Fifth stage Lec-2
د
.
عبد الرحمن عبد العزيز
Medicine
30/10/2016
Gastrointestinal bleeding in infancy and childhood
Bleeding whether mild or massive can occur from either end of the alimentary tract.
The appearance of even small amount of blood in the vomits or mixed with stool Is the cause of
anxiety to parents and hospital staff.
The assessment of blood lose should be related to the size and weight of the child.
Blood volume in the children usually estimated as 80 ml of blood per kg body weight .
So the blood volume in the neonate who's weight is 3 kg is 240 ml (approximately half pint)
Alimentary tract bleeding may present with a variety of symptoms, according to the level and
rate of hemorrhage. It may be ‘occult’ and present as iron-deficiency anemia, or it may be seen
as blood passed per rectum; in this instance, there may be malena (dark changed blood)or bright
red bleeding .
GASTRO INTESTINAL BLEEDING CAN BE GROUPED UNDER FOUR
DIVISION
1.Anorectal bleeding
2.Hemorrhage in the neonates.
3.Bleeding with other clinical feature.
4.Massive bleeding (haematamess and malena)
ANO RECTAL BLEEDING :
To know the cause of ano rectal bleeding we have to ask about the following:
1.
Amount of the bleeding.
2.
Color of the bleeding.
3
Whether painless of painful.
4.
Presence or absence of any prolapsing mass.
5.
History of trauma or fall.
6.
Any familial bleeding tendency.
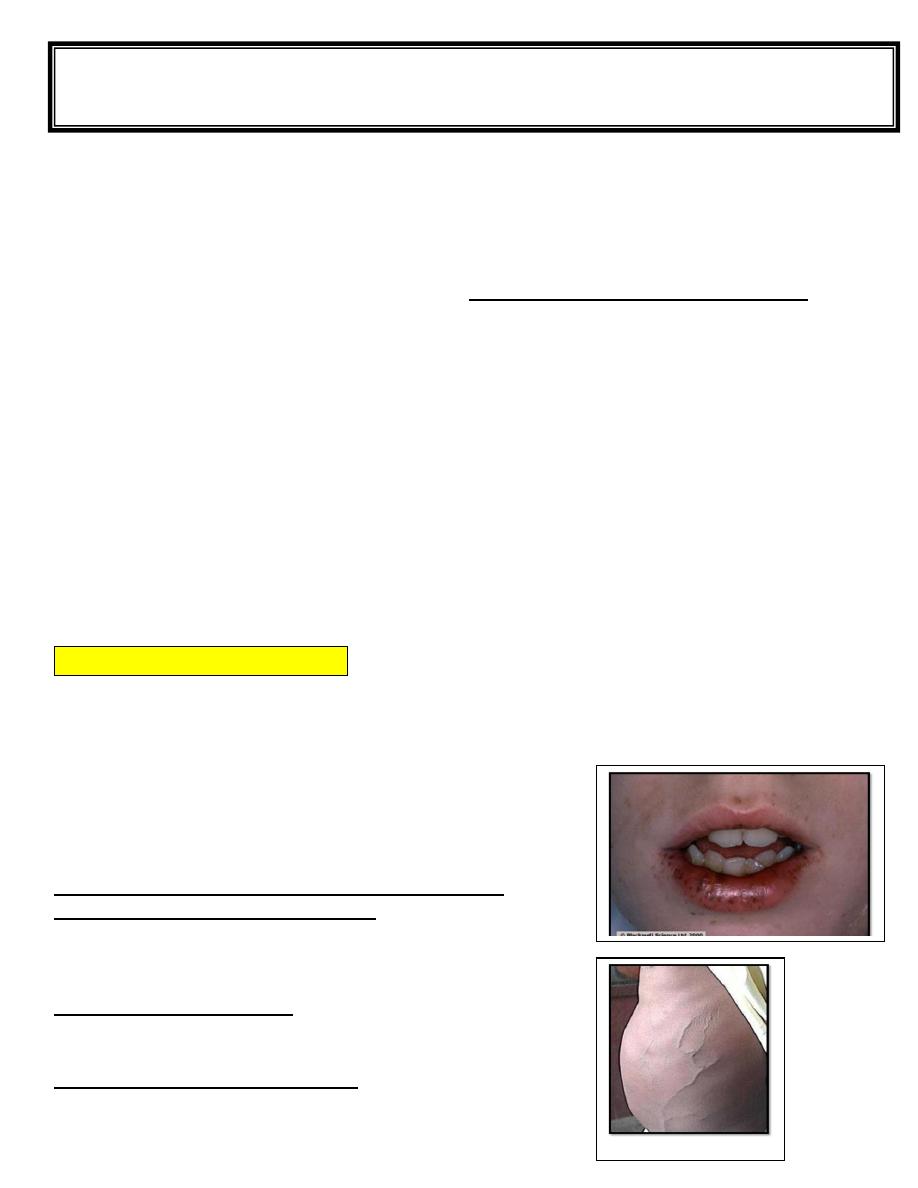
On physical examination we have to look for:
1.General appearance of the patient: including
- the face ,the skin ,and mouth looking for anemia.
- Purpora haemangioma and circum oral melanin spots.
2.Abdominal examination: looking for
liver or splenic enlargements ,ascites or any dilated veins.
3. Examination of the extremities:
For painfull or swollen joints
Fifth stage Lec-
د
.
عبد الرحمن عبد العزيز
Surgery
30/10/2016
On local examination
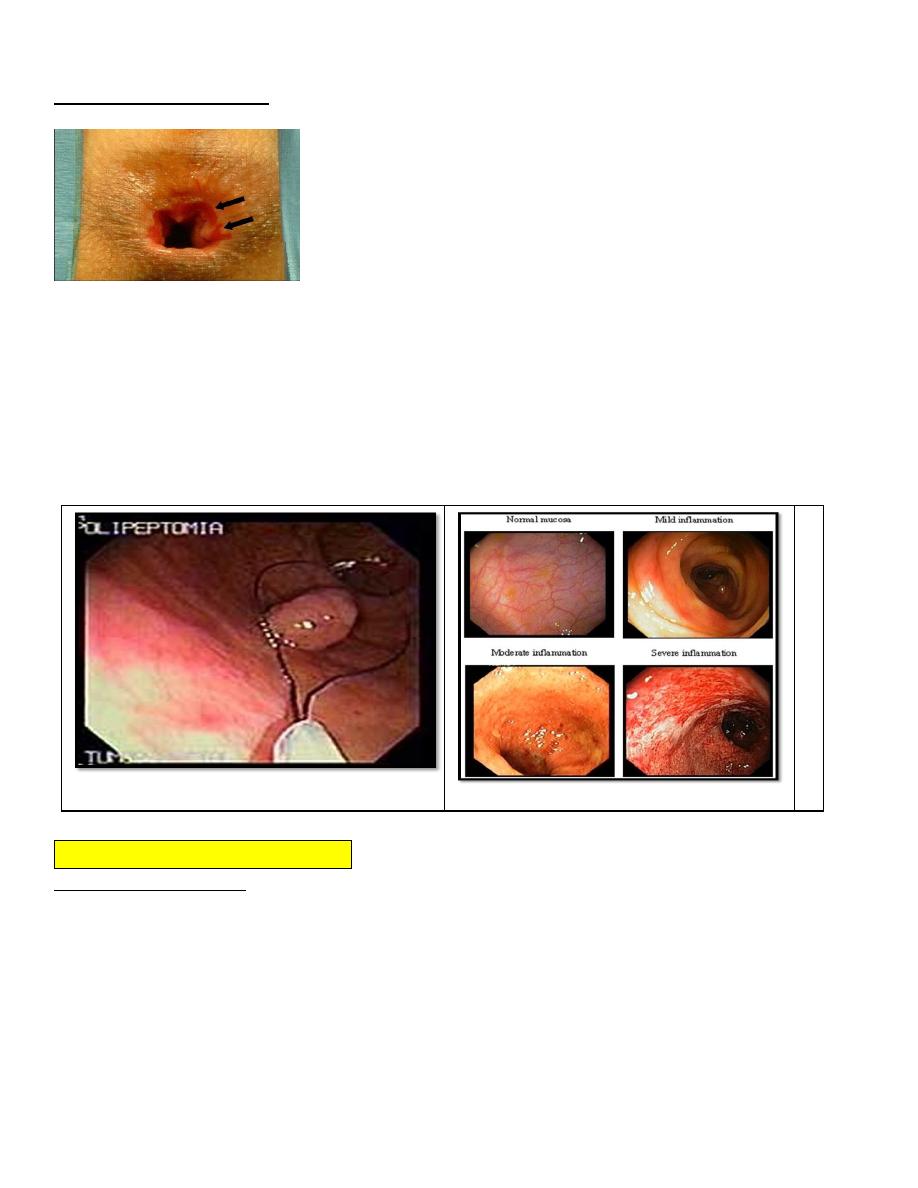
Inspection of the anal verge may reveal fissure in the anal mucosa or rectal prolapse or polyp.
Rectal examination my reveal fecal impaction constipation and juvenile rectal polyp which can
be delivered out side the anus .
Some time the cause of the bleeding can not be determined by history and clinical examination .
Further investigation may be required
1.Stool examination to see whether there is any pus cells ,or worm infestation .
2.Barium enema and double contrast enema as in case of multiple familial polyposis.
3.Endoscopic examination whether rigid sigmoidoscope or flexible colonoscopy to look for
Ulcerative colitis or polyps or hemangioma or telangactasias
Hemorrhage in the neonates.
RECTAL BLEEDING In the neonate is very rare .
Dark blood mixed with mucous occur in the volvulous neonatorum.
Bloody diarrhea with abdominal distension and vomiting is a feature of necrotizing
Enterocollitis Which could occur in the newborn baby especially at the first two weeks of life
and usually occur in the premature babies Or baby subjected to a distress such as respiratory
distress syndrome.
HAEMORRHAGE WITH OTHER SYMPTOM AND SIGNS
Here in these condition bleeding is one of the less important clinical feature examples:
1.
INTUSSUSCEPTION
:which occur at the age of 6-9 months usually the baby
present with screaming or crying ,vomiting and abdominal mass with passage of red
current jelly stool ,which is due to blood mixed with mucous secretion of the alimentary
tract.
2.
ULCERATIVE COLLITIS
:
Can affect young children between 6- 12 years and the main feature here is weight loss, anemia,
chronic diarrhea and abdominal pain. in rare situation the patients may develop Massive
hemorrhage which may necessitate urgent surgical treatments(total collectmy)
3. GASTRO INTERITIS :
here the condition occur acutely with abdominal pain
,vomiting and diarrhea
The condition is usually associated with fever and in rare condition bleeding may occur
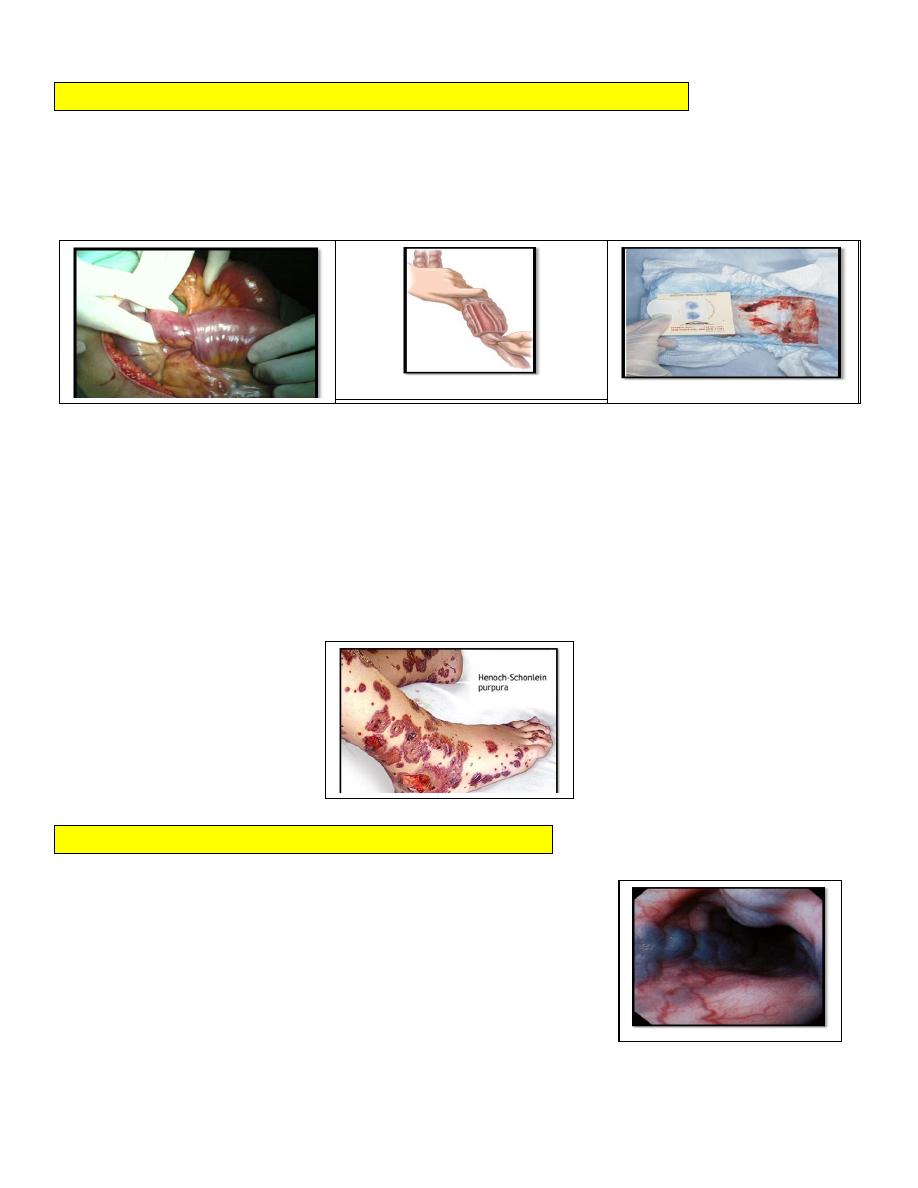
4. HENOCH-SCHOENLIEN PURPURA:
Gastrointestinal bleeding may occur here the patient has got purpuric spots ,joint involvement in
addition to GIT involvement.
MASSIVE GASTROINTESTINAL BLEEDING
This is not a common pediatric problem, but 2 conditions are common and have to be
considered
1.Hematamesis from esophageal varices in portal hypertension.
2. Malena from peptic ulcer especially from the site of mickle,s diverticulum

PORTAL HYPERTENSION
Portal hypertension in children is the result of obstruction of the blood flow from the portal vein
system into the inferior vena cava-according to the site of obstruction tow type were recognized
1. Intra –hepatic obstruction result from liver cirrhosis .whether from hepatitis or biliary
atresia.
2. Extra-hepatic which is more common in children usually due to neonatal sepsis with
spread of infection and thrombosis along the umbilical vein to the portal vein.
The portal venous pressure will rise to 250-300 ml of water this will cause enlargement of the
spleen and development of the collateral circulation specially the gastro – esophageal venous
plexus were bleeding may developed
MICKLES DIVERTICULUM
Some times bleeding from mickles diverticum is very difficult to diagnose. mickles diverticum
is present in 2 % of population .Ectopic tissue in the lining is found in more than 50% of them
.gastric mucosa or pancreatic tissue may be found may be found and it is not rare to find both
lining together.
The diverticulum is symptom less until complication occur .
These complication present in one of the following ways.
1. Massive hemorrhage. 45%
2. Intestinal obstruction. 25%
3. Acute inflammation. 20%
4. Persistent communication with the umbilicus. 10 %
Massive hemorrhage occur in children less than 3 years ,usually stared as malena than
become bright red ,it is painless bleeding and sometime very difficult to prove the diagnosis
1. Barium meal, follow through and enema is not helpful.
2. The diverticulum is not with in reach of colonoscopy .
3. Angiogram ,if the rate of bleeding is rapid (helpful)
4.Technetium scan (TC
99
), here the isotope is concentrated in mickles diverticulum
5. Laparotomy or laparoscopy may be required in some cases to diagnose and to treat such
problem
A technetium
scan showing
ectopic gastric
mucosa