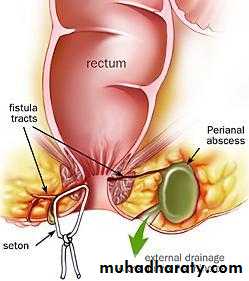
ANORECTAL ABSCESSES
Acute sepsis in the region of the anus is common.anorectal sepsis is more common in men than women,
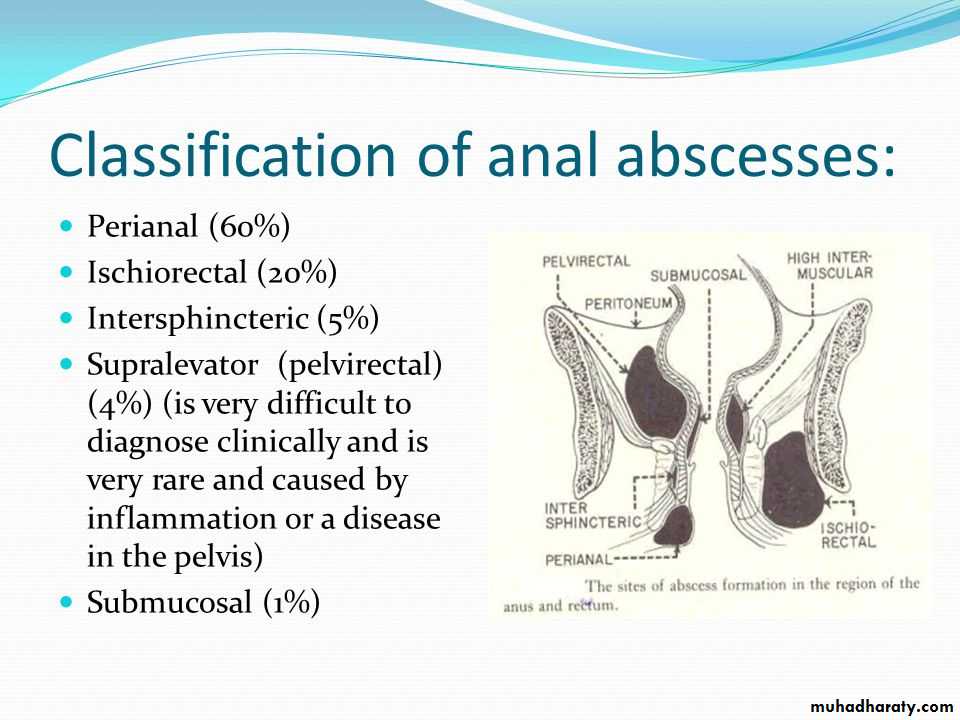
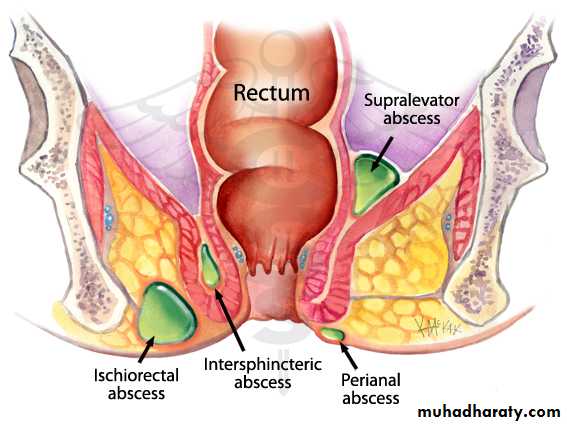
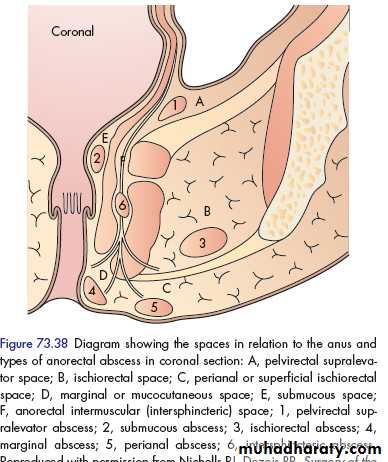
The cryptoglandular theory of intersphincteric anal gland infection holds that, upon infection of a gland, pus, which travels along the path of least resistance
, may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction to form a supralevator intermuscular or pararectal abscess
Sepsis unrelated to anal gland infection may occur at the same or at other sites (including submucosal abscess (following haemorrhoidal sclerotherapy, which usually resolve spontaneously), mucocutaneous or marginal abscess (infected haematoma),
ischiorectal abscess (foreign body, trauma, deep skin-related infection) and pelvirectal supralevator sepsis originating in pelvic disease.
Presentation
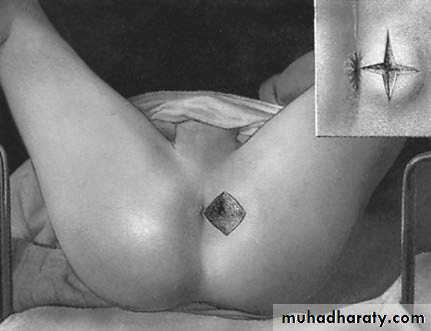
usually associated with a short (2–3 day) history of increasingly severe, well-localised pain and a palpable tender lump at the anal margin.Examination reveals an indurated hot tender perianal swelling.
constitutional upset and fever
Management
Management of acute anorectal sepsis is primarily surgical,including careful examination under anaesthesia, sigmoidoscopy and proctoscopy, and adequate drainage of the pusIncision of an ischiorectal abscess. The cavity is exploredand, if septa exist, they should be broken down gently with a fingerand the necrotic tissue lining the walls of the abscess removed by th finger wrapped in gauze. It is wise to biopsy the wall and send the pus for culture.
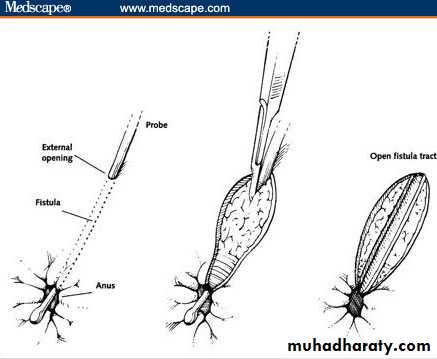
FISTULA-IN-ANO
A fistula-in-ano, or anal fistula, is a chronic abnormal communication, usually lined to some degree by granulation tissue, which runs outwards from the anorectal lumen (the internal opening) to an external opening on the skin of the perineum or buttockAnal fistulae may be found in association with specific conditions, such as Crohn’s disease,
However, the majority are termed non-specific, idiopathic or cryptoglandular, and intersphincteric anal gland infection is deemed central to them.
Presentation
more common in men than women
The overall incidence is about nine cases per 100000 population per year
those in their third, fourth and fifth decades of life are most commonly affected.
Patients usually complain of intermittent purulent discharge, pain (which increases until temporary relief occurs when the pus discharges).
Classification
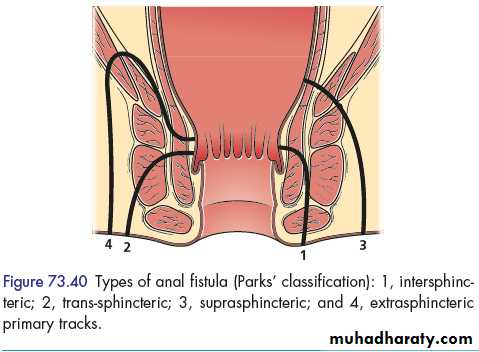
Goodsall’s rule
used to indicate the likely position of the internal opening according to the position of the external opening(s), is helpful but not infallible. The site of the internal opening may be felt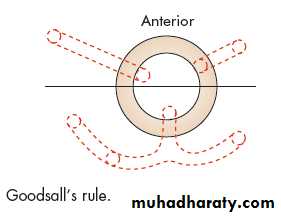
Special investigations
endoanal ultrasoundFistulagram
Magnetic resonance imaging (MRI) is acknowledged to be the ‘gold standard’ for fistula imaging, but it is limited by availability and cost and is usually reserved for difficult recurrent cases.
computed tomography (CT)
Surgical management
Fistulotomy That the fistulous track must be laid open
Fistulectomy This technique involves coring out of the fistula
seton
Advancement flaps
Biological agents agents that essentially plug and seal the track and allow ingrowth of healthy tissue to replace it



ANAL INTRAEPITHELIAL NEOPLASIA
is a multifocal virally induced dysplasia of the perianal or intra-anal epidermis which is associated with the human papilloma virus
A high index of suspicion and targeted biopsy yields the diagnosis, whereas multiple (mapping) biopsies give an indication of the extent and overall severity of the disease.
Extensive anal intraepithelial neoplasia (AIN), which extends intra-anally.

NON-MALIGNANT STRICTURES – ANALSTENOSIS
Spasmodic An anal fissure causes spasm of the internal sphincterOrganic Anal stenosis is a rare but serious complication of anorectal surgery, Other causes include trauma, inflammatory bowel disease, radiation
Postoperative stricture
Irradiation stricture
Senile anal stenosis
Lymphogranuloma inguinale
Inflammatory bowel diseaseEndometriosis
Neoplastic
Clinical features
Increasing difficulty in defaecation is the leading symptom.if the stools are formed, they are ‘pipe-stem’ in
shape.
In cases of inflammatory stricture, tenesmus, bleeding and the passage of mucus are superadded.
Treatment
Before starting treatment, it is important to ascertain the cause of the stricture.
Non-operative treatment is recommended for mild stenosis.
The use of stool softeners and fibre supplements helps aid the passage of stools.
Prophylactic
The passage of an anal dilator during convalescence after haemorrhoidectomy greatly reduces the incidence of postoperative stricture.Dilatation
Anal dilatation can be performed under general anaesthesia and then, by the patient, using an anal dilator.Anoplasty
For severe anal stenosis, an anoplasty is used to replace loss of anal tissue.The stricture is incised and a rotation or advancement flap of skin and subcutaneous tissue replaces the defect
Colostomy
Colostomy must be undertaken when a stricture is causing intestinal obstructionRectal excision and coloanal anastomosis
When the strictures are at or just above the anorectal junction and are associated with a normal anal canal,
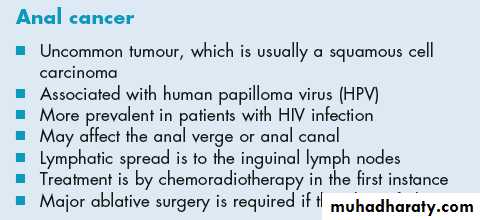
MALIGNANT TUMOURS
Anal malignancy is rare and accounts for less than 2 per cent of all large bowel cancers.incidence rate is 0.65 per 100 000.
Those arising below the dentate line are usually squamous,
whereas those above are variously termed basaloid,cloacogenic or transitional. Collectively, they are known as epidermoid carcinomas,
A mass, pruritus or discharge is less common
Advanced tumours may cause faecal incontinence by invasion of the sphinctersin women, anterior extension may result in anovaginal fistulation.
primary treatment is by chemoradiotherapy