Urinary stone disease II
Dr Ammar Fadil
1

Treatment of renal stone
•
Treatment for patients with calculi are
commonly organized by stone size
1.
Conservative therapy
2.
ESWL
3.
PCNL
4.
RIRS
5.
Open surgery
2

Classification
Stones may be classified according to
size,
Location,
X-ray appearance,
shape &
composition
• Stone location
– Calyceal : upper, middle or lower calyx;
– renal pelvis
3
A.F

1. Conservative treatment
Calculi 5mm and less are likely to pass
spontaneously.
A. increase in fluid intake to achieve a
daily urine output of 2 liters
B. Dissolution agents
4

Dissolution agents
• Uric acid stones are suitable for dissolution
therapy.
A.
Oral alkalinizing agents
alkalinize the urine to pH 6.5
–7 include
sodium bicarbonate 650 mg 3 or 4 times/d
potassium citrate 30
–60 meq/day, equivalent
to 15
–30 ML 3 or 4 times daily.
B.
allopurinol
300
–600 mg/day (inhibits conversion of hypoxanthine
and xanthine to uric acid)
5

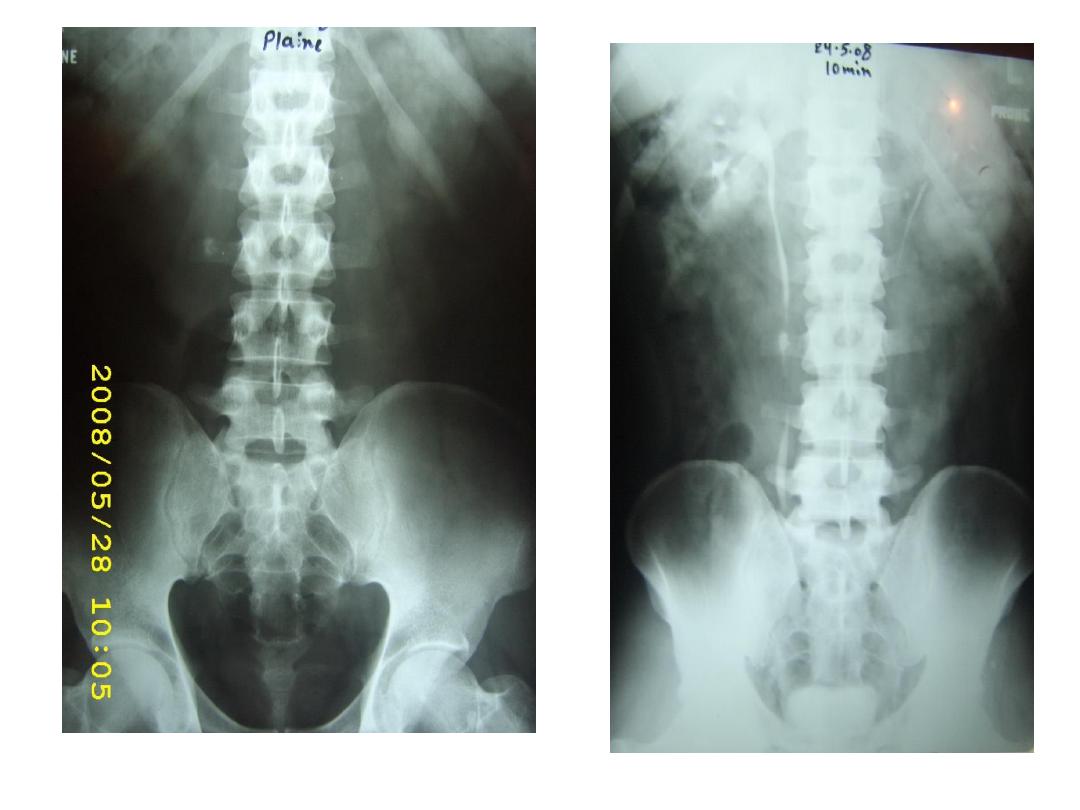
2. Extracorporeal shock wave lithotripsy
“ESWL
”
• ESWL
– It is used for renal and ureteric stone
– Regarding renal stone is used for
stone size
≤ 20 mm
6
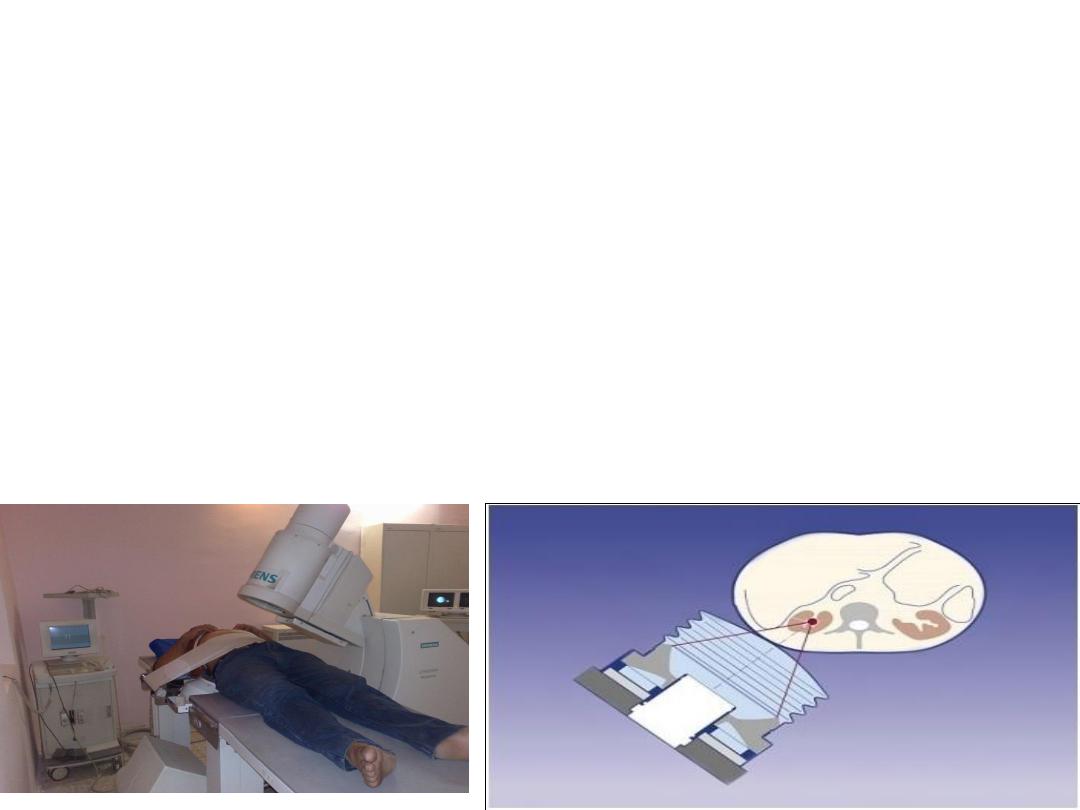
principles
• ESWL
It’s acoustic shock waves
are generated by a source external to the
patient's body and are then propagated into
the body and focused on a kidney stone.
Underwater shock waves are generated by a spark
gap electrical discharge contained within a Faraday
cage.
7
ESWL
8

Contraindications
Absolute:
1) pregnancy
2) uncontrolled coagulation
relative
1.obstruction distal to stone
2. cardiac pacemaker
– cardiologist should present.
3. AAA
4. severe orthopedic deformities
5. serum creatinine > 3 mg/dl
9
Complications
1
.
Hematuria
100% (disappears within 24 hr)
2.
Renal hemorrhage
perinephric, subcapsular,
intraparenchymal
3.
Infection
many calculi contain bacteria which are
released when the stone is broken. It is
wise to give ABS
.
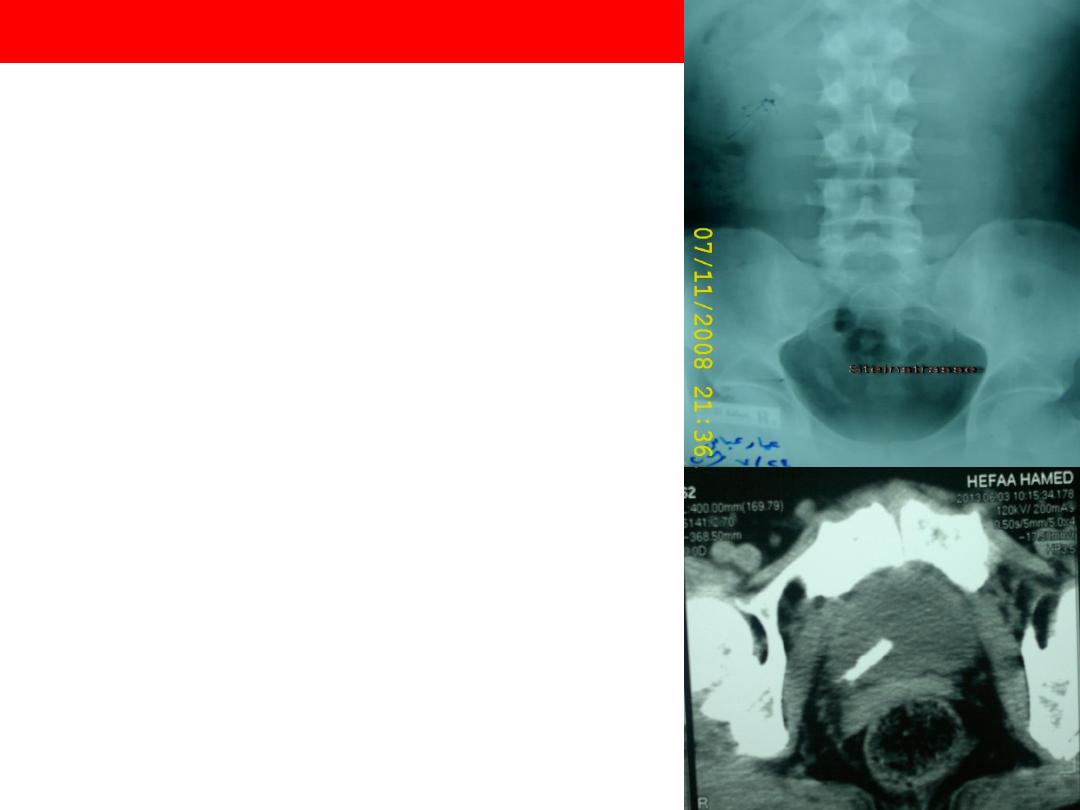
4.
Steinstrasse (SS)
(German “street of stone”) 5%
10

• to avoid this (SS),
double J stent should be
placed in the ureter so that
the kidney can drain while
the pieces of stone pass.
• JJ indication in ESWL
–
stone > 2 cm
–
Single kidney with stone
11

ESWL

3. PCNL
PCNL is the removal of a kidney stone via a
track developed between the surface of the
skin and the collecting system of the kidney
is recommended for stones >2 cm in
diameter
failed ESWL.
It is the first-line option for staghorn calculi
13
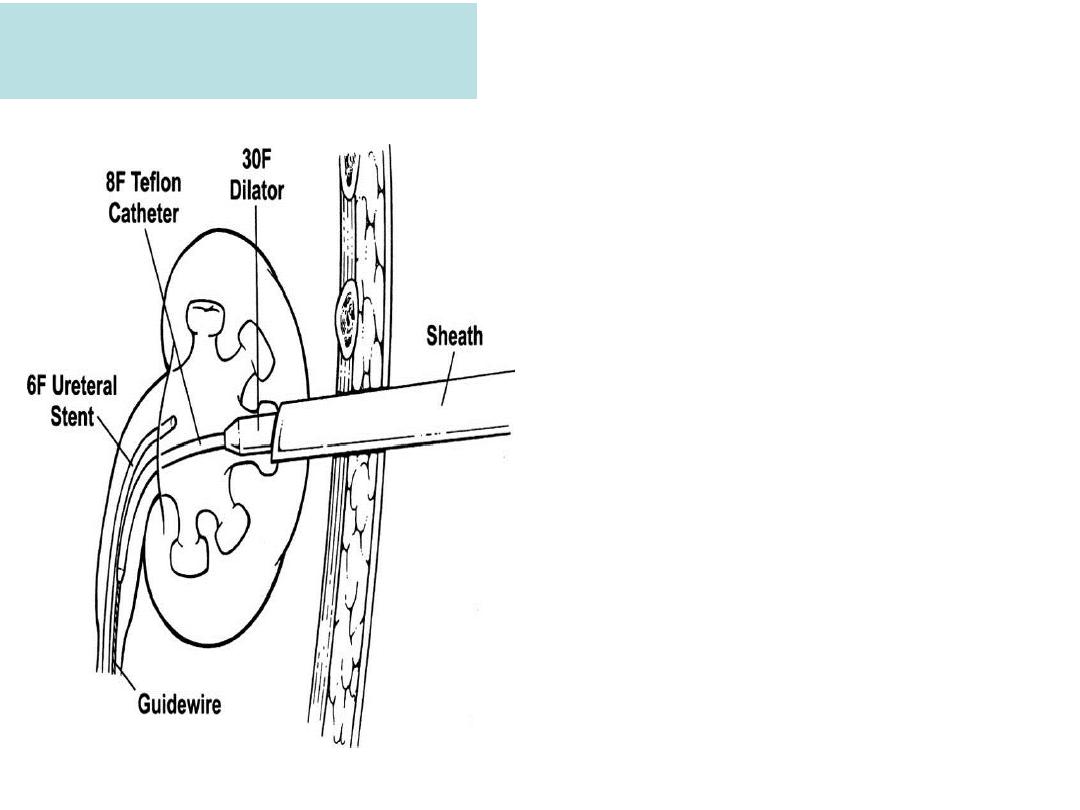
PCNL
This involves the
placement of a hollow
needle into the
collecting system
through the loin and the
renal parenchyma
A wire inserted through the
needle is used to guide
the passage of series of
dilators which expand the
track
14
PCNL
• the nephroscope used to look for the
stone.
• stones must be fragmented by
Lithoclast (pneumatic) lithotriptor
Ultrasounic lithotripsy
laser
15
Intracorporeal techniques of
stone
fragmentation (fragmentation within the body)
A. Pneumatic (ballistic)
lithotripsy
A metal projectile is propelled
backwardand forward at great
speed by bursts of compressed
air.
This technique is used for stone
fragmentation in the
ureter and
kidney
16

B. Ultrasonic lithotripsy
The ultrasound energy is transmitted to a hollow metal
probe, which in turn is applied to the stone
this causes it to break into small fragments,
uses include fragmentation of
renal calculi during
PCNL
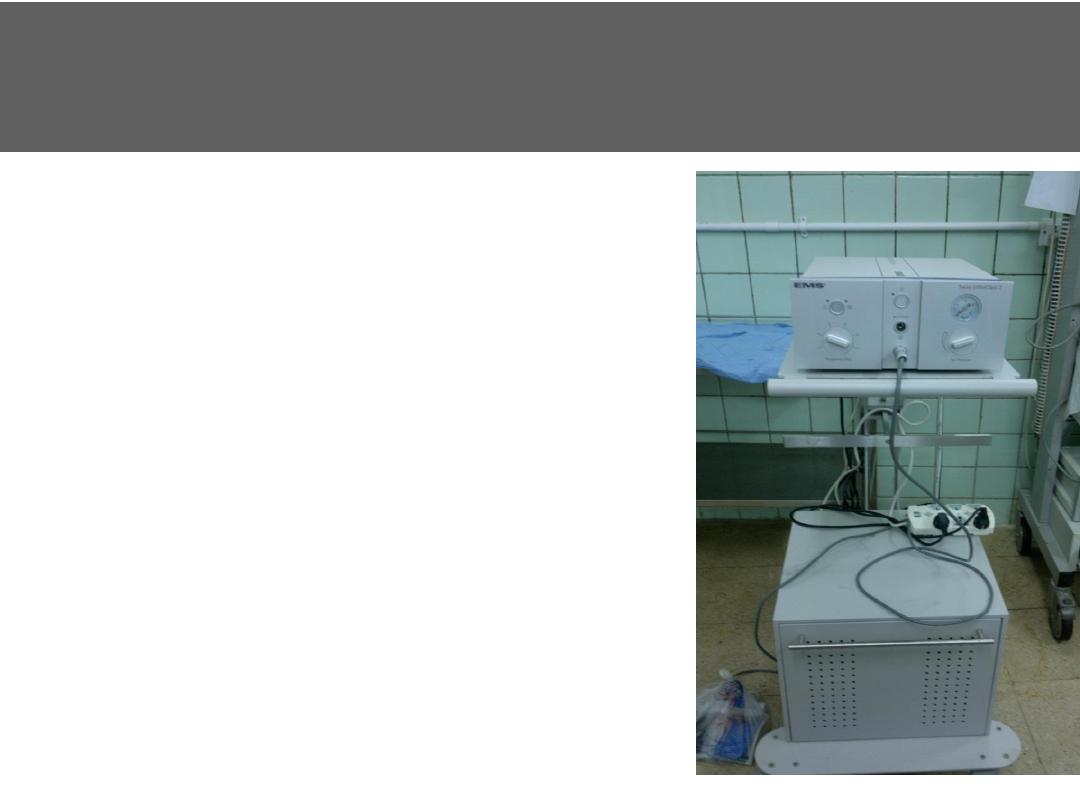
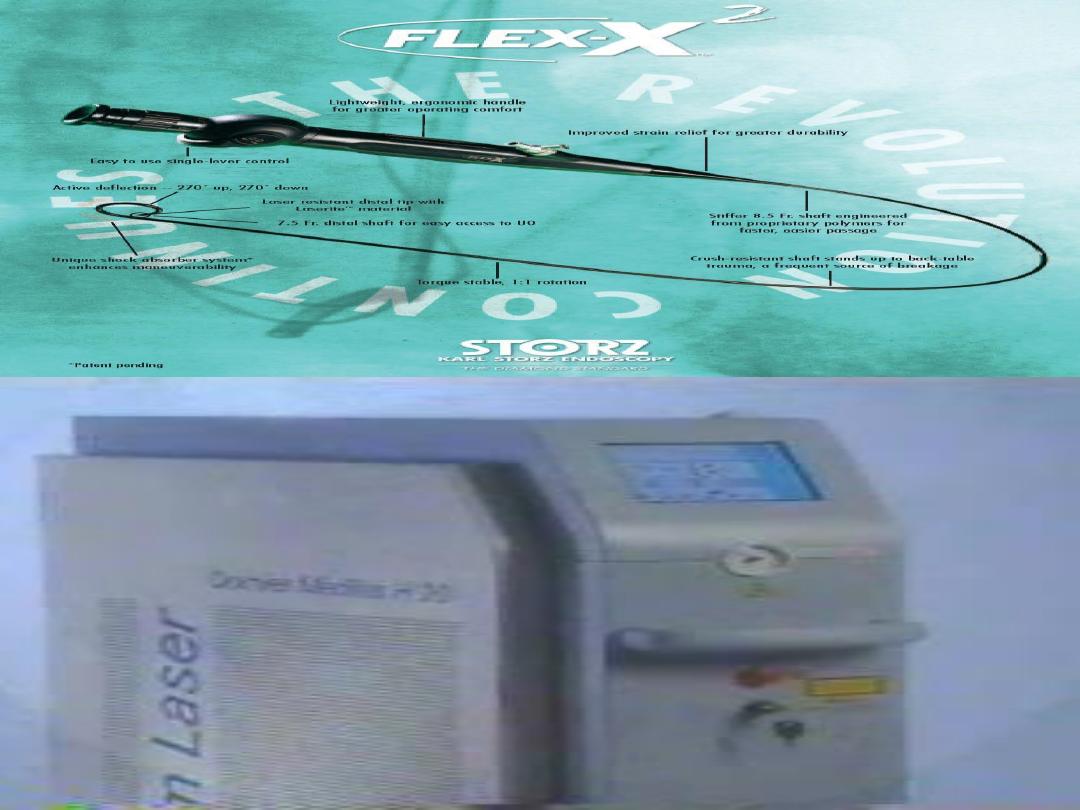
C. Laser lithotripsy
The holmium:YAG laser is principally a
photothermal mechanism of action, causing
stone vaporization
Principal uses are for
ureteric stones & small
renal stones
17

4. RIRS
• RIRS retrograde intrarenal surgery
• Using flexible Ureterorenoscopy and using
LASER for stone fragmentation
It is most suited to stones <2 cm in diameter
Cons
expensive equipment
18

INDICATIONS:
Complex stone burden (projection of stone
into multiple calyces)
Failure of endoscopic treatment (technical
difficulty gaining access to the kidney)
Body habitus that precludes endoscopic surgery
e.g., gross obesity, Kyphoscoliosis
Non functioning kidney
If the kidney is non functioning, the simplest way
of removing the stone is to remove the kidney.
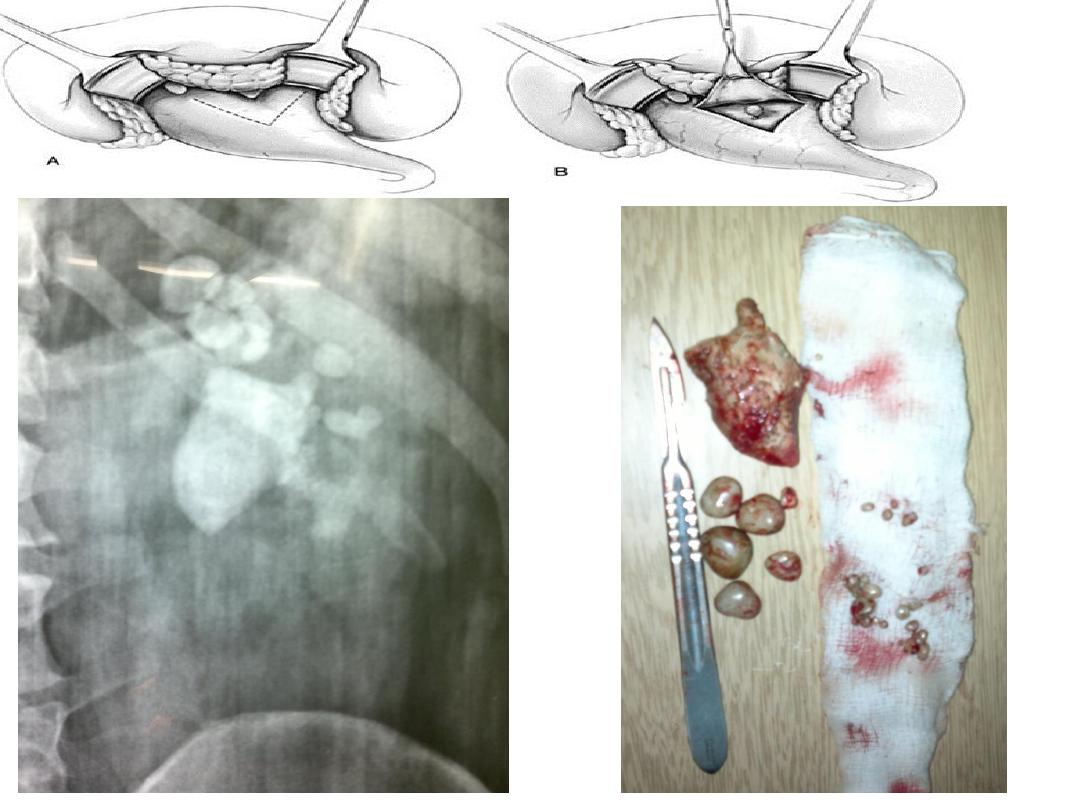
5. Open surgery
20

Open surgery
Operations for kidney stone are usually
performed via a loin approach
.
A. Pyelolithotomy for renal pelvic stone.
21
22
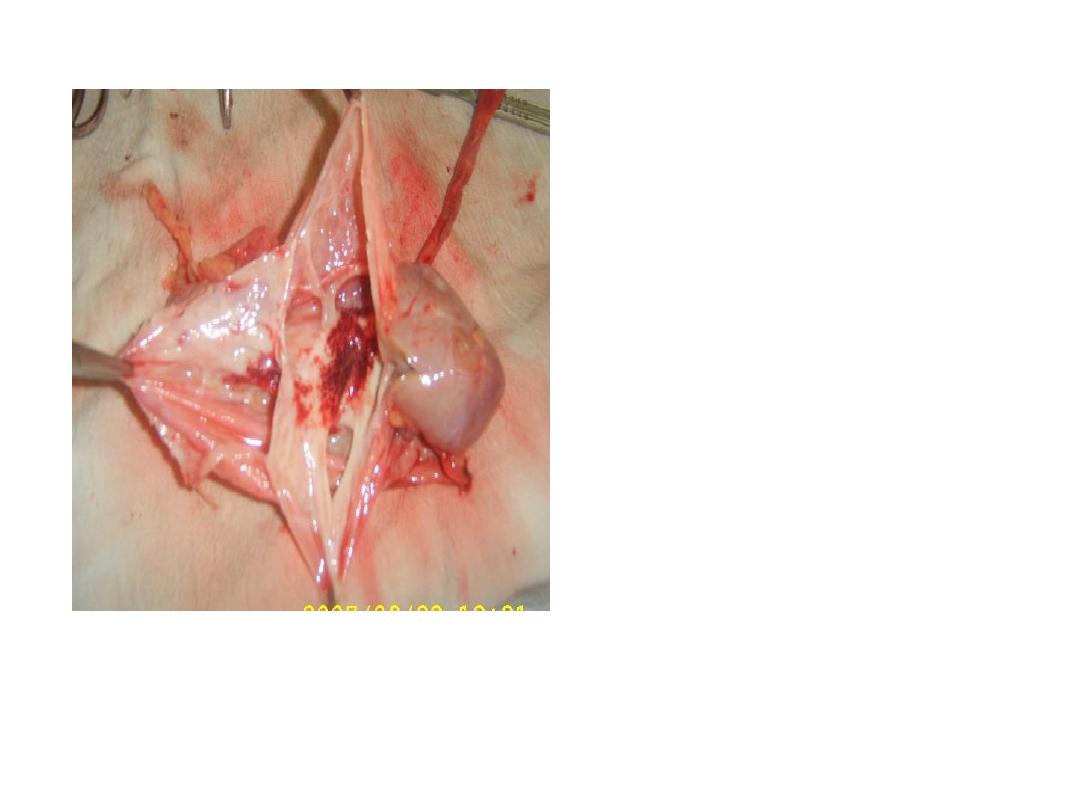
B
. Nephrectomy
is
indicated when the
kidney has been
destroyed by
obstruction and
infection associated
with stone disease.
23

Treatment of bilateral renal stones
• Usually the kidney with better function is
treated first.
• the more painful one.
24

Ureteric calculus
Ureteral stones
•
originate in the kidney
•
become
obstructed during passage through the ureter
.
•
Most are single small stones pass spontaneously
•
some stones are too large to pass and lodge in the
ureter.
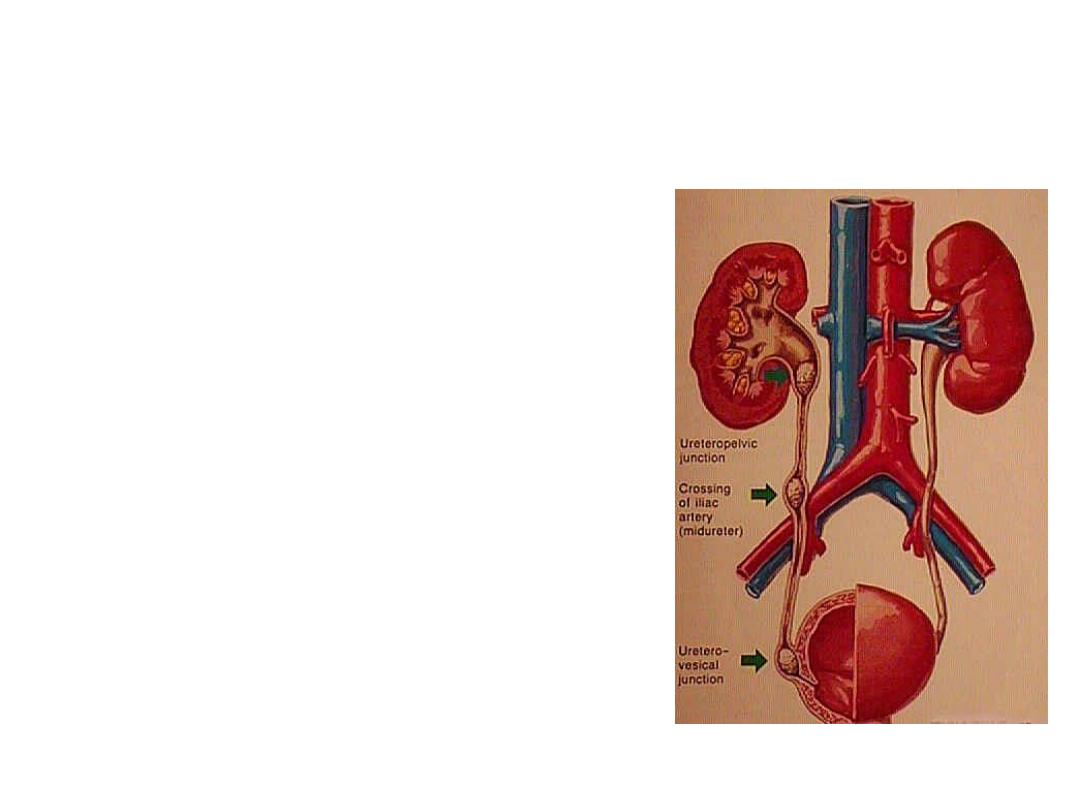
25
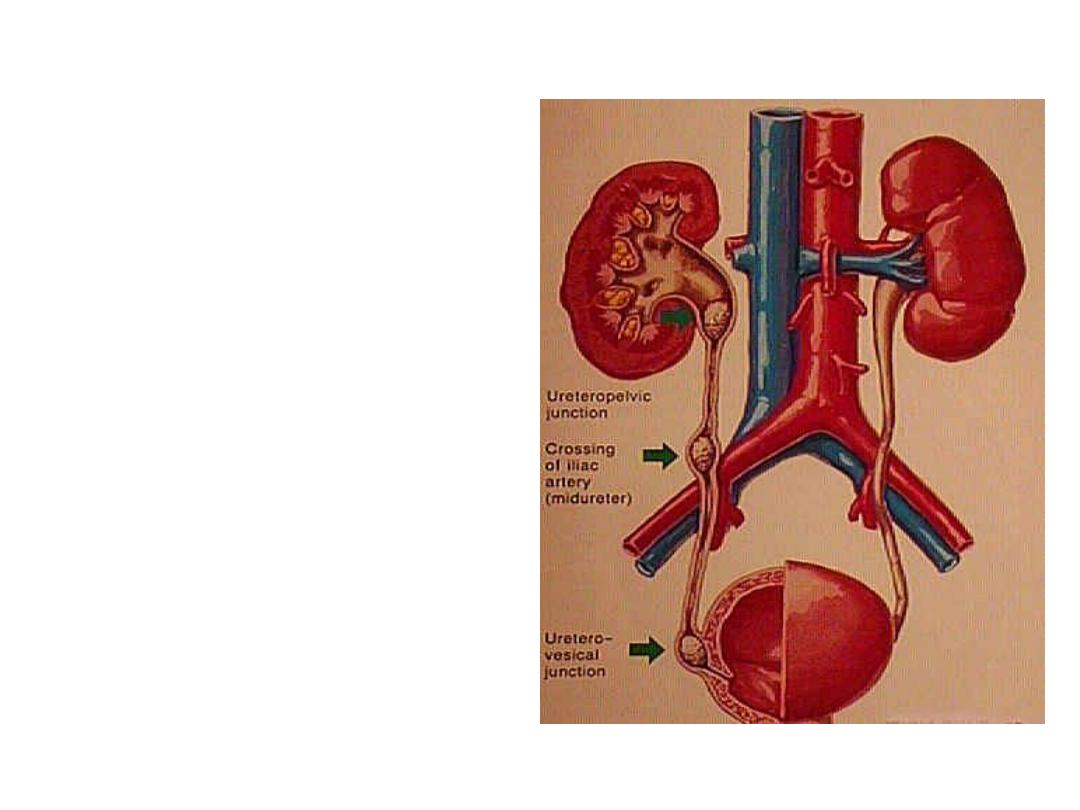
the narrowest parts of the
ureteral lumen and the
locations of most
impacted ureteral stones
are
o
UPJ,
o
crossing of the ureter
over the iliac vessels
o
UVJ
26

C/F
Patients with ureteric colic most commonly present
with
sudden onset pain passing from loin to groin is
colicky in nature.
As stone progress to the
lower ureter
pain are referred
more to the groin, external genitalia and the anterior
surface of the thigh.
The patient cannot get comfortable, and tries to move in
an attempt to relieve the pain.
is frequently associated with nausea & vomiting.
Pain is occur from obstruction or renal capsular
Distension
27
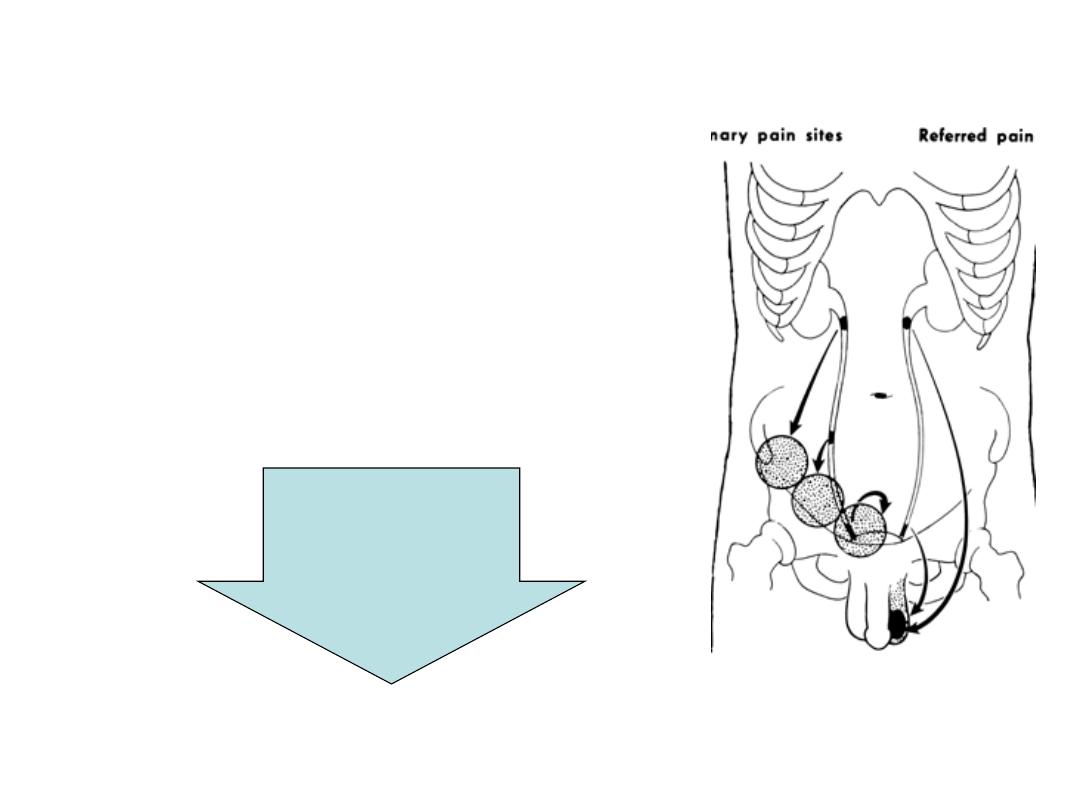
C/F
• Upper ureteric stone: loin pain
radiating to testis
• Mid ureteral loin pain radiating
to iliac fossa
• Lower ureteral loin pain radiating
into bladder, vulva or scrotum.
Frequency
Strong desire to
pass urine
Discomfort on tip
of penis , or
urethra in female
Pathognomonic
of UVJ stone
28

C/F
There is often microscopic or gross hematuria owing
to the abrasive effect of the stone on the urothelium.
Patients with stones may also present with infection
that is complicated by the ureteral obstruction,
resulting in dysuria, fever, leukocytosis, & sepsis.
29

D.D
• Musculoskeletal pain (L1 nerve root irritation, L1
Herpes zoster
• pyelonephritis (fever, chills, pyuria)
• appendicitis
• acute abdomen (leaking abdominal aortic
aneurysm
Rt. Ureteric colic Vs AA (clinically)
The presence of hematuria
although doesn’t rule out appendicitis, because an inflamed
appendix lying near the ureter can give rise to hematuria
pt is usually in greater pain and less systemically ill.
Renal tenderness
U/S show hydronephrosis suggesting presence of ureteric stone
CT scan
30

DX
O\E
renal angle tenderness as well as
tenderness in the ipsilateral lower abdomen
• Urinalysis
frequently shows microscopic hematuria
> 3 RBC \HPF
• Initial blood studies should include (BUN, serum
creatinine, calcium ) serum uric acid and
phosphorus
.
– Nonenhanced spiral computed tomography (CT)
OR
– U/S+KUB
31
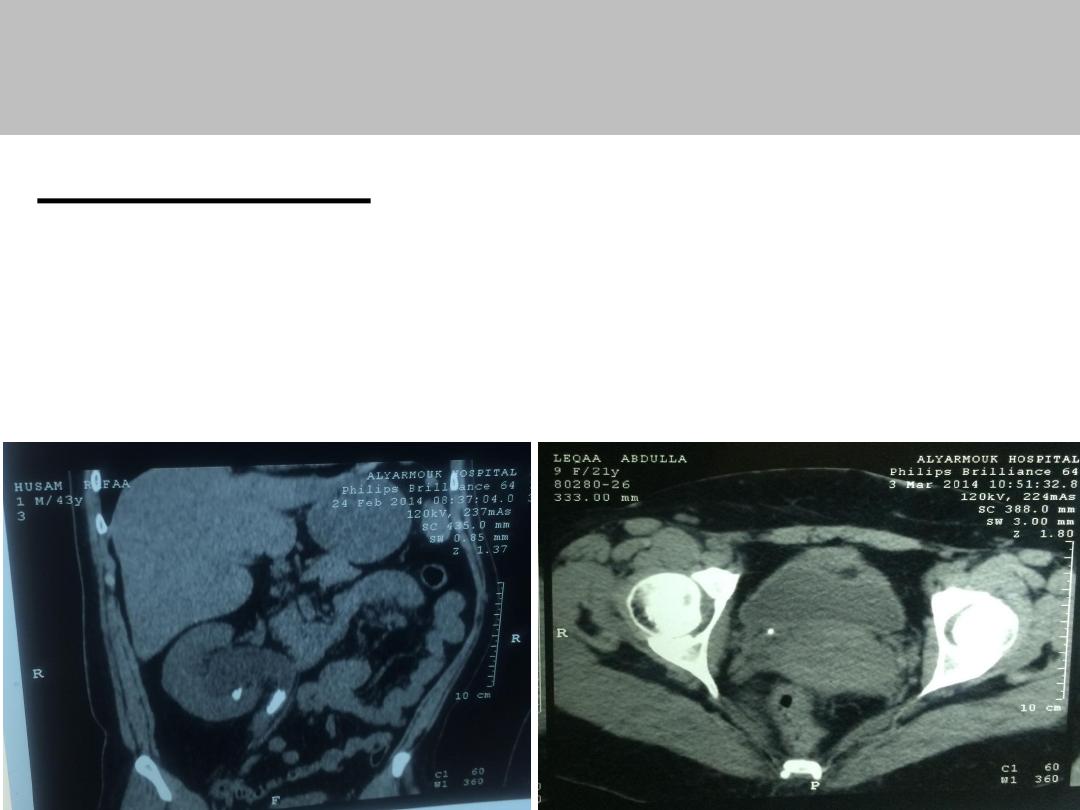
CT scan/ Renal colic
Non-enhanced (CT)
study of choice
has high sensitivity and specificity for calculi.
does not require bowel preparation or IV contrast
32
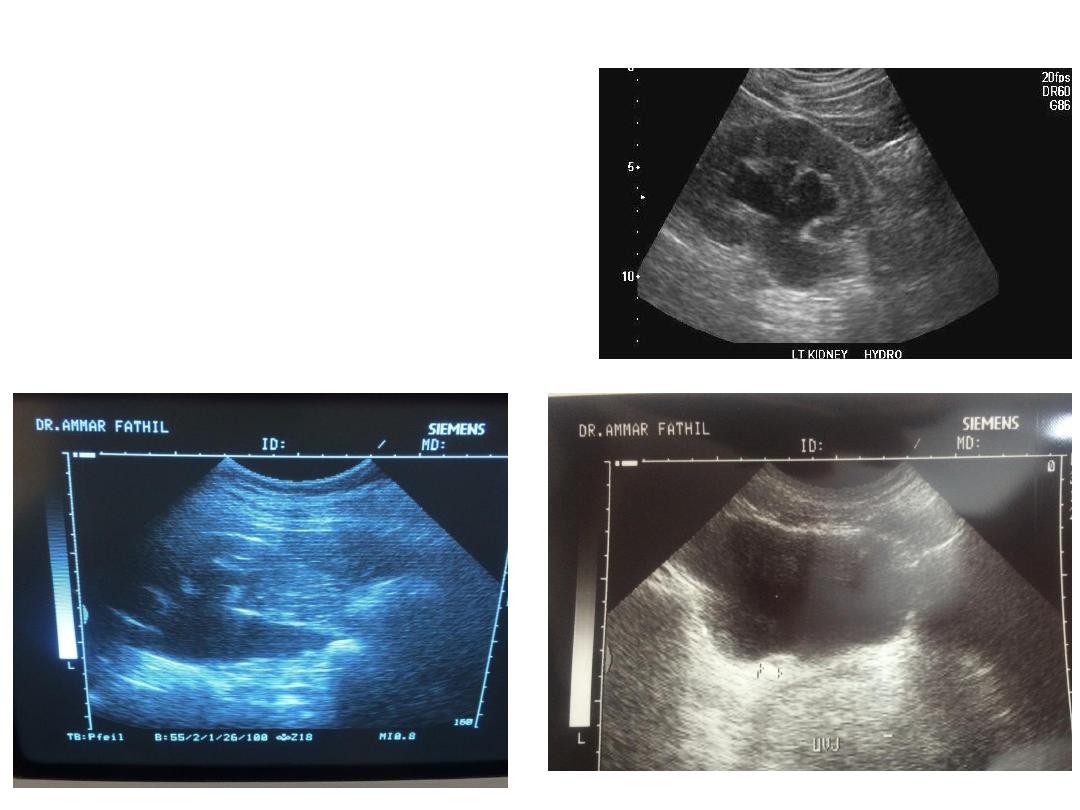
• US:
Hydronephrosis
or
ureteric stone can be
seen if its in
upper ureter or
near UVJ
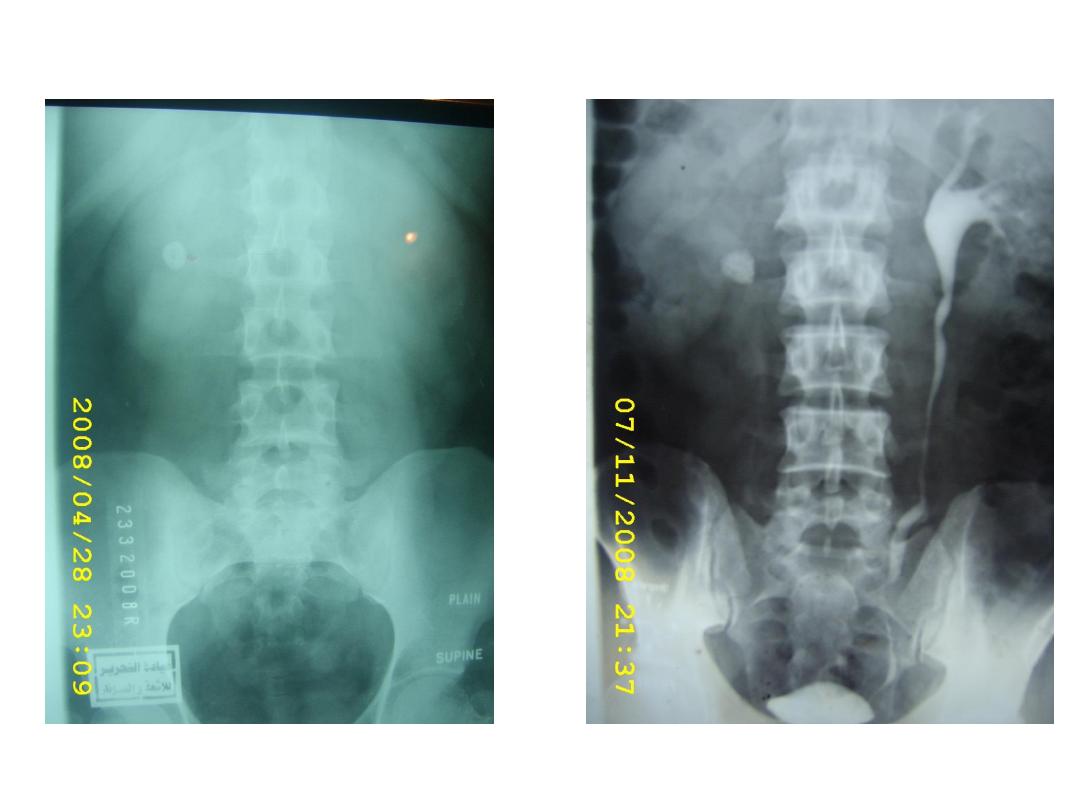
33
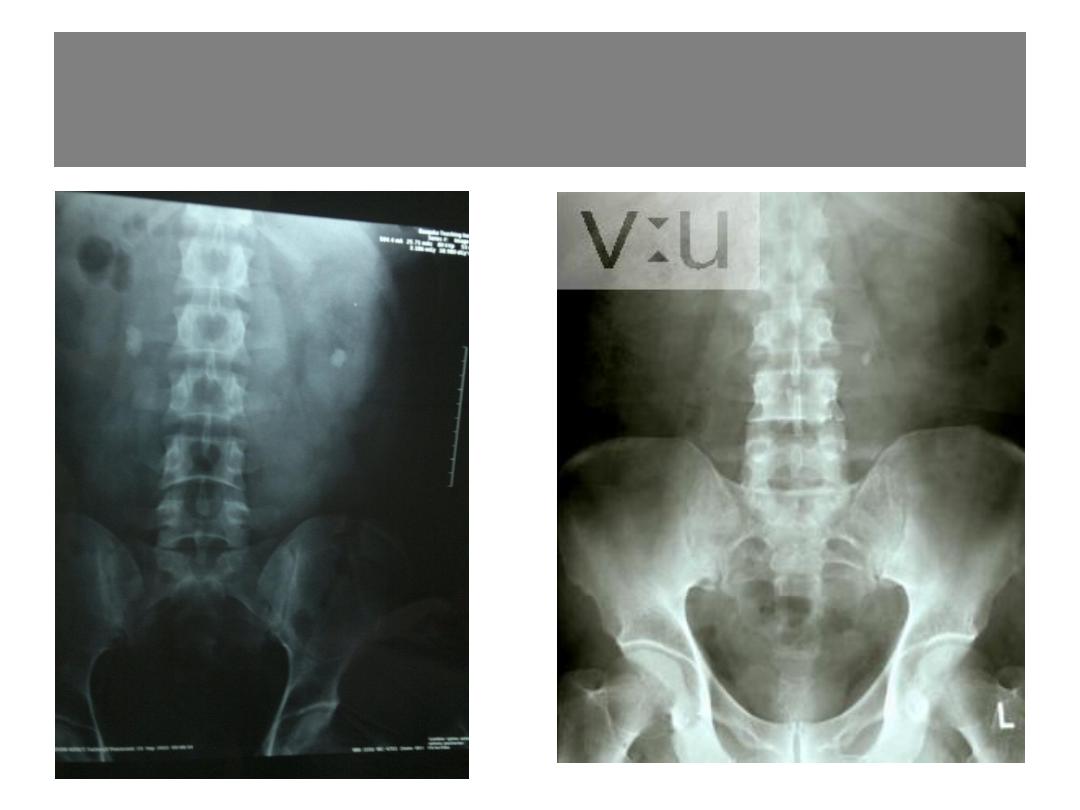
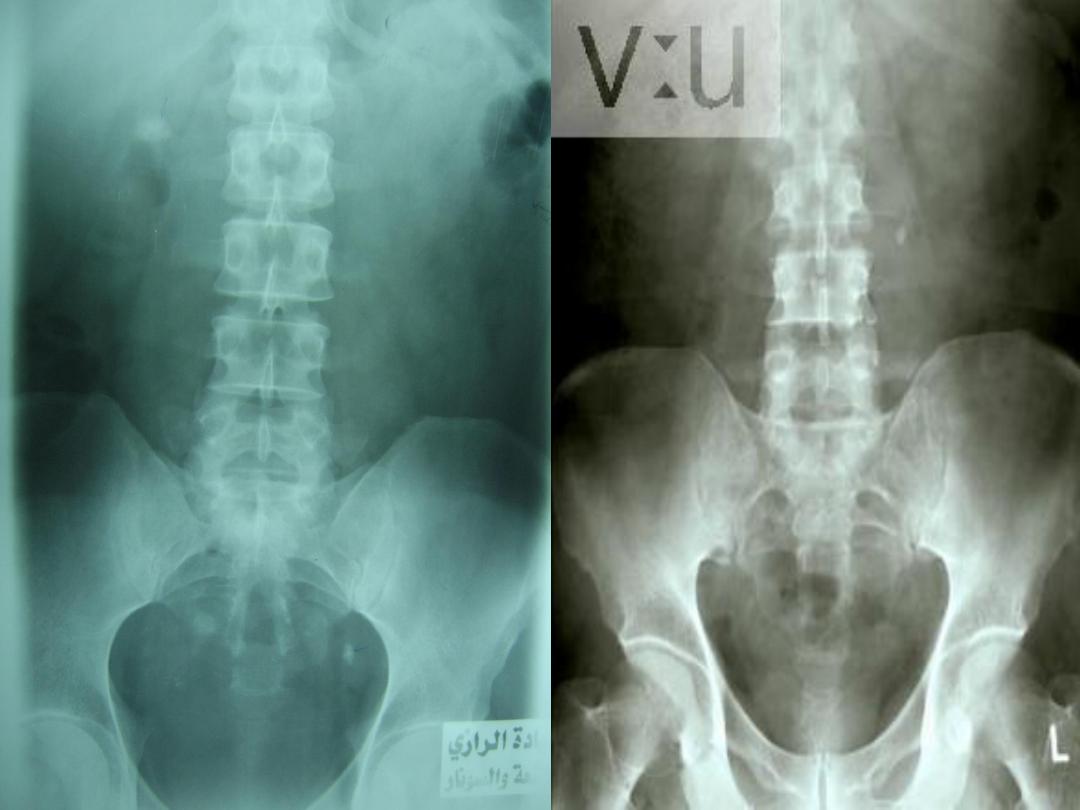
KUB
34

Initial treatment of ureteric colic
1. Pain relief
is the first therapeutic step in patients with an acute stone episode
.
Non-steroidal anti-inflammatory drugs (NSAIDs) e.g.,
.
diclofenac
—Voltaren IM 75 mg
have
better analgesic efficacy than opioids
.
Its analgesic effect is partly anti-infl ammatory &
partly by reducing ureteric peristalsis.
Opioids are associated with a high rate of vomiting
compared to NSAIDs
When NSAIDs are inadequate, opiate analgesics
such as tramal, pethedine or morphine are added
May be managed with antidiuretic desmopressin.
35

2. Prevention of recurrent renal colic
A. NSAID tablets or suppositories (e.g., diclofenac
sodium, 100-150 mg/day, 3-10 days) may help
reduce inflammation and risk of recurrent pain .
B. Daily α-blockers(
MET
) Tamsulosine 0.4 mg
There is no need to !!
encourage the patient to drink copious amounts of
fluids or to give them
large volumes
of fluids
intravenously in the hope that this will flush out the
stone.
36

Renal blood flow and urine output from the
affected kidney fall during an episode of acute,
partial obstruction due to a stone
• MIS PRACTICE
– I.V fluid unless pt has repeated vomiting
Initial treatment of colic
37

• The ureter can be
divided into
o
upper third from the UPJ
to
the upper edge of the
sacrum
;
o
middle third from the
upper
to the lower edge of
the sacrum;
o
lower third from the lower
edge of the sacrum to the
VUJ
38

Modalities of treatment of ureteric stone
Expectant therapy
ESWL
Ureteroscopy
Open surgery (ureterolithotomy)
39
1.Expectant therapy
conservative measures are recommended depending
on the clinical circumstance
stones pass spontaneously do so 4-6
weeks
80% will pass the stone spontaneously
stones under 6 mm considered for
observation
Stones located more distally typically pass more
readily than those located in the mid or upper
ureter.
NSAID + MET
High fluid intake
(>7mm) typically do not pass
40

Indications for interventions
pain refractory to analgesics
obstruction with infection
Impaired renal function (solitary kidney
obstructed by a stone, bilateral ureteric stones
lack of stone progression
Large stone unlikely to pass
pt preferance
41

2.ESWL
• is more efficient for stones <1 cm in
diameter than for those >1 cm in size
– ESWL: in situ;
– after push-back into the kidney (JJ stent
insertion
42
43

44
Push bang (back)
a stone that is lying in
the upper part of the
ureter can often be
flushed back into the
kidney by a JJ-stent.
The patient can then be
treated by ESWL
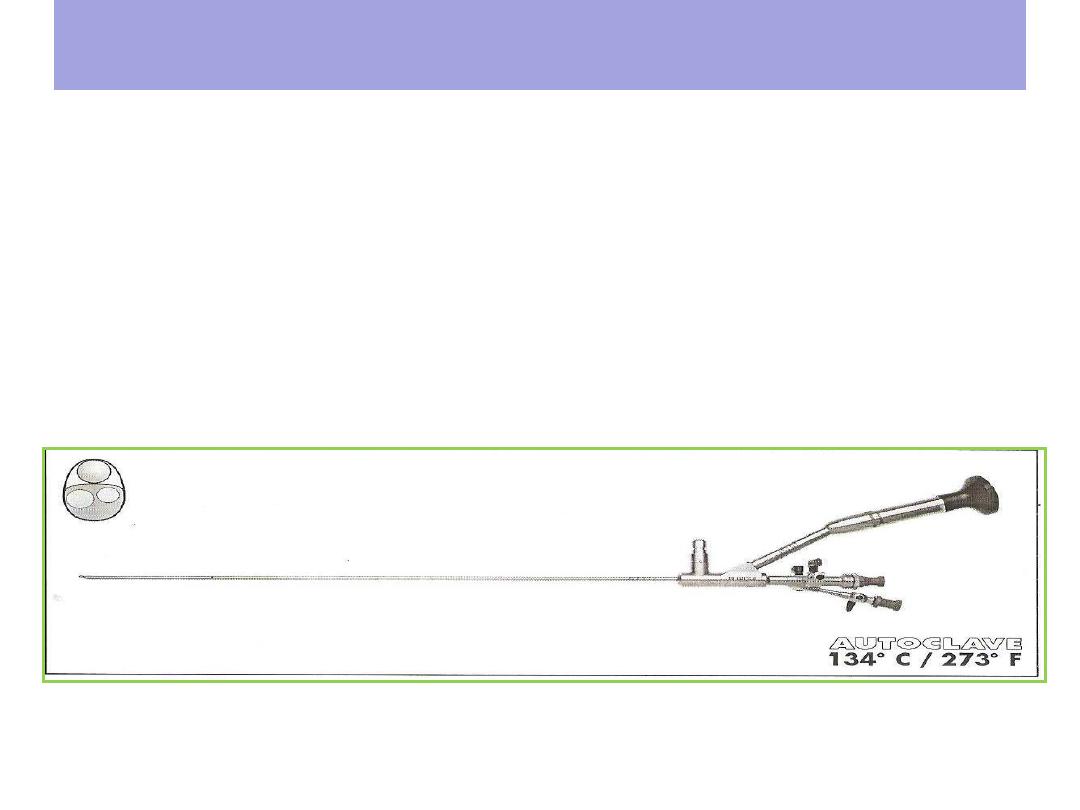
3.Endoscopy
Ureteroscopy & intracorporeal lithotripsy
A ureteroscope is a long endoscope which can be
passed transurethrally across the bladder into the
ureter .Stones are fragmented using an laser
lithotriptor or lithoclast
45

Recommendations
Upper ureteric stones
- <1 cm diameter: ESWL (in situ, push-back)
- >1 cm diameter: ureteroscopy, ESWL
Mid ureteric stone URS
Lower ureteric stones
-
ESWL and ureteroscopy are acceptable options
46

4.Open Ureterolithotomy
Open ureterolithotomy is used
when ESWL or ureteroscopy have been tried
and failed or were not feasible.
Calculi in the upper third of the ureter are approached through a loin
incision as used for a stone in the renal pelvis.
midureteric stones is through a muscle-cutting iliac fossa incision;
lower ureteric stones are best reached through a Pfannenstiel incision
.
47
Prevention
– 50% of individuals experiencing recurrent another
stone with in 10 years of the first occurrence
– One mainstay of conservative management is the
forced increase in fluid intake to achieve a daily
urine output of 2 liters
– moderate animal protein (meat) intake
– sodium restriction
– Dietary calcium avoidance actually increases stone
recurrence risk.
48

Fluid recommendation
– Patients should be strongly encouraged to
consume enough fluids to produce 2 liters of
urine per day.
– Soda flavored with phosphoric acid may increase
stone risk, whereas soda with citric acid may
decrease risk.
– Citrus juices (particularly lemon juice) may be
a useful adjunct to stone prevention.
49

Pharmacological treatment
Recurrent Calcium stone
thiazide diuretic and / or potassium citrate
Recurrent Uric acid stone
Potassium citrate to raise urine PH & or Allopurinol
50
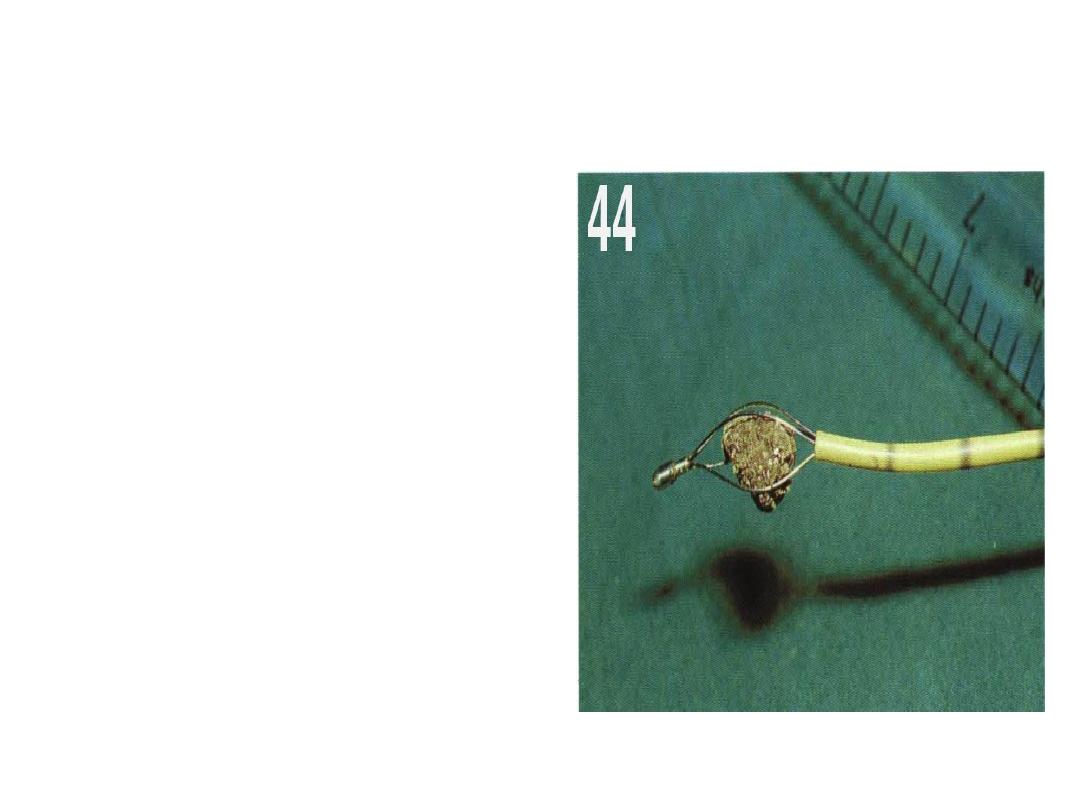
Dormia basket
• The use of wire
baskets used for
small stones that
are within 5 or 6
cm of the ureteric
orifice
51
Ureteric meatotomy
Stones often lodge in the
intramural part of the
ureter. endoscopic
incision using a
diathermy knife can
enlarge the opening and
free the stone.
52