Preprosthetic Surgery
Dr. Wafaa KhalilPreprosthetic surgery involves operations aiming to eliminate certain lesions or abnormalities of the hard and soft tissues of the jaws, so that the subsequent placement of prosthetic appliances is successful.
Definition
Hard Tissue Lesions or Abnormalities
The abnormalities associated with hard tissues are classified into two categories:• Those that may be smoothed with alveoloplasty immediately after extraction of the teeth, ( sharp spicules, bone edges ),
or those detected and recontoure in an edentulous alveolar ridge.
b. Congenital abnormalities, such as;
• Torus palatinus,
• Torus mandibularis,
• Multiple exostoses.
Alveoloplasty
Alveoloplasty is the surgical procedure performed to smooth or recontour the alveolar bone, aiming to facilitate the healing procedure as well as the successful placement of a future prosthetic restoration.
Protrusion of alveolar bone of the premaxilla after multiple extractions of anterior teeth

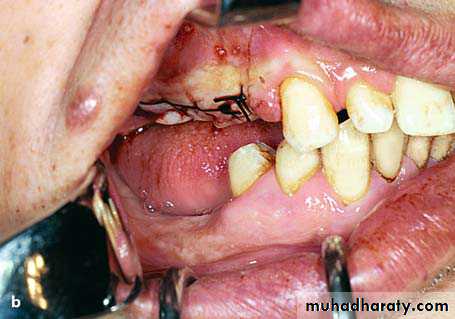
Supraeruption of maxillary teeth dragging down the alveolar ridge. Indication for alveoloplasty after extraction
Alveoloplasty After Extraction of Single Tooth.
When a tooth is hypererupted due to the absence of an antagonist, bone irregularity is usually observed after its extraction. This may cause problems for the normal healing process and abnormality of the alveolar bone, resulting in obstruction of the placement of a prosthetic restorative appliance. In such cases, immediatelyafter extraction of the tooth, recontouring of the bone in the area must be performed.
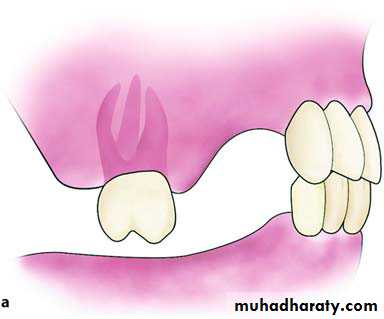

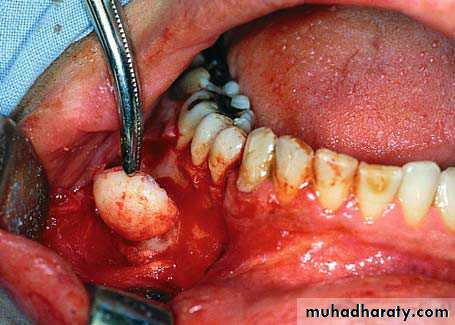
Supraeruption of a maxillary molar. After extraction of the tooth, surgical recontouring of alveolar bone is required. The procedure aims to create a normal interarch space.
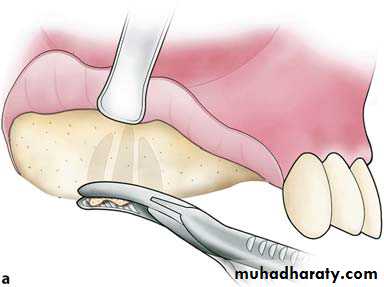
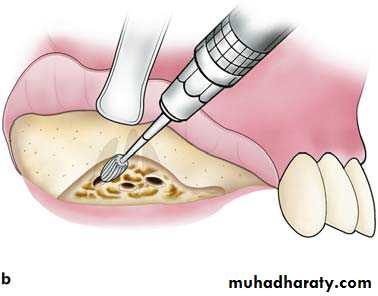
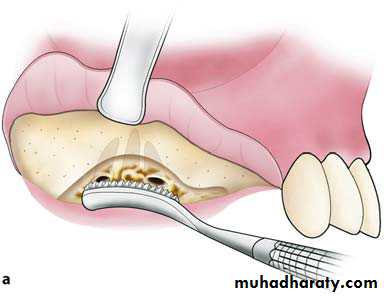
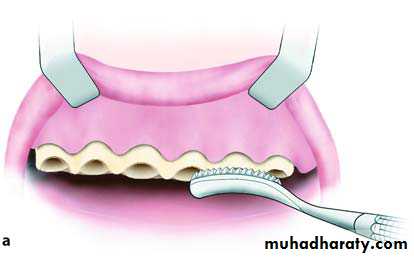
Smoothing of the alveolar ridge with a bone rongeur (a), and with a bone bur (b)
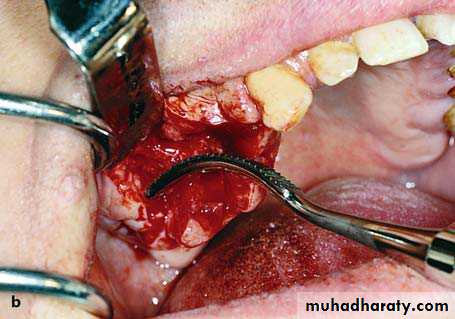
Smoothing of bone surface with a bone file. a Diagrammatic illustration. b Clinical photograph
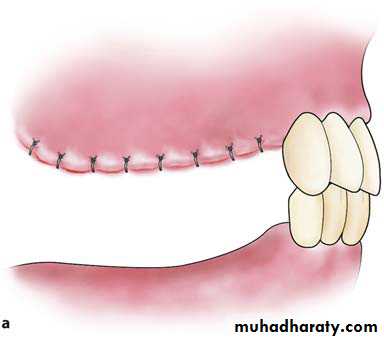
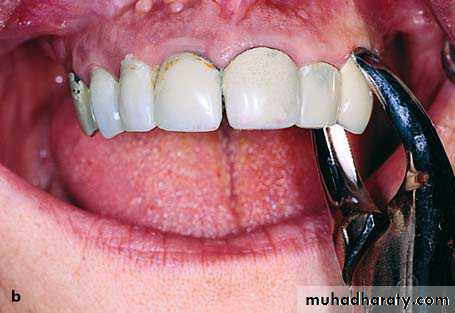
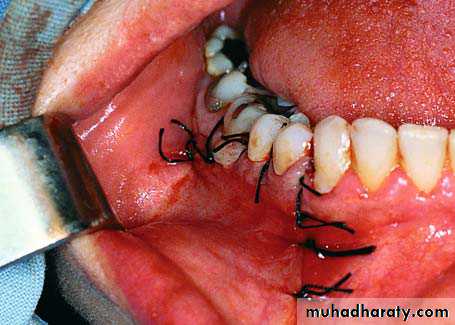
Operation site after suturing. A satisfactory interarch space is created to allow the placement of prosthetic restoration. a Diagrammatic illustration. b Clinical photograph
Alveoloplasty After Multiple Extractions
This procedure includes:a. Scheduled extractions.
b. Reflection of the gingivae.
c. Smoothing of alveolar bone.
d. Care of wound.
e. Suturing of the mucoperiosteum

a Radiograph of maxillary teeth, after whose removal smoothing of alveolar bone is required. b Clinical photograph of teeth to be extracted
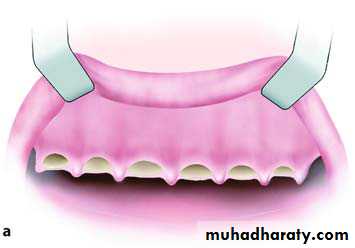
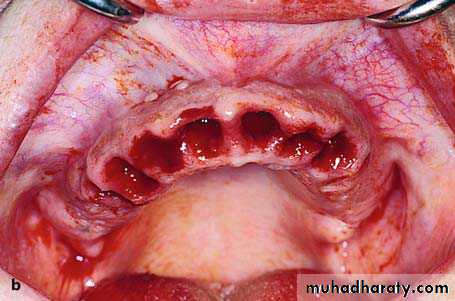
Diagrammatic illustration (a) and clinical photograph (b) of gross intraseptal irregularities after multiple tooth extractions
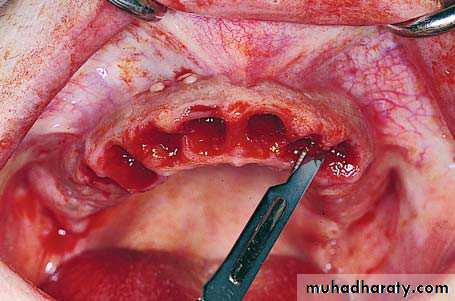
Incision along the alveolar ridge to cut the interdental papillae of the gingivae
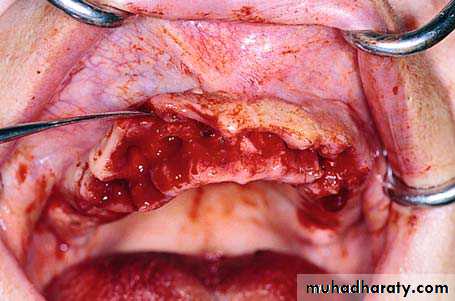
Reflection and elevation of the mucoperiosteal flap to expose the bone area to be recontoured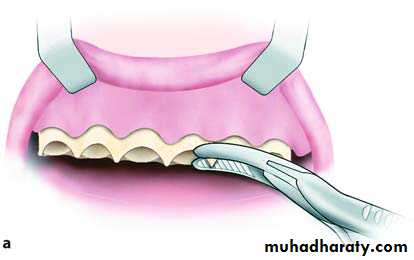
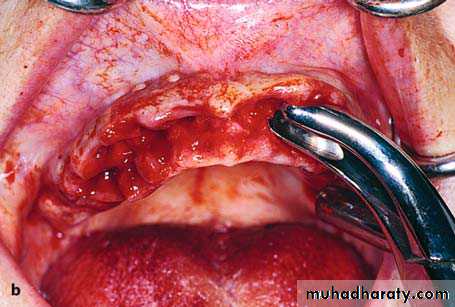
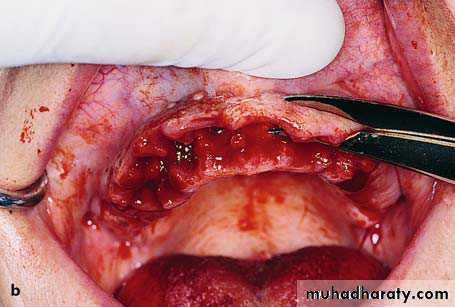
Removal of sharp bone edges with a rongeur. a Diagrammatic illustration. b Clinical photograph
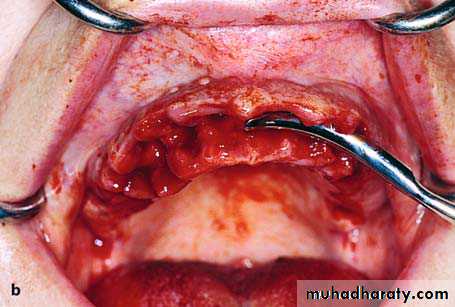
Smoothing of bone with a bone file. a Diagrammatic illustration. b Clinical photograph
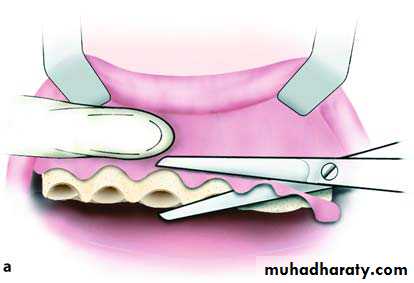
Removal of excess soft tissues with soft tissue scissors.

Operation site after suturing
Recontouring of Edentulous Alveolar RidgeSometimes, after tooth extractions and the wound has been healed for a long time, the residual ridge may present irregularities at a certain point or even along the entire alveolar ridge.
In such cases, the bone must be smoothed, to avoid injury and avoid obstructing the proper support of complete dentures.

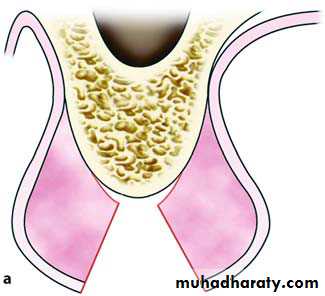
Bone irregularities of an edentulous alveolar
ridge of the mandible after multiple tooth extractionsIncision along the alveolar ridge where the bone irregularity is located
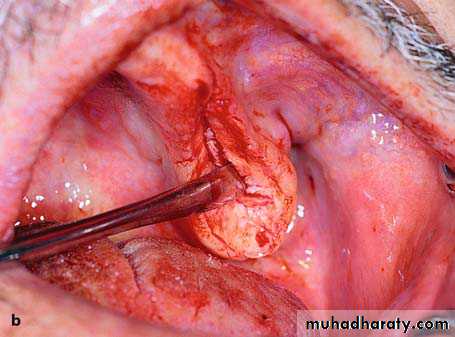
Reflection of the mucoperiosteum flap and smoothing of the alveolar ridge with a bone file, then removal of excess soft tissue.
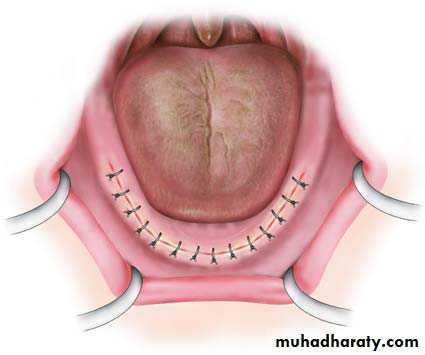
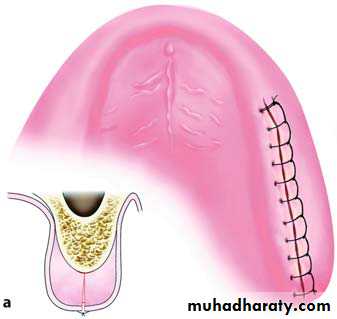
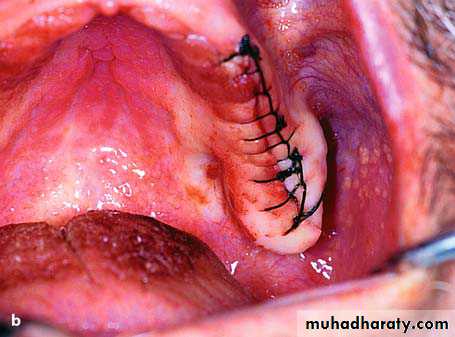
Continuous suture along the alveolar ridge
This procedure, despite its extent, is not particularly difficult, because large or smaller vessels and nerve branches of the area have a known course and emergence, so that it is easy to avoid injury or trauma.Exostoses
Exostoses are generally bony protuberances, which develop in various areas of the jaw. They are not considered real neoplasms, but dysplastic exophytic lesions.The etiology of these lesions remains unknown, even though evidence suggests that genetic and environmental factors determine their development.
Exostoses are classified into three types:
(1) torus palatinus.
(2) torus mandibularis.
(3)Multiple exostoses.
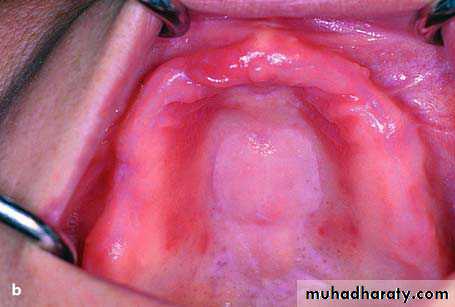
torus palatinus

torus mandibularis
• large nodular and lobulated tori interfering with seating of dentures;• torus with traumatized mucosal surface;
• torus extending beyond the palatal region;
• torus with deep undercuts and multiple nodules;
• torus that complicates speaking;
• psychological problems
Indications for removing the palatal tori are:
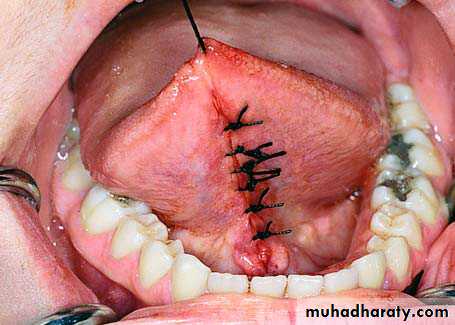
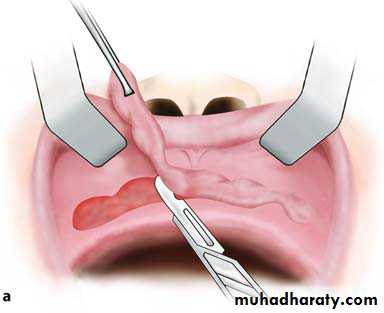
Surgical procedure for removal of torus palatinus
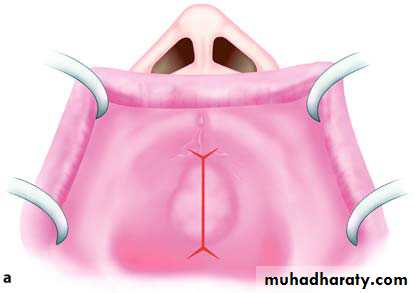
Incision along the midline of the palate with anterolateral and posterolateral incisions.
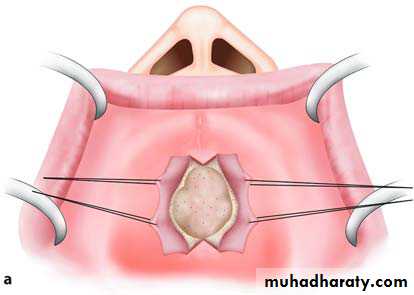
Mucoperiosteal flaps on either side of the exostosis. Retraction of flaps during the surgical procedure is achieved with the help of traction sutures.
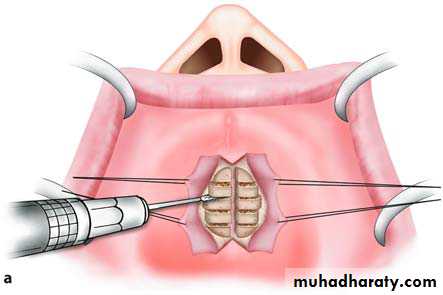
Sectioning of the lesion into smaller parts using a fissure bur
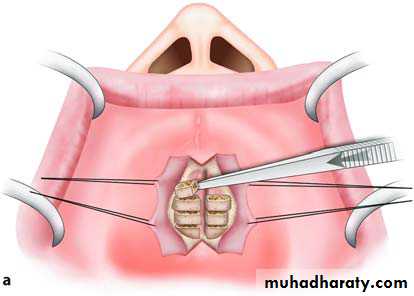
Removal of the exostosis in fragments with a monobevel chisel
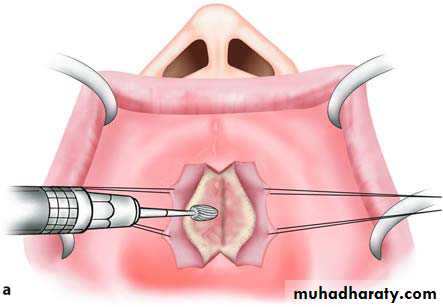
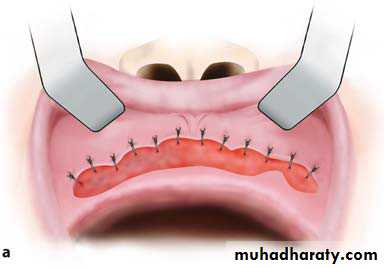
Smoothing of the bone surface with a bone bur.
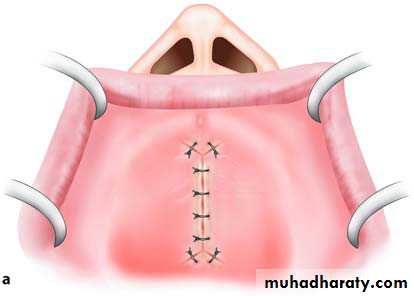
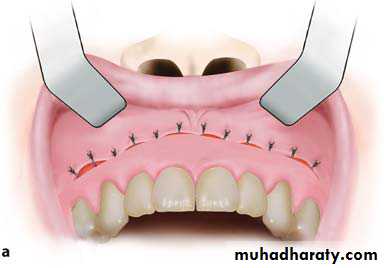
Operation site after the placement of sutures
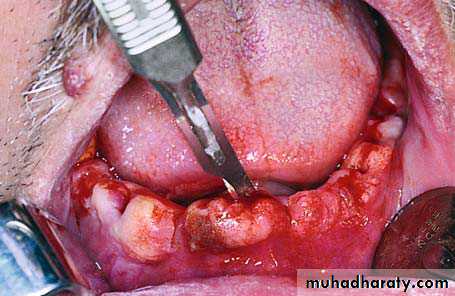
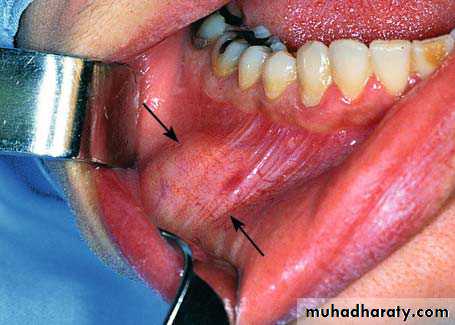
Torus MandibularisTorus mandibularis is an exostosis of unknown etiology.
It is localized in the lingual aspect of the body of the mandible, either on one side or more commonly on both sides (canine & premolar region).
Clinically, it is an asymptomatic bony protuberance covered by normal mucosa. Radiographically, it presents as a circumscribed radiopacity in the area of localization.
Torus mandibularis is completely innocent in nature and does not require any therapy whatsoever, except in cases where complete dentures are to be constructed.
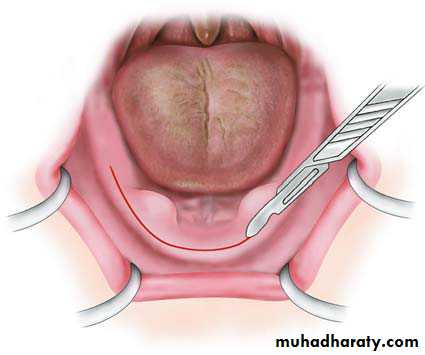
Incision along the alveolar ridge (without vertical releasing incisions)
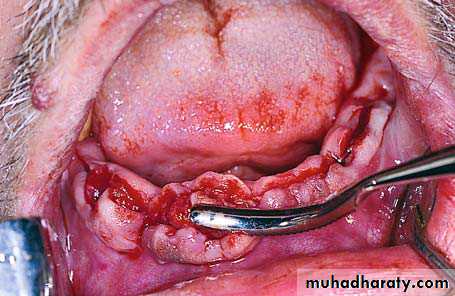
Mucoperiosteal flap reflected to expose the
exostoses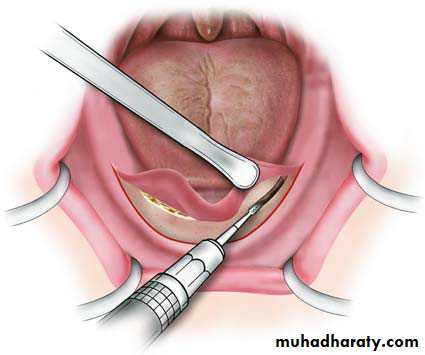
Removal of exostoses with a bone bur
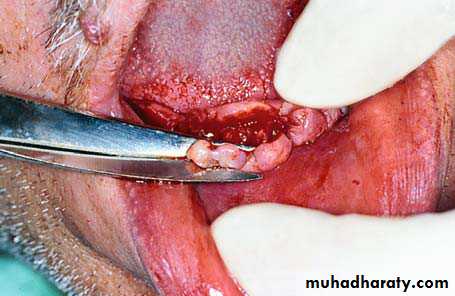
Smoothing of the bone surface with a bone file
Surgical field after the recontouring of bone
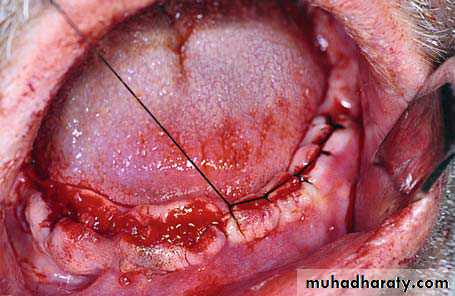
Operation site after suturing
Multiple Exostoses
These are rare asymptomatic bony excrescences, usually localized at the buccal surface of the maxilla and mandible. The causes are unknown, although some people suggest that they may be due to bruxism as well as chronic irritation of the periodontal tissues. No therapy is usually required, except for those cases where, due to the large size of the exostoses, severe esthetic and functional problems are created.

Extremely large multiple exostoses in the maxilla with a multilobular and irregular shape
Localized Mandibular Buccal ExostosisThis case presents rarely, and, depending on its size, creates esthetic and functional problems in edentulous as well as dentulous patients. Its presence especially in edentulous patients obstructs the placement of complete dentures, in which case its removal is deemed necessary.

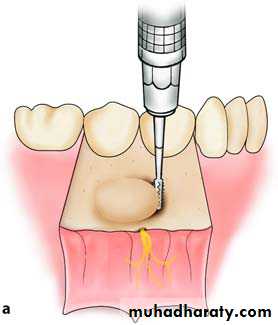
Mental nerve
Small trough created at the base of the exostosis with a fissure bur

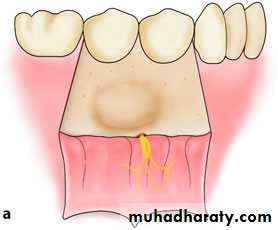
Removal of bone along the line of cleavage completed. Removal is performed using a chisel
Removal of the excised portion of the exostosis with a hemostat
Reduction of genial tuberclesThe genioglossal muscle attaches to the genial tubercle located at the lingual aspect of mandible. As the mandible resorbs, the genial tubercle becomes prominent and the mouth floor ascends simultaneously with the resorption process.
During fabrication of dentures, the activity of the genioglossal muscle and protuberance of the genial tubercle complicates wear of dentures by causing dislocation during function.
when the genial tubercle and genioglossal muscle interfere with retention and stability of a prosthesis; Lowering of mouth floor procedures is considered
Surgical technique
• A crestal incision is performed along the anterior ridge
• Subperiosteal dissection is continued under the lingual mucoperiosteum until the genial tubercles and muscles become evident.
• Sharp dissection of the genioglossal muscles is performed.
• The genial tubercle is resected with a fissure or round bur.
• Strict hemostasis should be obtained prior to closure of the lingual flap otherwise life-threatening airway restriction may occur due to hematoma formation in the floor of the mouth.
Reduction of mylohyoid ridge
In extensive resorption of the mandible, the mylohyoid ridges become prominent that cause denture displacement with strain of the mylohyoid muscles. Pain is felt because of mucosal impaction of dentures at the sharp mylohyoid ridges. Surgical resection of sharp ridges is indicated.
Surgical technique
• A crestal incision is made along the posterior mandibular ridge.
• Subperiosteal dissection is carried out to expose the mylohyoid ridge and muscle.
• Mylohyoid muscle is grasped with a curved clamp and the muscle is separated by electrocautery.
• The mylohyoid ridge is smoothened or resected with a bur.
• Then flap is sutured.
Soft Tissue Lesions or Abnormalities
classified into two categories:a. Congenital abnormalities, such as a hypertrophic frenum, etc.
b. Abnormalities created after the use of dentures(e.g., fibrous hyperplasia of the mucosa), and other causes.
Frenectomy
In many cases, the placement of a complete denture of the maxilla, or orthodontic procedures in younger persons requires the removal of the labial frenum, especially if it is hypertrophic. Also, in the mandible, the lingual frenum may create problems, causing partial or complete ankyloglossia. This case is due to attachment of the frenum to the floor of the mouth or to the alveolar mucosa. It may even be the result of an extremely short frenum that is connected to the tip of the tongue. Ankyloglossia greatly limits movements of the tongue, resulting in speech difficulties.

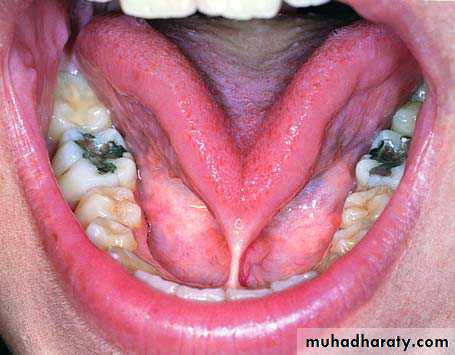
Ankyloglossia as a result of a short frenum
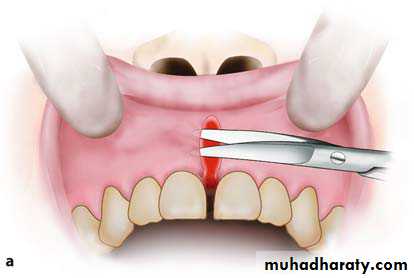
Hypertrophic maxillary labial frenumFrenectomy
Various techniques have been described for removal of active and strong frenum attachments. These are ; V–Y advancement flap, Z-plasty, and diamond shaped excision.
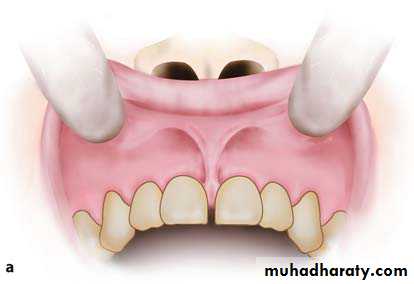
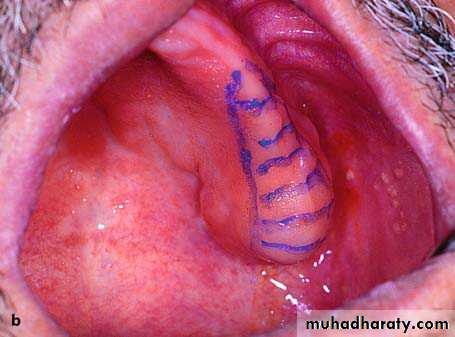
Characteristic case of a maxillary labial frenum with a low gingival attachment.
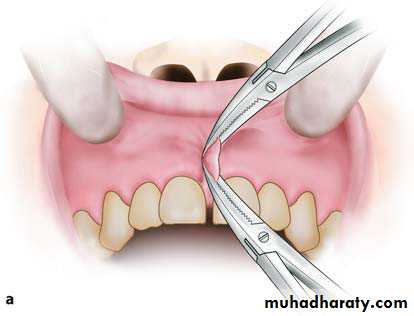
The superior and inferior margins of the frenum are grasped using curved mosquito hemostats
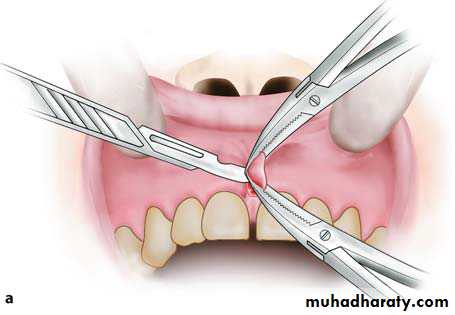
Initial step in excision of the frenum with a scalpel in contact with the posterior surface of the lower hemostat.
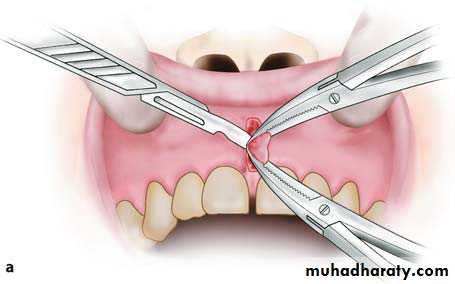
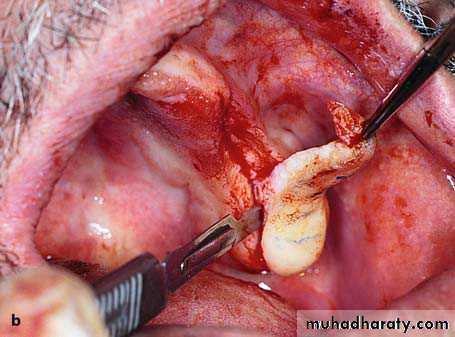
Final step in excision of the frenum. Incision behind the upper hemostat is performed
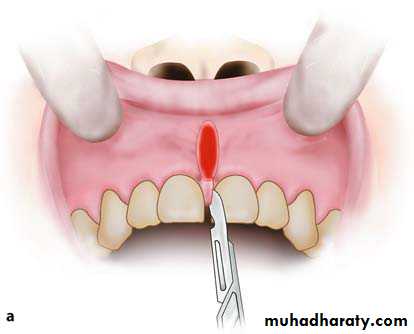
Removal of hypertrophic tissue found between and behind the central incisors
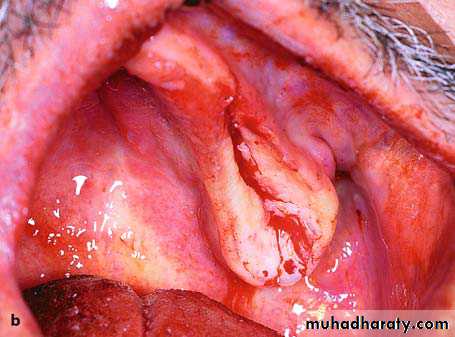
Undermining of mucosa of wound margins from underlying tissues
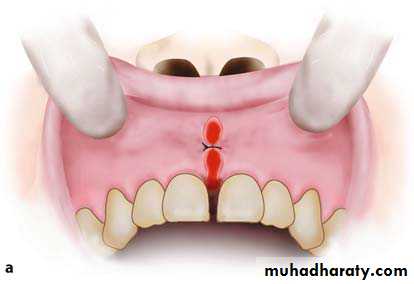
The first suture is placed at the middle of the wound to facilitate subsequent suturing
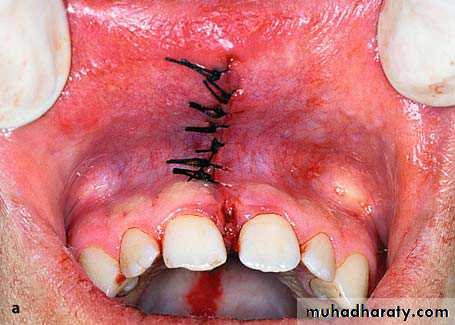

aOperation site after placement of sutures. b Postoperative clinical photograph 3 months later
The Z-plasty technique may produce less scar than the diamond-shaped excision. Z-plasty is usually indicated for a frenum with a wide crestal part and shorter alveolar height because it increases alveolar height.
An incision is made directly along the length of a frenum. Superior and inferior incisions are placed to form triangles. After supraperiosteal undermining, the apex of the inferior triangle is rotated upwards and conversely the apex of the superior triangle is rotated downwards.
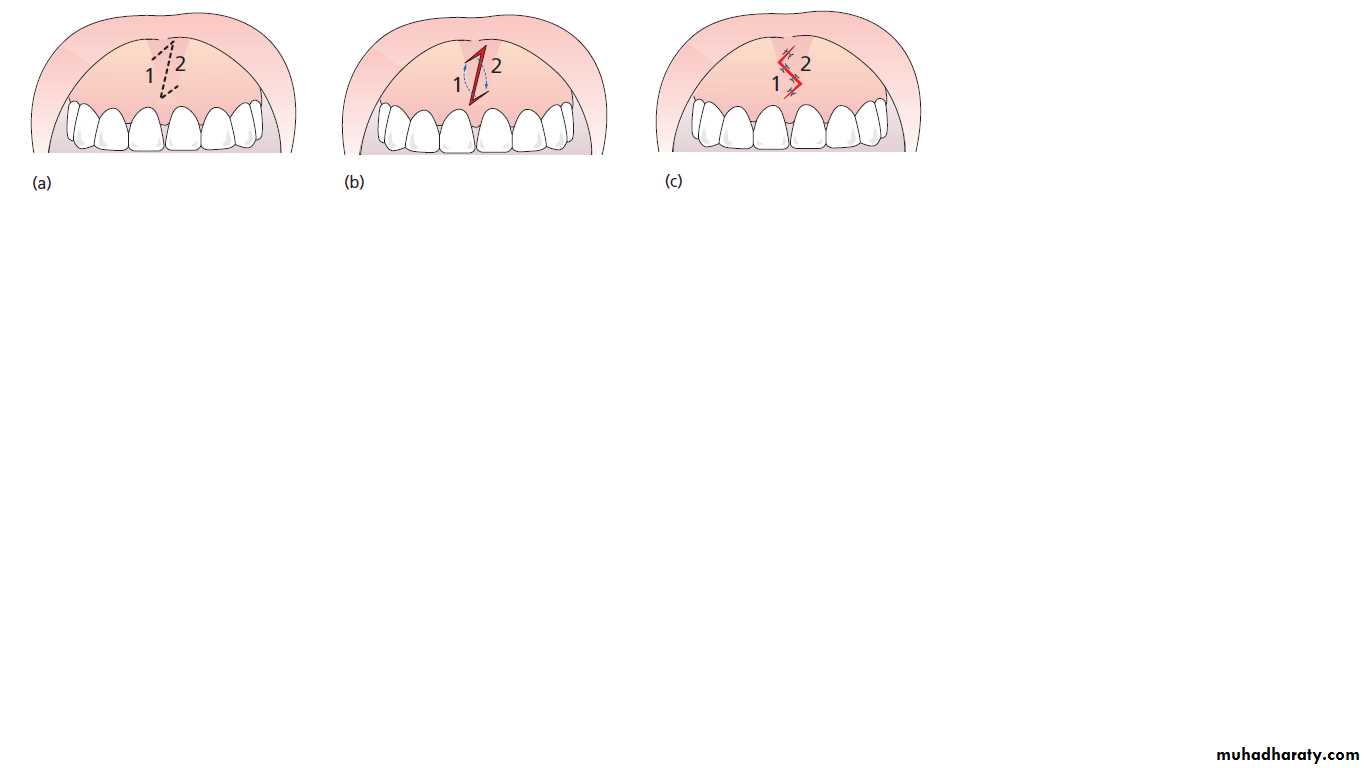
The Z-plasty frenectomy technique. (a) Outlining of the Z flaps. (b) Creating the small triangular flaps. (c) Rotation of the flaps and final closure.
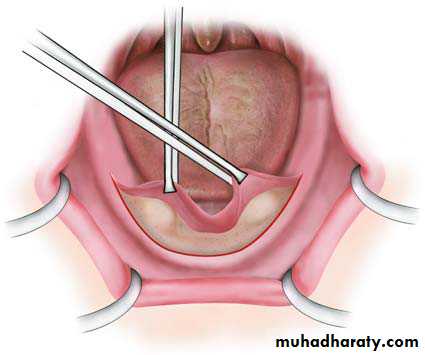
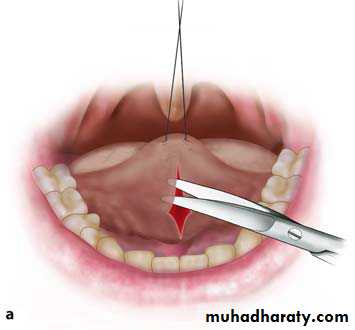
Lingual Frenectomy (tongue tie, ankyloglossia treatment)
Removal of the lingual frenum is also a simple procedure, which may be performed with or without the help of a hemostat.
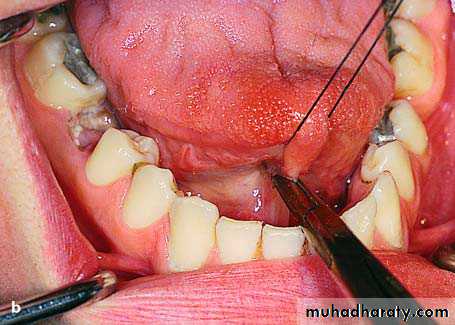
Elevation of the tongue with the aid of a suture and retraction of the frenum with a straight hemostat, to facilitate removal
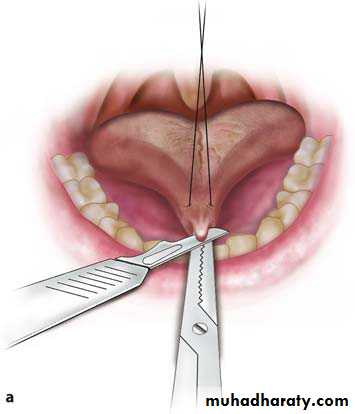
First step in frenectomy. The scalpel is always in close contact with the upper surface of the hemostat.
Steps in Frenectomy with Hemostat
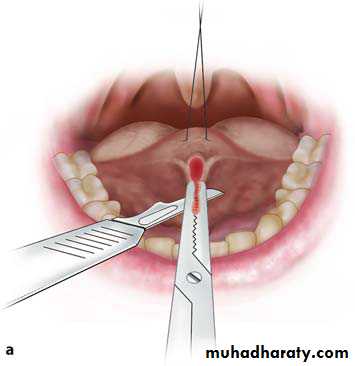
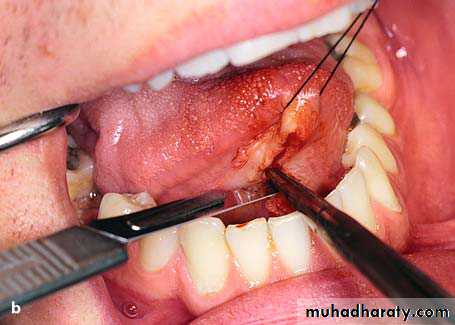
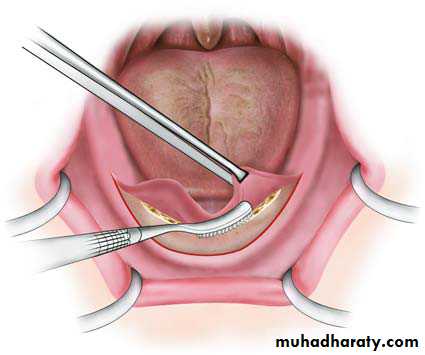
Second step in frenectomy, involving the portion beneath the hemostat
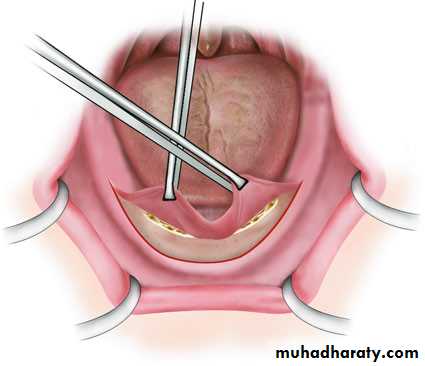
Undermining the mucosa at wound margins from underlying tissues
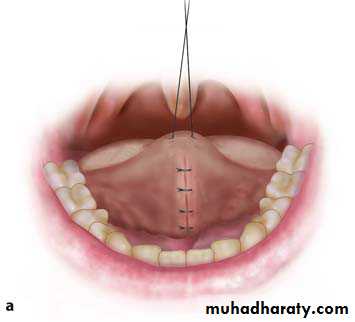
Operation site after suturing
Steps in Frenectomy without Hemostat

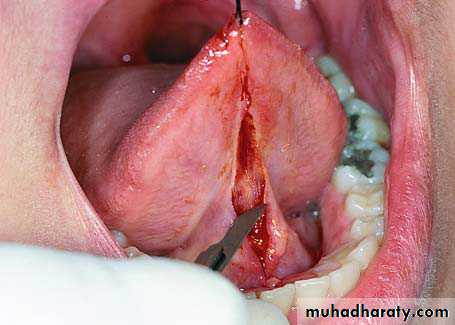
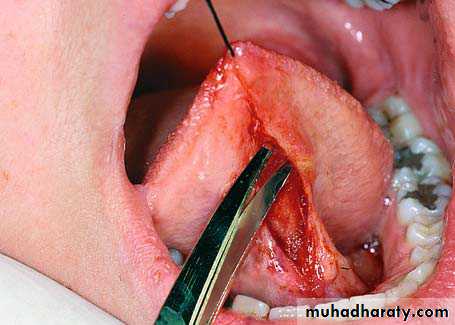
• Elevation of the tongue with a suture placed at the tip of the tongue.
• Excision of the frenum with converging incisions towards the base of the tongue.• Undermining the wound margins with scissors.
• Suturing of the operation site.
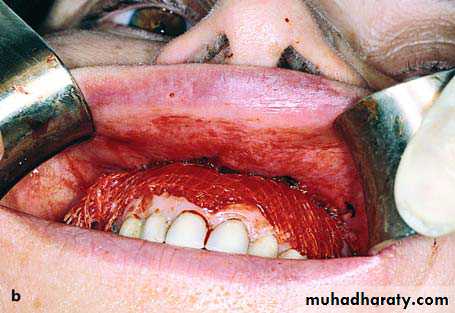
Denture-Induced Fibrous Hyperplasia
Fibrous hyperplasia of the mucosa (formerly known as epulis fissuratum or inflammatory hyperplasia) is usually due to chronic trauma of the mucosa of the mucolabial or mucobuccal fold, due to ill-fitting complete or partial dentures. More specifically, the denture flanges injure this area, because they are very thin and longer than normal. Treatment is surgical and consists of excision of the hyperplasiaSurgical Technique

Removal of the lesion in segments with a scalpel
The lesion is grasped with surgical forceps and is gradually excised along the length of the lesion superficial to the underlying periosteum.
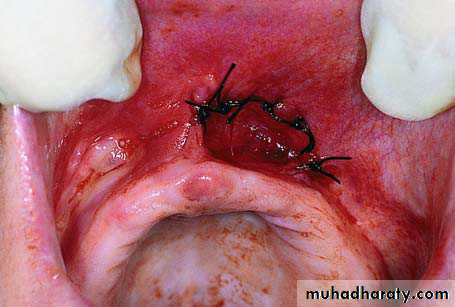
Suturing of the wound margins with periosteum that has not been reflected, which remains exposed, avoiding a decrease in the depth of the mucobuccal fold.
Replacement of old denture, immediately after the end of the operation, retaining the depth of mucosa of the newly created sulcus. The internal surface of the denture is lined with tissue conditioner
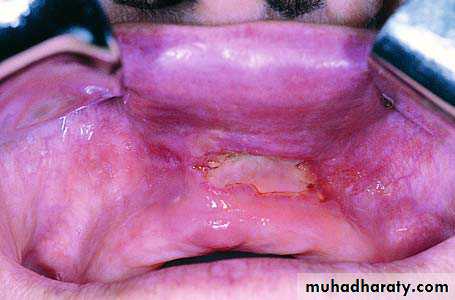
Removal of Localized Denture-Induced Hyperplasia

Localized fibrous hyperplasia of mucosa as a
result of ill-fitting denture
Injection of local anesthetic peripherally
around the lesion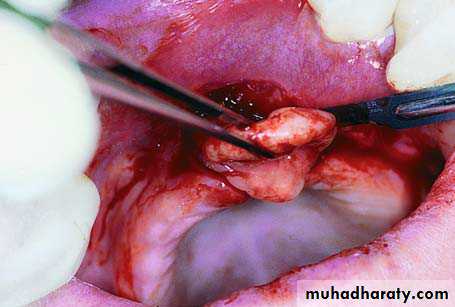
Gradual excision of hyperplasia with scalpel
and scissors
Suturing of superior lip of incision with periosteum that has not been reflected, to avoid a decrease of the depth of the mucolabial fold
Postoperative clinical photograph immediately
after removal of sutures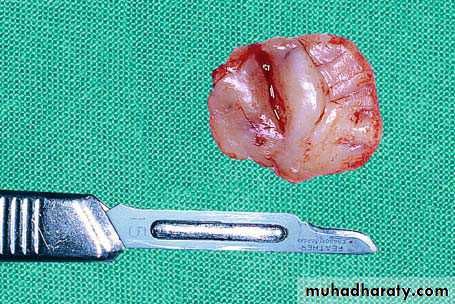
Surgical specimen (hyperplasia) after excision
Fibrous Hyperplastic Retromolar TuberosityFibrous hyperplasia of the soft tissues of the alveolar process is reactive in nature, usually observed in the retromolar edentulous area of the maxilla and is the result of constant irritation during mastication. Clinically, bilateral asymptomatic symmetric lesions with a smooth surface are noted, which are elastic and firm during palpation. Size varies and sometimes the lesion may grow to be so big that it occupies all of the interarch space during occlusion, creating serious problems for construction of a partial or complete denture. Treatment is surgical recontouring the alveolar process to decrease the size of the fibrous connective tissue lesion.
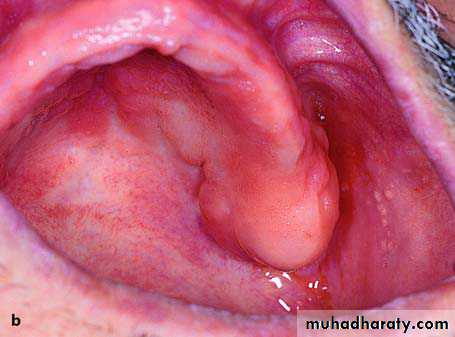
Fibrous hyperplastic retromolar tuberosity of left maxilla
Surgical Technique
Continuation of the incision
toward the palatal side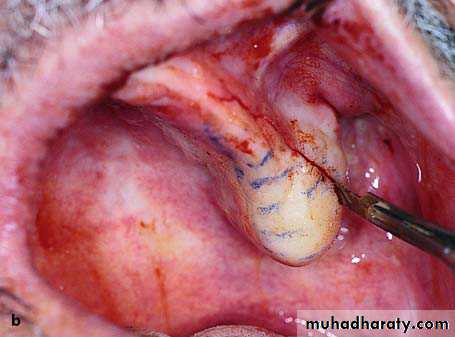
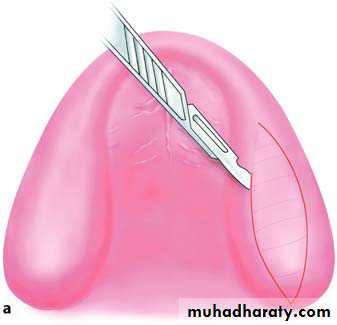
buccal incision
demarcated segment of hyperplastic
tissue to be removed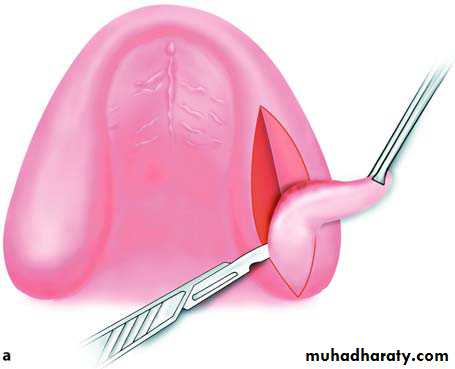
Gradual excision of the lesion with a wedge-shaped incision reaching as far as the bone
Surgical field after removal of hyperplastic tissue
Reflection of tissues with periosteum, so that wound margins can be reapproximated and sutured
Operation site after placement of sutures
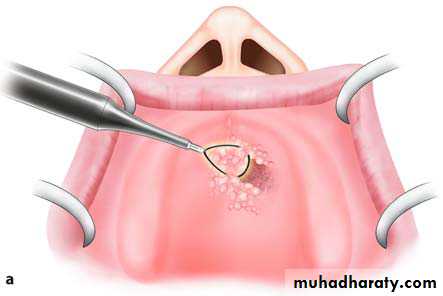
Papillary Hyperplasia of the PalatePapillary hyperplasia is a rare pathologic condition localized most often in the palate. It usually occurs in edentulous patients who have been wearing dentures for a long time and is possibly due to inflammatory hyperplasia of the mucosa because of chronic local irritation. It also occurs in dentate patient, etiological factors include mechanical and thermal irritation from foods, smoking, etc.
Clinically, these are multifocal hyperplastic nodules of the mucosa of the palate, between which food may accumulate, potentiating the inflammatory reaction.
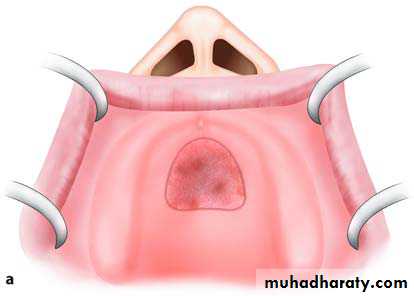
Treatment is surgical and consists of removal of the lesion with a scalpel or electrosurgical loop.
The traumatized area is covered with a surgical dressing and healing is achieved by secondary intention