Family Neissericeae
The family Neisseriaceae includes the generaNeisseria
Kingella
Eikenella
Simonsiella
Alysiella
and several unnamed species.
morphology
Members of the genus Neisseria are coccal gram negative organisms that are frequently occur in pairs called Diplococci with adjacent flat side give the coffee bean appearance it is approximately 0.8 μm in diameter non –motile and do not form spores.culture
• These organisms and most species grow optimally at 35 to 37 C. In 48 hours on enriched media• the pathogenic spp form convex, glistening, elevated, mucoid colonies 1–5 mm in diameter transparent or opaque, non-pigmented, and non-hemolytic.
• The organism are aerobic and grow well in the presence of 5 % CO2 (Capnophilic) and grow best in moist environment.
• The oxidase test is a key test for identifying them.
Species of genus Neisseria
Non pathogenic
Neisseria cinerea
Neisseria flavescens
Neisseria lactamica
Neisseria mucosa
Neisseria ploysaccharea
•
Pathogenic Species
The genus includes
N. gonorrhoeae ( also called gonococcus (GC))
(N. meningitides ( also called meningococcus
Neisseria gonorrhoea
Virulence factors :Lipooligosaccharide (LOS): is a major in vivo virulence factor that mediates damage to body tissues and elicits inflammatory response.
Pili: pili is important in the initial attachment of the mo to the mucosal surfacesinhibit phagocytosis of the mo and helps in the exchange of the genetic materials between the cells.
Outer membrane proteins:
Por I proteins (-PorA/PorB): the major outer membrane porin protein form channels for nutrients to pass into and waste product to exit the cell it also influence the intracellular killing of the mo by PMN.Protein II (Opa for opacity) a group of protein that facilitate adherence to phagocytic and epithelial cells.
Protein III (reduction modified protein [RMP]) blocks the host serum bactericidial (IgG) action against the organism.
Iron repressible proteins: these are produced under condition of iron starvation or anaerobiosis.
IgA1 proteases which hydrolyze the IgA1 but not IgA2 at the hinge region.
Plasmid : plasmid born virulence of N gonorrhoea is mainly associated with antimicrobial resistance.
Clinical infections:
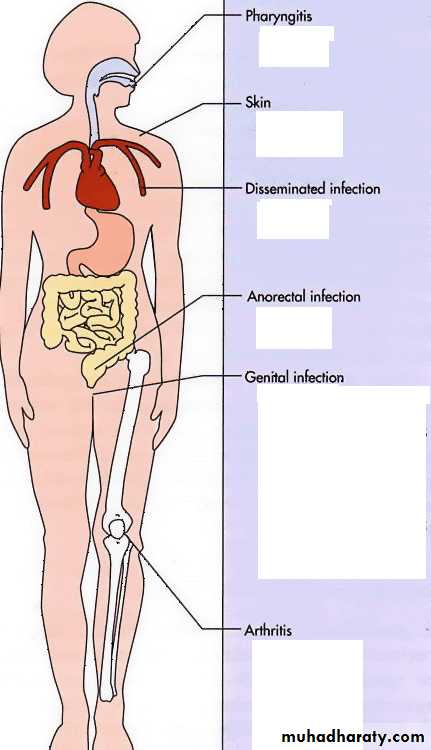
Oropharngeal
anorectalAcute urethritis in male
Cervicitis in female
purulent arthritis
Diagnosis
Specimens collectionSmears: gram stain of urethral or endocervical swabs reveal many diplococci inside the pus cells.
Culture: A variety of enriched culture media used for e.g modified Thayer Martin The culture is incubated 3-7 % CO2 at moist 35-37C for 24-72hr.
oxidase test (positive) and sugar utilization test.
Immunological assay:
a. monoclonal Ab coagulation (antigonococcal Ab).
b. direct fluorescent Ab .
c. Gongen II test anti-por monoclonal Ab.
Nucleic acid assays: nucleic acid probe and PCR.
Treatment
Currently recommended antimicrobial agents are ceftriaxone, cefixime, ciprofloxacin, or oflaxacin.
Neisseriameningitides
Virulence factorCapsule polysaccharide: The capsule renders the mo resistant to phagocytosis and enhances organism survival during bloodstream and CNS invasion. There are 13 different capsular poly saccharide most important are A, B, C, Y and W-135.
Pili : pili mediate attachment of mo to the epithelia lining of the nasopharynx.
Outer membrane protein.
Por Aand PorB
Opa and Opc protein: class 5 OPa protein are found in the outer membrane of NM. It facilitate adherence to different cell. Opc function in mucosal adherence and invasion of endothelial cells.
Cont…
Iron binding protein same as GC.LOS same as GC.
IgA protease same as GC.
Plasmids: are uncommon in NM. However beta lactamases encoding plasmids from GC can be transferred to NM.
Clinical infection
Humans are the only natural hosts for whom meningo-cocci are pathogenic.The nasopharynx bloodstream
the symptoms may be like those of an upper respiratory tract infection.
Fulminant meningococcemia is more severe, with high fever and hemorrhagic rash
there may be disseminated intravascular coagulation and circulatory collapse (Waterhouse-Friderichsen syndrome).
Meningitis is the most common complication of meningococcemia.
Diagnosis
Specimens include CSF, blood, nasopharngeal swab and rarely urogenital specimens. Incubated under CO2 (same as GC)
Gram stain of cytocentrifuged CSF ( intracellular gram negative diplococci) .
Culture on selective and non-selective media (SBA or CHOC).
oxidase , catalase and CHO fermentation.
Latex agglutination to detect group specific surface Ag of NM. They do not replace gram stain or culture.
Molecular methods: available but none present commercially
Treatment
The DOC for treatment of NM meningitis is penicillin., but rifampicin or sulfonamide recommended as prophylaxis for close contact. Patient with meningococcemia is best treated with 3rd generation cephalosporins.Meningococcal Vaccine
The new meningococcal vaccine like previous quarivalent vaccine , contain polysaccharide antigens to serogroups A, C, Y, and W-135 conjugated to diphtheria toxoid protein , this conjugate vaccine is expected to provide long term immunity.This vaccine does not protect caused by group B , because group B polysaccharide is very poor immunogen in human.
It is recommended to be given to students 11-12 years of age, those entering high school, military recruits, asplenic patients, traveler to area of epidemics, and Lab personnel.
Moraxella catarrhalis
Gram negative diplococcic commensal of the URT (nasopharynx).It causes otitis media and sinusitis upper & lower respiratory infection.
catalase +ve, oxidase+ve and differentiated from Neisseria that it does not utilize sugars .