1
5th stage
Pediatric surgery
Lec-2
د.عبدالرحمن
22/10/2015
Anorectal Anomalies
A perinium without an anal opening is traditionally described as imperforated anus .This is
inappropriate terminology because most of anorectal malformations communicate by
afistulous track with either the urinary or genital system or actually open to the skin of the
perineum .
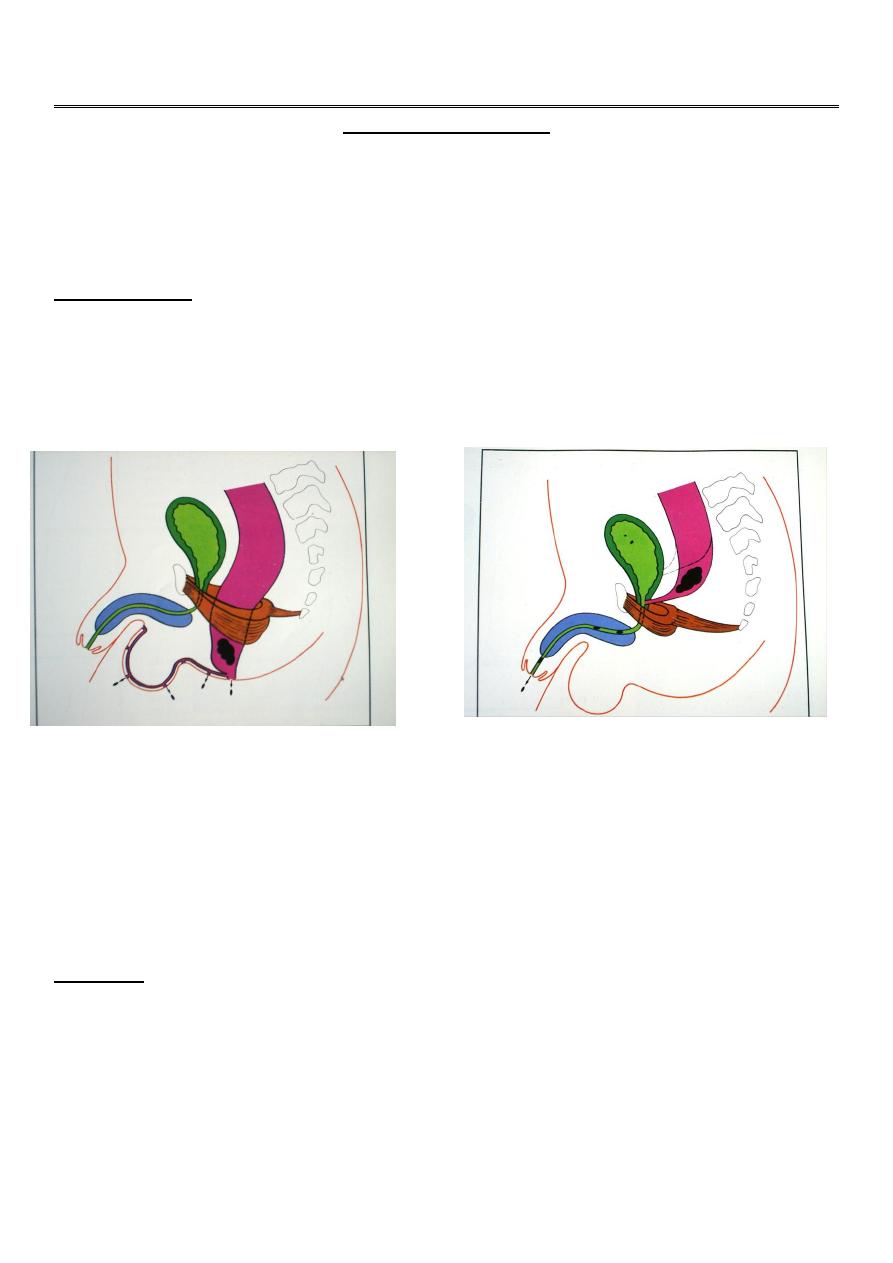
Classification:
Development of the distal bowel is arrested at one of two levels ,each with it’s subtypes.
The principle of distinction is in the relation of the end of the bowel to the chief muscle of
continence the puborectalis component of levator ani.
Arrested development at or above this sling (supralevator lesion) produces rectal deformities .
Arrested development below the sling (translevator lesion) produce anal deformities .
In each group the bowel may end blindly or communicate by a fistula with neighboring
viscus or the perineal skin.
Generally :Anorectal anomalies classified into 2 types :
1.
Low type
(Anal deformities),this is subdivided into :
-Stenosed anus
-Covered anus
-Ectopic anus
-Cutanous fistula ,extending to the perineum or to the scrotum or ventral
skin of penis in male.
-Ano vestibular fistula in females
There are some variations between male and females .
2
2.
High type
(Rectal deformities),in this group the colon or rectum terminates above the
levator ani muscles ,there may be a fistulous communication to the urinary tract in
males(Recto-urethral fistula) or to the genital tract in females(recto-vaginal fistula) ,some
times there is no connections .
There is a higher rate of associated anomalies in the urinary tract ,vertebral column
,alimentary canal and heart ,for this reason the mortality is higher than low type lesions in
addition to technical difficulties (i.e. pull through surgery).
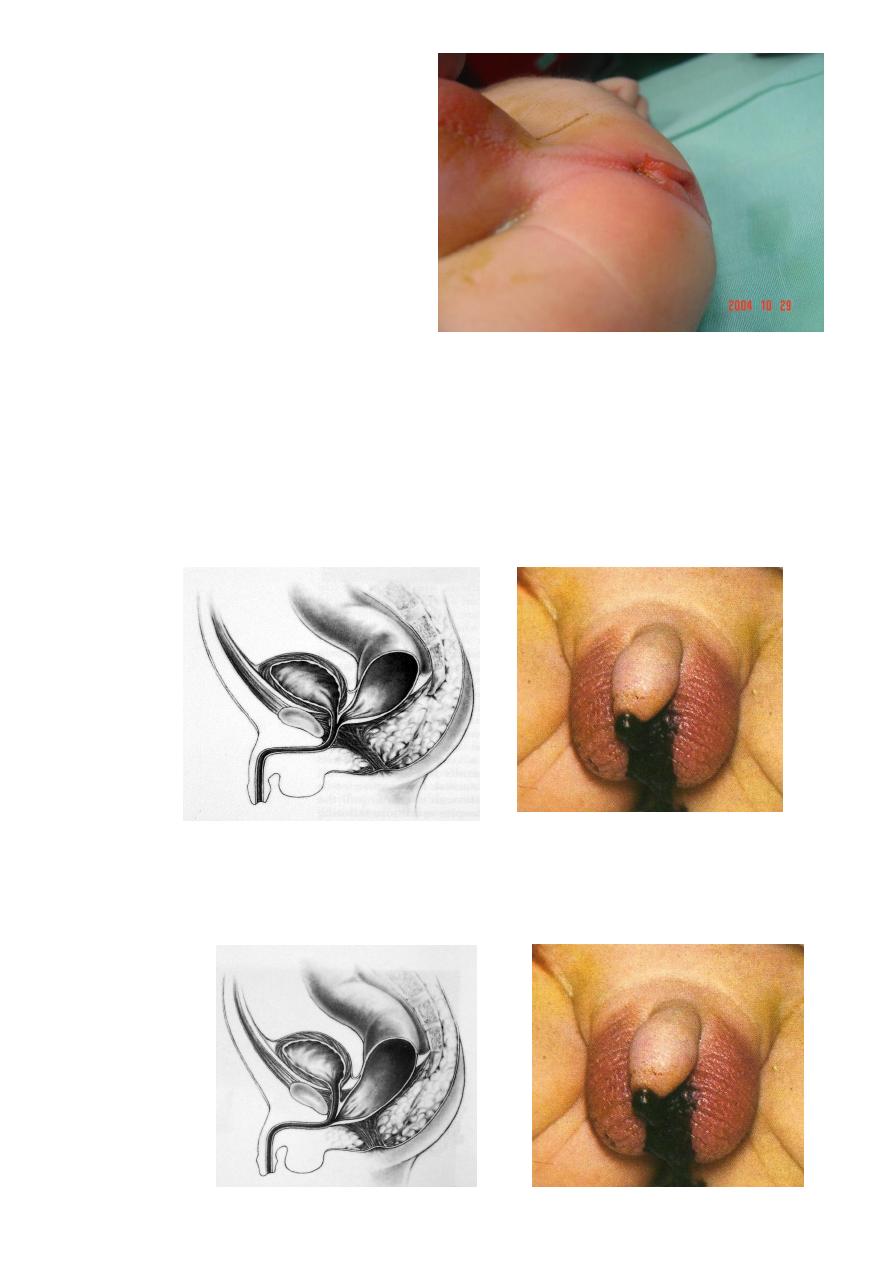
Clinical features :
Any newborn baby should be examined for the presence of congenital abnormalities.
Examination of the perineum is part of this routine examination, which may reveal the
absence or abnormal anal opening .
Some times the parents are unaware of the baby problem and they bring him with
abdominal distention , vomiting and the passage of meconium through the urethra or
vagina .
Infants with anal stenosis may present weeks or months later with excessive screaming on
defecation with the passage of toothpaste like stool due to narrow anus.
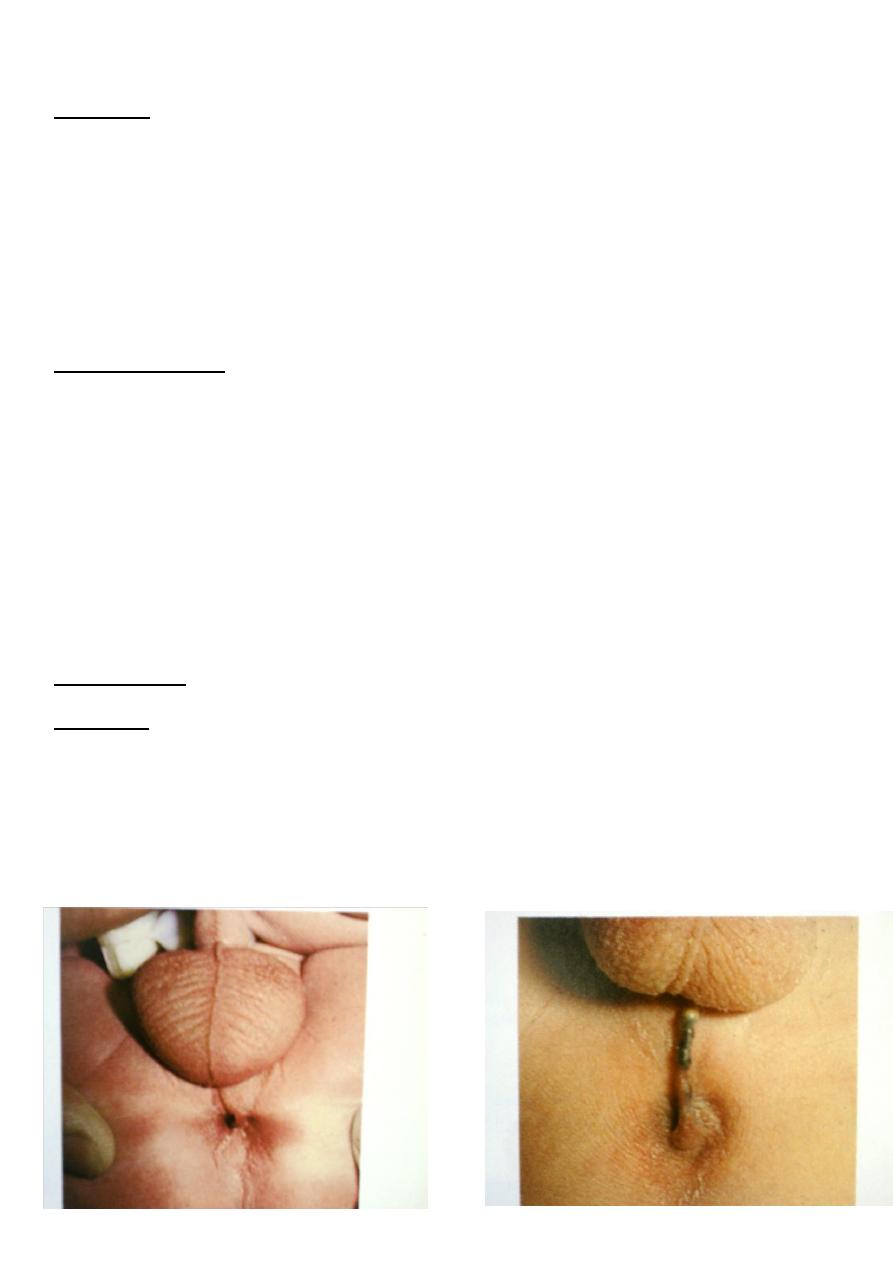
Examination:
we may be able to differentiate low from high lesions :
Low type
there is anal dimple with:
- Stenosed anus :you can’t admit you little finger .
- Covered anus with skin covering the anus with meconium under the skin .
- Anterior ectopic anus .
- Cutanous fistula filled with meconium.or vestibular fistula.
3
High type:
- flat perineum(no anal dimple)
- Meconium may be passed from the urethra or vagina indicating the presence of fistula .
TYPES OF DEFECTS ( classification )
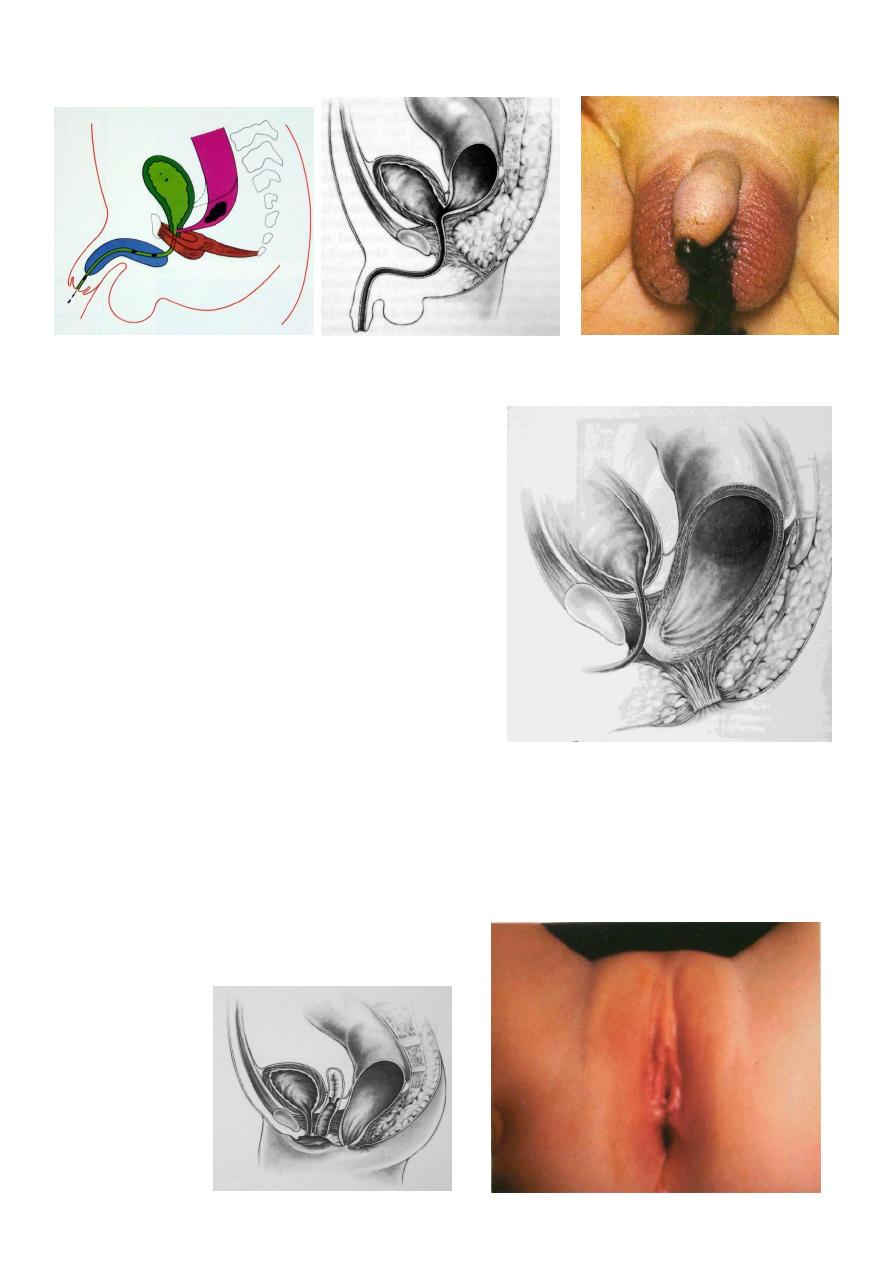
MALE DEFECTS
1. Low Defects : Perineal fistula
Median raphe fistula
Bucket handle malformation
Anal stenosis
Anal membrane
4
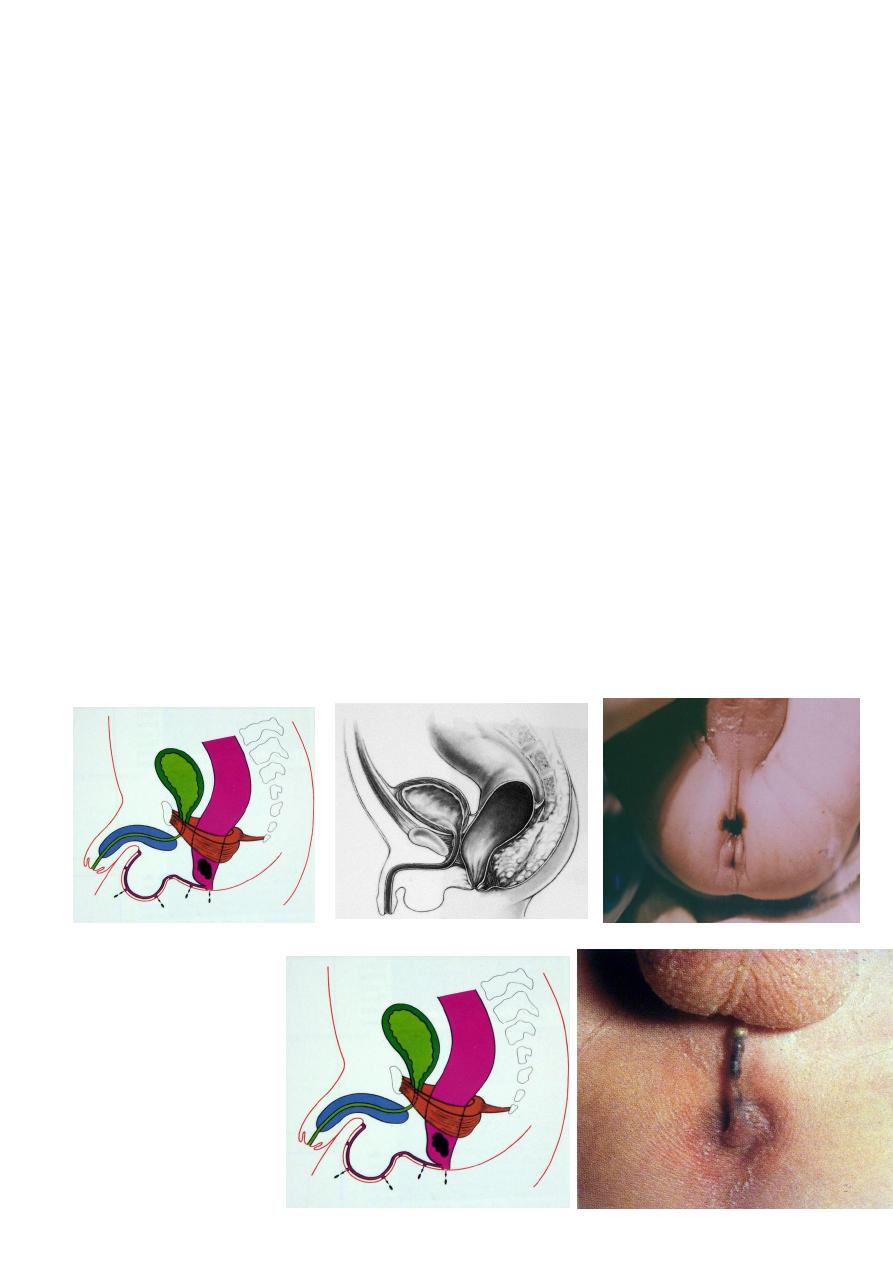
2. Rectourethral bulbar fistula
3. Rectourethral prostatic fistula
4. Rectovesical ( bladder neck ) fistula
5. Imperforate anus without fistula
6. Rectal atresia and stenosis
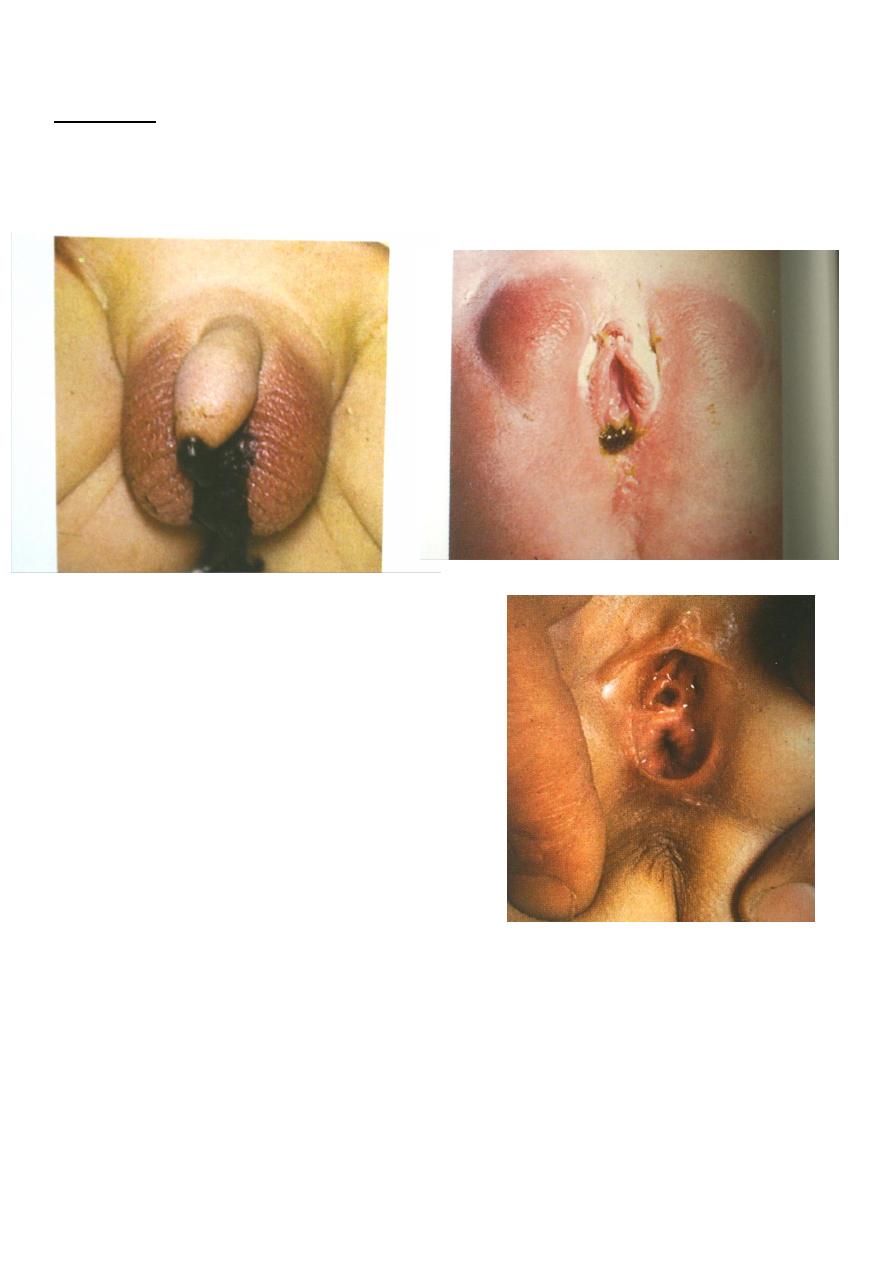
FEMALE DEFECTS
1. Low defect : Perineal fistula
2. Vestibular fistula
3. Vaginal fistula
4. Imperforate anus without fistula
5. Rectal atresia and stenosis
6. Persistent cloaca
MALE DEFECTS
1. Low Defects :
Perineal fistula
Median raphe fistula
5
Bucket handle malformation
Anal stenosis
Anal membrane
2.Rectourethral bulbar fistula
3. Rectourethral prostatic fistula
6
4
. Rectovesical (bladder neck ) fistula
5. Imperforate anus without fistula
6. Rectal atresia and stenosis
( as in female )
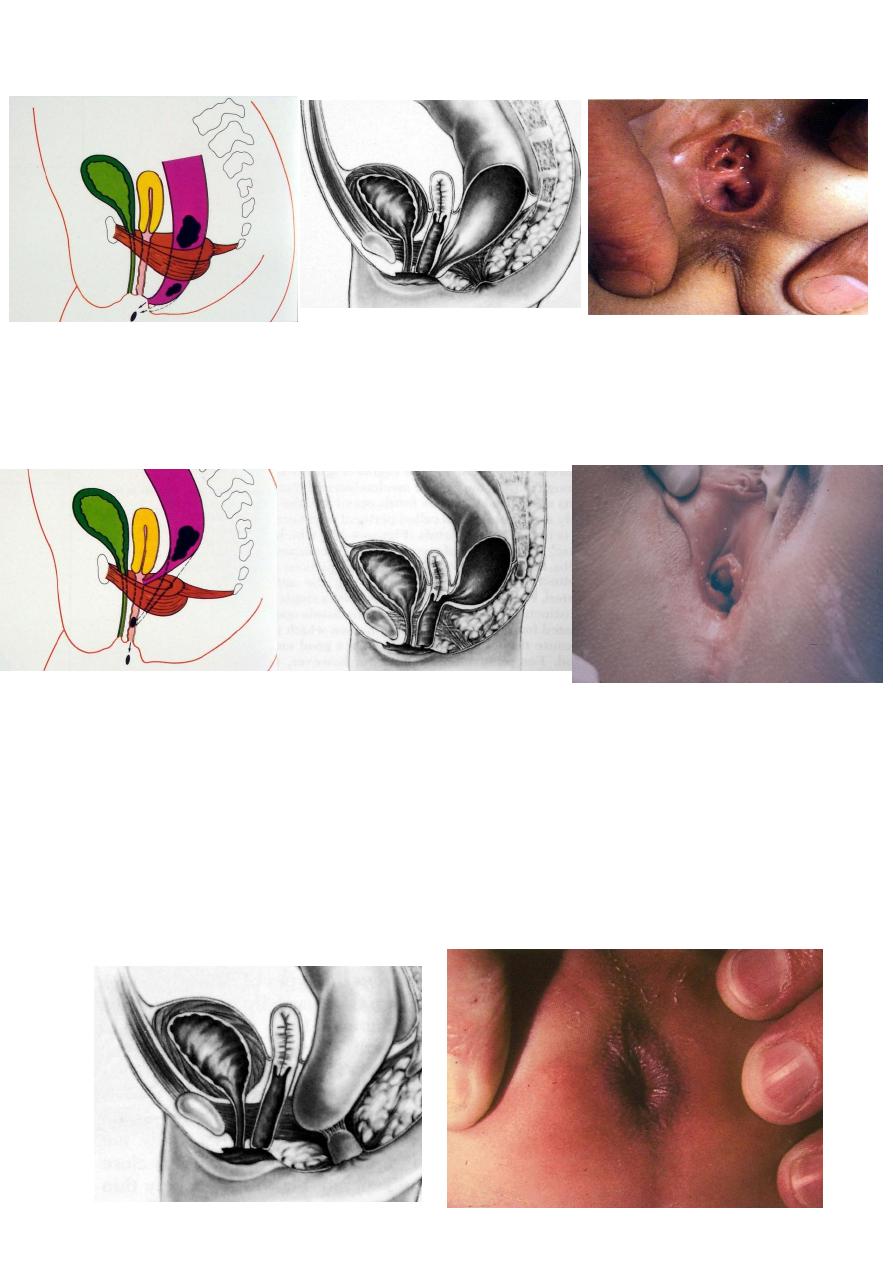
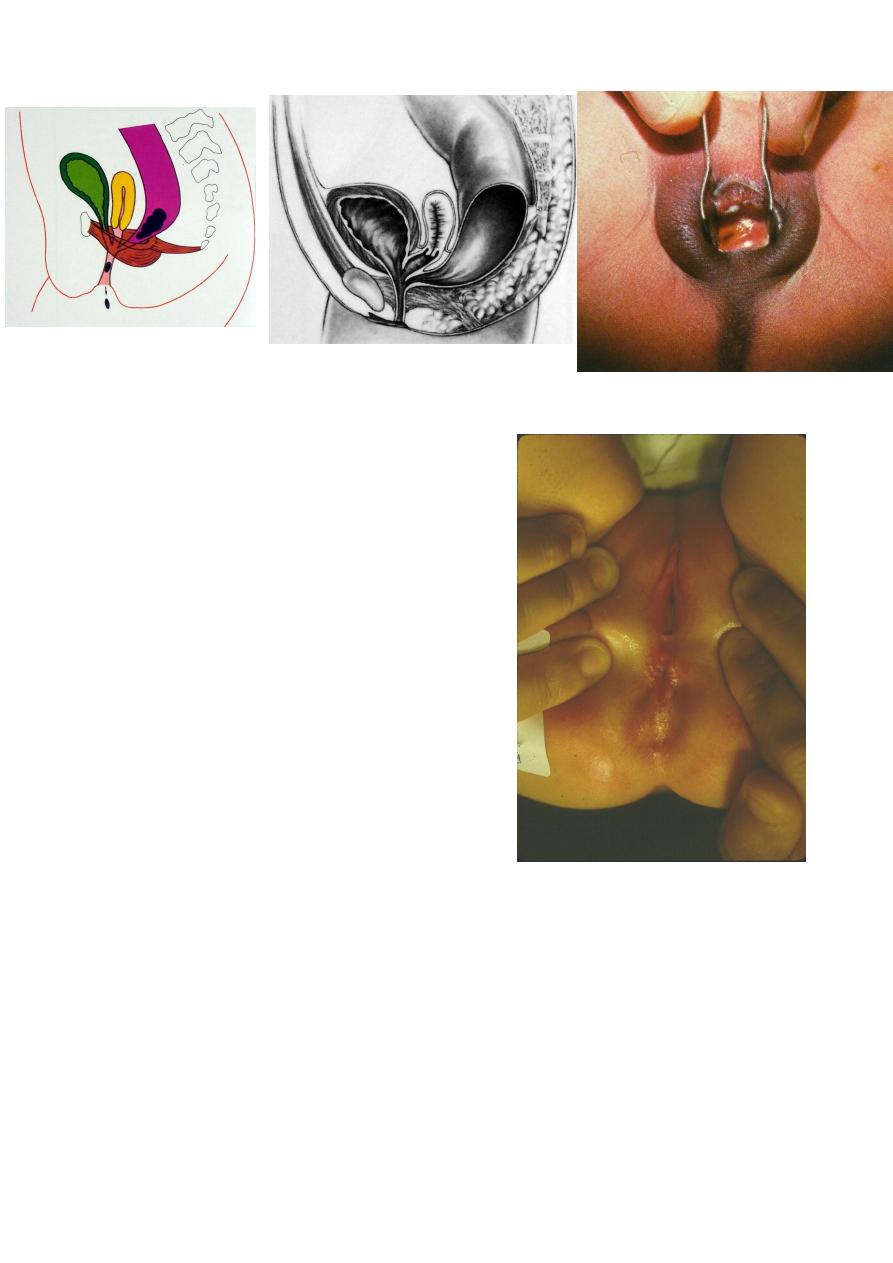
Female Defects
1.
Low Defect : Perineal Fistula
7
2. Vestibular fistula (3 orifices)
3. Vaginal Fistula (2 orifices )
4. Imperforate anus without fistula
( as in male )
5. Rectal atresia and stenosis
8
6. Persistent cloaca (1 orifice)
N.B. Anteriorly displaced anus
is a normal anus
situated anteriorly
ASSOCIATED DEFECTS
Urogenital
- Most common
- 20 – 45 %
-the higher the malformation the higher the incidence.
9
Sacrum and Spine
- Sacrum frequently abnormal deformed
reduced in number
hemisacrum
- Spine frequently shows hemivertebrae
Investigations:
1. General Urine Examination(GUE).the presence of meconium indicate the presence of fistula
to the bowel.
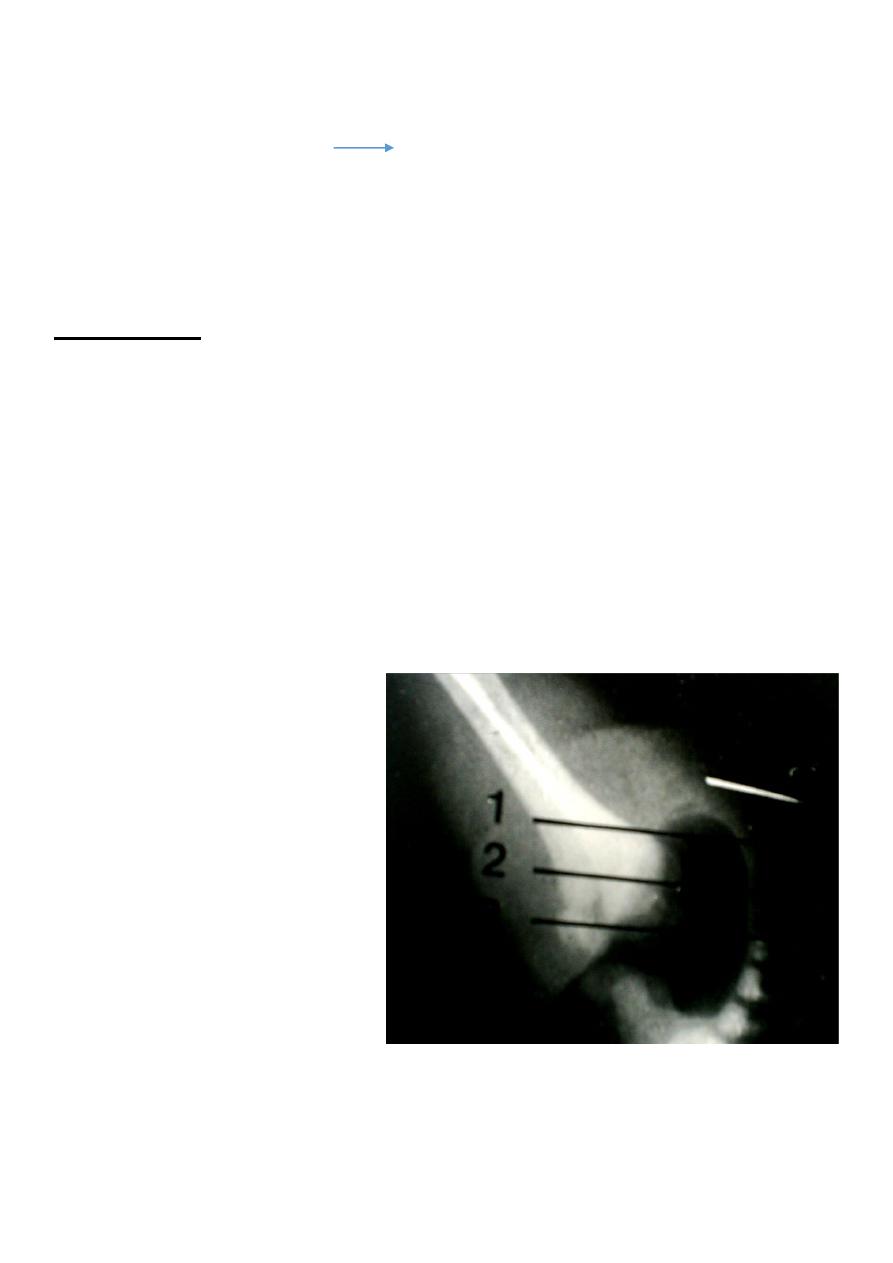
2. Invertogram X-ray taken 12-18 hours after birth ,inverted position ,lateral view, after
putting a mark to see the distal bowel end and it’s relation to pubococcygeal line and the
distance to the mark.
3. X-ray of the spine for vertebral anomaly (e.x.sacral agenesis).
4. Very rarely :we may need to do micturating cysto-urethrogram(MCU)for fistulas or other
urological anomalies e.x. neurogenic bladder or vesico-ureteric reflux .
11
Management of Anorectal Malformations:
Low type lesions have good prognosis .Surgical reconstruction is much simpler and
continence is usually normal .Colostomy is not required and the fistulas don’t involve other
viscera and the coexisting anomalies are less common and less severe.
Anal stenosis :repeated anal dilatation with dilators.
Imperforated anal membrane (covered anus)need incision and dilatation .
Anterior ectopic anus :mild form need nothing or only dilatation .Severe form need cut
back surgery or transposition .
Anovestibular fistula(low type):transposition surgery with or without colostomy.
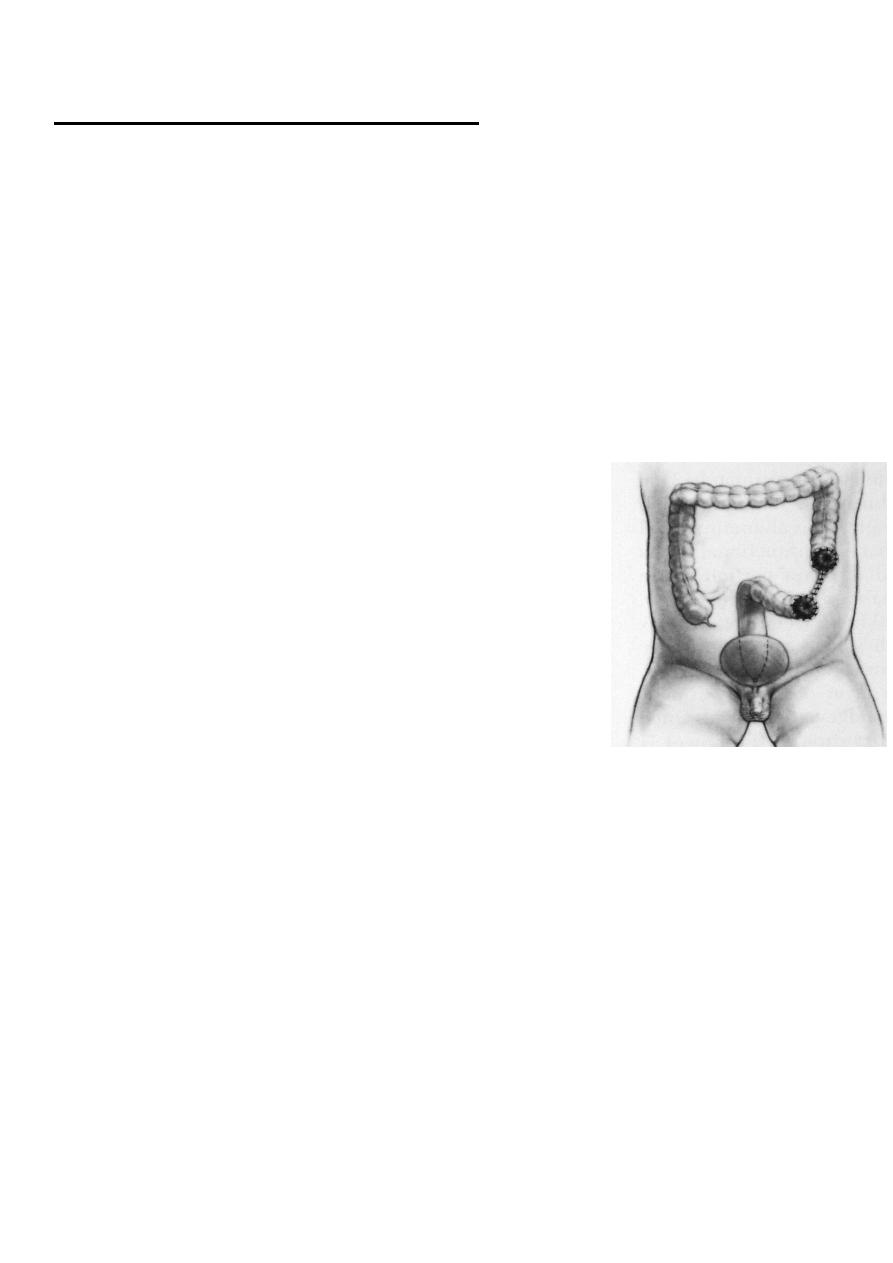
COLOSTOMY
Type :
sigmoid defunctioning with separate stomas
Site :
junction of descending with sigmoid
Incision :
left iliac , muscle cutting
N.B. Distal loop should be cleared of meconium during
operation
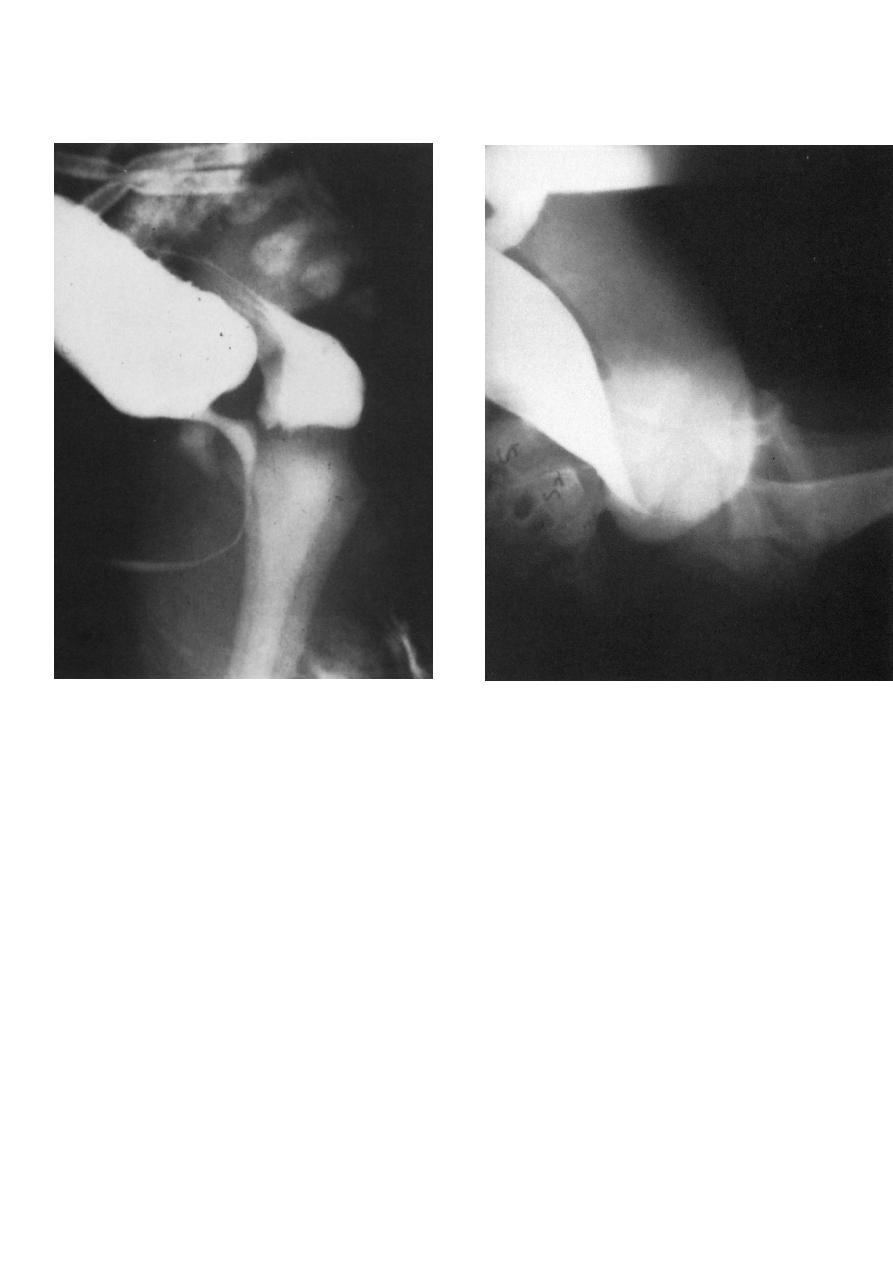
DISTAL COLOSTOGRAM
-
Most valuable test
-
Water soluble contrast into distal stoma
-
Significant pressure needed
-
Under fluoroscopic control
-
Contrast usually fills proximal urethra &bladder
-
Injection must continue till a voiding episode
-
Pictures taken during micturition

11
-
It shows in a single picture :
sacrum
height of rectum
perineum
fistula location
bladder
vesicoureteral reflux
urethra
No need for voiding cystourethrography or cystoscopy
Rectourethral bulbar
fistula
12
Rectour
ethral prostatic fistula
High types:
The prognosis is not good especially in those with multiple congenital anomalies
.Continence is usually affected .
Surgery include:
1.
Colostomy done at the neonatal period .
2.
The definitive surgery done at 9-12months by penna technique or posterior sagital
anorectoplasty (PSARP),through posterior midline incision exploring the end of the
rectum & separating the fistula connected to the urethra in males or the vagina in
females .Then the rectum is pulled through the puborectalis muscle ,closing the muscle
around the rectum &fixing the new opening in the perineum
3. Colostomy closure 4-6 weeks later .
Rectovesical (bladder neck ) fistula