Cryptosporidium
1
1
Cryptosporidium:
Cryptosporidium species are protozoan parasites that infect a broad range of
hosts including humans, domestic and wild animals, causing asymptomatic,
mild to severe gastrointestinal disease in their host species. The most common
species reported in humans worldwide are Cryptosporidium parvum and
Cryptosporidium hominis.
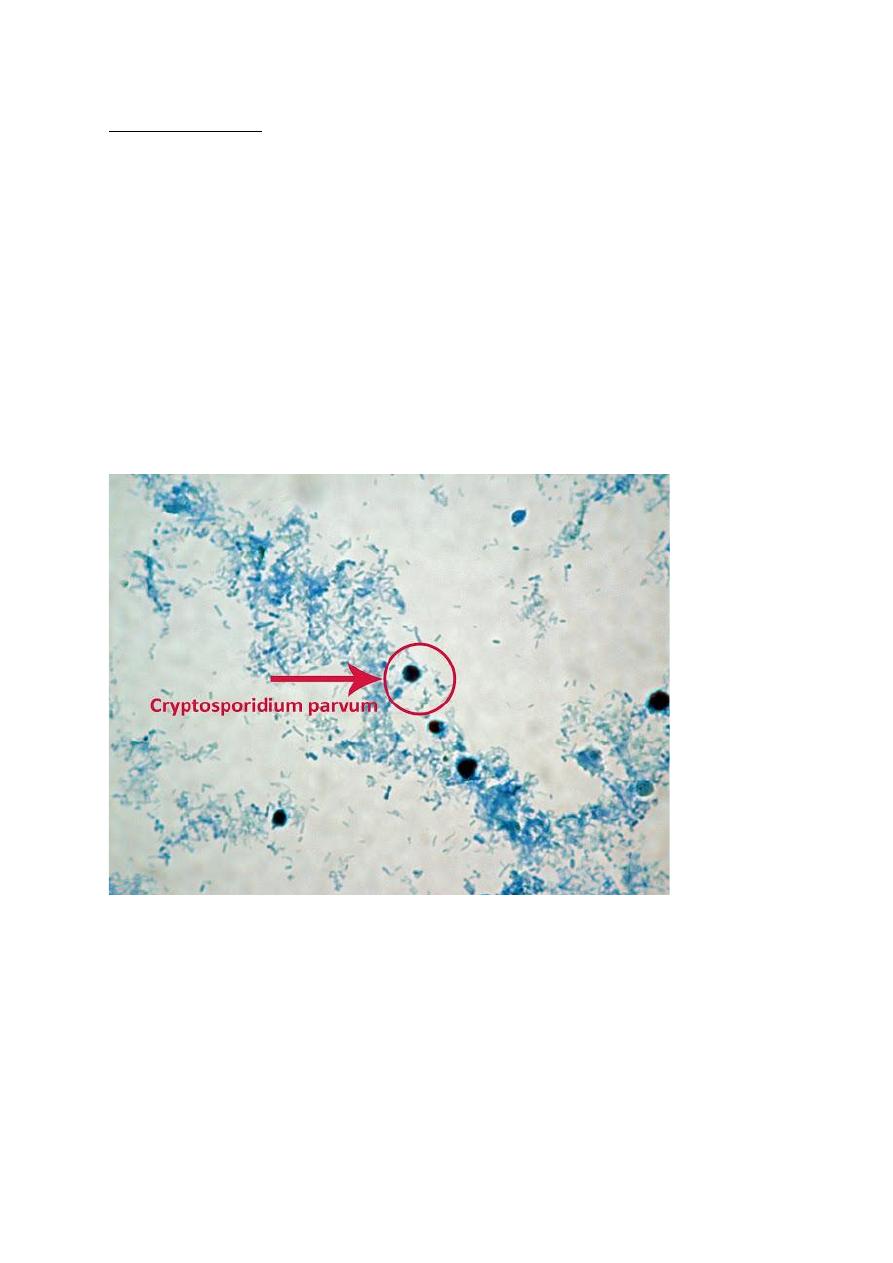
Oocyst morphology:
Round to oval oocyst 4-6 ㎛ in diameter. Oocyst seems often refractile at wet
smear. They appear as black dots or small vacuoles seen after modified acid
fast staining.
Cryptosporidium Oocyst stained by modified acid-fast stain.
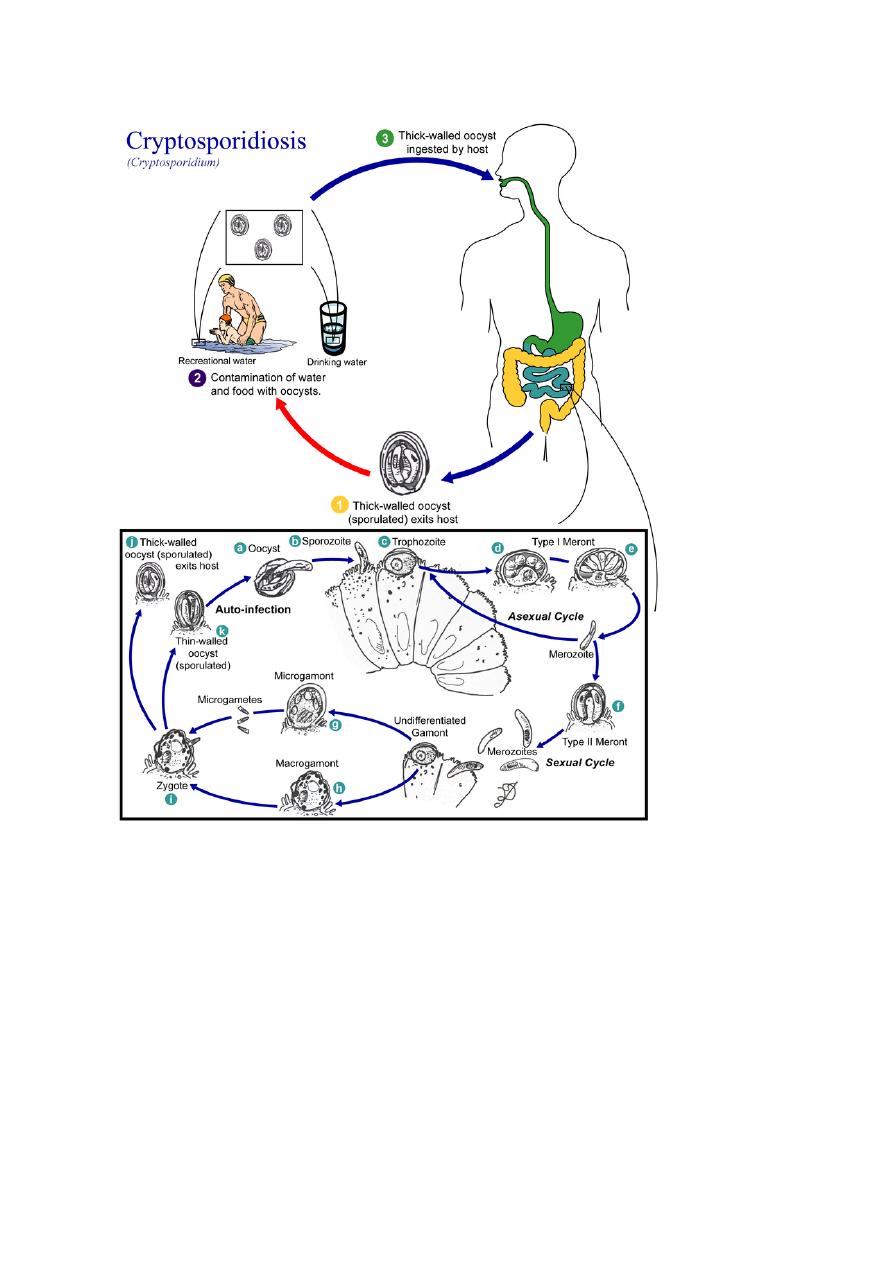
Life cycle
Cryptosporidium species exist as multiple cell types, which correspond to
different stages during the infection (e.g., a sexual and asexual stage).
Cryptosporidium oocyst is hardy, thick-walled, can survive in the environment
for months and is resistant to many common disinfectants, particularly chlorine-
based disinfectants.

Cryptosporidium
2
2
After being ingested, the oocysts exist in the small intestine. They release
sporozoites that attach to the microvilli of the epithelial cells of the small
intestine. They become trophozoites that reproduce asexually by multiple
fission (schizogony). The trophozoites develop into Type 1 meronts that contain
8 daughter cells. These daughter cells are Type 1 merozoites, which get released
by the meronts. Some of these merozoites can cause autoinfection by attaching
to epithelial cells and develop into new trophozoites and multiply a sexually.
Others of these merozoites become Type II meronts, which contain 4 Type II
merozoites. These merozoites get released and they attach to the epithelial cells.
Type II merozoites changed to either macrogamonts or microgamonts. These
are the female and male sexual forms, respectively. This stage, when sexual
forms arise, is called gametogony. Zygotes are formed by microgametes from
the microgamont penetrating the macrogamonts. The zygotes develop into
oocysts of two types. 20% of oocysts have thin walls and so can reinfect the
host by rupturing and releasing sporozoites that start the process over again.
80% of the oocysts are thick-walled oocysts, which are excreted into the
environment. The oocysts are mature and infective upon being excreted.
Cryptosporidium
3
3
Life cycle of Cryptosporidium spp
Transmission of oocysts:
Infected individuals shed large numbers of oocysts (infective stage), which are
environmentally resistant to inactivation by commonly used drinking water
disinfectants including chlorine treatment and are able to survive routine
wastewater treatments. Cryptosporidium oocysts are highly infectious as few as
10 or less Cryptosporidium oocysts can produce disease in healthy adults.

Cryptosporidium
4
4
Mode of transmission:
1-The faecal–oral route, either directly or indirectly.
For humans, direct transmission can be from person to person due to poor
hygiene in overcrowded areas as day care centres, aged care facilities, schools,
kids nurseries and other institutions, or from animals to persons such as
farmworkers and pet owners.
Most indirect transmission is from contaminated drinking or recreational water.
Contaminated food can also be a source of transmission.
2- Cryptosporidium is rarely transmitted via inhalation of aerosolized droplets
or by contact with fomites contaminated by coughing.
Pathogenesis:
Two to ten oocysts are enough to initiate an infection. The parasite is located in
the brush border of the epithelial cells of the small intestine. The parasite can
cause damage to the microvilli where it attaches. The most pronounced
morphologic alteration is villous atrophy, although villous blunting and fusion
might also occur. The severity of mucosal injury correlates with the numbers of
infecting organisms. Moderate to severe infections can be accompanied by a
patchy or prominent neutrophil and mononuclear infiltrate in the lamina propria
and numerous intraepithelial neutrophils. Pro-inflamatory cytokines such as
interleukin IL-1, IL-6, IL-8, and tumour necrosis factor (TNF) are released
during the infection and they could induce leucocytes chemotaxis increasing
inflammatory response in the wall of the intestine. Prostaglandins level
increases leads to increase excretion of NaCl leading to increase severity of
diarrhoea.
The immune status of the host, both innate and adaptive immunity, has a major
impact on the severity of the disease and its prognosis. In immunocompetent
hosts, disease–parasite development and replication is relatively confined to the
terminal jejunum and ileum. In immunocompromised hosts, the entire
gastrointestinal tract, as well as biliary and pancreatic ducts could be infected.
Less frequently there could also be involvement of the respiratory tree.

Cryptosporidium
5
5
Clinical picture:
The incubation period for symptomatic cryptosporidiosis is 1–2 weeks.
Human cryptosporidiosis is frequently accompanied by abdominal pain, fever,
vomiting, malabsorption and diarrhoea, which may sometimes be profuse and
prolonged. Immunocompetent individuals typically experience self-limiting
disease.
Immunocompromised individuals, including HIV/AIDS patients often suffer
from intractable diarrhoea, which can be fatal. Immune compromised patients
may get extra intestinal cryptosporidiosis as biliary involvement, or pancreatitis.
Pulmonary infection in immunocompromised patients leads to respiratory tract
infection symptoms. Rarely, conjunctival irritation is also present.
Cryptosporidium is second only to rotavirus as a major cause of severe
diarrhoea in children. Cryptosporidium spp. is one of the five highest
attributable burdens of diarrhoea in the first year of life. Globally,
cryptosporidiosis is estimated to be responsible for the majority of deaths
among children less than 5 years of age. Cryptosporidium infection in children
is also associated with malnutrition, persistent growth retardation, impaired
immune response and cognitive deficits.
Diagnosis:
Detection of Cryptosporidium in clinical pathology laboratories is based
mainly on microscopic detection by stains and/or fluorescent antibodies (IFA)
and other antigenic detection methods.
1- Acid-fast (AF)-modified Ziehl–Neelsen staining is one of the most common
differential staining techniques used for detection of Cryptosporidium. Three
separate faecal samples should be examined for immunocompetent patients and
two samples for patients with AIDS for confident diagnosis of cryptosporidial
infections using acid-fast staining
2- IFA is superior to acid-fast modified Ziel-Neelson staining method for
detection of cryptosporidium, but it is more expensive than acid-fast staining
and requires a fluorescence microscope and well-trained staff. Three separate
faecal samples should be examined for immunocompetent patients and two

Cryptosporidium
6
6
samples for patients with AIDS for confident diagnosis of cryptosporidial
infection by this method.
3- Other detection techniques that depends on antigen detection as enzyme-
linked immunosorbent assays (ELISAs), enzyme immunoassays (EIAs) and
immunochromatographic assay for Cryptosporidium are also available and have
the advantage of reducing assay times with disadvantage of variable diagnostic
sensitivities.
Major limitation of both conventional microscopy and antigen detection
methods is that they cannot identify to species or subtype level, which is
essential for understanding transmission dynamics and outbreaks, in particular
for zoonotic species.
4- Serology for detection of anti-cryptosporidium antibodies as IgG and IgM
antibodies may be used, however these antibodies may stay for long time in the
circulation. A finding of sero-conversion from negative to positive or titter
rising in two successive tests reflects active infection.
5- PCR as Real-time or quantitative PCR (qPCR) or multiplex PCR assays have
been developed to quantitate the numbers of Cryptosporidium oocysts present
in human and animal faecal and water samples with 100% specificity and
sensitivities as low as 200 oocysts per gram of faeces.
Treatment:
Nitazoxanide is licensed for children and adults. It can be prescribed for all
patients ≥ 1 year of age.
Prevention of cryptosporidiosis:
1. Wash hands thoroughly with soap and warm water: before preparing and
eating food, after handling raw food, after going to the toilet or changing
a baby’s nappy, after working, feeding, or playing with pets and other
animals.
2. Do not drink untreated water and always wash fruits and vegetables
before eating them.
3. Take care of toilets hygiene.

Cryptosporidium
7
7
4. Do not allow patients who have had cryptosporidiosis to go swimming at
least two weeks after being free from diarrhoea.