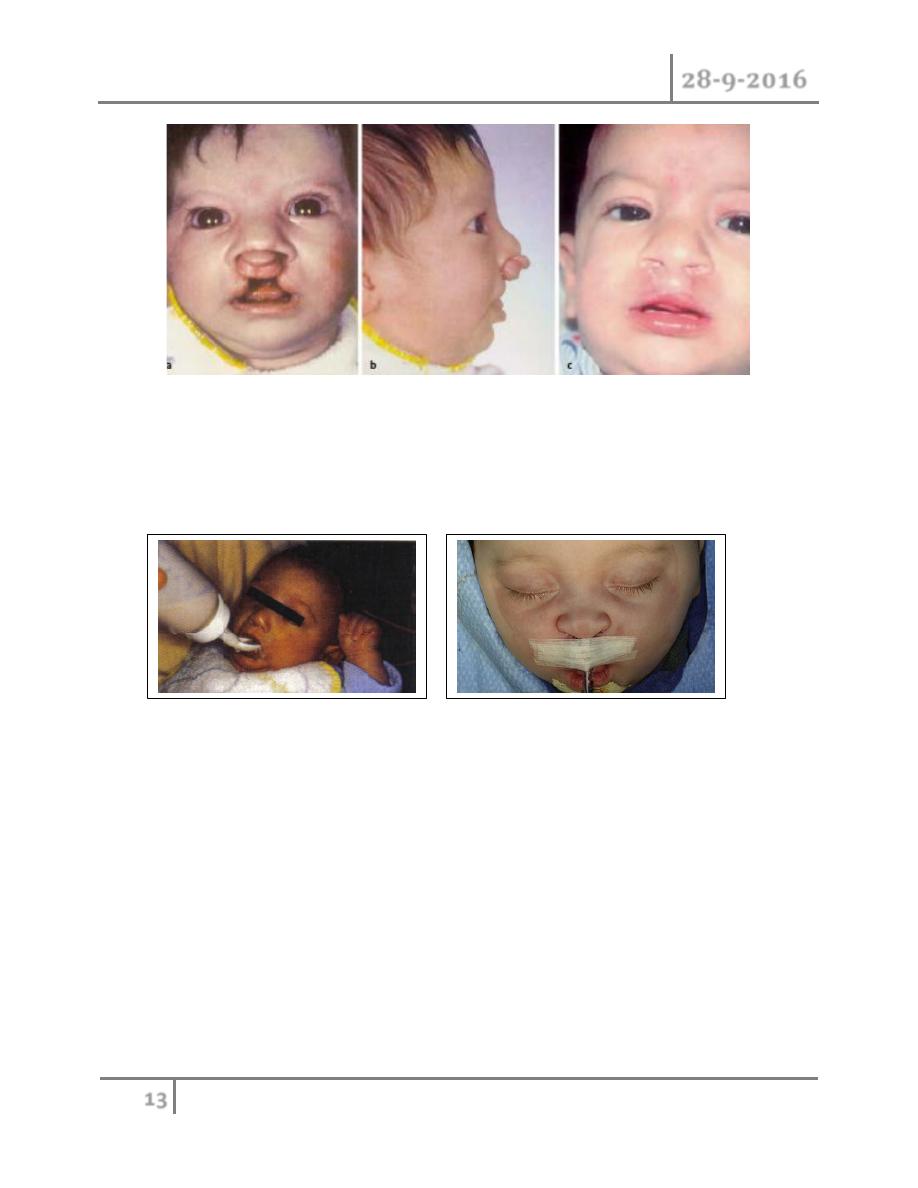
Postoperative care
o Avoid using nipple of bottle for feeding instead used spoon for feeding.
o Keep using tape in place for support after suture removal (usually suture
removed under general anesthesia after 5 days).
Cleft palate
o It could occur as separated deformity or in combination with cleft lip
deformity. It may be unilateral or bilateral deformity.
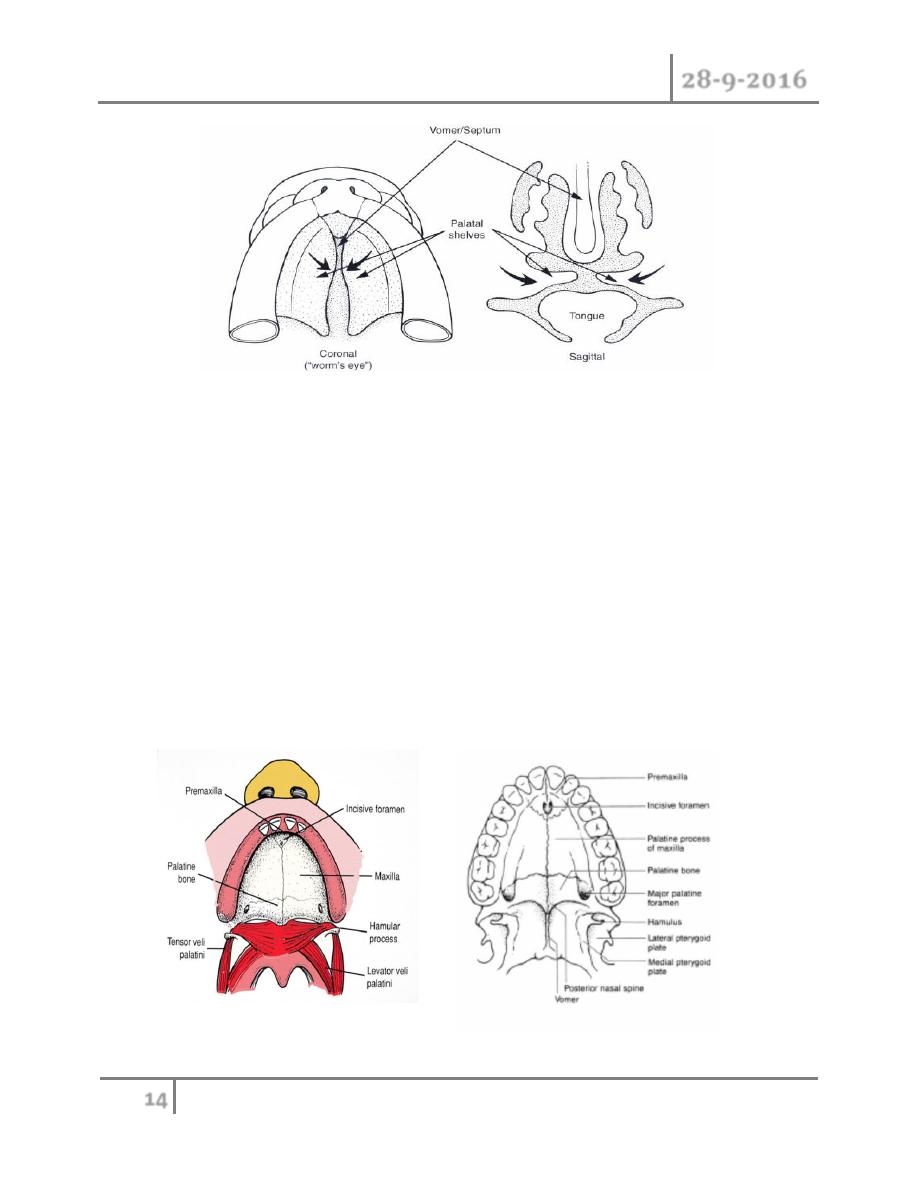
Embryology
o Cleft of the primary palate which located anterior to incisive foramen is
result from failure of the mesenchymal masses in the lateral palatine process
to fuse with those in median palatine process.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
14
©Ali Kareem 2016-2017
o cleft of the secondary palate which is located posterior to incisive foramen is
result from failure of the mesenchymal masses in the lateral palatine process
to fuse with each other and with nasal septum
, it is believed that delay in
elevation of the palatal shelves from vertical to horizontal is part of the
underlying mechanism.
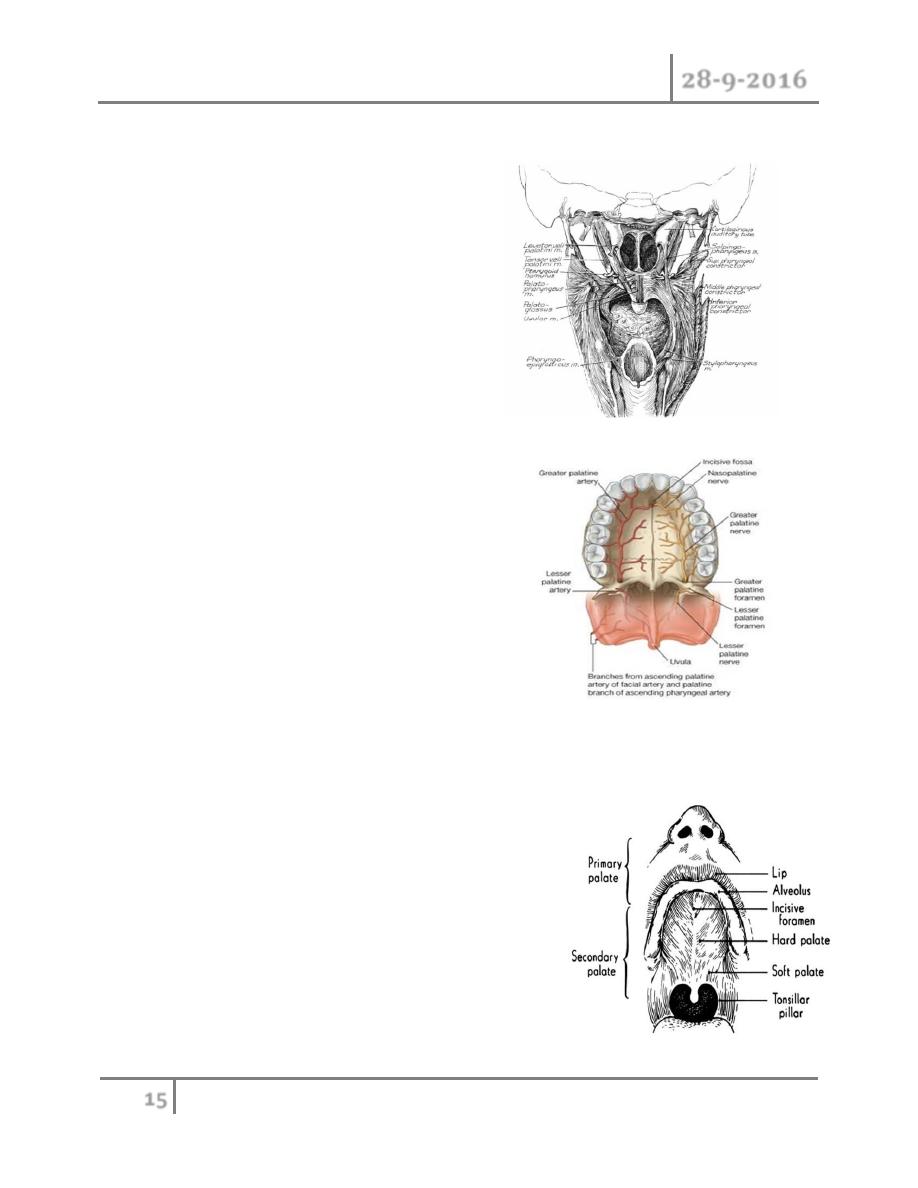
Anatomy :
1- Hard palate: it is the bony part consists of primary and secondary palate
which separated by incisive foramen. It consist of :
o Premaxilla, extended to incisive foramen.
o Paired maxilla.
o Palatine bone.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
15
©Ali Kareem 2016-2017
2- soft palate(velum): contains muscle involved in velopharyngeal closure
which:
1- extrinsic muscles:
o Levator palate muscle.
o Tensor veli palatini muscle.
o Palatopharyngeus
o Palatoglossus
o Salpingopharyngeus
o Superior constictor
2- intrinsic muscle:
o musculus uvulae
All are supply by vagus and glossopgaryngeal
nerve except the tensor veli palatini which
supply by trigeminal nerve.
Vascular and nerve supply of hard palate is
through the greater palatine artery and nerves
through the greater palatine foramen.
Secondary blood supply through the lesser
palatine artery and nerve through lesser palatine foramen
o The prepalatal structures (primary palate):
structure anterior to incisive foramen
(alveolus, lip, nasal floor, and alar cartilage).
o The palatal structures (secondary palate):
those posterior to incisive foramen.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
16
©Ali Kareem 2016-2017
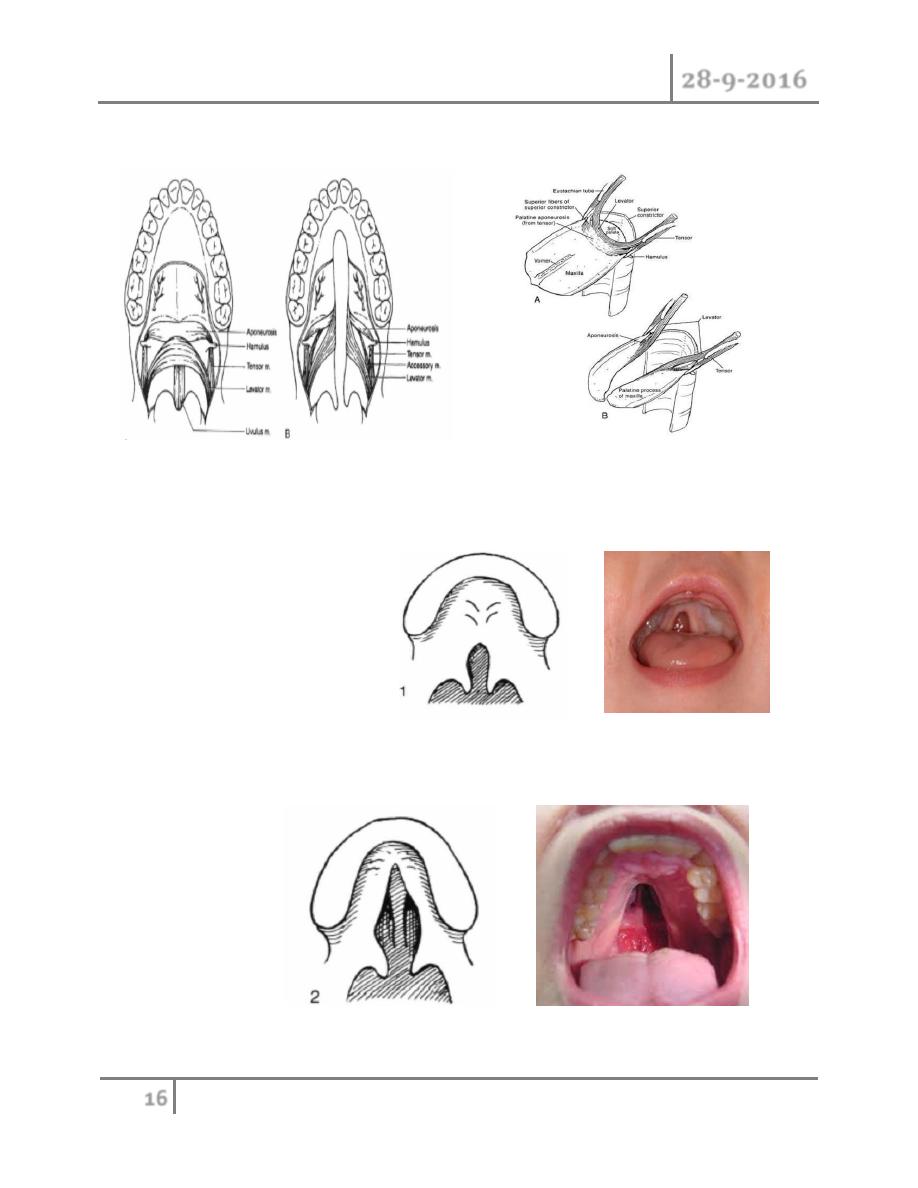
Cleft palate anatomy :
Classification of cleft palate :
Veau described a classification divided into four groups:
group 1: cleft of the soft palate.
Group 2: cleft of the hard and soft palate up to incisive foramen involving the
secondary palate.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
17
©Ali Kareem 2016-2017
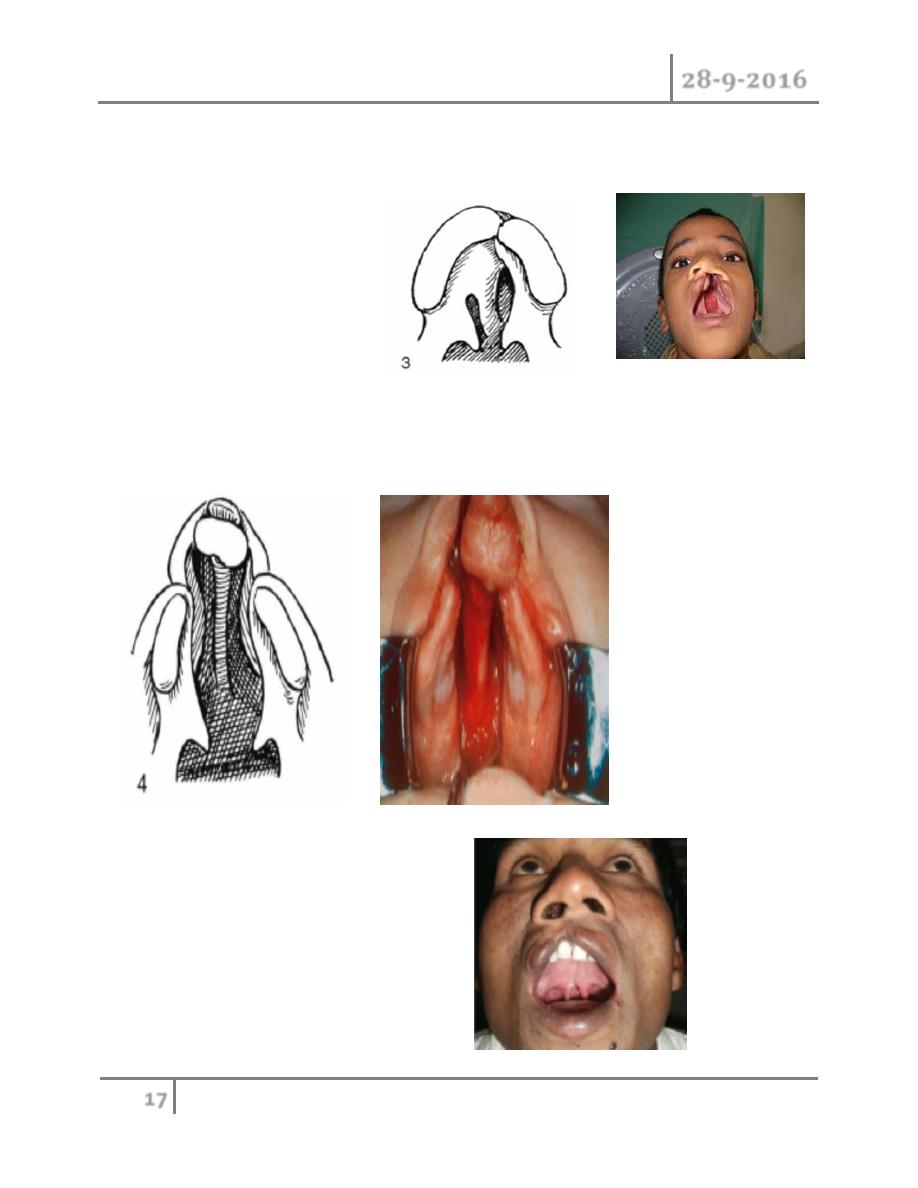
Group 3: complete unilateral cleft, extending from uvula to the incisive foramen in
midline , then reflecting to one side and extending through alvelous at the position
of future lateral incisor tooth
Group 4: complete bilateral cleft, resembling group 3 with two cleft projecting
forward from incisive foramen through alveolus; the small anterior segment of
palate, the premaxilla, remains suspended from the nasal septum.
other rare type of cleft palate include:
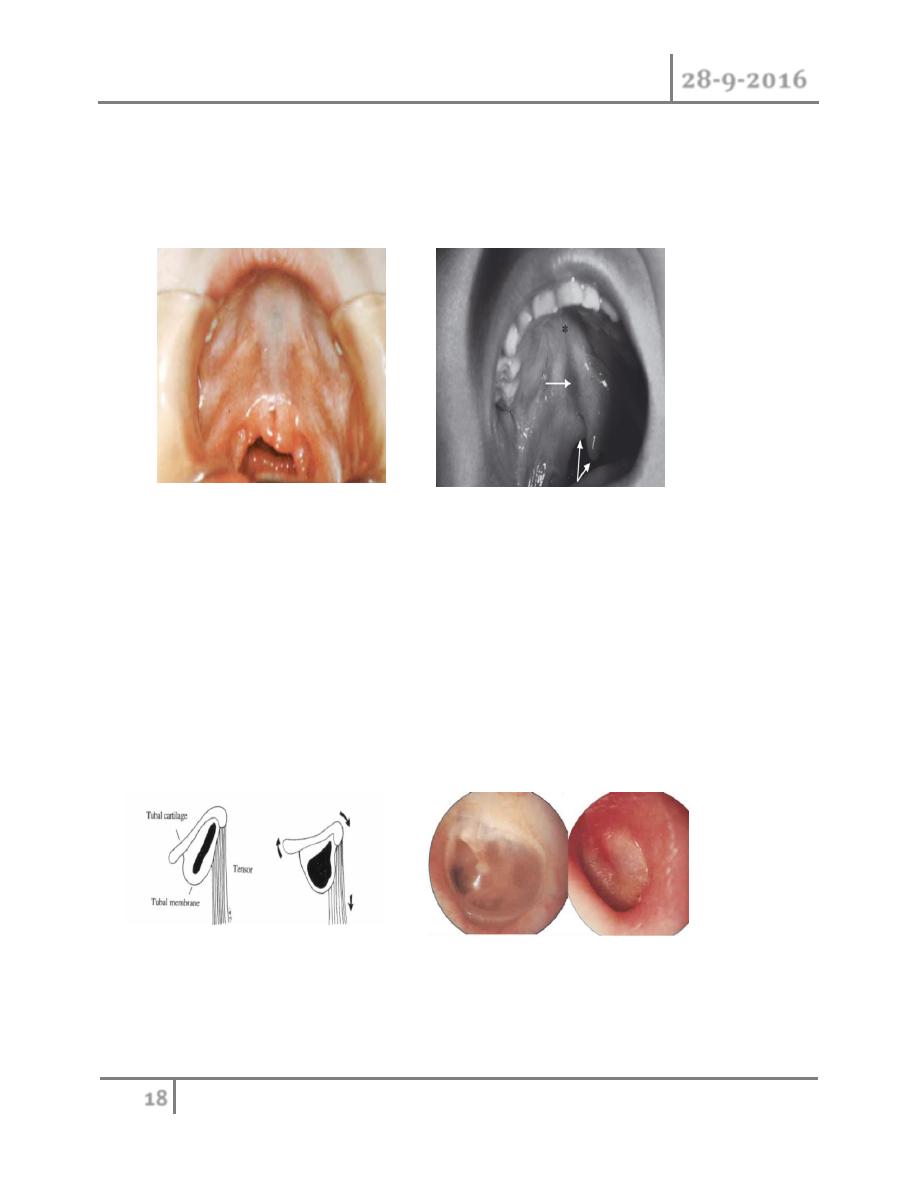
Bifid uvula :
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
18
©Ali Kareem 2016-2017
o Submucous cleft : bifid uvula plus dehiscence of levator muscle plus short
palate plus notch of posterior third of bony palate. the majority of the
patients with submucous cleft palate are asymptomatic, although
approximately 15% will develop velopharyngeal insufficiency (VPI)
Management :
1- Feeding: since the baby with cleft palate is unable to create adequate
suction so that the feeding should be done with nipple with large holes, and
baby should hold in 45° degree to decrease regurgitation into the nose, and
feeding should take longer time.
2- Maintenance airway by prone position during sleeping.
3- Patient usually has otitis media because of Eustachian tube abnormalities
the child need careful fallow up with otolaryngologist and audiologist.
4- Associated deformity occurs in about 29% of children with cleft palate.

Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
19
©Ali Kareem 2016-2017
Surgical correction :
Time usually between ages of 9-11 months.orthopaedic appliances should be
wear by patient before surgery.
Goals of reconstruction:
1- Recreate a continuous hard palate with palatal tissue that allow no
communications between oral and nasal cavities.
2- Reconstruct the muscular anatomy to that of normal to allow the action of
the levator veli palatini muscle to elevate the mobile soft palate and separate
the nose.
These goals should be accomplished without creating significant scarring of
maxilla which increase the incidence of midface retrusion.
Surgical procedures are :
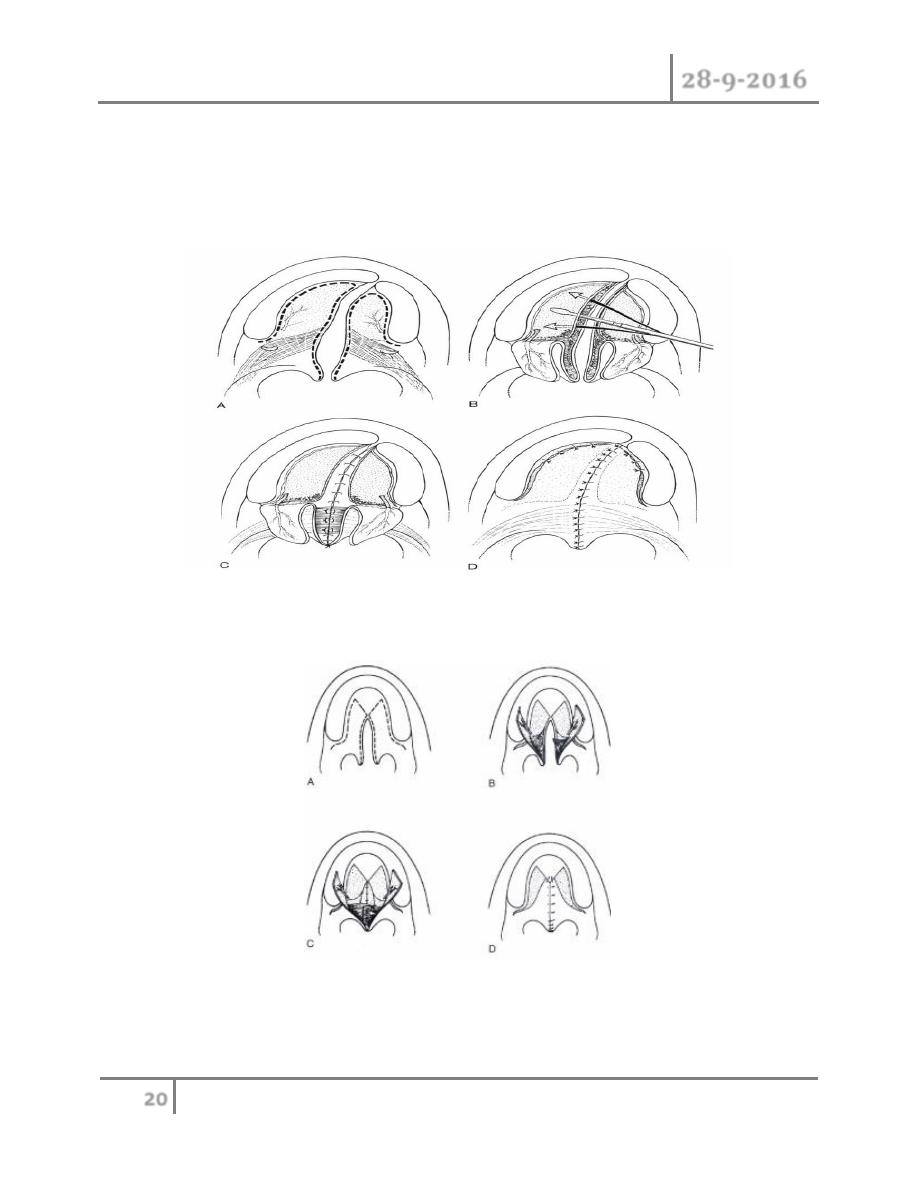
1- Bilateral bipedicled mucoperiosteal flap (Von Longenbeck repair): the flaps
are elevated and then closed at midline, nasal mucosa first and oral mucosa
last. This technique is not involving elongation of palate.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
20
©Ali Kareem 2016-2017
2- Two flap palatoplasty (Baradach): its modification of Langenbeck techniqe,
where the incision extend along the alveolar margins to edge of cleft.making
the flap entirely dependent on circulation from greater palatine artery. This
technique is not involving elongation of palate.
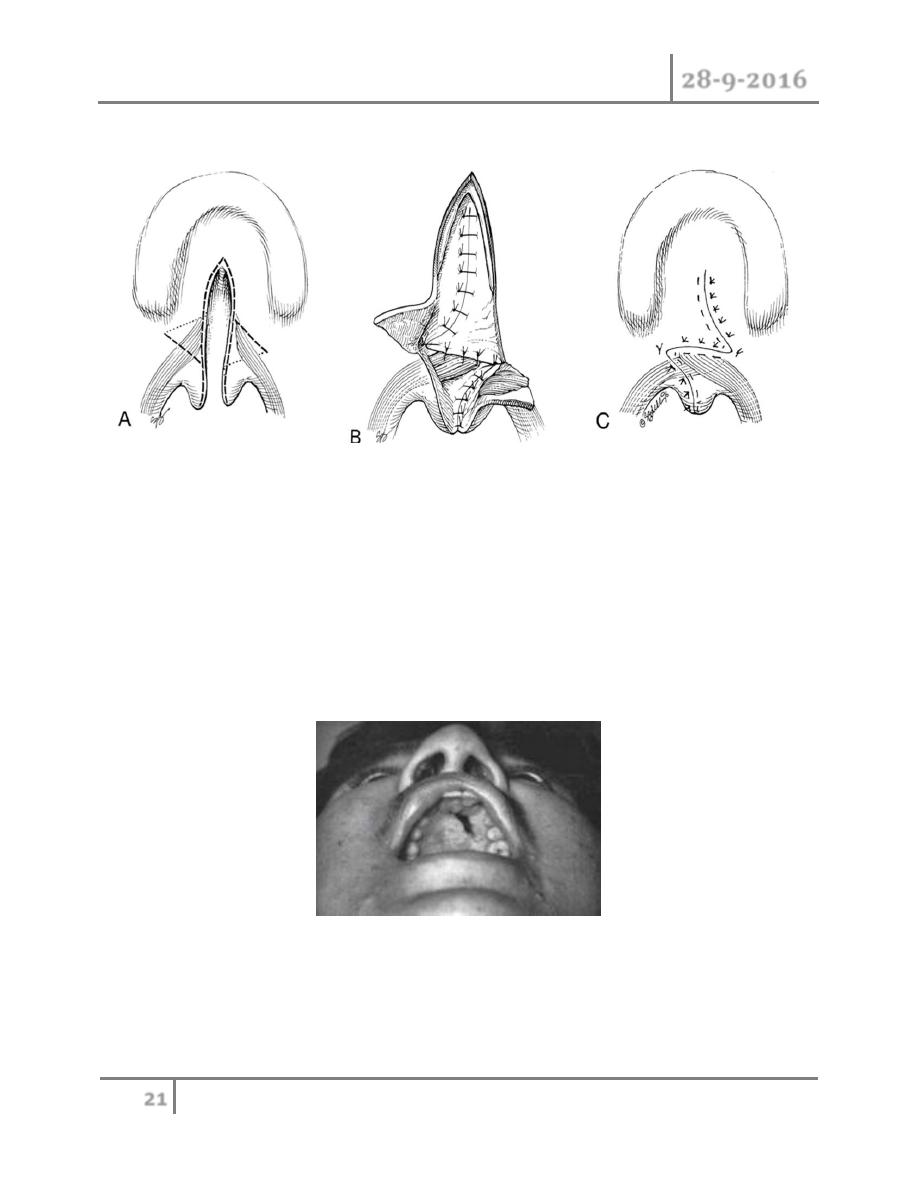
3- V-Y elongation technique (Veau-Wardil-kilner). This technique is involving
elongation of palate.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
21
©Ali Kareem 2016-2017
4- Furlow technique: soft palate elongation with double reversing Z-plasties
Postoperative care:
o Elbow restrain are worn continually for 4-6 weeks.
o The airway is observed and the child placed on oxygen monitor.
o Patient are given liquid only diet for 3 week and child is transitioned to soft
diet for an additional 3 weeks.
Surgical complication of cleft palate surgery :
1- Fistula: most common in wide bilateral cleft palate.
2- Airway obstruction may occur secondary to postoperative bleeding.
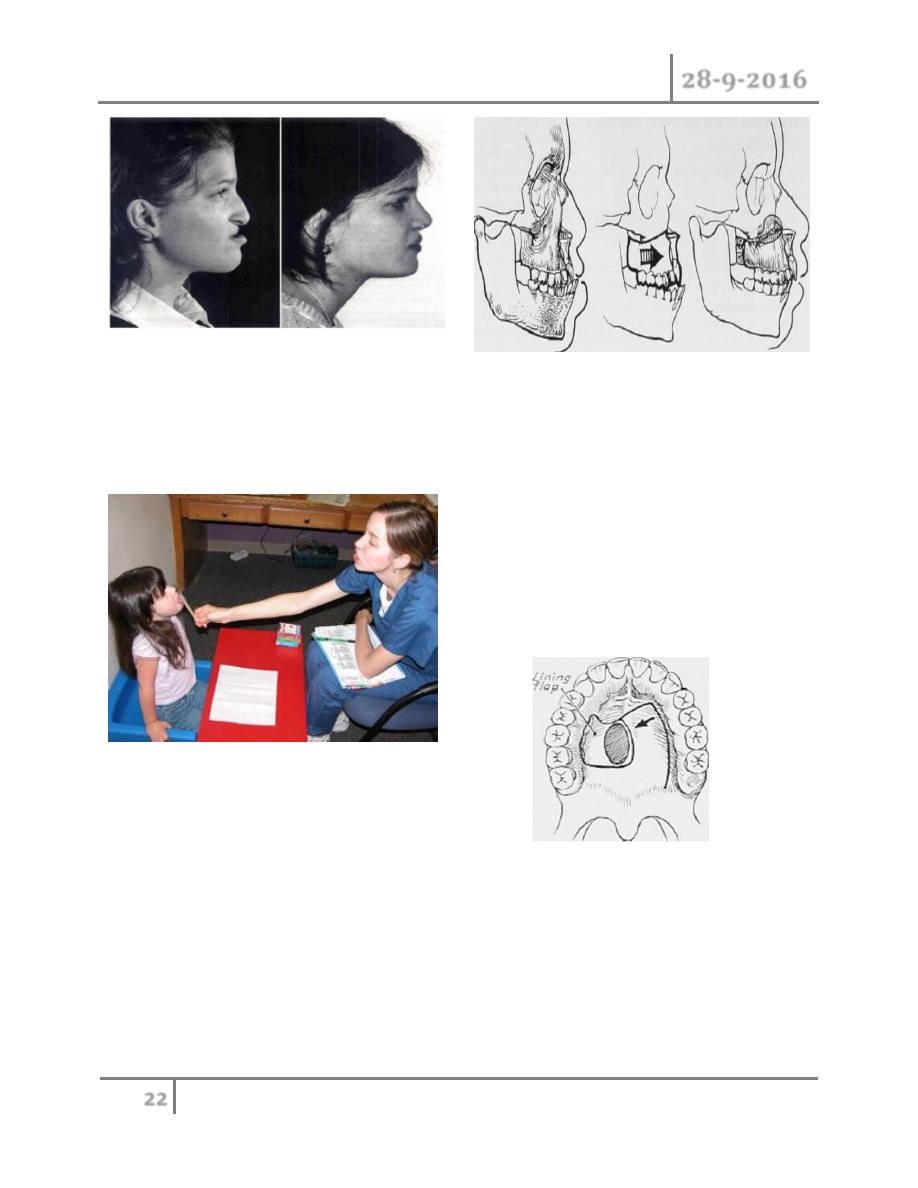
3- Midfacial growth problem.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
22
©Ali Kareem 2016-2017
Outcome :
1- Speech problem: velopharyngeal incompetence will need speech therapy.
2- Secondary palatal procedure:
o Treatment of palatal fistula.
o Treatment of velopharyngeal
incompetence.
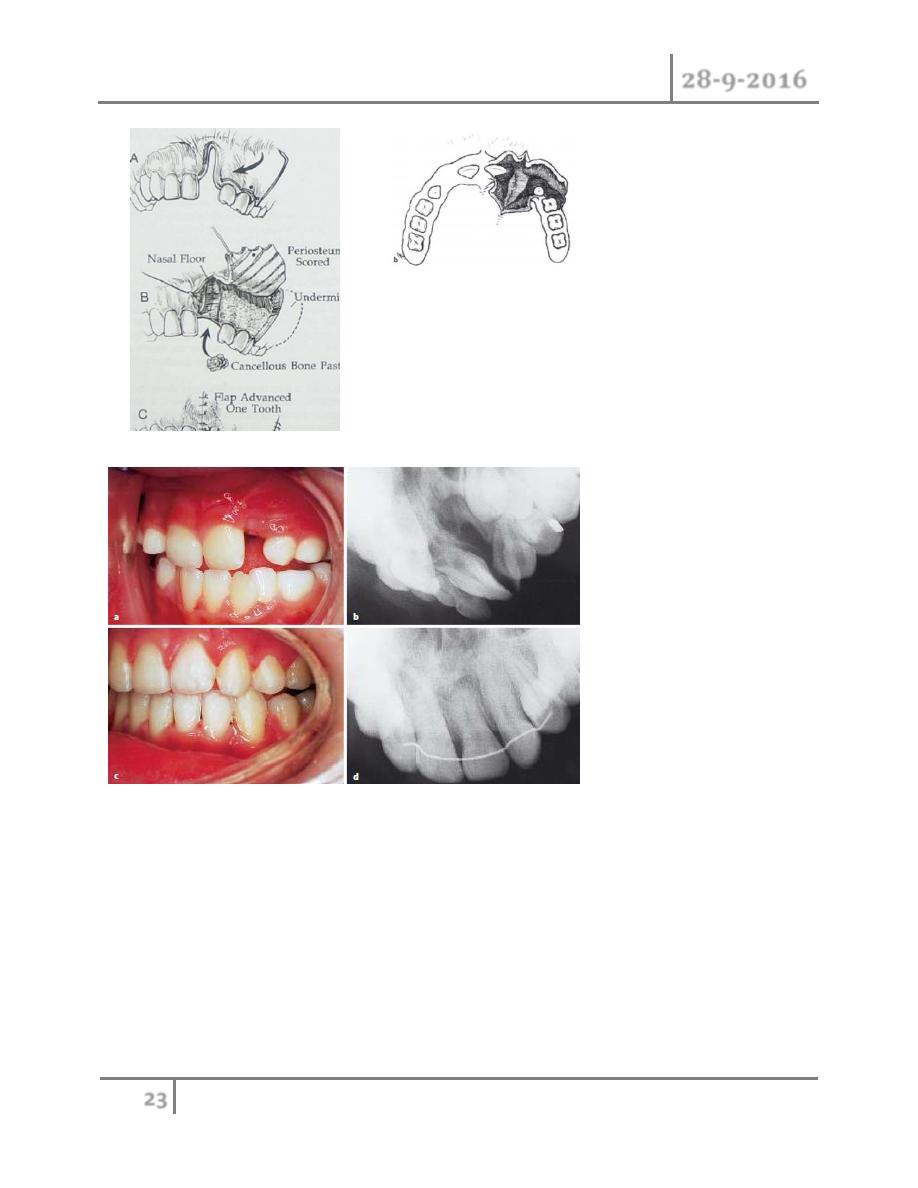
3- Alveolar reconstruction at 7-10 : years of age with initial orthodontic
alignment, then bone graft.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
23
©Ali Kareem 2016-2017
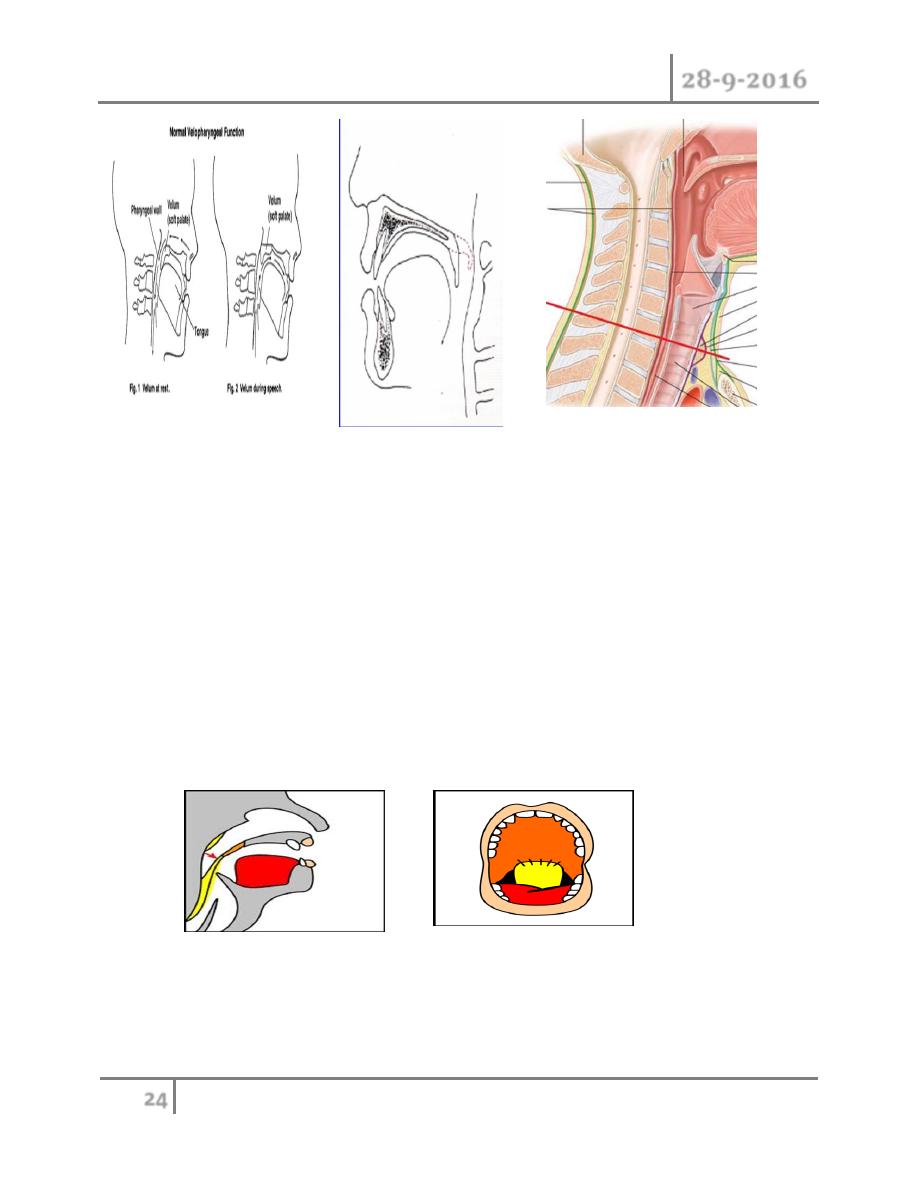
Velopharyngeal incompetence :
Incomplete closure of soft palate against the posterior pharyngeal wall during
speech , this lead to escape the air from oropharynx up through nasopharynx
which lead to hypernasal speech.
Cleft Lip and Palate Dr. Ahmed Khalaf
28-9-2016
24
©Ali Kareem 2016-2017
Management :
1- Preoperative increasing the pharyngeal muscles strength by asking the baby
to blow.
2- Using the procedure which elongate the soft palate e.g. V-Y advancement
and double opposite Z- plasty.
3- Using mymucosal flap from posterior pharyngeal wall that suture to
posterior soft plate.
4- Posterior pharyngeal wall augmentation using autologus tissues or
alloplastic materials to reduce the size of velopharyngeal orifice.
#END of this Lecture …