STOMACH & DUODENUM -2
Duodenal villous adenomas• Commonly found around the ampulla of Vater
• Premalignant
• Often found in patients with familial adenomatous polyposis.
DUODENAL TUMOURSBenign duodenal tumours
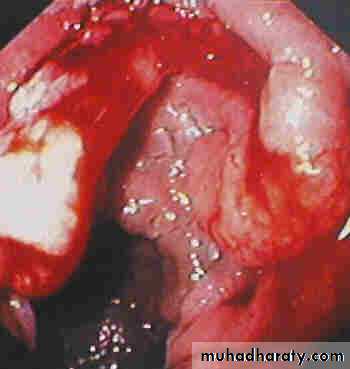
Duodenal adenocarcinoma
• uncommon,• The most common site for adenocarcinoma arising in the small bowel.
• Patients present with anemia (ulceration), or duodenal obstruction.
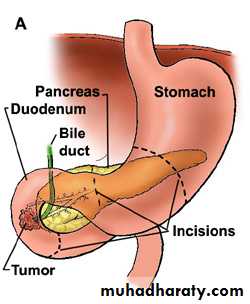
• Curative surgical treatment will involve a pancreaticoduodenectomy (Whipple’s procedure).
MALIGNANT DUODENAL TUMOURS
Doudenal GIST
Neuroendocrine tumoursNon-functioning neuroendocrine tumours (Carcinoid tumors)
Zollinger–Ellison syndrome (Gastrinoma):
• It is a cause of persistent peptic ulceration.
• Also occurs in the pancreas, especially the head.
• either sporadic or associated with the autosomal dominantly inherited multiple endocrine neoplasia (MEN) type I (in which a parathyroid adenoma is almost invariable).
• Diagnosis: High Basal Acid secretion
High Gastrin level
• Cancer of pancreatic head is the most common cause.
• Metastases from colorectal and gastric cancer.• Primary duodenal cancer
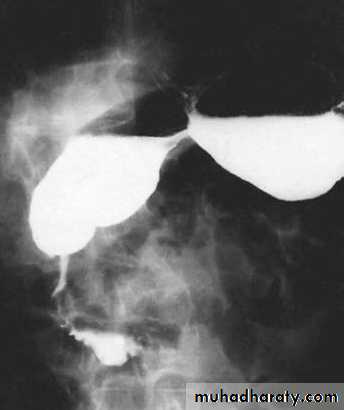
• Annular pancreas
• Pancreatitis
• Arteriomesenteric compression: fourth part of the duodenum is compressed between the superior mesenteric artery and the vertebral column
DUODENAL OBSTRUCTION
Acute gastric dilatation
• Associated with pyloroduodenal disorders or postsurgery without nasogastric suction.
• Can result in a sudden massive vomit with aspiration into the lungs.
Trichobezoar and phytobezoar
• Trichobezoar (hair balls) exclusively found in female psychiatric patients, often young.
• Hair, which remains undigested in the stomach can lead to ulceration and gastrointestinal bleeding, perforation or obstruction.
• Phytobezoars are made of vegetable matter and found principally in patients who have gastric stasis.
Foreign bodies in the stomach e.g. needles, usually pass spontaneously, or removed endoscopically, rarely surgery required.
OTHER GASTRIC CONDITIONS

Volvulus of the stomach
Rotation around its fixed points (cardia & pylorus):• Horizontal (Oraganoaxial).
• Vertical (Mesenteroaxial).
• Usually associated with diaphragmatic hernia, eventration of diaphragm.
• The transverse colon moves upwards taking the
stomach with it & both may enter the chest
• Presentation: - chronic (vomiting)
- acute (ischemia)
• Surgery:
Reduction of hernia
Close diaph. Defect.
Separate stomach from T. colon
Anterior gastropexy (fixed to abd wall).