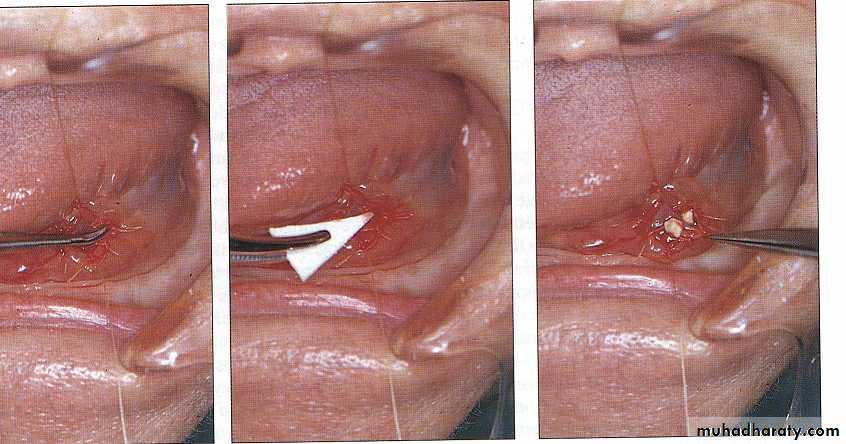
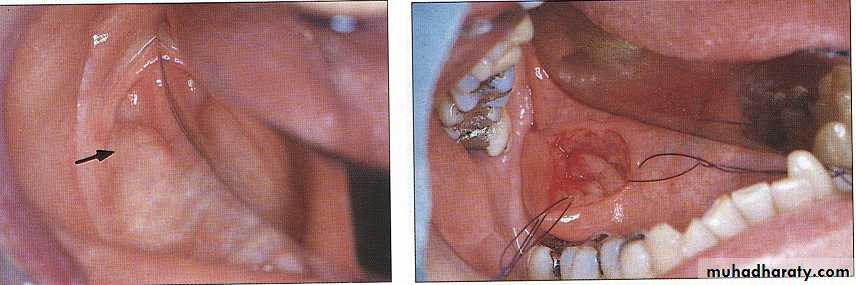
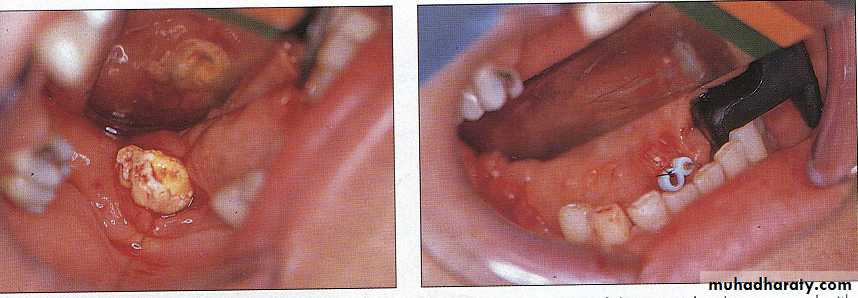
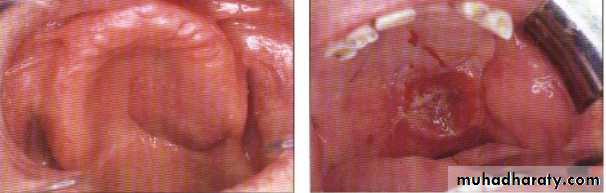
Duct obstruction
A- Due to causes in the lumenCauses is calculi . Submandibular s.g is most common site for calculus production.
Sign & symptom:-
1-sever &large swelling
2-pain during eating
3-diminshed saliva
Diagnosis of calculi:-
clinical: by manual palpation of the duct
Radiographical:
plain radiograph
sialogram
a. The secretion of the gland is thick and viscous as compared to watery secretion of the parotid.
b. The upward course of the submandibular duct does not provide adequate drainage.
c. The duct orifice lies in the floor of the mouth where foreign bodies may lodge into it and provide nucleus for stone formation.SALIVARY GLAND STONES(SIALOLITHIASIS)
The stones may be singly or multiple and may lie in the gland, duct or both.
They contain high proportion of calcium.
The gland often enlarged and inflamed as chronic irritation and obstruction by the stone.PATHOLOGY:
Treatment:• Depend on the location of calculi in the duct
• Vitamine- c – lozenges
• Milking of the gland
• Surgical removal of the stone from the duct
• Surgical removal of the gland
B- Obstruction due to causes in the wall
As a result of calculi in the duct which may ulcerated & lead to stricture or stenosis after healing.As a result of trauma to the duct wall.
As a result of chronic irritation and friction of the ductal wall with coronoid process of the mandible.
diagnosis:-
In sialogram see stricture or stenosis of the duct with dilatation of the duct behind the stricture.
Treatment:
• If the stricture in the ant. Part of duct use conservative method of dilatation.
• If the stricture in the post. Part of duct we do surgical operation by creating a new opening of duct behind the stricture.
C- Obstruction due to causes out side the wall:
1- Due to presence of a tumor either benign or malignant neoplasm.2- Sjogren syndrome:
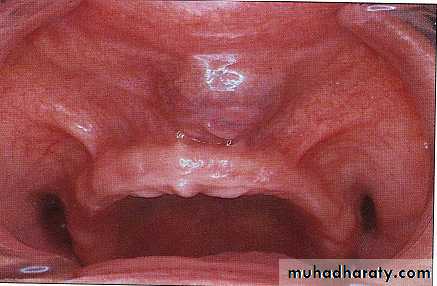
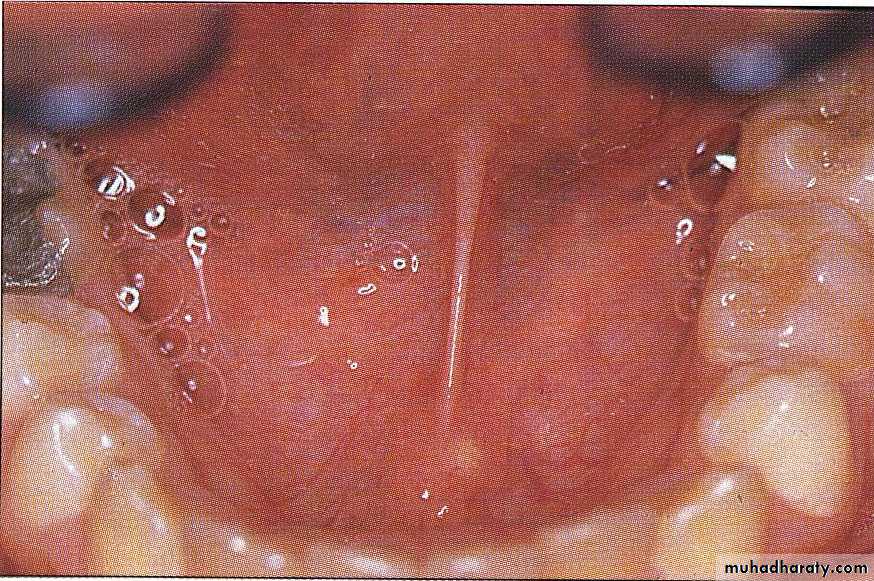
Its an autoimmune condition characterized clinically by:
A-Dry mouth
B-Dry eye
C- Difficulty in swallowing
D- Rheumatoid arthritis
Histologically:
There is destruction of acini & replaced by plasma cell infiltration & lymphocyte with epithelial hyperplasia.There are dilatation of the ductal tree.
Cast & or stones within the duct.
Radiographically:
There is snow strom apperance after injection of radio-opaque material.
Treatment:-
• 1. Use sips of water during eating & swallowing to compensate for saliva.• 2. Use cream on the lip.
• 3. Use artificial tear.
• 4. Give cortisone to stop the progress of condition into wars.
Gland distension:
Caused by:
a. Drug: ( thiouracil or thiocyanates, phenyl & phenyl butazone ).
b. Allergy:
May found in certain time of a year,
Or with Hay fever,
Or with asthma.
Histamine may reduce the swelling &discomfort.
Salivary Gland Tumors
80 % occur in parotid gland5-10 % occur in the submandibular gland
1 % occur in sublingual gland
10-15% occur in the minor salivary glands
Incidence of Malignancy According to Site
Sublingual 70%Submandibular 40%
Parotid 20 %
Clinical Classification
Benign (seldom recurrent)Adenolymphoma (Wharthins Tumor)
Oxyphil adenoma (Oncocytoma)
Other types of Monomorphic adenoma
Benign tumor less than 10% of salivary tumor. It occur in parotid glands only between the ages 40-60 years male strong predominance. They are sometimes bilateral.
Clinically: The tumor present as painless cystic swelling
Treatment: Surgical removal (superficial parotidectomy)ADENOLYMPHOMA (Warthin’s Tumor)
Clinical Classification
Benign (often recurrent)Pleomorphic adenoma (mixed tumor)
Mucoepidermoid tumor ( low-grade)
Acinic cell tumor (same)
The most common benign neoplasms of salivary glands. Most pleomorphic present in middle age but may occur at any age and equally in either sex.
It usually remains benign for many years but unless adequately removed it tend to recur and to turn malignant.
Clinically:
a) Slow growing painless lump mostly in parotid and some in submandibular and few in the minor glands.b) Mobile with well defined edge and smooth or lobulated surface.
Definitive diagnosis can only be made histologically after excision
Treatment surgical removal (superficial parotidectomy)
PLEOMORPHIC ADENOMAClinical Classification
MalignantCarcinoma in pleomorphic adenoma
Adenoid cyctic carcinoma
Adinic cell tumor
Mucoepidermoid tumor (high-grade)
Clinical Features:
Affects elderly people and common in parotid with equal sex distribution.The tumor forms rapidly growing hard swelling with ill defined edges and nodular surface.
Soon becomes fixed with pain-facial palsy, and lymph nodes enlargement but distant metastasis are rare.1. Operable Tumors:
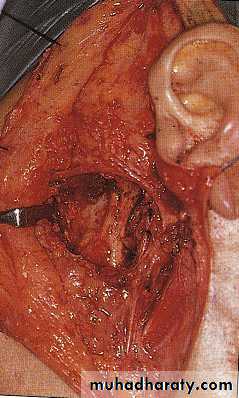
a) Radical parotidectomy combined with block dissection of the cervical lymph node.b) Post-operative radiotherapy
c) When the tumor arises in the other site of salivary tissues wide local excision is performed with block dissection of lymph node.
2. Non operative tumor with infiltration to the skull and pharynx. Radiotherapy can be given.
TREATMENT:
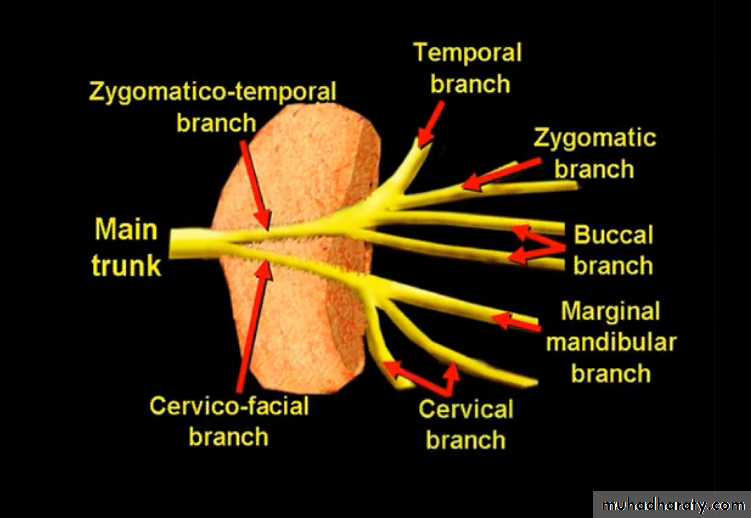
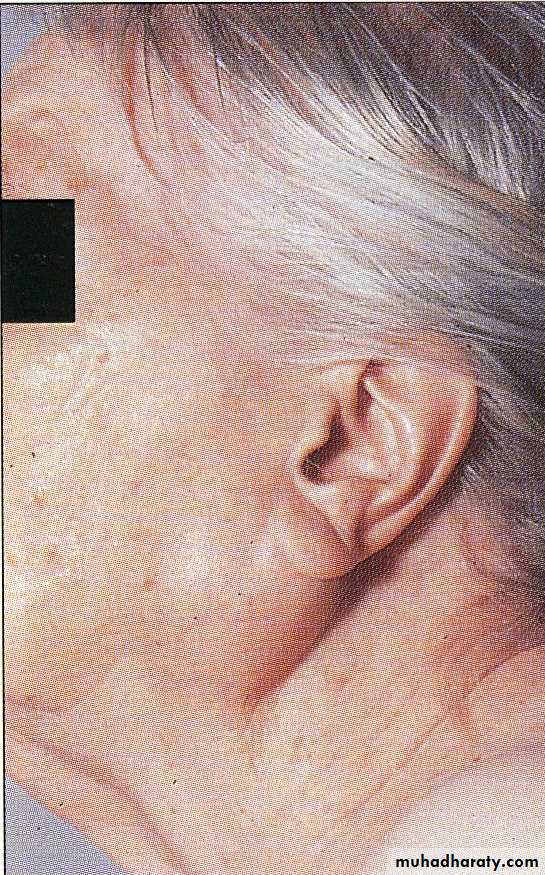
1) Damage to facial nerve causes facial palsy or damage to its branches
2) Salivary fistula3) Frey’s syndrome:
also known as gustatory sweating or auriculotemporal syndrome, it is characterized by facial flushing and sweating. It is thought to be the result of misdirected nerve regeneration in which the postganglionic parasympathetic fibers of the auriculotemporal nerve supplying the parotid gland regenerate and connect sympathetic nerves that innervate subcutaneous sweat glands. When salivation is stimulated, the nerves now stimulate sweat glands in the distribution area of the auriculotemporal nerve. It can be managed safely and effectively following parotidectomy with injections of botulinum toxin.
with severed distal.92
Complication of Parotidectomy: