1
Fifth stage
pediatrics
Lec-
Dr. Athal
9/11/2016
Pneumonia
Definition
:
• Pneumonia is an infection of the lower respiratory tract that involves the airways and
parenchyma with consolidation of the alveolar spaces.
• Lobar pneumonia describes pneumonia localized to one or more lobes of the lung.
• Bronchopneumonia refers to inflammation of the lung that is centered in the bronchioles and
leads to the production of a mucopurulent exudate that obstructs some of these small airways
and causes patchy consolidation of the adjacent lobules.
• Atypical pneumonia describes patterns typically more diffuse or interstitial than lobar
pneumonia.
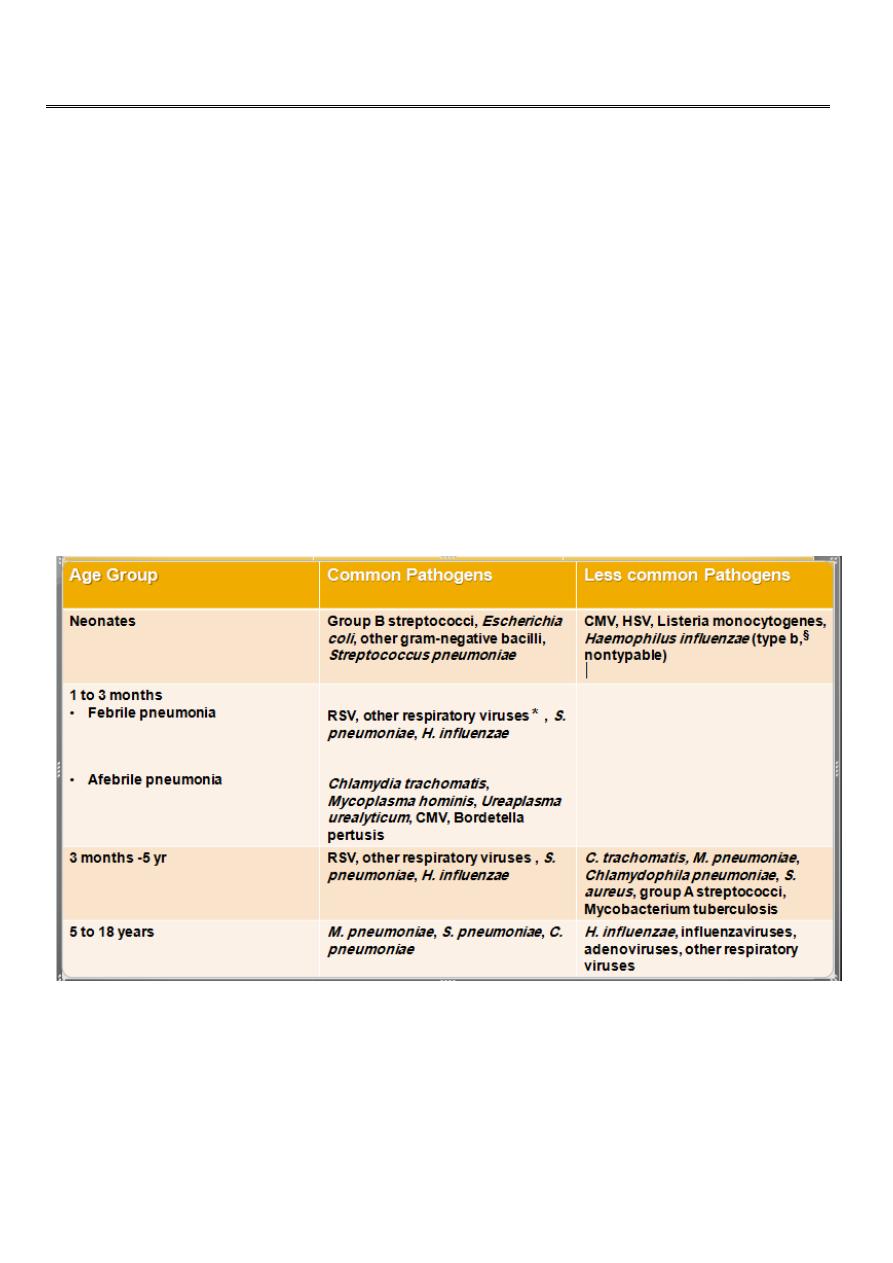
ETIOLOGY :
§
:
H. influenzae type b infection is uncommon with universal H. influenzae type b
immunization.
*: other respiratory viruses (parainfluenza viruses, influenzaviruses, adenoviruses, human
metapneumovirus.
2
Additional agents causes of pneumonia:
• SARS (severe acvute respiratory syndrome): due to corona virus.
• Avian influenza (bird flu): is highly contagious viral disease of poultry & other birds caused by
influenza A (H5N1). There were outbreaks among humans in South East Asia in 1997 & 2003-
2004 with high mortality rate.
• A novel influenza A (H1N1) of swine origin began circulating in 2009.
• M. pneumoniae and Chlamydophila pneumoniae are principal causes of atypical pneumonia.
Causes of pneumonia in immunocompromised persons include:
• gram-negative enteric bacteria
• mycobacteria (M. avium complex)
• fungi (aspergillosis)
• viruses (CMV)
• Pneumocystis carinii
Pneumonia in patients with cystic fibrosis usually is caused by:
• Staphylococcus aureus in infancy
• Pseudomonas aeruginosa or Burkholderia cepacia in older patients.
Risk factors for lower respiratory tract infections include:
• GERD
• Neurologic impairment (aspiration)
• Immunocompromised states.
• Anatomic abnormalities of the respiratory tract.
• Hospitalization, especially in an intensive care unit (ICU) or requiring
invasive procedures.
CLINICAL MANIFESTATIONS
Fever, chills, tachypnea, cough, malaise, pleuritic chest pain, retractions, SOB &
apprehension. Apnea especially in young infant.
Examination cannot distinguish viral from bacterial pneumonia, in general:
Viral pneumonias:
are associated more often with cough, wheezing, or stridor; low
fever. Hyperexpansion cause low diaphragm or liver. Sign of consolidation diffuse.
Bacterial pneumonias:
typically are associated with higher fever, chills, cough, dyspnea,
and findings of lung consolidation localized (bronchial breathing, dull percussion, distant
breath sound & course crepitation). Poor diaphragmatic excursion may indicate large
consolidation or effusion.

3
LABORATORY AND IMAGING STUDIES
WBC: in viral pneumonias is often normal or mildly elevated, with a predominance of
lymphocytes, whereas with bacterial pneumonias the WBC count is elevated
(>20,000/mm
3
) with a predominance of neutrophils.
Blood cultures are positive in 10% to 20% of bacterial pneumonia.
Viral detection: by serology or culture, but not routine.
M. pneumoniae: Mycoplasma IgM or PCR.
M. tuberculosis: is established by tuberculin skin test, and analysis of sputum or gastric
aspirates by culture or PCR.
When there is effusion or empyema, performing a thoracentesis to obtain pleural fluid
can be diagnostic and therapeutic.
The need to establish an etiologic diagnosis of pneumonia are:
• immunocompromised patients
• recurrent pneumonia
• pneumonia unresponsive to empirical therapy.
For these patients:
bronchoscopy with bronchoalveolar lavage and brush mucosal biopsy, needle aspiration of
the lung, and open lung biopsy are methods of obtaining material for microbiologic
diagnosis.
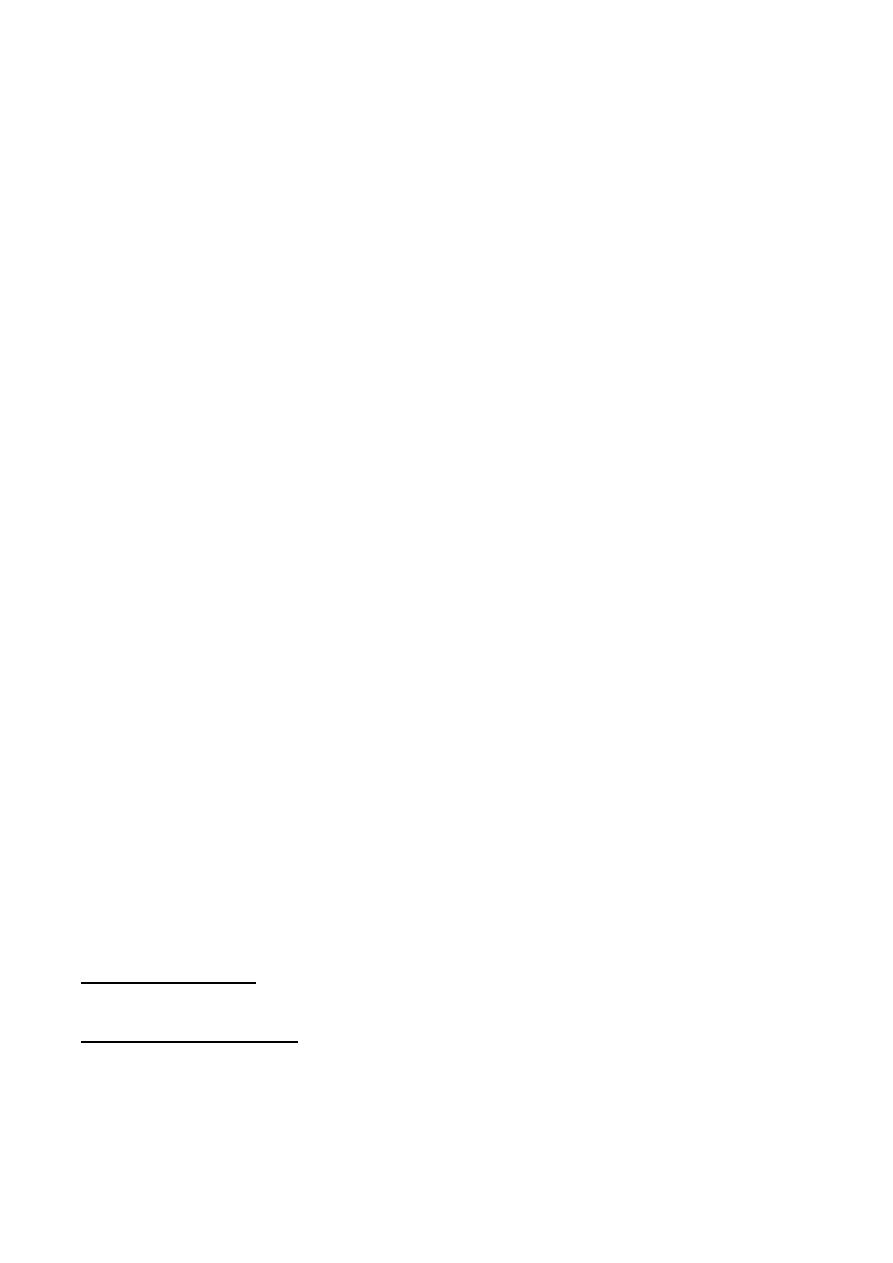
"Lobar Pneumonia"
4
"Bronchopneumonia"
"
Mycoplasma pneumoniae infection (atypical pneumonia)"
CXR:
Frontal & lateral:
-Bacterial pneumonia characteristically shows lobar consolidation, or a round
pneumonia, with pleural effusion in 10% to 30% of cases.
-Viral pneumonia characteristically shows diffuse, streaky infiltrates of
bronchopneumonia.
-Atypical pneumonia, such as with M. pneumoniae and C. pneumoniae, shows
increased interstitial markings or bronchopneumonia.
Decubitus
views to assess size of pleural effusions.
Ultrasound:
to assess pleural effusions.
CT:
is used to evaluate serious disease, abscesses & effusions.

5
TREATMENT
Therapy for pneumonia includes supportive and specific treatment and depends on the
degree of illness, complications, and knowledge of the infectious agent likely causing the
pneumonia.
Factors Suggesting Need for Hospitalization :
1. Age <6 months with suspected bacterial pneumonia.
2. Immunocompromised state
3. Toxic appearance
4. Severe respiratory distress
5. Requirement for supplemental oxygen
6. Dehydration
7. Vomiting
8. No response to appropriate oral antibiotic therapy.
9. Suspect pathogen with increased virulence e.g. methicillin resistant staph
aureus.
10. Noncompliant parents
Outpatients treatment: 7-10 days
Amoxicillin
Erythromycin, azithromycin, or clarithromycin if atypical pn. suspected.
Hospital treatment: 10-14 days
Usually combined antibiotic therapy according to age & suspected organism.
Neonate
: treated as sepsis
< 5 years:
Amoxicillin or ampicillin (if fully immunized for s. pneumoniae & H. influenzae type b).
Alternative: cefotaxime or ceftriaxone if not fully immunized or local pencillin resistant.
Plus clindamycin
Plus macrolide if atypical pneumonia suspected.
> 5 years:
Ampicillin Plus macrolide if atypical pneumonia suspected.

6
Treatment in the ICU: 10-14 days
Intravenous administration for inpatients except for the macrolides (erythromycin,
azithromycin, and clarithromycin), which are given orally.
< 5 years:
o Cefotaxime or ceftriaxone
o Plus nafcillin , oxacillin, clindamycin or vancomycin.
o Plus macrolide if atypical pneumonia suspected.
> 5 years:
o Cefuroxime or ceftriaxone
o Plus macrolide if atypical pneumonia suspected.
o
With or without clindamycin or vancomycin.
COMPLICATIONS AND PROGNOSIS
• Parapneumonic effusion
• Empyema
• Lung abscess
• Pneumatocele
• Bronchiectasis
•
Bronchiolitis obliterans: due to severe adenovirus pneumonia, inflammatory process in
which the small airways are replaced by scar tissue, resulting in a reduction in lung
volume and lung compliance.
PREVENTION
• Annual influenza vaccine is recommended for all children over 6 mo.
• Universal childhood vaccination with conjugate vaccines for H influenzae type b and S.
pneumoniae.
• The severity of RSV infections can be reduced by use of palivizumab in high-risk patients.
• Reducing the duration of mechanical ventilation and administering antibiotics judiciously
reduces the incidence of ventilator-associated pneumonias.
• The head of the bed should be raised to 30 to 45 degrees for intubated patients to minimize
risk of aspiration, and all suctioning equipment and saline should be sterile.
• Hand washing before and after every patient contact and use of gloves for invasive
procedures are important measures to prevent nosocomial transmission of infections.
• Hospital staff with respiratory illnesses or who are carriers of certain organisms, such as
methicillin-resistant S. aureus, should comply with infection control policies to prevent
transfer of organisms to patients.
7
• Most children recover from pneumonia rapidly and completely, although radiographic
abnormalities may take 6 to 8 weeks to return to normal.
• In a few children, pneumonia may persist longer than 1 month or may be recurrent. In such
cases, the possibility of underlying disease must be investigated further, such as:
Tuberculin skin test
sweat chloride determination for cystic fibrosis
serum Ig and IgG subclass determinations
Bronchoscopy to identify anatomic abnormalities or foreign body
Barium swallow for GERD.
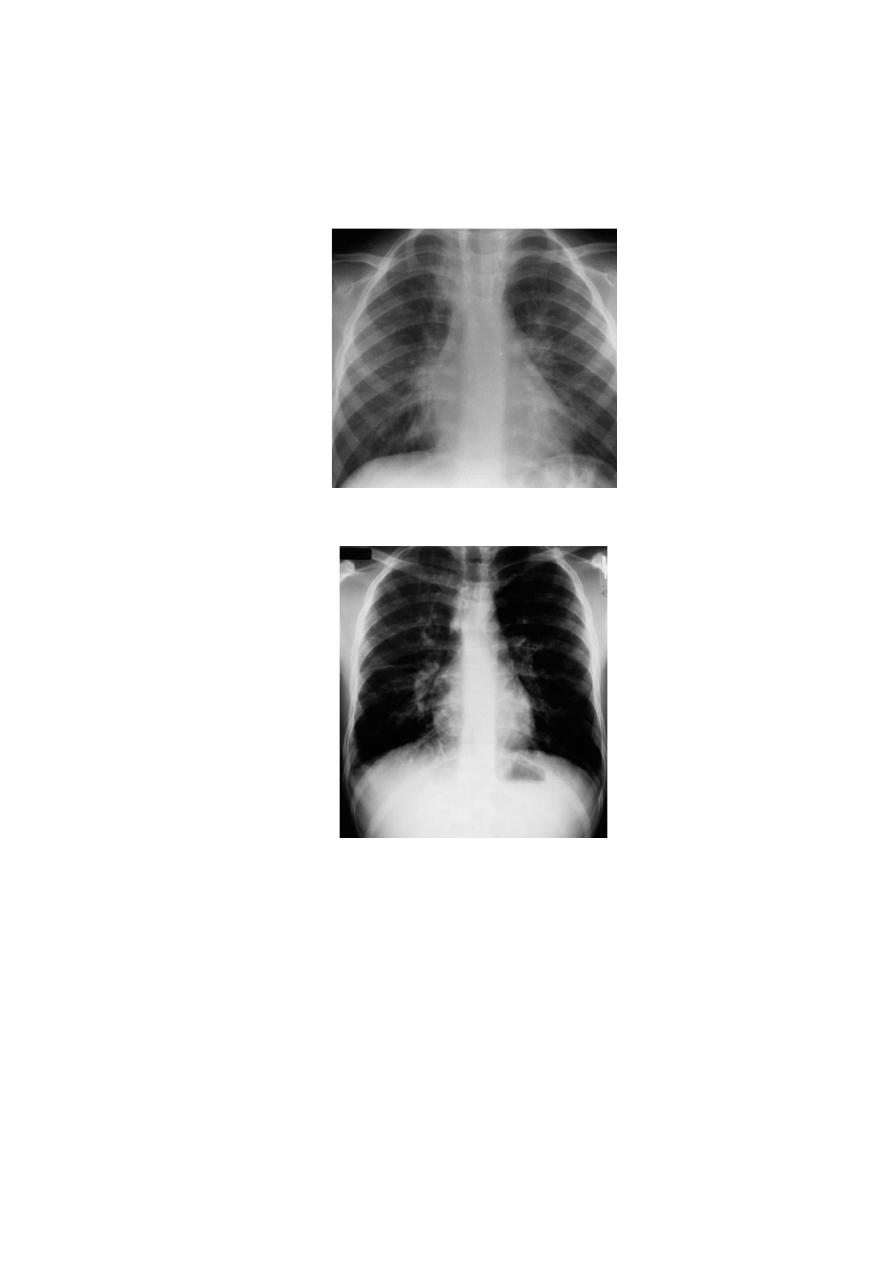
• Differential Diagnosis of Recurrent Pneumonia
PERTUSSIS
• Classic pertussis, whooping cough, is caused by B. pertussis, a gram-negative pleomorphic
bacillus with fastidious growth requirements.
• B. pertussis infect only humans and are transmitted person to person by coughing.
• The incubation period is 7-10 days. Patients are most contagious during the first 2 weeks of
cough.
• The peak age incidence of pertussis in the US is < 4 months of age-among infants too young
to be completely immunized and most likely to have the severe complications.
• Infections in adolescents have also been rising, likely due to waning immunity from previous
vaccines.
8
CLINICAL MANIFESTATIONS
The progression of the disease is divided into catarrhal, paroxysmal, and convalescent
stages.
• The catarrhal stage
: is marked by nonspecific signs (increased nasal secretions, and low-
grade fever) lasting 1 to 2 weeks.
•
The paroxysmal stage
: is the most distinctive stage of pertussis and lasts 2 to 4 weeks.
Coughing occurs in paroxysms during expiration, causing young children to lose their
breath. This pattern of coughing is needed to dislodge plugs of necrotic bronchial epithelial
tissues and thick mucus. The forceful inhalation against a narrowed glottis that follows this
paroxysm of cough produces the characteristic whoop. Post-tussive emesis is common.
•
The convalescent stage
: is marked by gradual resolution of symptoms over 1 to 2
weeks. Coughing becomes less severe, and the paroxysms and whoops slowly disappear.
Although the disease typically lasts 6 to 8 weeks, residual cough may persist for months,
especially with physical stress or respiratory irritants.
Infants
may not display the classic pertussis syndrome. The first sign in the neonate may
be episodes of
apnea.
Young infants are unlikely to have the classic whoop, more likely to
have
CNS damage as a result of hypoxia,
and more likely to have
secondary
bacterial pneumonia.
LABORATORY AND IMAGING STUDIES
• Isolation of B. pertussis by culture on specialized media.
• PCR
• Lymphocytosis: is present in 75% to 85% of patients but not diagnostic. WBC increase
to to more than 50,000 cells/mm
3,
consisting primarily of mature lymphocytes.
• CXR: segmental lung atelectasis. Perihilar infiltrates are common and are similar to
what is seen in viral pneumonia.
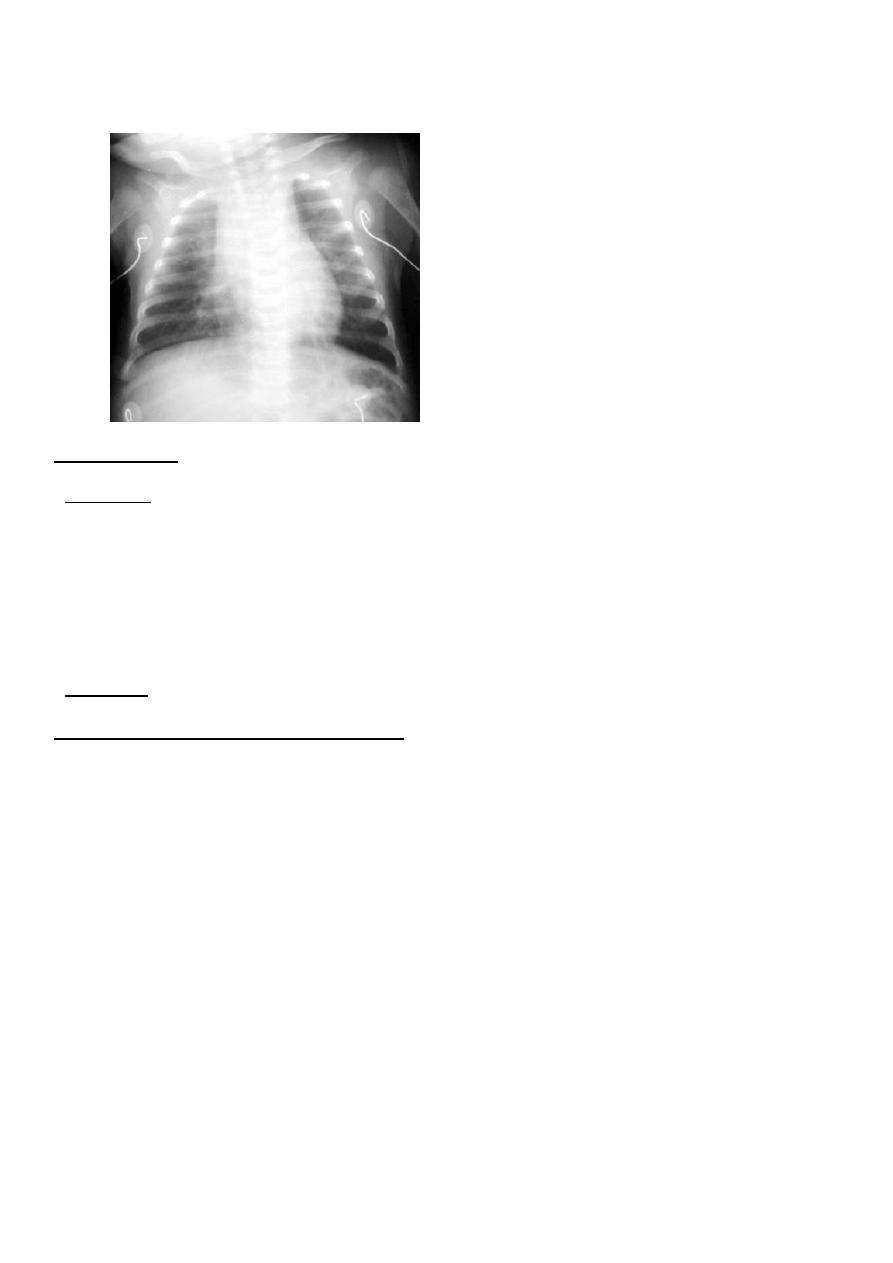
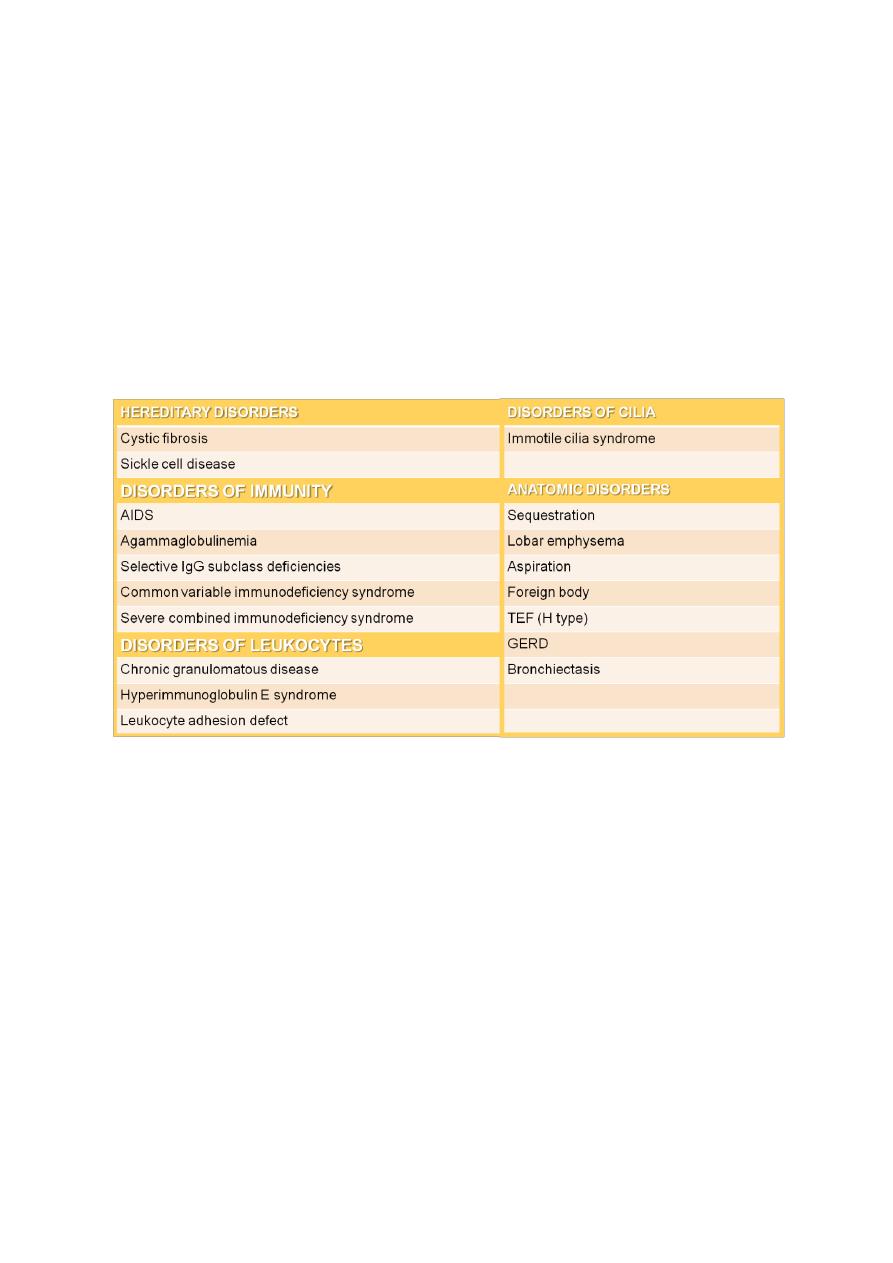
9
"shaggy heart" on CXR in a patient with Bordetella pertussis pneumonia.
TREATMENT
• Macrolide are recommended for children under 1 month of age. Azithromycin should be
used in neonates due to the association of erythromycin treatment and the development
of pyloric stenosis.
• Early treatment eradicates nasopharyngeal carriage of organisms within 3 to 4 days and
lessens the severity of symptoms.
• Treatment in the paroxysmal stage does not alter the course of illness but decrease the
potential for spread to others.
• TMP-SMZ is an alternative therapy among children >2mo, but this remains unproved.
COMPLICATIONS AND PROGNOSIS
Major complications are most common among infants and young children and include:
1. Hypoxia
2. Apnea
3. Pneumonia (caused by B. pertussis itself or resulting from secondary bacterial infection)
4. Atelectasis may develop secondary to mucous plugs.
5. The force of the paroxysm may produce pneumomediastinum, pneumothorax, or
interstitial or subcutaneous emphysema; epistaxis; hernias; and retinal and
subconjunctival hemorrhages.
6. Otitis media and sinusitis may occur.
7. Seizures
8. Encephalopathy
9. Malnutrition.
10. Most children do well with complete healing of the respiratory epithelium and have
normal pulmonary function after recovery. Young children can die from pertussis and
are more likely to be hospitalized than older children. Most permanent disability is a
result of encephalopathy.

11
PREVENTION
Active immunity is induced with acellular pertussis components given in
combination with the tetanus and diphtheria toxoids (DTaP ).
Macrolides are effective in preventing secondary cases in contacts exposed to
pertussis.
Under immunized close contacts under 7 years of age should receive a booster
dose of DTaP (unless a booster dose has been given within the preceding 3 years),
where as those 7-10 years of age should receive Tdap.
All close contacts should receive prophylactic antibiotic for 5 days (azithromycin)
or 7 to 14 days (clarythromcin or erythromycin)