
1
Fifth stage
Medicine
Lec-
د.خالد نافع
15/11/2016
Plasma cell disorder
Multiple Myeloma :
Malignant proliferation of plasma cells.
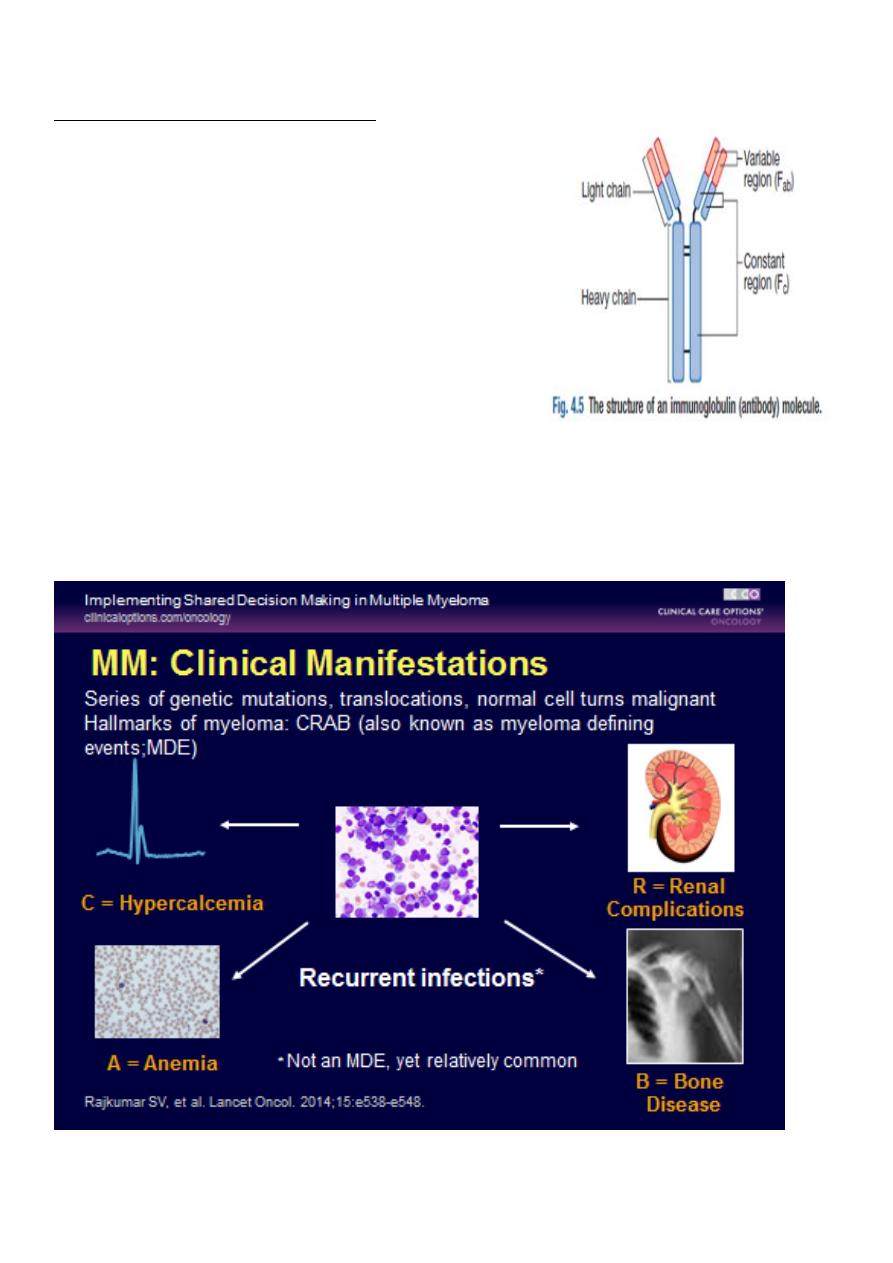
• Normal plasma cell form Ig which contain heavy and light chain
• Normal variety of Ig polyclonal & each contain Kappa & Lambda light chain
• Myeloma plasma cell : Ig of single heavy and light chain lead to monoclonal protein
(para protein)
• In some light chain may be only produced and appear in urine as Bence-Jones
proteinuria.
• Incidence : 4 new cases/100,000 peoples/year.
• Sex ratio : M:F → 2:1
• Age : median age 60-70 years.
• Etiology : Unknown,chemical, enviromental
Plasma cell myeloma
Variants
Non - secretory myeloma
Indolent myeloma
Smouldering myeloma
Plasma cell leukaemia
Plasmacytoma
- Solitary plasmacytoma of bone
- Extramedullary plasmacytoma
Immunoglobulin deposition diseases
- Primary amyloidosis
- Systemic light and heavy chain deposition disease
Osteosclerotic myeloma (POEMS)
Heavy chain diseases
γHCD
αHCD
µHCD
2
Classification of MM :
Paraprotein
frequency %
IgG
55%
IgA
21%
Light chain only
22%
Other (D, E, non secretory) 2%
The diagnosis of MM requires two of the following
marrow plasmacytosis.
Serum and/or urinary paraprotein
+
≥ 1 of `` CRAB``
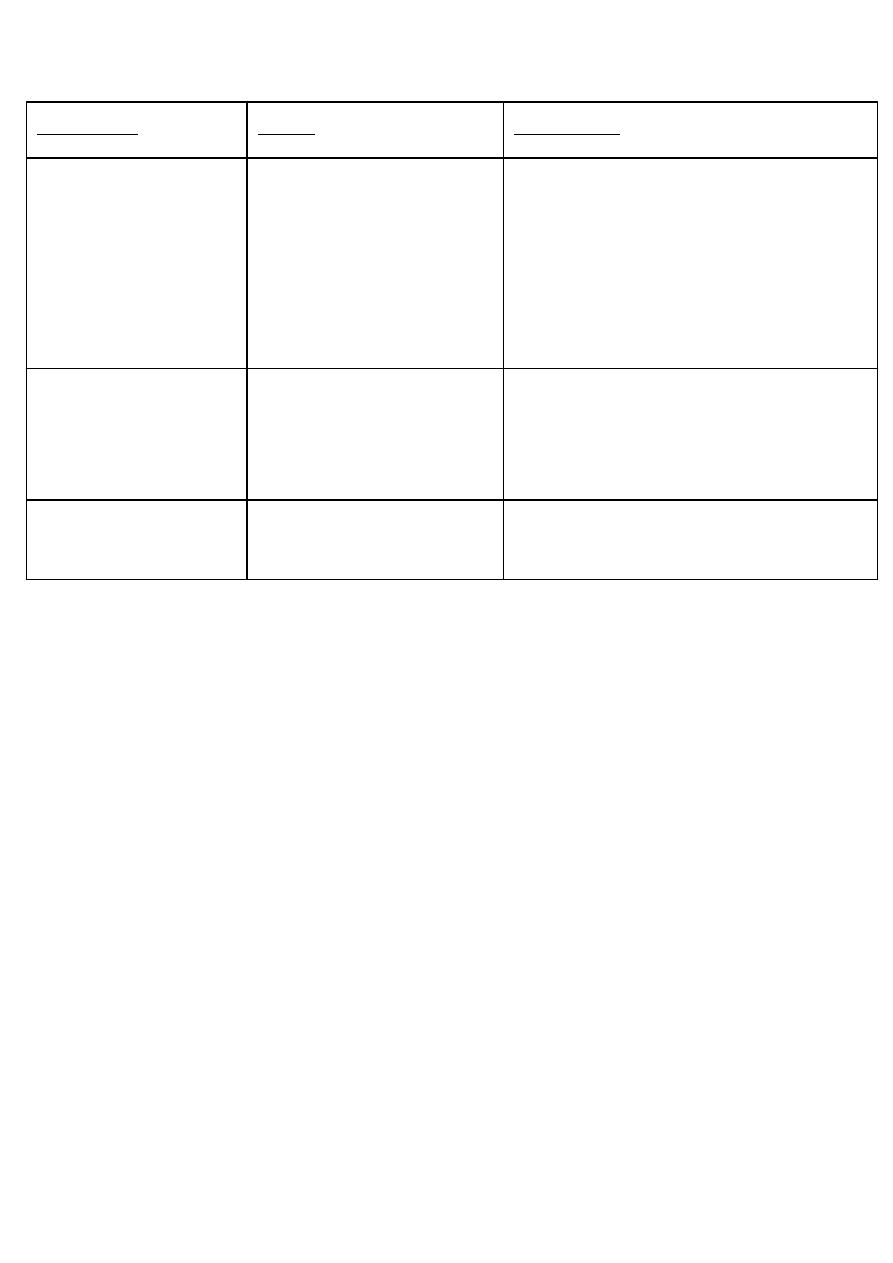
Clinical Manifestations of MM :
3
Multiple Myeloma :
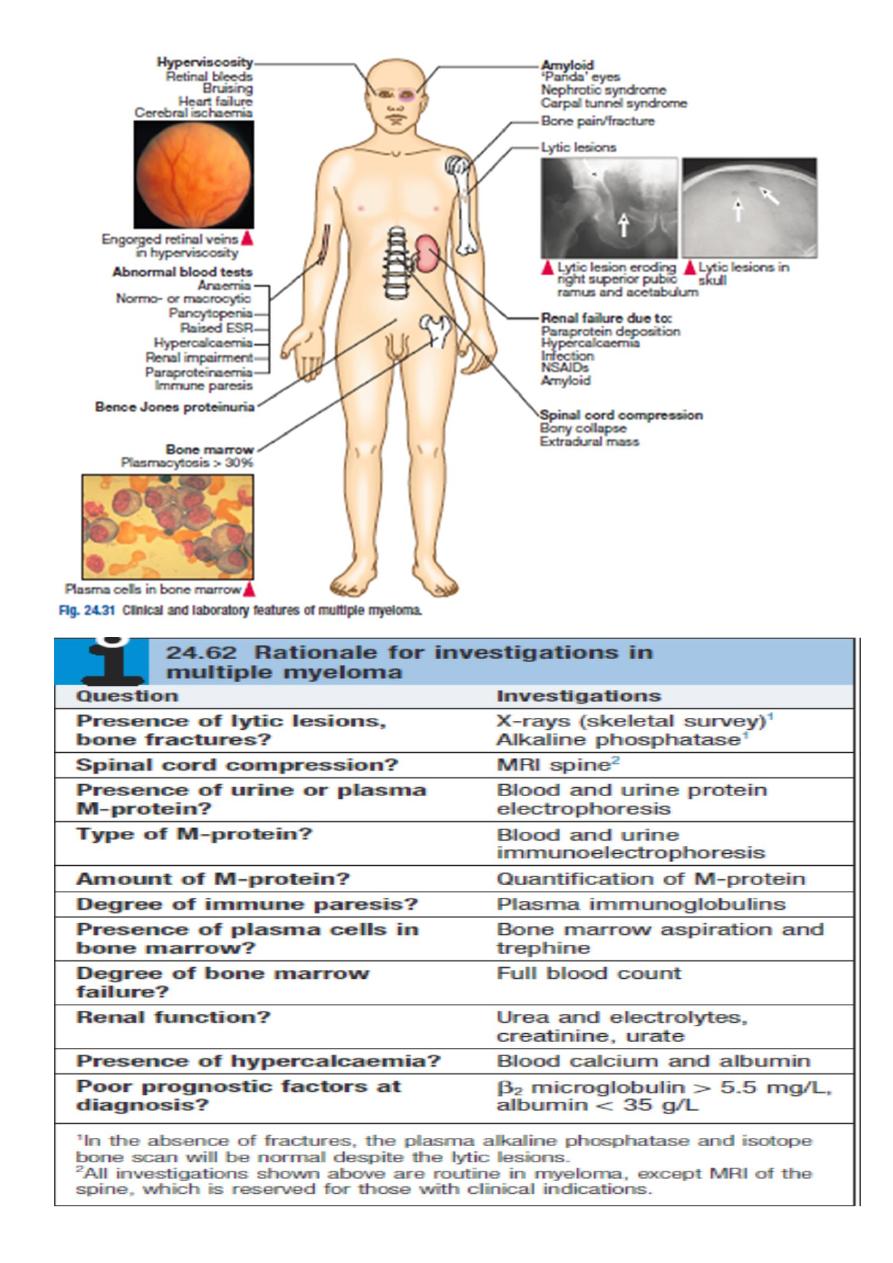
Clinical features :
• Weight loss ,malaise and fatigue.
• Bone pain found in 60% of cases at the back and ribs.
• Anorexia , diarrhea, vomiting, constipation, polyuria, polydipsia occur with
hypercalcemia in 30%,
• Renal impairment due to hypercalcaemia and dehydration present in 50% .
• Pneumococcal, chest and urinary tract infection due to low immunoglobulin(Ig)
production.
• Headache , Confusion, Breathlessness, Visual Disturbance and bleeding can occur
secondary to hyperviscosity (IgA).
• 5% present with paralysis secondary to spinal cord compression by extra-dural
plasma cell mass.
• Carpal-tunnel syndrome, nephrotic syndrome, cardiac failure and neuropathy
secondary to amyloid deposition.
Symptoms
Effect
Pathology
Pain
Severe local pain
Lethergy,
thirst
Anaemia& tiredness
Bone erosion due to
stimulation of oesteoclast.
Pathological fracture
Hypercalcaemia
BM failure
Marrow involvement
with malignant plasma
cell
Renal damage
Increased blood viscosity
Amylidosis -renal damage
Excess production of
light chains and
paraprotein
Infection (Resp.)
Impaired immune function
Reduction in number
of normal plasma cells
4
5
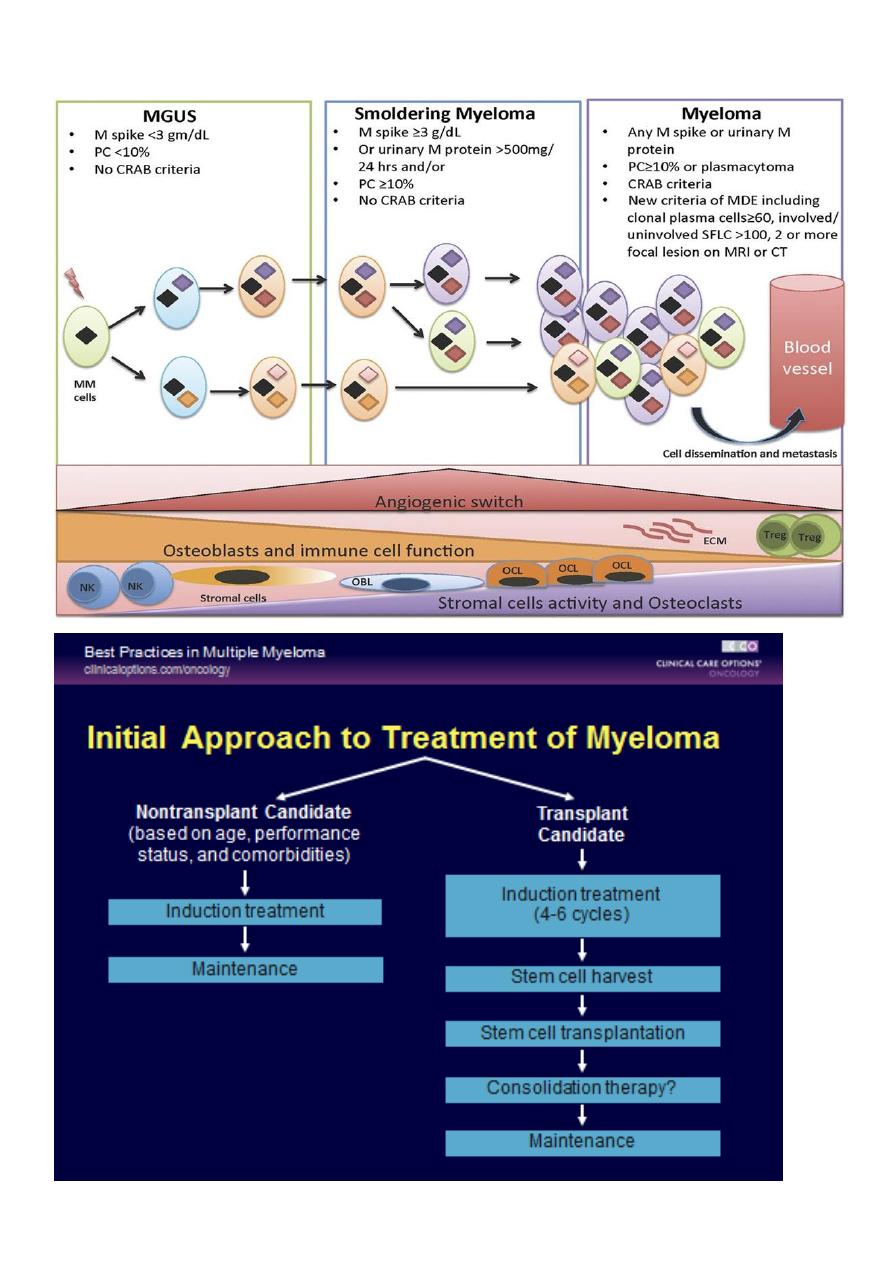
Revised IMWG Criteria (2014) :
6
Supportive Care :
Bone: 85% will develop bone disease
– All should receive monthly bisphosphonates after dental exam; monitor renal
function long term
Infection: major cause of death in MM
– Impaired antibody formation after antigenic stimulations
– Immunizations: pneumococcal (PCV13, PPSV23), seasonal inactivated influenza
– Shingles prophylaxis (proteasome inhibitor, transplant)
Renal: monitor status, dose reductions may be necessary
– Acute renal failure can occur due to NSAIDs, CT dyes, antibiotics
– Hydrate (carefully), monitor monthly

7
Management- Cont…
Allopurinol to prevent urate nephropathy.
Plasmapheresis, if necessary, for hyperviscosity
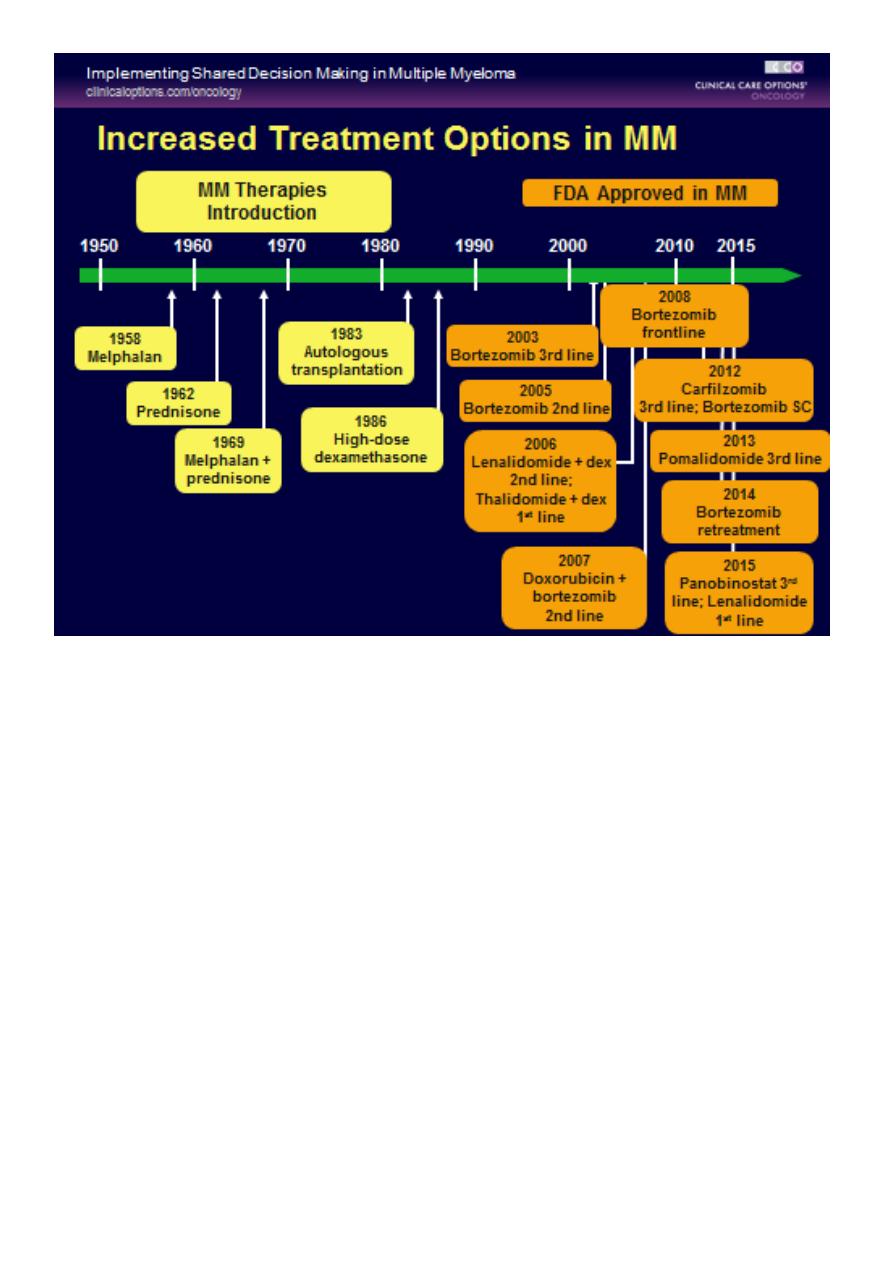
**Chemotherapy with or without HSCT
In older patients, thalidomide combined with the alkylating agent melphalan and
prednisolone has increased the median overall survival to more than 4 years.
In younger, fitter patients, standard treatment includes first-in chemotherapy to
maximum response and then an autologous HSCT
Cont.-Management :
1- BORTEZOMIB(VELCADE) VTD+Z
2- Thalidomide
3- Lenalidomide(Revlimid) VRD+Z
4- Dexamethasone
5- Bisphosphonate (Zoledronate)
Treatment is administered until paraprotein levels have stopped falling. This Is
termed‘plateau phase’ and can last for weeks or years.
Radiotherapy; for localised bone pain and for pathological fractures.
It is also useful for the emergency treatment of spinal cord compression complicating
extradural plasmacytomas
Long-term Effects of Treatment :
1. Diarrhea (lenalidomide)
2. Peripheral neuropathy (bortezomib, MM, diabetes)
3. Secondary cancers
4. Cardiovascular/pulmonary disease
Health maintenance is important as patients are at risk for same illnesses as
those without MM
5. Financial
Chronic illnesses are costly
Loss of income, hospital and medical bills can be high
Refer to patient care organizations, copay foundations

8
Waldenstrӧm macroglobulinaemia :
This is a low-grade lymphoplasmacytoid lymphoma associated with an IgM paraprotein.
Patients classically present with features of hyperviscosity,such as nosebleeds , bruising,
confusion and visual disturbance.
Anaemia, systemic symptoms, splenomegaly or lymphadenopathy
Investigation , have an IgM paraprotein associated with a raised plasma viscosity. The bone
marrow with infiltration of lymphoid cells and prominent mast cells.
Treatment :
1- Plasmapheresis for anaemia and hyperviscosity.
2- Chlorambucil
3- Fludarabine
4- Rituximab
*Monoclonal gammopathy of uncertain significance (MGUS)
a paraprotein is present in the blood but with no other features of myeloma, Waldenstrӧm
macroglobulinaemia, lymphoma or related disease.
The bone marrow may have increased plasma cells but these usually constitute less than
10% of nucleated cells.
After follow-up of 20 years, only one-quarter of cases will progress to myeloma or a related
disorder (i.e.around 1% per annum)