INFLAMMATORY BOWEL DISEASES
chronic inflammatory bowel diseases (Ulcerative colitis and Crohn's disease)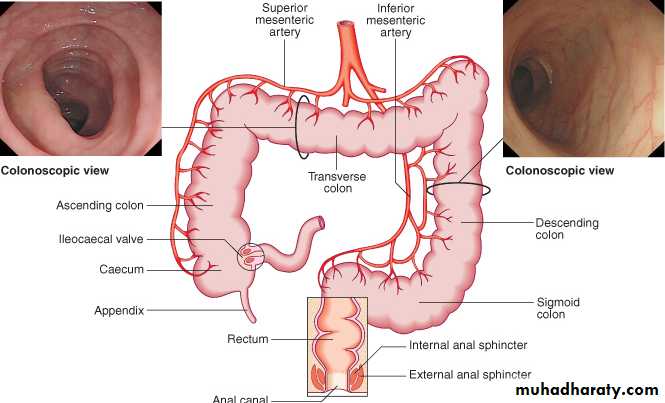
LARGE BOWEL
Characters:relapsing and remitting course.
The diseases have many similarities and it is sometimes impossible to differentiate between them.
ulcerative colitis only involves the colon, while Crohn's disease can involve any part of the gastrointestinal tract from mouth to anus.
Epidemiology
1. Crohn's disease appears to be very rare in the developing world but ulcerative colitis, is becoming more common.2. In the West, the prevalence of ulcerative colitis 100-200 per 100 000, while the prevalence of Crohn's disease is 50-100 per 100 000.
3. Both diseases most commonly start in young adults (20-40) years, with a second incidence peak in the seventh decade.
FACTORS ASSOCIATED WITH THE DEVELOPMENT OF IBD
Genetic factors1. More common in Ashkenazi Jews
2. 10% have a first-degree relative or at least one close relative with IBD
3. High concordance between identical twins
4. Association with autoimmune thyroiditis and SLE
5. Gene mutations on chromosome 16 and some time on chromosomes 12, 6 and 14.
6. HLA-DR association in severe ulcerative colitis
and with HLA-B27 and ankylosing spondylitis in both (UC and CD) commonly develop
Environmental
Ulcerative colitis-more common in non-smokers and ex-smokers
Crohn's-most patients are smokers
Associated with low-residue, high refined sugar diet
Appendicectomy protects against ulcerative colitis
PATHOLOGY
1. In both diseases the intestinal wall is infiltrated with acute and chronic inflammatory cells.
2. There are important differences in the distribution of disease and in histological features
SITE OF INVOLVEMENT
UC1. Inflammation is almost always involves and start from the rectum (proctitis).
2. It may spread proximally to involve the sigmoid colon (proctosigmoiditis)
3, and in a minority the whole colon is involved (pancolitis).
4. Inflammation is confluent and is more severe distally.
5. In long-standing pancolitis the bowel becomes shortened and 'pseudopolyps' develop which represent normal or hypertrophied residual mucosa within areas of atrophy
HISTOPATHOLOGY
the inflammatory process is limited to the mucosa (not involve the deeper layers) of the colon
Both acute and chronic inflammatory cells infiltrate the lamina propria and the crypts ('cryptitis').
Crypt abscesses are typical.
Goblet cells lose their mucus and in long-standing cases glands become distorted.
Dysplasia occurs and may lead to the development of colon cancer
NORMAL HISTOLOGY-COLON
UC PATHOLOGY
B. CD - PATHOLOGY
The sites most commonly involved, in order of frequency, are:
1. terminal ileum and right side of colon
2. colon alone
3. terminal ileum alone
4. ileum and jejunum
Fistulae may develop between adjacent loops of bowel or between affected segments of bowel and the bladder, uterus or vagina, and may appear in the perineum.
a. The changes are patchy and interrupted by islands of normal mucosa ('skip' lesion).
b. The mesenteric lymph nodes are enlarged and the mesentery thickened.
Histology:
1. chronic inflammation is seen through all the layers of the bowel wall, which is thickened as a result.2. focal aggregates of epithelioid histiocytes, which may be surrounded by lymphocytes and contain giant cells.
3. Lymphoid aggregates or microgranulomas are also seen, and when these are near to the surface of the mucosa they often ulcerate to form tiny aphthous-like ulcers.
CD GRANULOMA
CLINICAL FEATURES
UCThe major symptom is bloody diarrhoeaGENERAL FEATURES
1. The first attack is usually the most severe and thereafter the disease is followed by relapses and remissions.2. Only a minority of patients have chronic, unremitting symptoms.
3. Emotional stress, intercurrent infection, gastroenteritis, antibiotics or NSAID therapy may provoke a relapse.
4. The clinical features depend upon the site and activity of the disease
INVOLVES LARGE BOWEL ONLY
CLINICAL FEATURES ACCORDING TO SITE INVOLVED
1. Rectal involvement (Proctitis) causes:
rectal bleeding
mucus discharge
tenesmus.
Some patients pass frequent, small-volume fluid stools.
others are constipated and pass pellety stools.
Constitutional symptoms do not occur
2. Rectum and sigmoid (Proctosigmoiditis) cause
a. Bloody diarrhoea with mucus.
b. Almost all patients are constitutionally well but a small minority who have very active, limited disease develop fever, lethargy and abdominal discomfort
3. The whole colon Extensive colitis causes
a. bloody diarrhoea with passage of mucus. b. In severe cases anorexia, malaise, weight loss and abdominal pain occur, and the patient is toxic with fever, tachycardia and signs of peritoneal inflammation
CDThe major symptoms are abdominal pain, diarrhoea and weight loss
LARGE AND SMALL BOWEL
1. Ileal Crohn's disease (small bowel) causes
abdominal pain, principally because of subacute intestinal obstruction, but inflammatory mass, intra-abdominal abscess or acute obstruction may be responsible.Pain is often associated with diarrhoea which is watery and does not contain blood or mucus. 3. Weight lose almost always occur ( because eating provokes pain and also may be due to malabsorption).
Some patients present with features of fat, protein or vitamin deficiencies e. g. B12 due to malabsorption. B12 def. causes anaemia and neuropathy.
2. Crohn's colitis presents similar to ulcerative colitis.
Bloody diarrhoea.Passage of mucus.
Constitutional symptoms including lethargy, malaise, anorexia and weight loss.
Rectal sparing and the presence of perianal disease are features which favour a diagnosis of Crohn's disease rather than ulcerative colitis.
3. Many patients present with symptoms of both small bowel and colonic disease.
4. A few have isolated perianal disease, vomiting from jejunal strictures or severe oral ulceration5. Physical examination:
Evidence of weight loss.
Anaemia
Glossitis and angular stomatitis.
There is abdominal tenderness, most marked over the inflamed area.
An abdominal mass due to matted loops of thickened bowel or an intra-abdominal abscess may occur.
Perianal skin tags, fissures or fistulae are found in at least 50% of patients
COMPLICATION OF IBD
INTESTINAL COMPLICATIONS
Toxic megacolon (mainly in ulcerative colitis).
Intestinal perforation (small and large-in both).
Haemorrhage (in both but rare).
Fistulae (in Crohn’s disease).
Colonic cancer (in ulcerative colitis and to lesser extend in Crohn’s colitis).
Small bowel adenocarcinoma (in Crohn’s disease).
TOXIC MEGACOLON:
Is severe, life-threatening inflammation of the colon, occurs in both ulcerative colitis and Crohn's disease.
the colon dilates (toxic megacolon) and bacterial toxins pass freely across the diseased mucosa into the portal then systemic circulation.
This complication occurs most commonly during the first attack of colitis .
An abdominal X-ray should be taken daily because when the transverse colon is dilated to more than 6 cm there is a high risk of colonic perforation.
Perforation of the small intestine or colon: This can occur without the development of toxic megacolon
Life-threatening acute haemorrhage due to erosion of a major artery is a rare complication of both.
Fistulae : Fistulous connections between loops of affected bowel, or between bowel and bladder or vagina are specific complications of Crohn's disease and do not occur in ulcerative colitis.
increased risk of colon cancer in patients with extensive active colitis of more than 8 years' duration especially in UC.
Small bowel adenocarcinoma is a rare complication of long-standing small bowel Crohn's disease.
SYSTEMIC COMPLICATIONS OF IBD
Seronegative arthritis:a. Acute medium size joint involvement.
b. Sacroiliatis.
c. Ankylosing spondylitis.
2. Dermatological:
a. erythema nodosum.
b. Pyoderma gangrenosum.
c. oral aphthous ulcers.
3. Ocular complications:
a. Conjunctivitis.
b. iritis.
c. episcleritis.
4. Hepatic and billiary:
a. Primary sclerosing choliangitis (UC).
b. Gall stone.
c. Autoimmune hepatitis.
d. fatty liver.
e. Portal pyaemia and liver abscess.
5. Renal complications:
a. Oxalate calculi (Crohn’s).
b. Amyloidosis.
c. Ureteric obstruction (Crohn’s).
6. Vascular:
a. DVT
b. Portal or mesenteric vein thrombosis.
FOLLOW UP
surveillance colonoscopy programmes
Patients with long-standing (8-10 years)
extensive colitis (total) .
Multiple random biopsies are taken every 10 cm throughout the colon and additional biopsies are taken from raised or ulcerated areas.
Mild dysplesia: Do colonoscopy every 1-2 years.
If high dysplesia: Do proctocolonectomy.
MICROSCOPIC COLITIS
Some patients experience watery diarrhoea as a consequence of microscopic ('lymphocytic') colitis. The colonoscopic appearances are normal but histological examination of biopsies shows a range of abnormalities.
Collagenous colitis
Is a type of microscopic colitis, characterised by the presence of a thick submucosal band of collagen; a chronic inflammatory infiltrate is usually seen. The disease is more common in women and is associated with rheumatoid arthritis, diabetes and coeliac disease. Patients have a history of intermittent watery diarrhoea and treatment is based on anti-diarrhoeal drugs, bismuth, aminosalicylates and topical corticosteroid enemas.COMPARISON BETWEEN UC AND CD
UC more in non-smoker or ex-smoker, while CD more common in smoker.Sever UC is associated with HLA-DR103, while CD with chromosome 16 mutation (CARD15/NOD2).
Involve colon , start from rectum and extend proximally, the lesions are confluent. CD involve any part of GIT from mouth to anus, perianal lesions and lesion are patchy with skip-lesion.
Extra-intestinal involvement is common in both.
In UC: Main presentation is bloody diarrhea, while in CD: Abdominal pain, diarrhea and weight loss.
In UC the lesions are limited to mucosa with cryptitis and crypt abscess, but in CD submucosa, transmural, deep fissuring ulcers, fistula, patchy changes and granuloma.
R of UC: 5ASA, steroid, azathioprine, colectomy is curable. In CD: steroid, azathioprine, methotrexate, infliximab, nutritional R, surgery for complications is not curable.
Differential diagnosis of IBD
CONDITIONS WHICH CAN MIMIC ULCERATIVE OR CROHN'S COLITIS
Infective (with first attack of IBD colitis)
Bacterial
Salmonella
Shigella
Campylobacter jejuni
E. coli O:157
Gonococcal proctitis
Pseudomembranous colitis (Antibiotics)
Chlamydia proctitis
Viral
Herpes simplex proctitis
Cytomegalovirus
Protozoal
Amoebiasis
Non-infective
Vascular
Ischaemic colitis
Radiation proctitis
Idiopathic
Collagenous colitis
Behçet's disease
Drugs
NSAIDs
Neoplastic
Colonic carcinoma
Other
Diverticulitis
The major diagnostic difficulty is to distinguish the first attack of acute colitis from infection. In general, diarrhoea lasting longer than 10 days is unlikely to be the result of infection.
Stool microscopy, culture and examination for Clostridium difficile toxin or for ova and cysts,
sigmoidoscopy and rectal biopsy.
blood cultures and serological tests for infection are useful
DIFFERENTIAL DIAGNOSIS OF SMALL BOWEL CROHN'S DISEASE
Other causes of right iliac fossa massCaecal carcinoma
Appendix abscess
Infection (TB, Yersinia, actinomycosis)
Mesenteric adenitis
Pelvic inflammatory disease
Lymphoma
Investigations of IBD
Blood examination
Full blood count may show anaemia resulting from bleeding or malabsorption of iron, folic acid or vitamin B12.
Serum albumin concentration falls as a consequence of protein-losing enteropathy, or because of poor nutrition.
The ESR is raised in exacerbations or because of abscess. Elevation of CRP concentration is helpful in monitoring Crohn's disease activity
Bacteriology Stool cultures are performed to exclude superimposed enteric infection in patients who present with exacerbations of IBD. Blood cultures are also advisable in patients with known colitis or Crohn's disease who develop fever.
Sigmoidoscopy and/or colonoscopy:
A. Ulcerative colitisloss of vascular pattern.
granularity.
friability
and ulceration.
Also pseudopolyps,
And carcinoma.
NORMAL RECTUM
NORMAL SIGMOID COLON
NORMAL SPLENIC FLEXURE
NORMAL TRANVERSE COLON
NORMAL ASCENDING COLON
UC GROSS
UCB. In Crohn's disease
patchy inflammation with discrete, deep ulcers or aphthus like ulcers.perianal disease (fissures, fistulae and skin tags)
or rectal sparing may occur.
CAPSULE ENDOSCOPY
Barium studiesBarium enema is a less sensitive investigation than colonoscopy. In long-standing ulcerative colitis the colon is shortened and loses haustra to become tubular, and pseudopolyps are seen. In Crohn's colitis a range of abnormalities occur. The appearances may be identical to those of ulcerative colitis but skip lesions, strictures and deeper ulcers are characteristic .
Reflux into the terminal ileum may show stricture and ulcers. Contrast studies of the small bowel are normal in ulcerative colitis, but in Crohn's disease affected areas are narrowed and ulcerated; multiple strictures are common .
Plain abdominal X-ray
is essential in the management of patients who present with severe active disease. Dilatation of the colon , mucosal oedema ('thumb-printing') or evidence of perforation may be found. In small bowel Crohn's disease there may be evidence of intestinal obstruction or displacement of bowel loops by a mass.
Ultrasound
may identify thickened small bowel loops and abscess development in Crohn's disease.
Diagnosis of Small bowel Crohn's disease
1. white cell scanning may help identify inflamed intestinal segments.2. In atypical cases biopsy or surgical resection is necessary to exclude other diseases . This can often be done endoscopically by ileal intubation at colonoscopy, but sometimes laparotomy or laparoscopy with resection or full-thickness biopsy is necessary.
Aim of treatment
1. To treat acute attacks
2. To prevent relapses
3. To detect carcinoma at an early stage
4. To select patients for surgery.


Methylprednisolone IV Drip (SEVERE IBD)

Cyclosporine IV drip(SEVERE UC)

Biological AgentsInfliximab 5mg/kg, IV drip (0, 2W, 6Ws. Adalimumab (subcutaneous)

Thiopurines
Maintenance therapy / steroid sparing
Medical management of ulcerative colitis
Treatment depends upon the extent and activity of colitis.Active proctitis
In mild to moderate disease Mesalazine (5ASA) enemas or suppositories combined with oral mesalazine are effective first-line therapy.
Topical corticosteroids are less effective and are reserved for patients who are intolerant of topical mesalazine.
Patients who fail to respond are treated with oral prednisolone 40 mg daily.
Active left-sided or extensive ulcerative colitis
In mildly active cases, high-dose aminosalicylates( Mesalazine) combined with topical aminosalicylate and corticosteroids are effective.
Oral Prednisolone 40 mg daily is indicated for more active disease or when initial aminosalicylate therapy is ineffective.
Severe ulcerative colitis
Admit to hospital.
Systemic high doses of steroid (iv methyl prednisolone or hydrocortisone).
Supportive treatment like iv fluid, blood transfusion and nutritional support.
Antibiotic therapy if infection is evidence of infection.
Lab tests (Hb, ESR, Electrolytes, S. Urea….)
Plain X-ray of abdomen to exclude toxic megacolon.
DVT prophylaxis by Heparin.
Avoid opiates and anti-diarrheal agents.
Iv ciclosporin (cyclosporine) (2mg/kg) or infliximab (5mg/kg) in patients not responding to 3-5 days of steroid therapy.
If Patient not responding to above treatment or develop toxic megacolon consider surgery (total colectomy).
INDICATIONS FOR SURGERY IN ULCERATIVE COLITIS
Impaired quality of life
Failure of medical therapy
Fulminant colitis
Disease complications unresponsive to medical therapy
Colon cancer or severe dysplasia
R OF ACTIVE CROHN’S DISEASE
Patients with active colitis or ileocolitis are initially treated in a similar manner to those with active ulcerative colitis. Aminosalicylates and corticosteroids are both effective and usually effect remission in active ileocolitis and colitis. In severe disease intravenous prednisolone is indicated, but abscess or fistulating disease should be excluded before instituting therapy with corticosteroids.R OF ILEAL DISEASE IN CD
Steroid: Budesonide is appropriate for treating moderately active disease, although it is marginally less effective thanprednisolone. Aminosalicylates have little added valuethere is some evidence to support the use of oral metronodazole.
Poorly responding patients should, at an early stage, be considered for surgical resection since this is associated with prolonged remission in most cases.
Infliximab (anti-TNF monoclonal antibody ) given as an intravenous infusion 4-8-weekly on three occasions induces remission in patients with active Crohn's disease at any site within the gastrointestinal tract and is also effective for the management of some extraintestinal complications including pyoderma gangrenosum and some forms of arthritis. combined with disease-modifying agents, either thiopurines or methotrexate, to maintain remission.
nutritional support which in the most severe cases involves prolonged parenteral nutrition