
1
Nutritional Disease
The object of this lecture is to describe some aspects of the relationship between nutrition
and disease; the basic principles are as follows:
1- The total nutritional requirements of an individual = the basal requirements +
additional or adaptive requirements e.g. during disease, pregnancy, lactation or
growth (Neonates).
2- Nutritional requirements are met by oral intake unless artificial support is
necessary, so it is important to be sure about the appropriate food and absorption.
3- Adequate food intake, because deficiency states may lead to further problems such
as anorexia and changes in the immune status of patients.
4- Malnutrition is common even in affluent societies, as is obesity, which is frequent
in western world.
Normal dietary requirements:
Normal diet could be defined as one in which the contents of various nutrients are
sufficient to maintain optimal growth and functions of the body.
Metabolic effects of starvation:
The mechanisms of adaptation to an inadequate nutritional intake are of fundamental
importance to survival.
The changes depend on the duration of starvation; they include
1-
Continuous utilization of glucose as an energy substrate, this leads to a fall of
blood glucose followed by a decrease in insulin secretion.
2-
To offset this hypoglycaemia, hepatic glycogen is broken down to glucose. This
mechanism lasts only for about 16 h. this is because hepatic storage is limited, and
muscle glycogen cannot be mobilized to sustain blood glucose (since muscles
lack the enzyme Glucose 6- phosphatase).
3-
When hepatic stores are exhausted, increased hepatic gluconeogenesis takes
place, utilizing amino acids as substrate. The amino acids are derived from the
breakdown of protein especially that of muscles; this leads to an increase in
urinary urea excretion.
4-
Increased fat catabolism (breakdown) in adipose fatty tissues that leads to
accumulation of keton bodies derived from fatty acids metabolism.
5-
Keton bodies could be used as source of energy by nervous tissue, especially in
the brain and if this is increased, it may lead to decrease glucose requirement,
decrease gluconeogenesis with subsequent decrease in protein catabolism. So urea
decreases in urine.
6-
In advanced starvation acidosis caused by the accumulation of keton bodies leads
to increase excretion of hydrogen ion by the kidneys as ammonium cations.

2
The aims and results of the above mentioned adaptations are that the major energy
stores of the body are mobilized in away that spares protein breakdown and permit
maximal survival.
The adipose tissue stores, which usually comprise 9-15 kg, provide energy for about
40-70 days.
The total body protein is about 9-11 kg including 3-4 kg of muscle proteins.
Muscle stores will allow survival for about 75 days
Nutrient deficiencies
These can be classified into
Type 1: characterized by specific signs or symptoms that reflect reduced tissue
concentration of such elements or nutrients as iron, iodine, and vit. B
Type 2: is characterized by reduction in growth rate as in protein-energy
malnutrition. The effects are more severe and are clearly evident in infancy and early
childhood.
Protein energy malnutrition Syndrome (PEM)
This syndrome is characterized by
1- Loss of adipose tissue (as measured by skin fold thickness) and loss of tissue
proteins. As a result of the latter the skin becomes thin and inelastic and the hair is
dry and fall easily.
2- Lowered basal metabolic rate with a fall in heart rate and blood Pressure
3- Amenorrhoea.
Causes of PEM
1- Inadequate food intake.
2- Chronic diseases.
3- Anorexia nervosa.
4- Alcoholism.
In children PEM is classified as marasmus, kwashiorkor and intermediate forms in
between these two.
A. Marasmus, which is a disease of infancy resulting from early weaning onto a diet,
which is deficient in protein and calories.
The main features of marasmus
1- Growth retardation.
3
2- Wasting with loss of subcutaneous fat.
3- Edema is usually absent.
4-
Wizened face and premature aged appearance
. (Wizened means wrinkled, dried up
and thin).
5- The patient is alert and hungry.
B. Kwashiorkor, this term is derived from Ga- language of West Africa (
Ga
pertaining to, a
member of, a Black people of Ghana; (of) the language of this people)
means sickness of the older child
when the next one is born.
It affects older children 18-24 months after weaning to high CHO, low protein diet.
Main features are
1- Growth failure (retardation).
2- Loss of skeletal muscle mass, but subcutaneous fat is present.
3- Generalized edema with moon face.
4- Skin exfoliation (
shedding of the surface of the skin in the form of thin layers or scales)
.
5- Straight friable hair due to atrophy of the hair follicles. The hair, additionally, is
depigmentated.
6- Fatty, enlarged liver.
7- Anemia.
8- Vitamin deficiency.
9- Apathy and irritability. (
Apathy refers to lack of interest or emotion).
Kwashiorkor and marasmus represent the extreme ends at the spectrum of PEM, hybrid
status exists between these two extremes as typified by edematous marsmus and wasted
kwashiorkor.
In PEM there is marked predisposition to infections such as T.B and viral infections
There is also diarrhea, which is caused sometimes by overgrowth of even normal flora in
the gut.
This predisposition to infections is due to reduced T lymphocytes count that results in
impaired delayed hypersensitivity reactions as well as impairment in complement system
responses.
Treatment
This aim is to
1- Control the infection.
2- Replace deficient diets.
3- Follow up the patients
Effects of the disease on nutritional status
Injury and infections are usually associated with hypercatabolic response to injury.
Two main groups of mediators are involved in this condition
4
1- Hormones such as glucocorticoids, adrenaline, and glucagon, all these can
mobilize carbohydrates and fat stores as sources of energy.
2- Cytokines such as interlukine (IL) 1 and 6 as well as TNF α (tissue necrosis factor),
which induce fever and gluconeogenesis.
Patients in hypercatabolic status require provision of extra-energy substrates and proteins,
for example this is about
10% for an abdominal surgery e.g. cholecystectomy
25% for major surgery complicated by sepsis
50%
– 100%: accidental trauma and widespread full thickness burn.
Malignant tumors:-
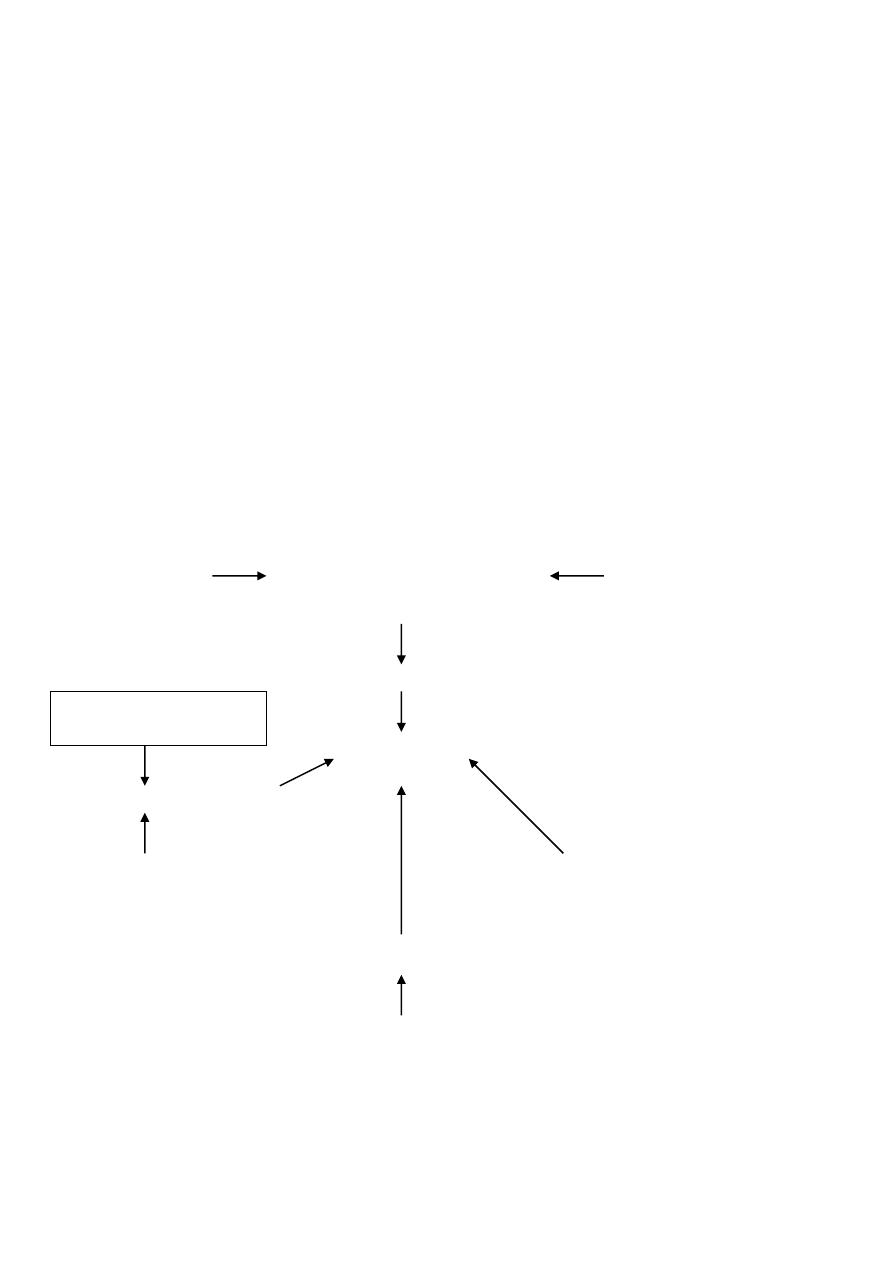
Most patients dying of cancer have evidence of PEM or (cancer cachexia )
the pathogenesis of cancer Cachexia is illustrated below
Anorexia Reduced nutrient Behavioral difficulties
intake
Abnormal losses Reduced absorption
Cancer cachexia
Reduced tissue synthesis
Chemotherapy-Radiotherapy Host/ tumor competition for
nutrients
Tissue Catabolism
Abnormal tissue metabolism
(Factors involved in cancer cachexia)
Vomiting, diarrhea
fistula
5
Tumor necrosis factor α formerly known as cachexin. It causes increased mobilization
of fat from adipose tissue through inhibition of lipoprotein lipase.
Systemic diseases associated with cachexia other than malignancy
G.I.T. diseases
* Malabsorption Syndrome: gluten-sensitive enteropathy.
* Surgical operation.
* Entero-cutaneons fistula.
* Artificial feeding.
Renal diseases
Renal failure: leads to restriction of protein diet
protein deficiency.
Liver diseases
The liver is a major nutrient-processing organ in the body, so in acute hepatitis
carbohydrate should be increased and low fat and protein diet is required.
In chronic liver diseases and hepatic failure, Na
+
intake should be reduced to minimize
edema and ascites.
Pulmonary disease
This is related to difficulties in chewing & swallowing because of difficulty in breathing.
Inborn errors of metabolism
These may affect absorption and metabolism of many nutrients.
Vitamins
They are divided into:
A. Fat-soluble types A, D, E, and K.
B. Water-soluble types B, C.
Factors responsible for vitamin deficiency
1- Reduced dietary intake.
2- Wrong procedures for cooking and storage.
3- Impaired G.I.T. absorption.
4- Increased metabolic demands.
5- Iatrogenic (Drugs like isoniazid that interferes with B
6
absorption).
Vitamin A
Functions
1- Affects function of mucus secreting epithelium.
2- Maintains normal vision.
6
Well-established deficiency, which is called (xerophthalmia), leads to drying and
wrinkling of the cornea. This in turn may lead to corneal ulceration and liquefaction
(keratomalacia) with subsequent scarring and blindness.
Vitamin A deficiency may also lead to recurrent respiratory tract infections; renal
stones formation (around keratin debris).
Vitamin D:
It can be regarded as a vitamin as well as a hormone.
Functions
Maintains normal plasma levels of Ca
++
and PO
4
-3
This function is achieved with the help of parathyroid hormone.
In humans vit D is derived from both dietary sources and endogenous synthesis
Endogenous Synthesis of Vit D
This occurs in the skin, where exposure to sunlight converts the abundant precursors
Sunlight
U.V of sun
7- Dehydro-cholesterol
Vit.D
Deficiency Features
Rickets in children, and osteomalacia in adults
Rickets
This is a bone disease produced by hypovitaniosis D and is characterized by
1- Failure of normal mineralization of newly laid- down osteoid.
2- Defective mineralization of epiphyseal cartilage, which is necessary to control
cartilaginous growth at the epiphyseal plate. This will lead to skeletal deformities
e.g. bowing of the legs.
Osteomalacia
This is a condition that affects adults due to hypovitaminosis D.
In this condition there is failure of bone mineralization that results in excess unmineralized
matrix and abnormally wide osteoid
These lead to radiolucency of the skeleton and
predispose to fracture.

7
Causes of Vit D deficiency
1- Decrease dietary intake.
2- Lack of cutaneous exposure to UV light.
3- Chronic renal failure.
4- Malabsorption.
Vitamin E
Functions
It is a potent antioxidant factor that can neutralize the free radicals generated by
many cellular redox reactions.
It minimizes free radical induced membrane lipid peroxidation, a protective role that
is particularly important in the nervous system and in preventing red cell lysis.
As an antioxidant, recent works suggest that it may have a role in the prevention of
atherosclerosis.
Deficiency features
- Peripheral neuropathy
- Retinopathy
Vitamin K
This vit is essential for synthesis of clotting factors such as II (prothrombin), VII, IX, and
X.
It is synthesized by intestinal bacterial flora and such a source can provide the body with
its requirement of this vit. Accordingly its deficiency is uncommon. However, in case of
neonates receiving broad-spectrum antibiotics, and also in patients receiving warfarine (an
anticoagulant, which block recycling of the vit), deficiency occurs.
Clinical manifestation of vit K deficiency
Hemorrhage, Ecchymosis, gingival bleeding, malena and haematemesis
Water Soluble Vitamins:
Thiamine (B1)
Functions
- Cofactor for the oxidative decarboxylation reaction for the synthesis of ATP.
- Cofactor in the pentose phosphate pathway.
- Maintains the integrity of cell membranes.
Thiamine deficiency is caused by
-
Long-term parenteral nutrition
. (Parenteral refers to the introduction of a substance into the
body other than by the mouth or gut, esp. by injection.)
- Severe diarrhea.
8
Deficiency features
1- Polyneuropathy (dry beriberi).
2- Cardiac dysfunction (wet beriberi), which is associated with edema.
3- Central nervous system dysfunction.
Riboflavin (vit B
2
)
Functions
- Flavoprotein (vit B
2
is one of its constituents) is essential for normal cell
metabolism.
- Act as coenzyme of many reactions.
Deficiency features
Seborrhoeic dermatitis
Keratitis of cornea
Niacin (Nicotinic acid)
Main functions
In oxidative metabolism it is a constituent of two coenzymes that are involved in the
metabolism of fat, CHO, and amino acids.
Niacin deficiency
This causes Pellagra (rough skin), which is characterized by the three D
s
Dermatitis
Diarrhea
Dementia
The dermatitis is called glove dermatitis, but it also affects face, neck, arms and feet. It is
an erythematous and burning lesion. Later the skin becomes scaly with irregular
pigmentation.
Pyridoxine (Vit B
6
)
Functions
Metabolism of amino acids
Haem synthesis
Stabilization of muscle phosphorylase.
9
Causes of deficiency
1. Pregnancy and lactation can render the mother and subsequently the
infant deficient in Vit B
6
.
2. Chronic alcoholism; an increased risk of deficiency is due to
accumulation of an alcohol metabolites which displaces pyridoxal- 5-
phosphate from its normal site of action.
3. Drugs like penicillamine and isoniazid; these are known to inactivate
B
6
, so after long term use Vit B
6
deficiency occur.
Features of deficiency include
Cheilitis
Glossitis
Seborrhoeic dermatitis
Peripheral neuropathy
Ascorbic acid (Vit C)
Functions
Reducing agent
Synthesis of stabilization of collagen.
Noradrenaline synthesis.
Absorption of iron.
Vit C deficiency (Scurvy)
This is a disease produced as a result of Vit C deficiency, which is uncommon nowadays.
It is characterized by
Skeletal changes,
Hemorrhage and gingival bleeding
Impaired wound healing.
Minerals and Trace elements
These are essential components of many of the body's enzymes. They are required in very
small amount.
Iron
Functions
Cellular respiration.
It is one of the components of hemoglobin, myoglobin, cytochromes, catalase and
peroxidase.
Deficiency
Signs and symptoms of iron deficiency include
1- Anemia with associated reduced capacity of physical activity

10
2- Increased susceptibility to infection.
3- Abnormal thermoregulation.
4- Koilonychia
Calcium
Total content of the body (wt of 70Kg.) is about 1300gm.
About 99 % of the calcium in the body is within the skeleton (bones).
Functions
1- Maintaining skeletal function.
2- Contraction and relaxation of skeletal and cardiac muscles.
3- Neuronal excitation and neuromuscular transmission.
Deficiency
This leads to neuromuscular irritability and tetany.
Magnesium
Function: maintains neuromuscular and nervous transmission.
Deficiency
1. Weakness of muscles and irritability.
2. Tetany and cardiac arrhythmias.
Copper
It is one of the trace elements.
Functions
It is involved in the following pathways
1- Cytochrome oxidase and superoxide dismutase.
2- Ceruloplasmin and haem synthesis.
3- Collagen synthesis.
4- Melanin production.
5- Dopamine beta-hydroxylase neuro-transmitter.
It is excreted in bile and feces.
Its deficiency may lead to hypochromic microcytic anemia with neutropenia and skeletal
disorders.
Wilson's disease: this is a disorder of copper metabolism determined by a pair of
autosomal recessive genes, in which there is increasing amount of copper that accumulates
in the liver, lenticular nuclei of the brain, kidneys and eyes
eventuates in macronodular cirrhosis, whereas brain damage leads to neurological
manifestations.

11
Zinc
Function: tissue repair, wound healing and maintenance of normal function of the
reproductive system.
Zinc deficiency is associated with
Hypogonadism and infertility.
Impaired wound healing.
Growth retardation in children.