Adult polycystic kidney disease
TUCOMInternal Medicine 4th class1-12-2016Dr. Hasan I. Sultan
Adult polycystic kidney disease (APKD)
ADPKD: It is an inherited multisystemic disease characterized by multiple cyst formation in both kidneys and other organs (like liver, pancreas or ovaries) with extrarenal noncystic manifestations such as mitral valve prolapse, intracranial aneurysms, and hernias.It is a common condition, with a prevalence of approximately 1 : 1000, and is inherited as an autosomal dominant trait. Small cysts lined by tubular epithelium develop from infancy or childhood and enlarge slowly and irregularly.
Mutations in the PKD1 gene (chromosome 16) account for 85% of cases and PKD2 (chromosome 4) for about 15%.
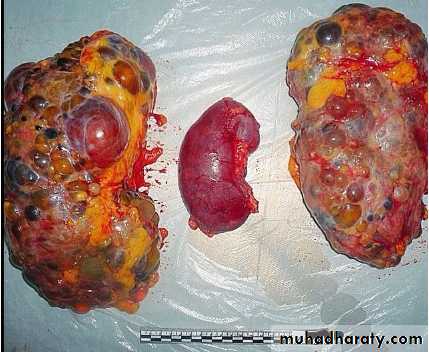
ADPKD kidneys compared to a normal kidney
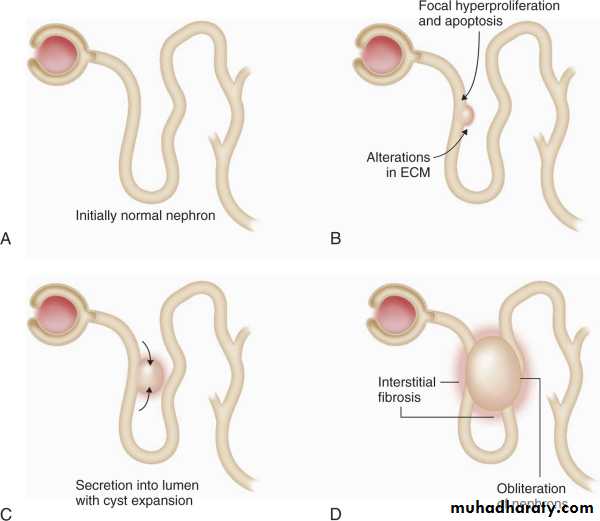
A to D, Steps involved in cyst formation: schematic of the sequence of events leading to renal cyst formation. Note that this process occurs hundreds or thousands of times during the natural history of polycystic kidney disease. ECM = extracellular matrix.
Clinical features
Common clinical features:
Vague discomfort in loin or abdomen due to increasing mass of renal tissue
Acute loin pain or renal colic due to haemorrhage into a cyst
Hypertension
Haematuria (with little or no proteinuria)
Urinary tract or cyst infections
Renal failure
Other clinical features:
Hepatic cysts and hepatomegaly
Cysts in other organs: pancreas, ovaries, lung and thyroid
Berry aneurysms of cerebral vessels and subarachnoid haemorrhage
Mitral and aortic regurgitation
Colonic diverticula
Abdominal wall hernias
Investigations
The diagnosis is usually based on family history, clinical findings and ultrasound examination.Ultrasound examination demonstrates cysts in both kidneys in approximately 95% of patients over the age of 20 years and 100% of patients over 30 years. U/S is the screening method of choice.
Cysts may also be identified by other imaging modalities, such as MRI
Mutation screening of PKD1 or PKD2 but this is seldom used in routine clinical practice.
Screening for intracranial aneurysms is not generally indicated but can be done by MR angiography in families with a history of subarachnoid haemorrhage.


MRI images of the kidneys. A Normal kidneys. B Polycystic kidneys; although the kidney enlargement is extreme.
A
B
Management
Good control of blood pressure is importantTreatment of urinary tract infection and nephrolithiasis
There is some evidence that the vasopressin V2 receptor antagonist (tolvaptan) can slow cyst formation in some patients but its place in treatment has yet to be established.
Patients with APKD are usually good candidates for dialysis and transplantation.
Surgery removing one or both kidneys to make space for a renal transplant or when it a source of pain or infection.
Prognosis
ESRD develops in approximately 50% of patients with ADPKD by 60 years of age.