1
Fifth stage
Pediatric surgery
Lec-1
د.عبدالرحمن
23/10/2016
Pediatric surgery
deals with surgical problems in children under the age of 14 years.
:
Pediatric Surgery
below 28 days of age .It deals
in neonate
deals with surgical problems
:
Neonatal Surgery
mainly with congenital malformations.
Fetal Surgery
: deals with some abnormalities in the intrauterine life ,like urinary
obstruction or Hydrocephalus or Sacrococcygeal taratoma .Such abnormalities if its left
without intervention it may lead to further deterioration in the general condition of the
fetus. For example :
1-Hydrocephalus in Utero :if left without drainage it may lead to increase in size of head
and atrophy of the brain tissue .Putting catheter will prevent cortical atrophy & reduce the
size of the head making vaginal delivery possible.
2-Bladder Neck Obstruction :will lead to Hydroureter & Hydronephrosis with impaired
renal function . Putting a catheter in the bladder or making a cystostomy in the intrauterine
life may prevent renal function deterioration.
3- Sacrococcygeal taratoma :It may cause poor fetal development or what is called
stealing phenomenon of fetal blood .
What is the main presenting symptoms that bring the parents to the pediatric surgeon?
1-Gross congenital abnormalities.
2-Vomiting.
3-Dyspnoea .
4-Urinary retention.
5-Jaundice
6-Constipation (failure of passing meconium).
7-Abdominal distention.

2
Congenital Abnormalities: Some congenital abnormalities are obvious at birth ,e.g:
Meningocele, Sacrococcygeal taratoma,Cleft lip&palate,…..
Other anomalies may reveal themselves within 24 hours such as Esophageal atresia
or Diaphragmatic hernia . Other anomalies present after 24 hours like Intestinal
atresia (when the baby starts to have oral feeding),or Urinary retention or anuria.
Some anomalies may reveal itself several weeks after birth e.g:Biliary atresia ,Pyloric
stenosis.
Other anomalies may show themselves months or years later like :Congenital
Hydronephrosis or Congenital polycystic kidney …
Vomiting in neonates
Vomiting is one of the most common symptoms in neonate. Vomiting may be non
significant: causes could be over or little feeding, or
significant if it is persistent, projectile, bile or blood stained, or if it is associated with weight
loss.
Bile stained vomiting should be considered . due to intestinal obstruction until prove
other wise
Causes of vomiting:
Non-surgical conditions:
A. Neonatal infections like septicemia ,meningitis :the vomiting is associated with pallor
,convulsions or twitching ,hypothermia ,cyanosis ….
B. Adrenogenital syndrome :abnormal genitalia, salt losing metabolic disturbances.
C. Gastroenteritis ,gastritis ,urinary tract infection may occur in the late neonatal period
&infancy .
D. Milk allergy (very rare)
E. Feeding mismanagement.
surgical conditions:
A. Neonatal intestinal obstruction .
B. Sphenicteric disorders at either ends of the stomach
Congenital hypertrophic pyloric stenosis Gastro-esophageal reflux
C. Cerebral birth injury(head injury)increased ICP(rare).
D. Necrotising Enterocolitis.

3
Neonatal intestinal obstruction
The pathological types of obstruction is as follow:
1. In the lumen
2. In the wall of the bowel
3. Extrinsic
4. Neurogenic
The effects of intestinal obstruction:
1-Secondary pathological changes
Hypertrophy of muscle coat
Marked dilatation of the bowel above the obstruction
Collapsed distal segment (microcolon).
2-Additional effects:
Fluid & electrolytes loss :extrinsic (vomiting)
intrinsic(to the bowel & peritoneal cavity)
Disturbances of acid base balance :acidosis or alkalosis
Respiratory distress (abdominal distention).
Local changes at the site of obstruction:
-Ischemia,
-Perforation if perforation occur in utero it leads to meconium peritonitis .
Clinical features:
There is a triad of clinical findings:
1-Vomiting ,abdominal distention, abnormal or retained meconium.
2-Rectal examination
3-General examination (fontanel, skin ,body temperature).
4
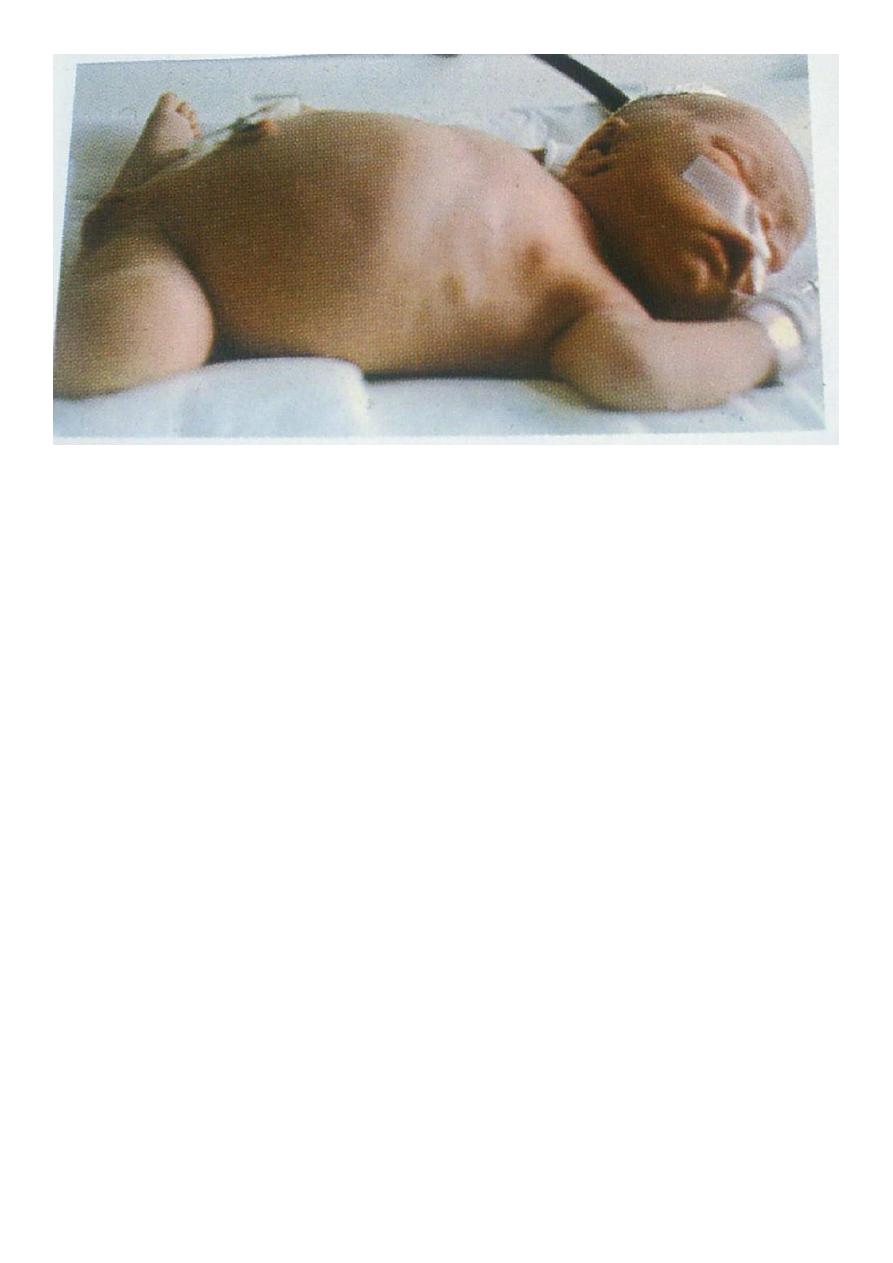
Investigations:
It has 2 objectives
1-To confirm the diagnosis
2-To determine the extent and severity of the physiological disturbances to do proper
preoperative resuscitation. So we have :
-Diagnostic investigations (plain X-ray ,contrast enema)
-Assessment investigations (Hb, pcv, platelet count,S-electrolytes, acid -base balance ,ph,
Pco2, bicarbonates. Cultures of Blood ,nasopharyngs, umbilicus&sites of sepsis .
5
Causes of neonatal intestinal obstruction:
1-Duodenal obstruction :
-Intramural: Duodenal mambrane
-Mural: stenosis or atresia
-Exramural:anular pancreas ,band of Ladd
2- Small bowel obstruction :
-Intramural :meconium ileus
-Mural:atresia,stenosis
-Exramural :volvulus neonatorum
3-Large bowel (colonic)obstruction:
-Intramural: meconium plug syndrome
-Mural : stenosis or atresia,Hirschsprung`s disease
-Exramural pelvic mass obstructing the rectum (teratoma).
4-Neurogenic & functional
-
Hirschsprung`s disease, ileus, sepsis.
6
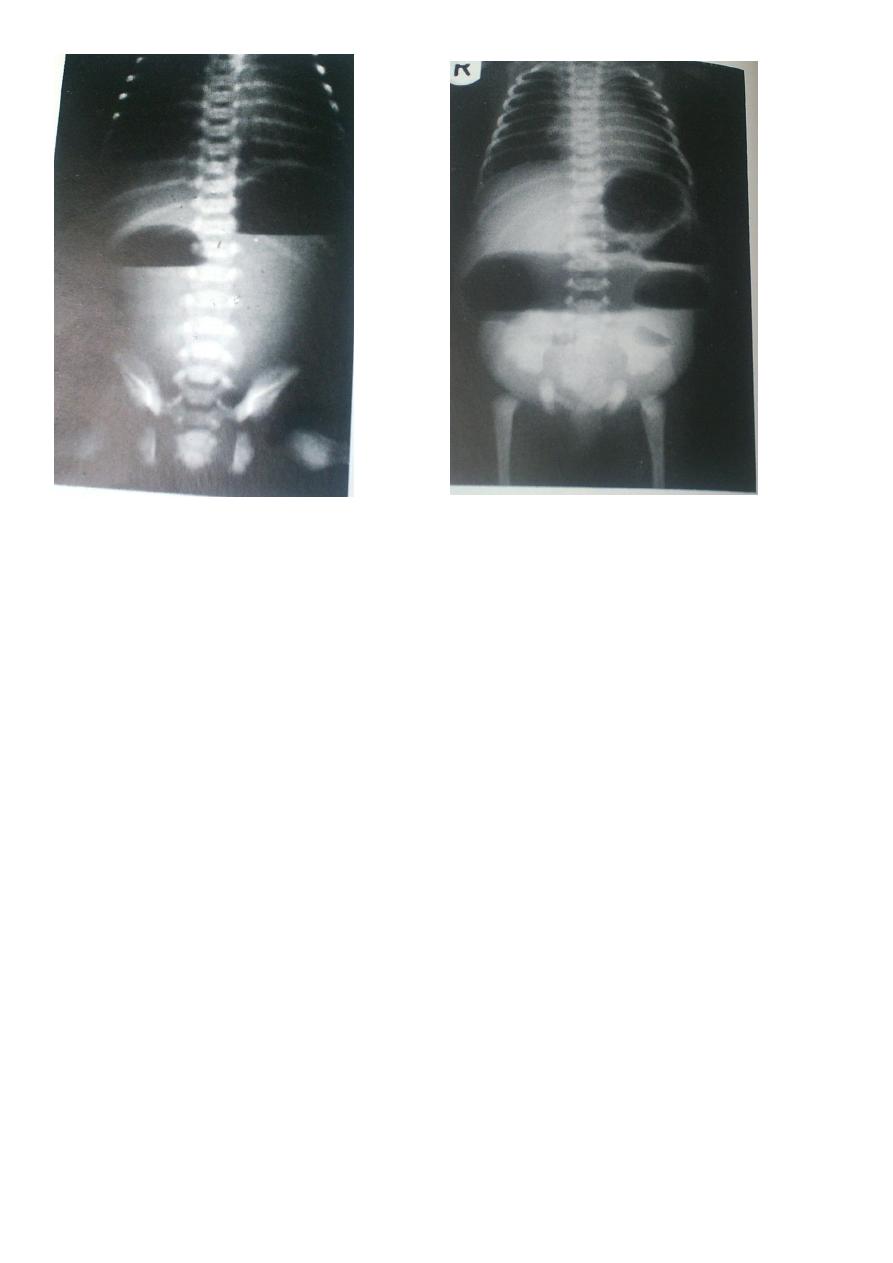
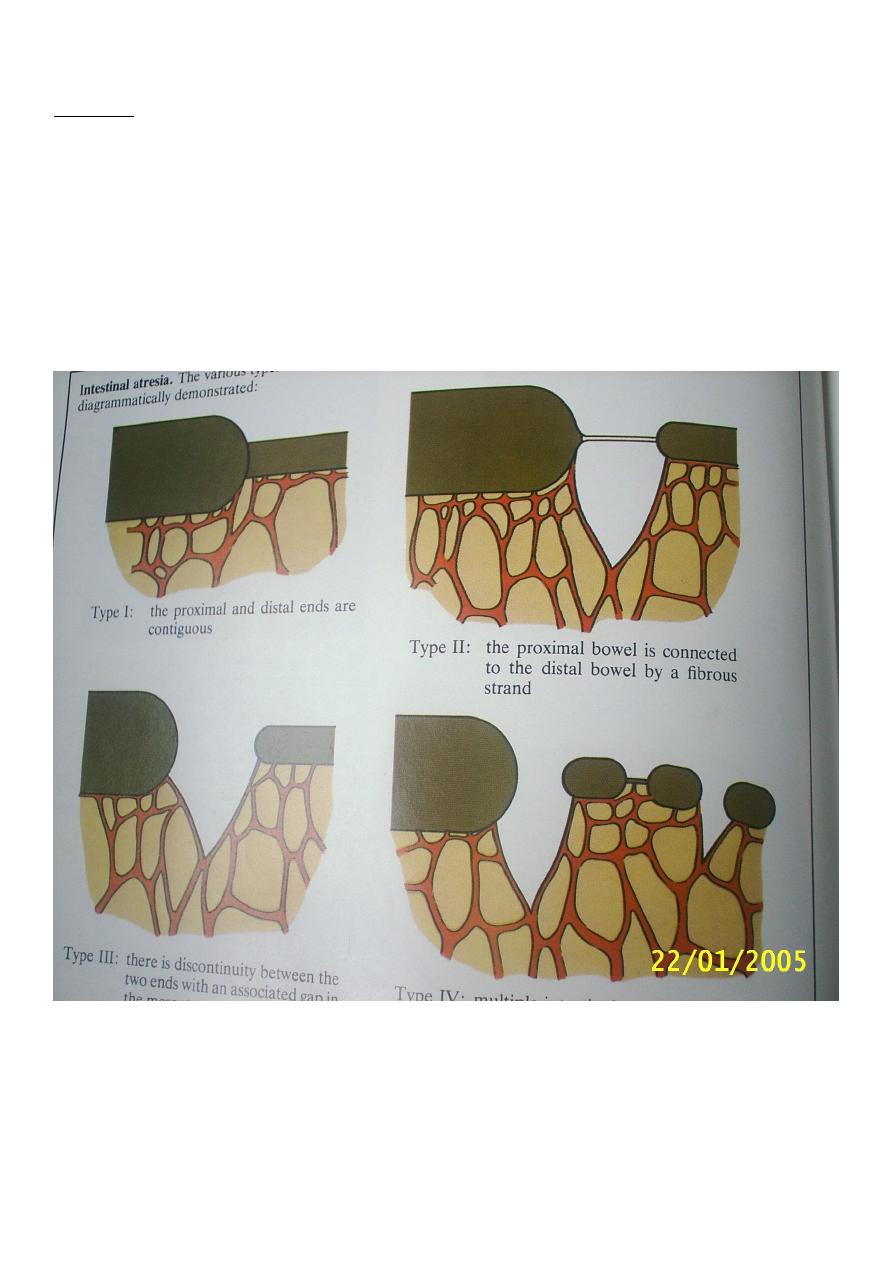
1-Atresia: Duodenum, Small intestine, Colon, Rectum, Anal atresia .
Type I: Membranous (thich membrane)
Type II: Missing segment of the bowel .
Type III: Missing segment of the bowel & mesentery.
Type IV: Multiple segment atresia.
The bowel proximal to the atresia is hugely distended and it's muscular coat is
hypertrophied ,it's tip is ballooned.
The Bowel distal to the atresia including the colon and rectum is unused ,collapsed
,(i.e microcolon).
7
Treatment:
Excision of reasonable length of the proximal bowel including the ballooned segment to:
1.
Have proper anastomasis (less dispropotion).
2.
To remove the tip which has poor blood supply .
3.
To have area with good peristalsis .
In cases of membranous duodenal obstruction -Duodenotomy with excision of part
of the membrane is done .
In cases of Anular pancreas Duodeno-duodenostomy is done.
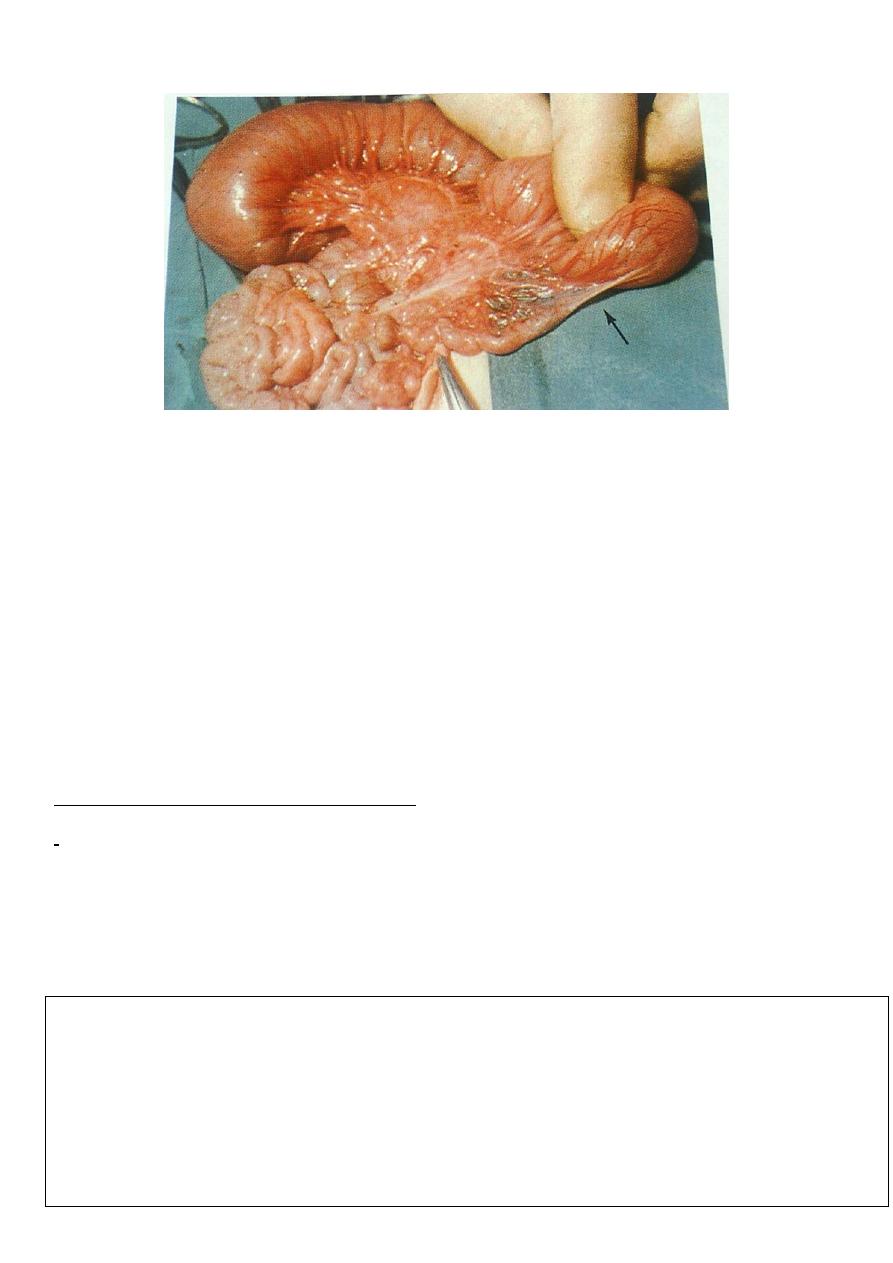
2-Malrotation and Volvulus Neonatorum:
The return of fetal alimentary canal from the extra embryonic coelom into the abdomen
occurs during the 10
th
week of intrauterine life ,then the bowel undergoes rotation and
fixation at certain points by attachments of it's mesentery to the posterior abdominal wall .
When there is arrest or incomplete rotation or less commonly deviation from normal
rotation ,It's called malrotation or malfixation .
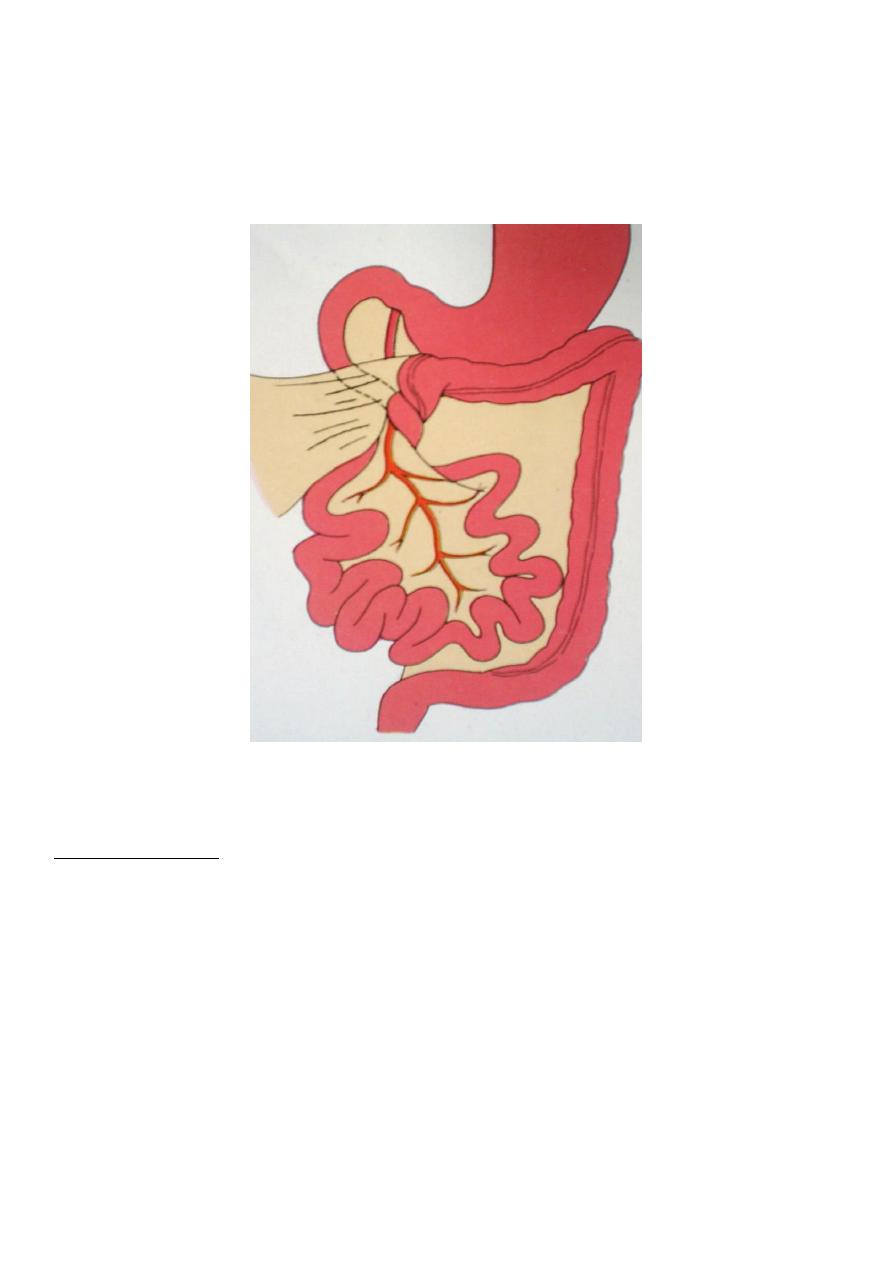
The Commonest abnormality when the small intestine (midgut) from the
duodenojejunal junction to the caecum has a very narrow mesenteric attachment to the
posterior abdominal wall based arround the superior mesenteric vessel .The caecum and
appendix is situated at the right hypochondrium and abnormally fixed by avascular band or
sheet of peritoneum running laterally across the second part of duodenum.
8
These abnormalities lead to 2 different types of presentatio
1- volvulus of midgut >>>strangulation .
2- Duodenal obstruction >>>by bands of Ladd .
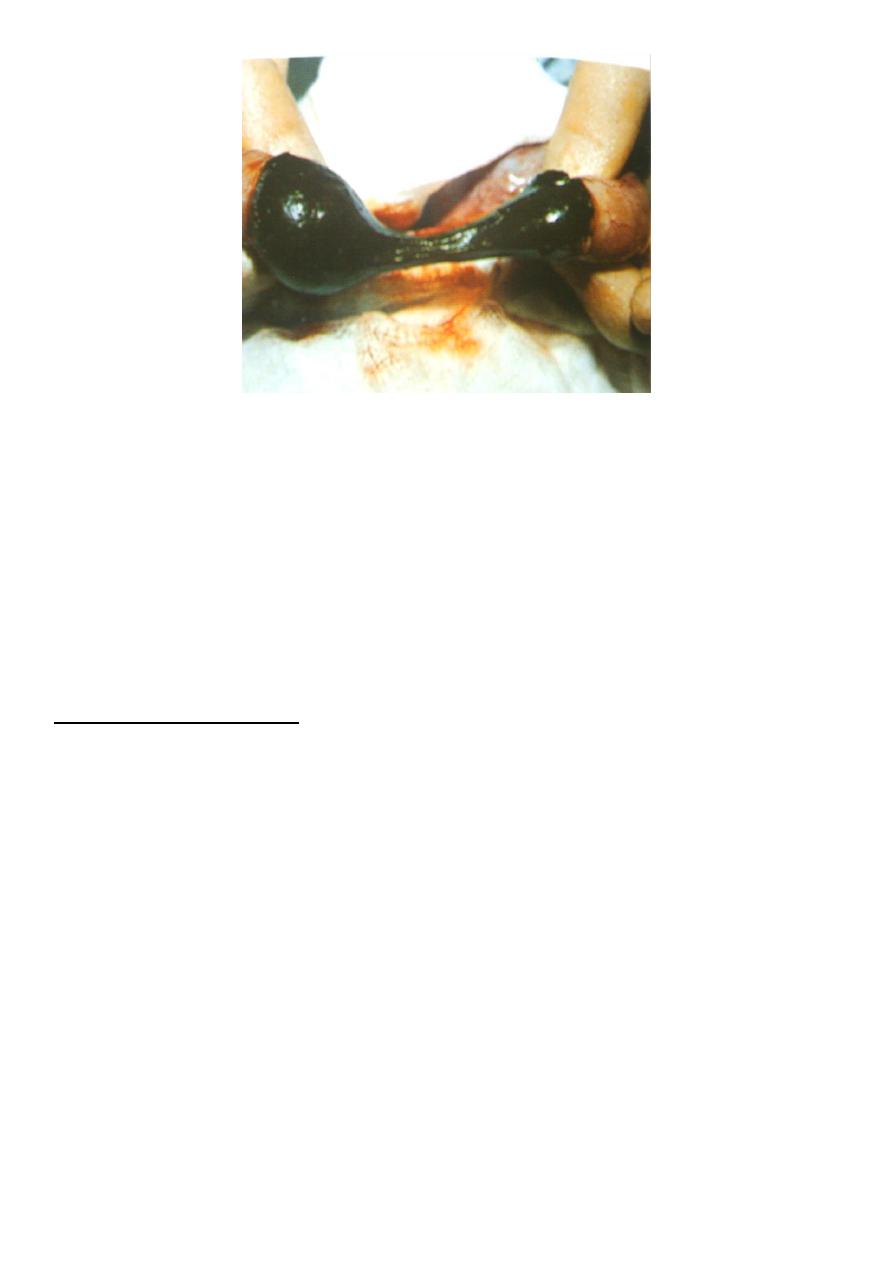
3-Meconium Ileus :
Meconium Ileus is the intestinal obstructive variant of cystic fibrosis (CF) or mucoviscoidosis
About 10-20 % of infants with CF present with intestinal obstruction related to meconium
ileus . Cystic fibrosis affects all the exocrine and mucus secreting glands in the baby (not
only the pancreas). It's a complex disorder of the respiratory and digestive systems.
Pathology: dilated segment of ileum containing impacted black-green meconium .Proximal
to this segment there are several loops of hypertrophied bowel distended with fluid .Distal
to the obstruction there is a few separated gray white globular pellets in the distal ileum .
Clinically: abdominal distension ,vomiting , &failure of passing meconium .
Investigation: Plain X-ray :multiple air fluid level .
Contrast study : Barium enema (microcolon)
9
Treatment: Rehydration, Broad spectrum antibiotics(including staphylococcus) .
Gastrographin enema under fluoroscopy .
Surgery:-
1. Enterostomy & removal of meconium.
2. Resection with end to end anastomosis .
3. Bishob Koop anastomosis.
4-Meconium Plug Syndrome
Present with the same triad :
-
Abdominal distension .
-
Vomiting
-
Delayed passage of meconium.
This is due to inspissated plug of mucous at the distal end the meconium column in
the rectum
P-R is normal unlike Hirschsprung's disease in which the anal canal is tight. P-R is
therapeutic and can relieve the obstruction and the plug is passed with large amount
of meconium and gases .
Plain X-ray is normal in the early stage ,fluid levels at the late stage .
Contrast study is normal and can relieve the obstruction
Rectal biopsy: is needed when we are in doubt to distinguish between Hirschsprung's
disease& meconium Plug Syndrome
A.L.Y