Giardia&lamblia&
&
&
&
!
!
1!
Giardia lamblia
Historical background
Giardia was originally observed by von Leeuwenhoek in 1681, in his own
diarrheal stool, and was described by Vilem Dusan Lambl in 1859 and by
Alfred Giard in 1895.
Although G intestinalis is one of the first protozoan parasites described, its
role, as a pathogenic organism was not recognized until the 1970s, after
outbreaks.
Morphology:
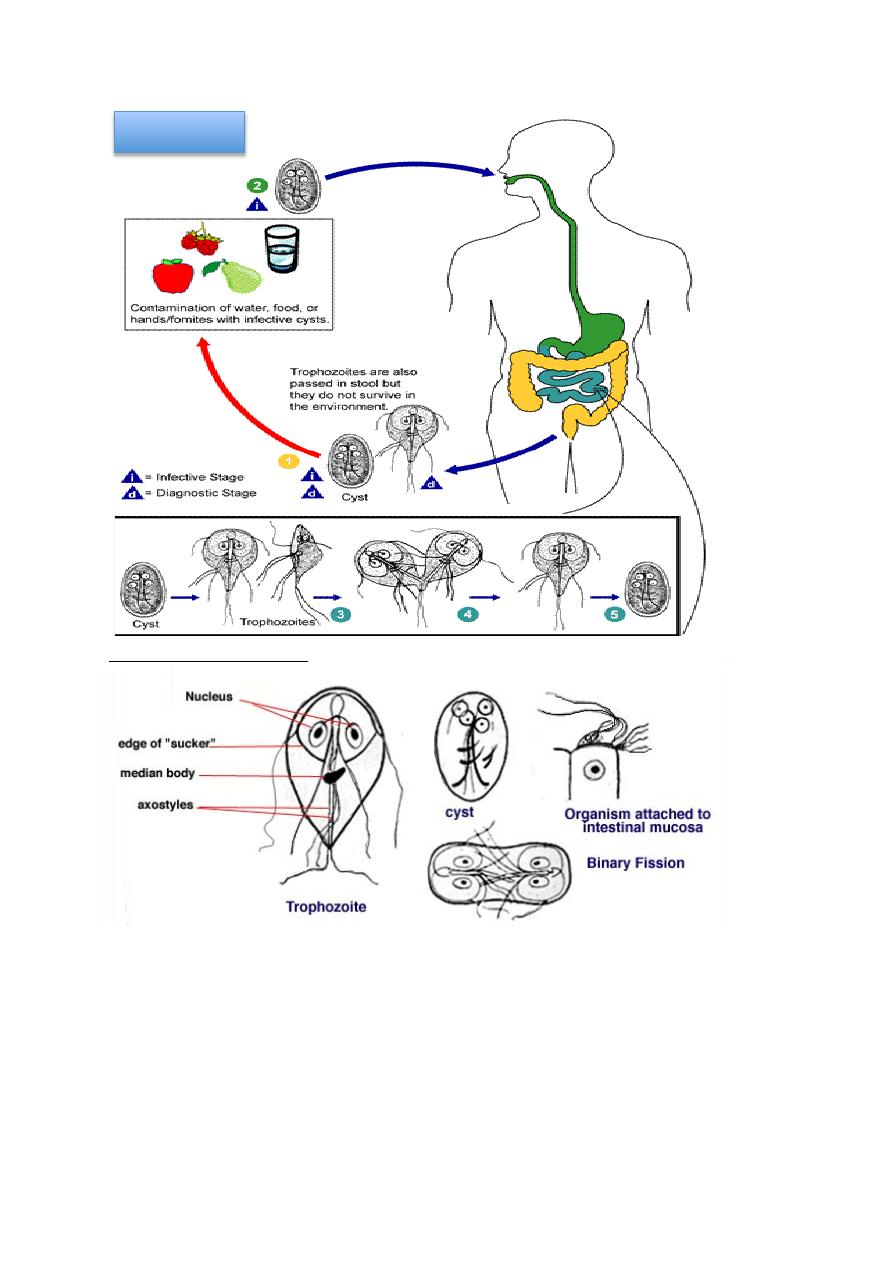
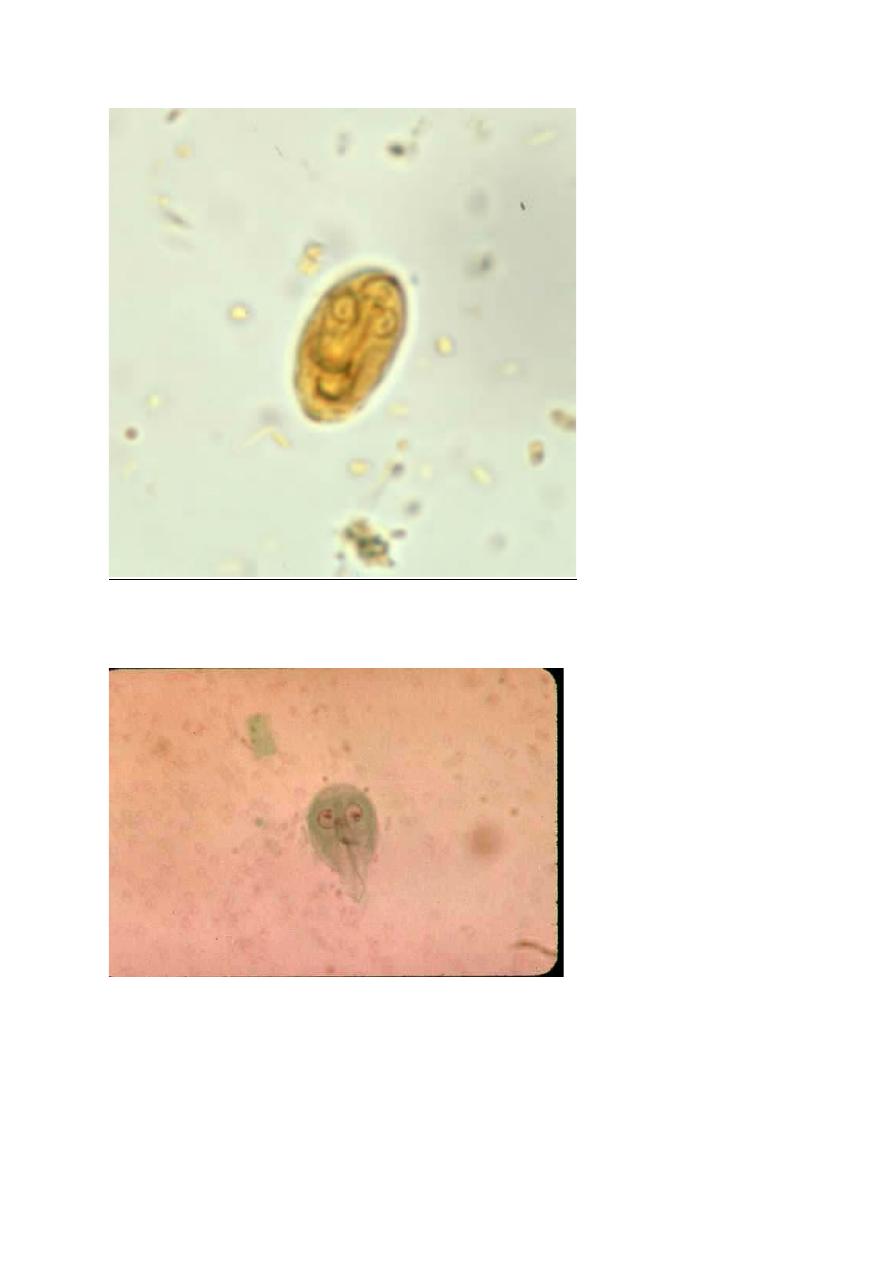
The cyst form of the protozoan is smooth-walled and oval in shape, measuring
8-12 µm long by 7-10 µm wide. As the cyst matures, nuclear division occurs.
Mature cyst contains 4 nuclei and then the cyst releases 2 trophozoites upon
excystation. Once the host is infected, trophozoites may appear in the
duodenum within minutes. Excystation occurs within 5 minutes of exposure of
the cysts to an environment with a pH between 1.3 and 2.7.
The trophozoite form of G lamblia is teardrop-shaped and measures 9-21
micrometers long by 5-15 micrometers wide. The trophozoite has a convex
dorsal surface and a flat ventral surface that contains the ventral disk. The
trophozoite also contains long axostyles, 4 pairs of flagella, directed posteriorly,
that aid the parasite in moving. Two symmetric nuclei with prominent
karyosomes produce the characteristic face like image that appears on stained
preparations.
Life cycle:
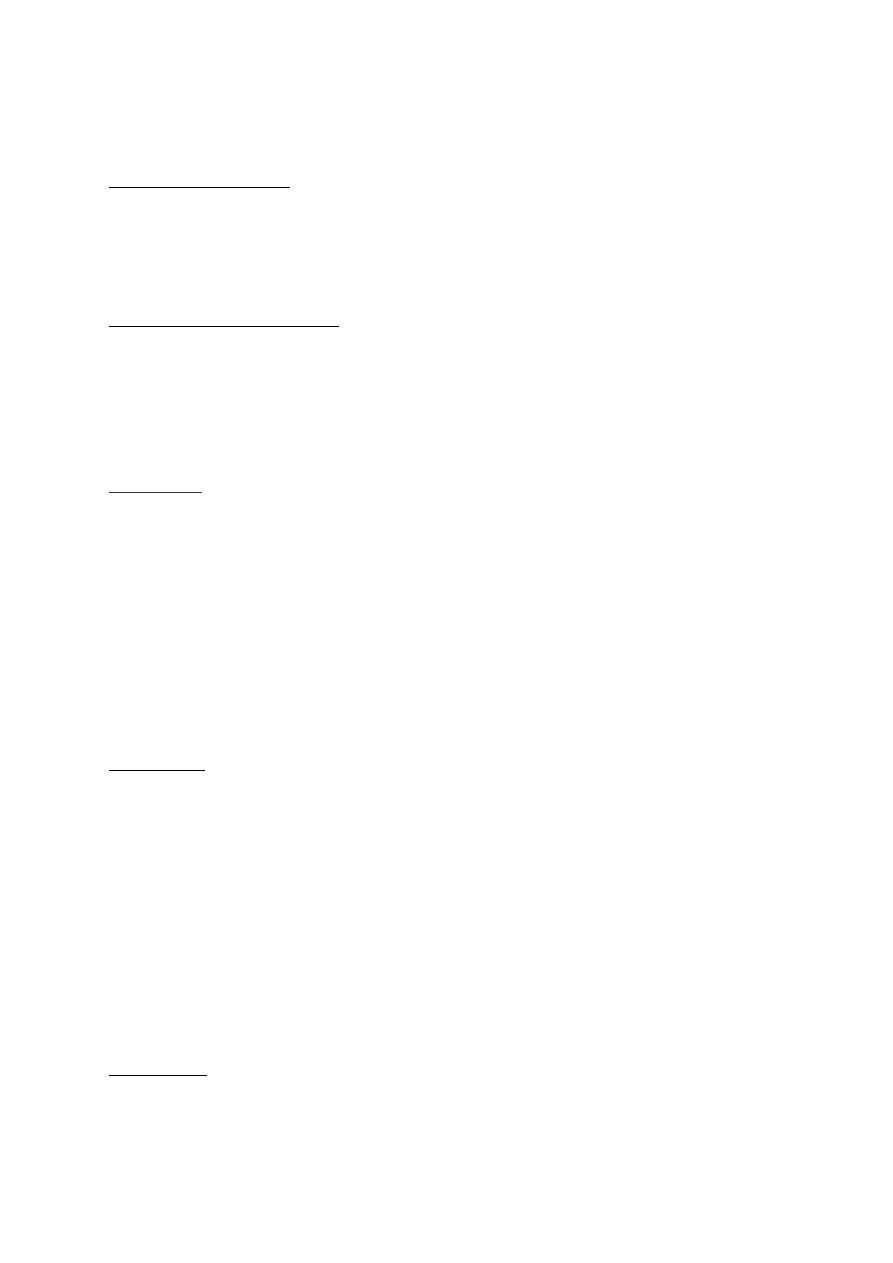
Giardia lamblia (also known as Giardia intestinalis, or Giardia duodenalis)
is a microscopic parasite that causes diarrheal illness known as giardiasis.
Giardia cyst (the infective stage) is found on surfaces or in soil, food, or water
that has been contaminated with feces from infected subjects. Giardia cyst is
protected by an outer shell that allows it to survive outside the body for long
periods of time and makes it tolerant to chlorine disinfection. The parasite can
be spread in different ways; water (drinking water and recreational water) is
regarded the most common mode of transmission. Cysts are responsible for
transmission of giardiasis.
(1) Both cysts and trophozoites can be found in the feces (both regarded as
Giardia&lamblia&
&
&
&
!
!
2!
diagnostic stages).
(2) The cysts are hardy and can survive several months in cold water. Infection
occurs by the ingestion of cysts in contaminated water, food, or by the fecal-oral
route (hands or fomites). Because the cysts are infectious when passed in the
stool or shortly afterward, person-to-person transmission is possible.
(3) In the small intestine, excystation releases trophozoites (each cyst produces
two trophozoites).
(4) Trophozoites multiply by longitudinal binary fission, remaining in the lumen
of the proximal small bowel where they can be free or attached to the mucosa
by a ventral sucking disk
(5) Encystation occurs as the parasites transit toward the colon. The cyst is the
stage found most commonly in non-diarrheal feces.
Geographic Distribution:
Worldwide, more prevalent in warm climates, especially among children.
Giardia intestinalis has been isolated from the stools of beavers, dogs, cats, and
primates. Beavers may be an important reservoir host for G. intestinalis.
However there is a small risk from getting infection from cats and dogs because
of differences among the human and cats or dogs strains The organism has been
found in as many as 80% of raw water supplies from lakes, streams, and ponds
and in as many as 15% of filtered water samples. Giardia species are endemic
in areas of the world that have poor sanitation. In developing countries, the
disease is an important cause of morbidity. Water-borne and food-borne
outbreaks are common.
Clinical Picture:
The mechanisms by which Giardia causes diarrhea and intestinal
malabsorption are probably multifactorial.
The proposed pathological
mechanisms include damage to the endothelial brush border, enterotoxins,
immunologic reactions, and altered gut motility and fluid hyper secretion.
G. intestinalis can cause asymptomatic colonization , acute or chronic diarrheal
illness and malabsorption. Because ingestion of as few as 10 Giardia cysts may
be sufficient to cause infection, giardiasis is common crowded areas and
institutions in developed countries.
High-risk groups for giardiasis include travelers to highly endemic areas,
patients with hypochlorhydria, immune compromised individuals, and certain
sexually active homosexual men, patients with malnutrition, patients with cystic

Giardia&lamblia&
&
&
&
!
!
3!
fibrosis and blood group A and crowded areas. Cyst passage rates as high as
20% have been reported among certain groups of sexually active homosexual
men. These individuals were frequently symptomatic.
Acute giardiasis develops after an incubation period of 1 to 14 days (average of
7 days) and usually lasts 1 to 3 weeks. Acute symptoms include:
• Diarrhea
• Gas
• Greasy stools that tend to float
• Stomach or abdominal cramps
• Upset stomach or nausea/vomiting
• Dehydration (loss of fluids)
The symptoms of giardiasis might seem to resolve, but come back again after
several days or weeks. Giardiasis can cause weight loss and failure to absorb
fat, lactose, vitamin A and vitamin B12.
In children, severe giardiasis might delay physical and mental growth, slow
development, and cause malnutrition.
Diagnosis:
Stool examination:
The traditional basis of diagnosis is identification of Giardia intestinalis
trophozoites or cysts in the stool of infected patients via a stool ova and parasite
(O&P, i.e. general stool examination) examination. Fresh stool can be mixed
with an iodine solution or methylene blue and examined for cysts on a wet
mount. If not immediately examined, stool should be preserved in 10%
formalin, with subsequent trichrome or iron hematoxylin staining. Trophozoites
may be found in fresh, watery stools but disintegrate rapidly. If the stool is not
fresh or is semi formed to formed, trophozoites will not be found. Cysts are
passed in soft and formed stools.
Ideally, 3 stool samples from each patient on different days should be examined
because of potential variations in fecal excretion rate of cysts. G intestinalis is
identified in 50-70% of patients after a single stool examination and in more
than 90% after 3 stool examinations. Stool concentration methods are also
beneficial in the diagnosis of giardiasis when there is low excretion rate of
cysts.
Cyst passage and may lag behind the onset of symptoms by a week or more.
Because many antibiotics, enemas, laxatives, and barium studies mask or cause
the disappearance of parasites from the stools, microscopic examination should
Giardia&lamblia&
&
&
&
!
!
4!
be postponed for 5-10 days following these interventions. Fecal leukocytes
should not be visualized in stool samples of patients with giardiasis.
Duodenal Aspiration:
Aspiration of duodenal contents and demonstration of trophozoites also have
been used for diagnosis but this is more invasive than stool examination and, in
direct comparison studies to stool microscopy, may have a lower diagnostic
yield.
Stool antigen and serology:
Stool antigen enzyme-linked immunosorbent assays also are available. Since
levels of immunoglobulin G (IgG) remain elevated for long periods, they are
not beneficial in making the diagnosis of acute giardiasis. Serum anti-Giardia
immunoglobulin M (IgM) can be beneficial in distinguishing between acute
infections and past infections.
String Test
The string test (Entero-test) consists of a gelatin capsule containing a nylon
string with a weight attached to it. The patient tapes one end of the string to his
or her cheek and swallows the capsule. After the gelatin dissolves in the
stomach, the weight carries the string into the duodenum.
The string is left in place for 4-6 hours or overnight while the patient is fasting.
After removal, it is examined for bilious staining, which indicates successful
passage into the duodenum. The mucus from the string is examined for
trophozoites in an iodine or saline wet mount or after fixation and staining.
Treatment
Standard treatment for giardiasis consists of antibiotic therapy. Metronidazole is
the most commonly prescribed antibiotic for this condition. The recommended
adult dose is 250 mg orally three times daily (tid) for 5-7 days. However,
tinidazole is now approved and considered a first-line agent .The recommended
dose is 50 mg/kg orally once.
Paromomycin has been recommended for use in pregnancy because systemic
absorption is low, but the cure rate is lower than other agents.
Appropriate fluid and electrolyte management is critical, particularly in patients
with large-volume diarrheal losses.
Prevention
• Infected persons and persons at risk should carefully wash their hands
after they have any contact with feces.

Giardia&lamblia&
&
&
&
!
!
5!
• Infected individuals should be prevented from using swimming pools,
lakes, and rivers until they are symptom-free for few weeks.
• Chlorination, sedimentation, and filtration methods should be
implemented to adequately purify public water supplies. Effective
chlorine inactivation of Giardia cysts in water requires an optimal
chlorine concentration, water pH, turbidity, temperature, and contact
time. These variables cannot be appropriately controlled in all water
supply units, and they are particularly difficult to control in swimming
pools.
• Drinking water can be purified by using filtration (pore size, < 1 µm) or
by briskly boiling water for at least 5 minutes. Chlorine or iodine water
treatments are less effective than boiling or filtration, but they may be
used as alternatives when other methods are not available
• Advise travelers to endemic areas to avoid eating uncooked foods that
may have been grown, washed, or prepared with contaminated water.
• Breastfeeding appears to protect infants from Giardia intestinalis
infection Breast milk contains detectable titers of secretory IgA, which is
protective for infants, especially in developing countries.
Giardia&lamblia&
&
&
&
!
!
6!
Life cycle of G.lamblia
Morphology of Giardia cyst and trophozoite
!
Giardia&lamblia&
&
&
&
!
!
7!
Giardia lamblia cyst in fecal smear
Giardia lamblia trophozoite under microscope