Sudden cardiac death:
Sudden cardiac death is form the major cause
of Sudden death, and the most common
cause of sudden cardiac death is ischemic
heart disease because chronic ischemia
predisposes the myocardium to the
development of lethal ventricular arrythemias
as ventricular fibrillation.
Morphology:
The
most common cardiac
lesions in sudden death are those of coronary
atherosclerosis and it's complication the

degree of atherosclerosis is marked with
more than 75% reduction in lumen of 2 or
more vessels, the acute plaque rupture
followed by coronary thrombosis and possibly
vasospasm triggers fatal ventricular
arrythmias in most cases.
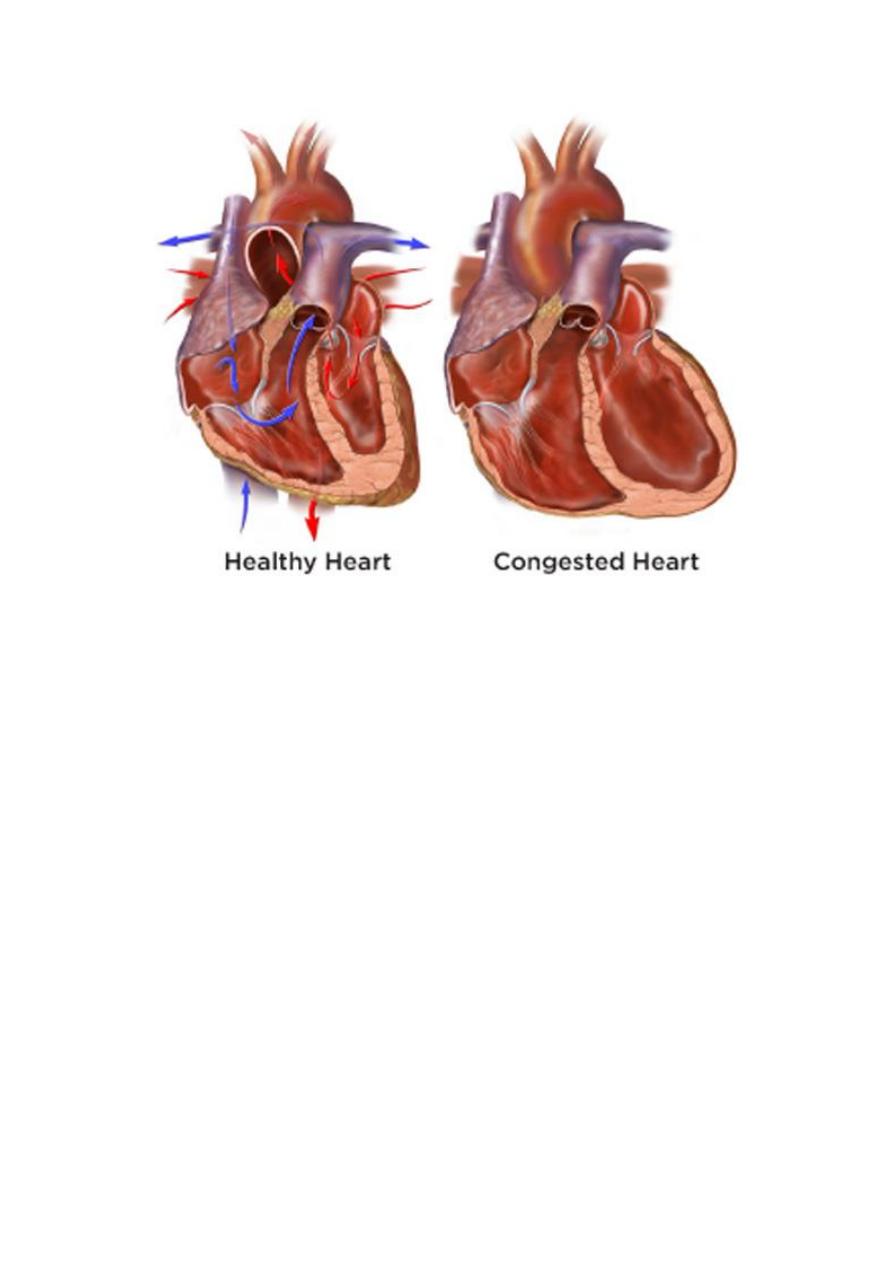
Cor pulmonale:
Or pulmonary heart disease is a disease of
right sided cardiac chambers caused by
pulmonary hypertension resulting from
pulmonary parenchymal or vascular diseases.
The condition may be acute or chronic, acute
cor pulmonale caused mostly from pulmonary
embolism, chronic cor pulmonale the most
common cause is chronic obstructive lung
disease.
Morphology:
In acute cor pulmonale the right ventricle is
usually dilated, but if sudden death occur
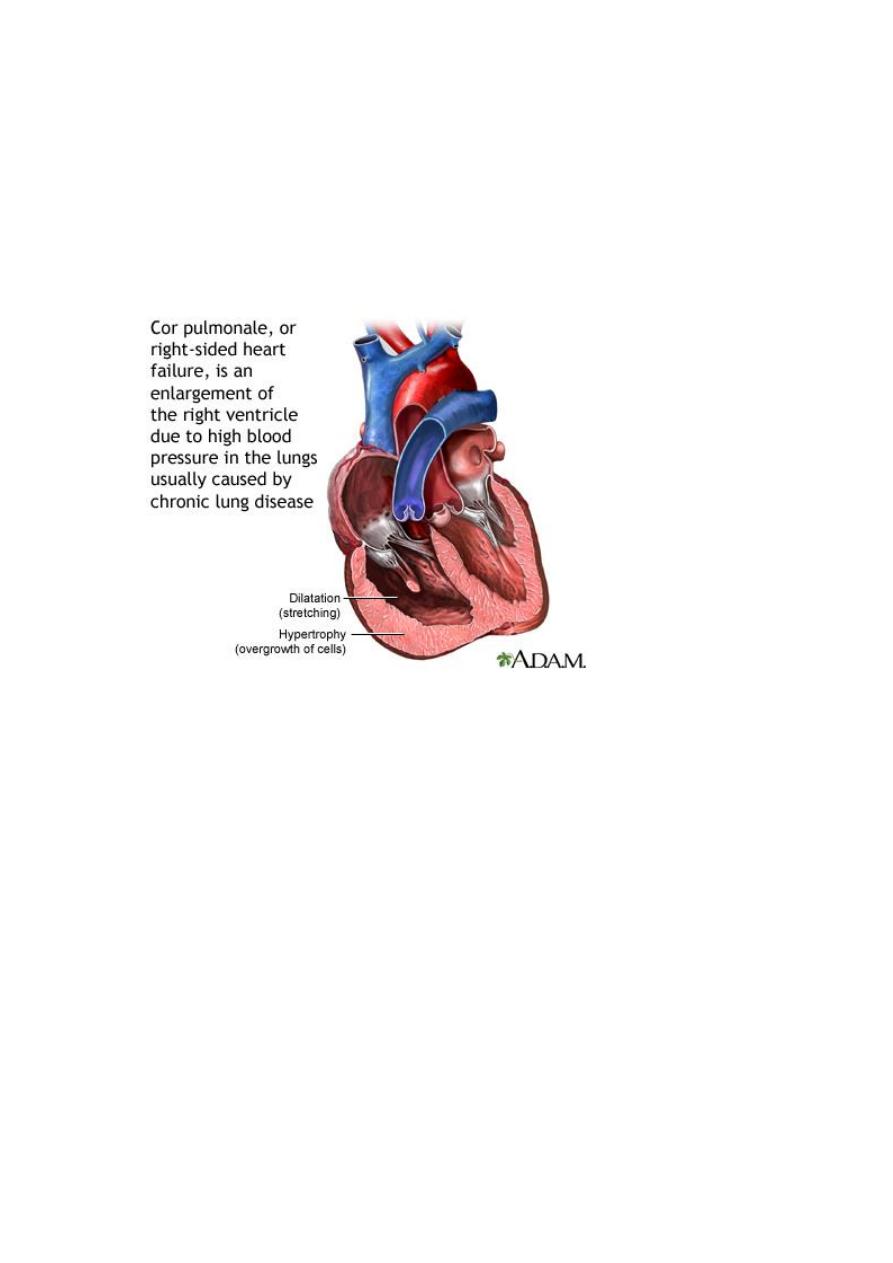
after massive pulmonary embolism the heart
may appear normal in size . Chronic cor
pulmonale is characterized by right ventricular
and right atrial hypertrophy.
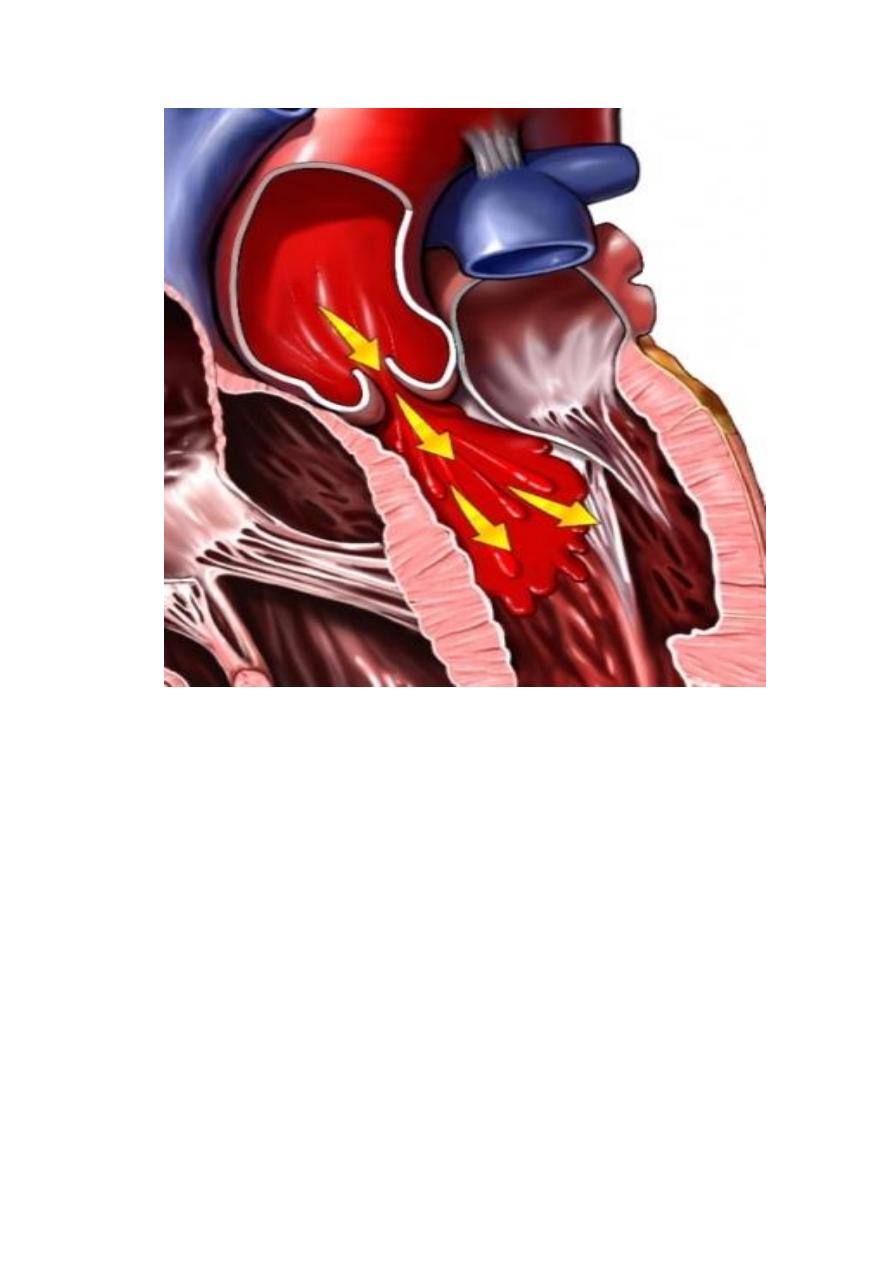
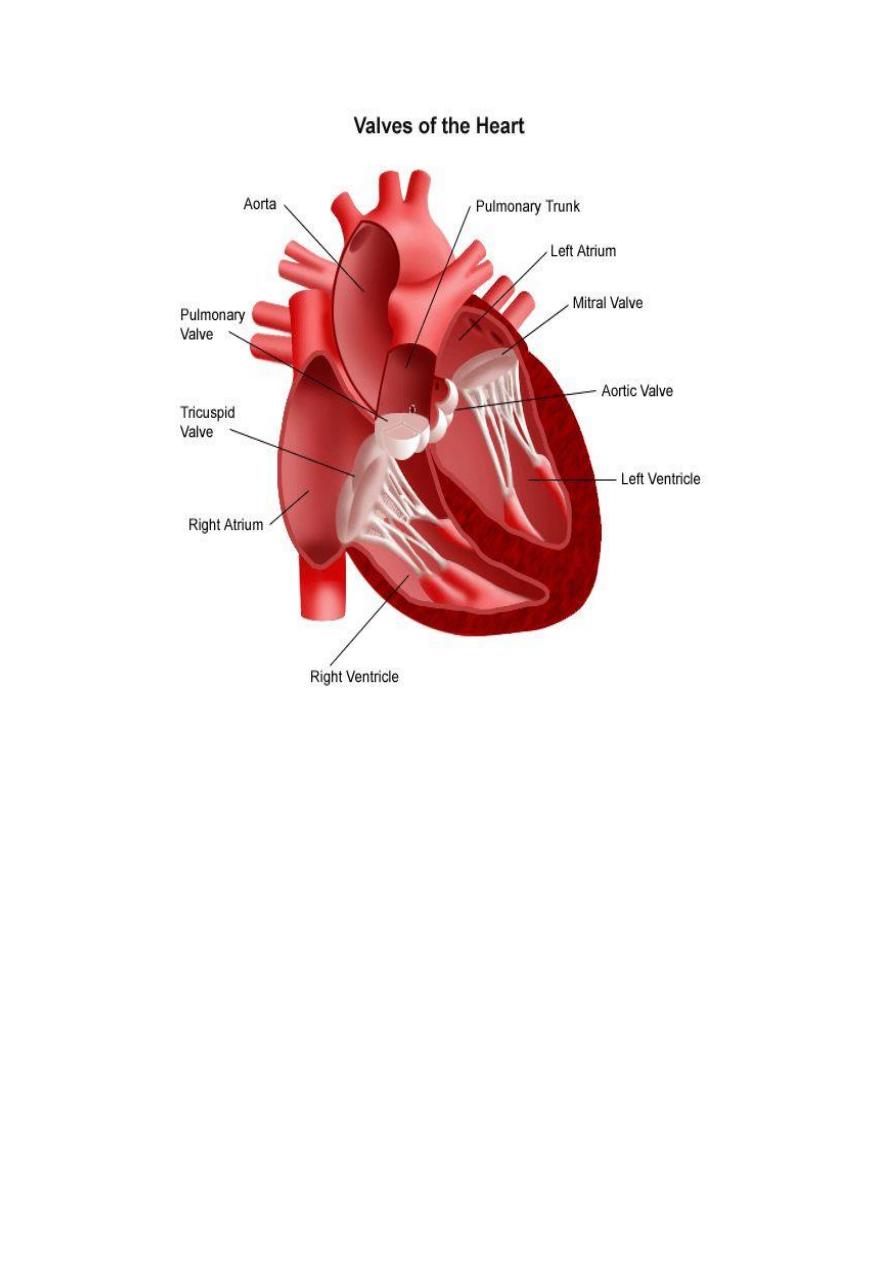
Valvular heart diseases:-
It's either congenital or acquired lesions,
some occur in isolation and other in
association with other heart diseases.
The abnormal cardiac valves cause disease by
two major mechanisms:-
1-They impose a major homodynamic
burden on the cardiac chambers by causing
obstruction (stenosis) or regurgitation
(incompetence) or sometimes combination
of two.
2- The abnormal valves are more
susceptible to infections and its
complications.
Mitral and aortic valves diseases are more
common than lesions of tricuspid and
pulmonic valves.
Rheumatic fever and heart diseases:
Rheumatic fever: is an acute,
immunologically mediated, multimultisytem
inflammatory disease that follows, after a
few weeks and episodes of group A
streptococcal pharyngitis.
Rheumatic fever may cause heart disease
during:
1- Acute phase (acute rheumatic carditis).
2- Chronic valvular deformities which's
become manifested after many years of
acute disease.

Rheumatic fever occur in only about 3/1 of
patients with group A streptococcal
pharyngitis.
Pathogenesis:-
Acute rheumatic fever is a hypersensitivity
reaction induced by group A streptococci,
the antibodies directed against the M
proteins of certain strains of streptococci
cross react with tissue glycoproteins in the
heart, joints and other tissues, the onset of
symptoms 2 to 3 weeks after infection and
the absence of streptococci from the lesions
support the concept that R.F result from
immune response against the bacteria.
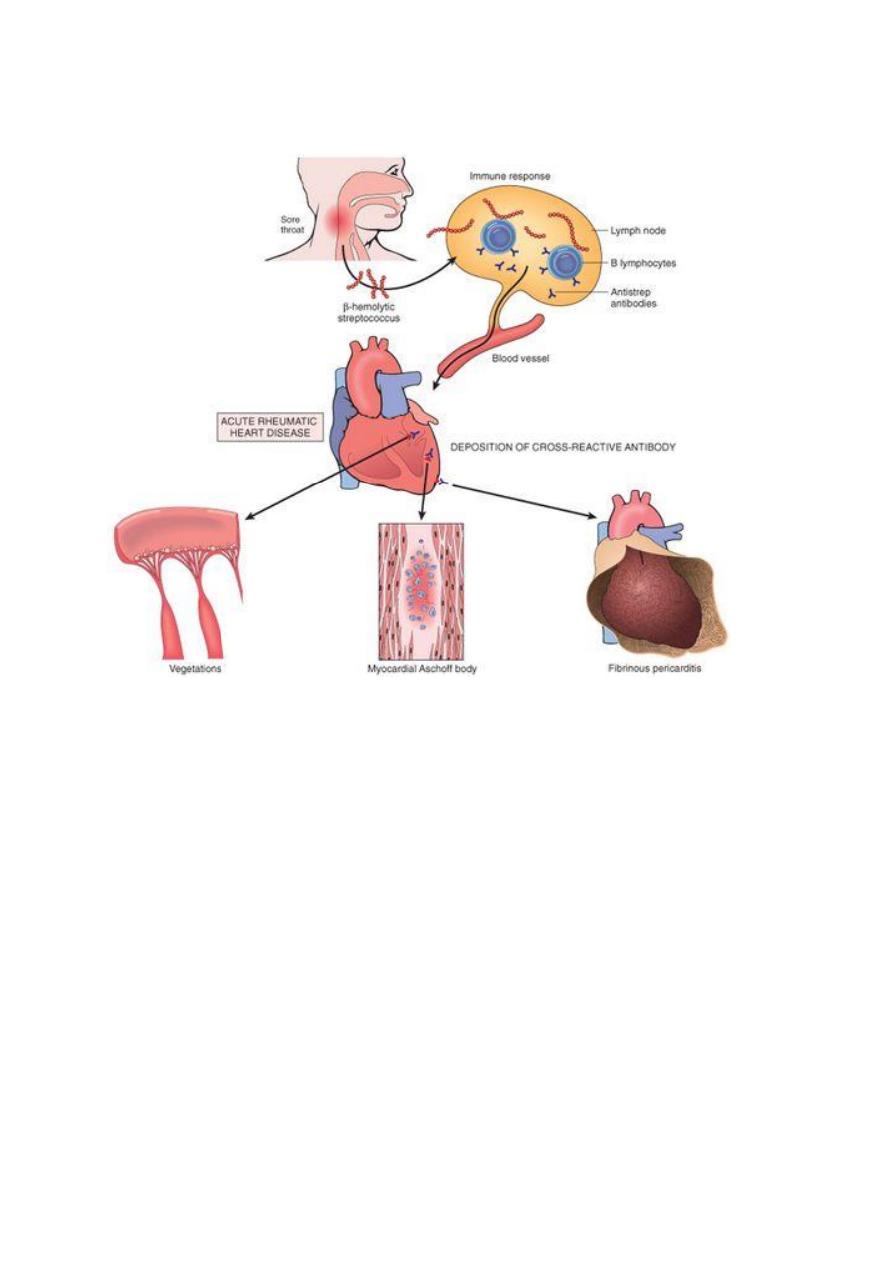
Morphology:-
Acute rheumatic carditis is characterized by
inflammatory changes in all 3 layers of the
heart, so it's designated a pancarditis, it's
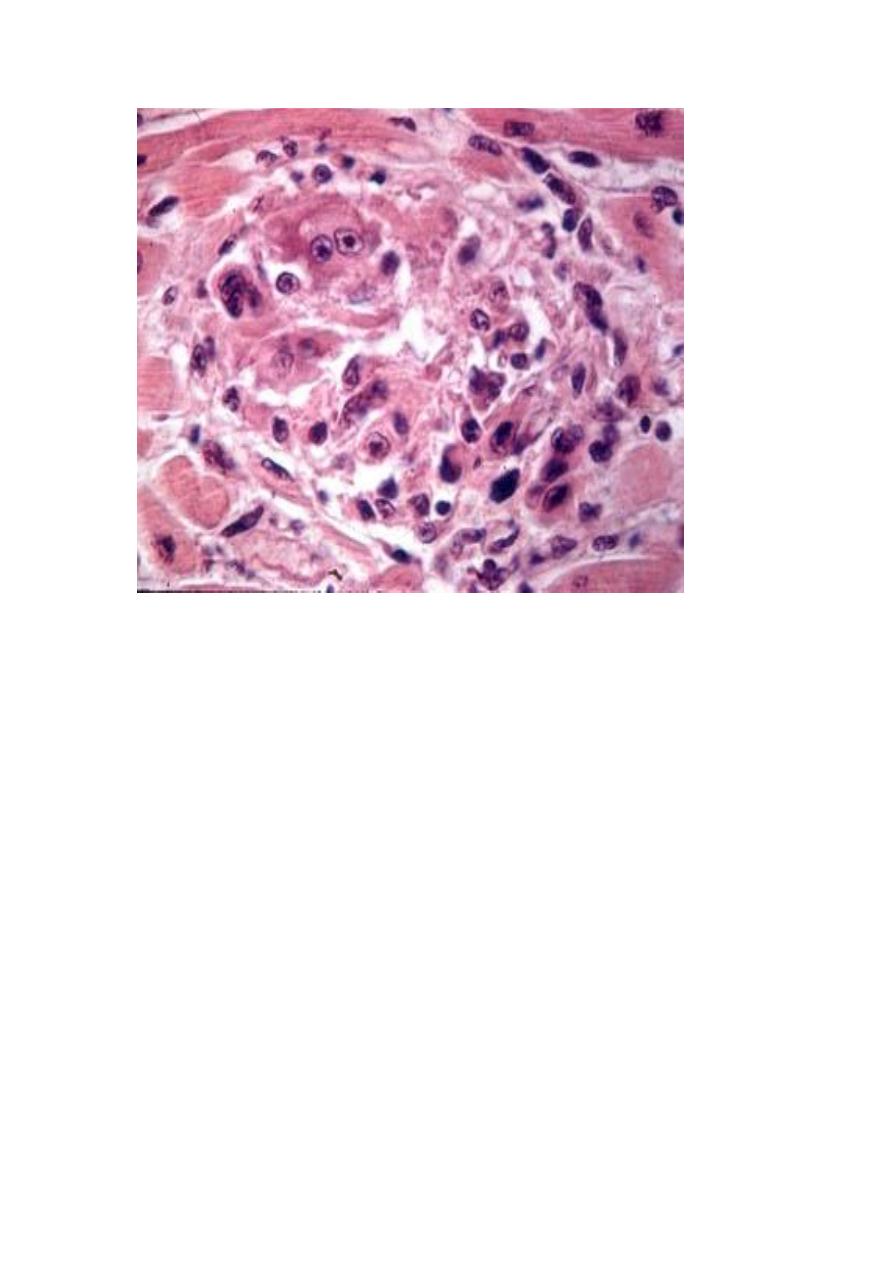
characterized by multiple foci of
inflammation within connective tissue of
the heart called Aschoff bodies: a
granuloma which contains a central focus of
fibrinoid necrosis, surrounded by a chronic
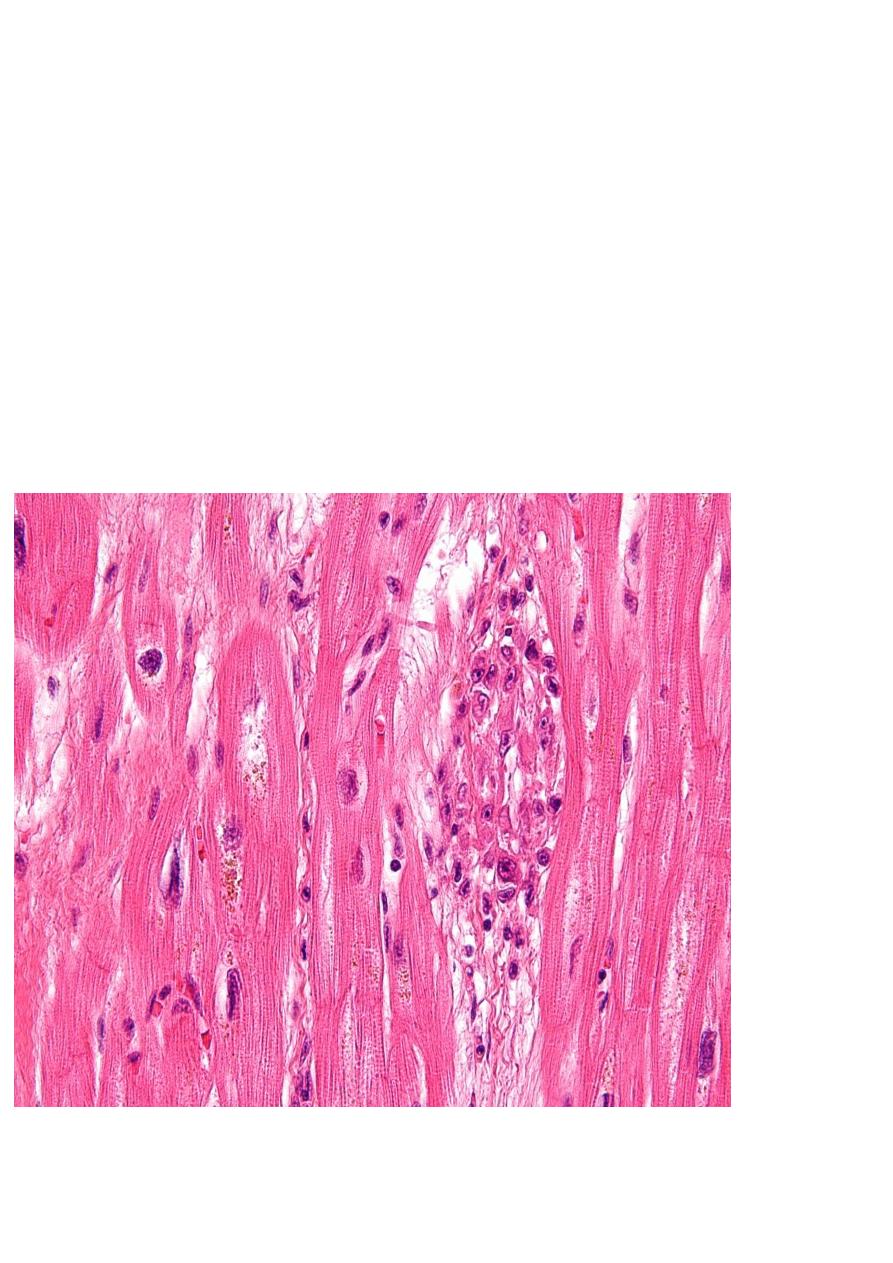
mononuclear inflammatory cells and some
large histeocytes with prominent nucleoli in
myocardium in addition to presence of
Aschoff bodies, there are diffuse interstitial
inflammatory infiltrates and in severe
myocarditis may cause generalized dilation
of cardiac chambers.
In endocardium involvement is common
and usually affect any valve but mitral and
aortic valves are common.
The valve is edematous, thickened and
show foci of fibrinoid necrosis but Aschoff
nodules are not common.
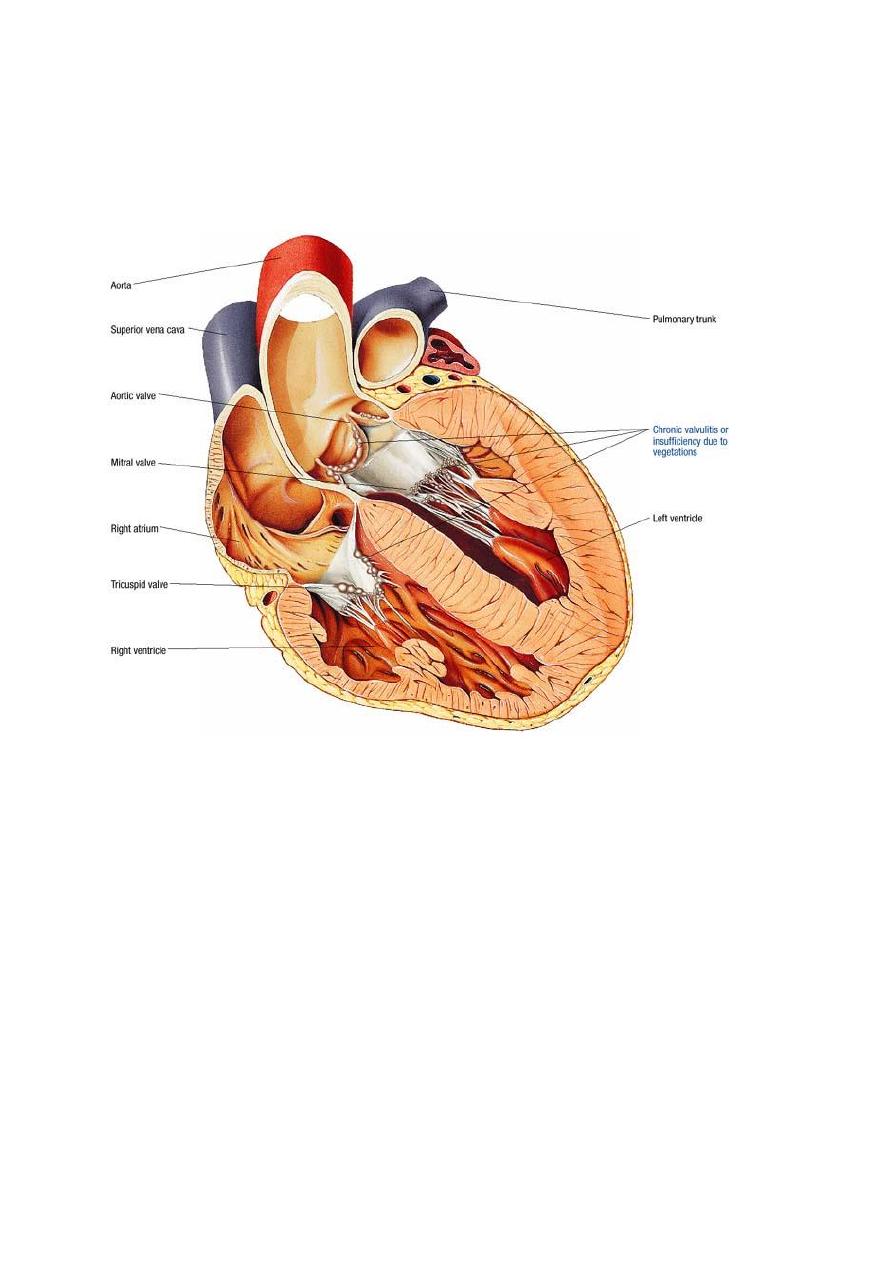
The acute inflammation of valve predispose
to the formation of small vegetations seen
as wart-like projections particularly along
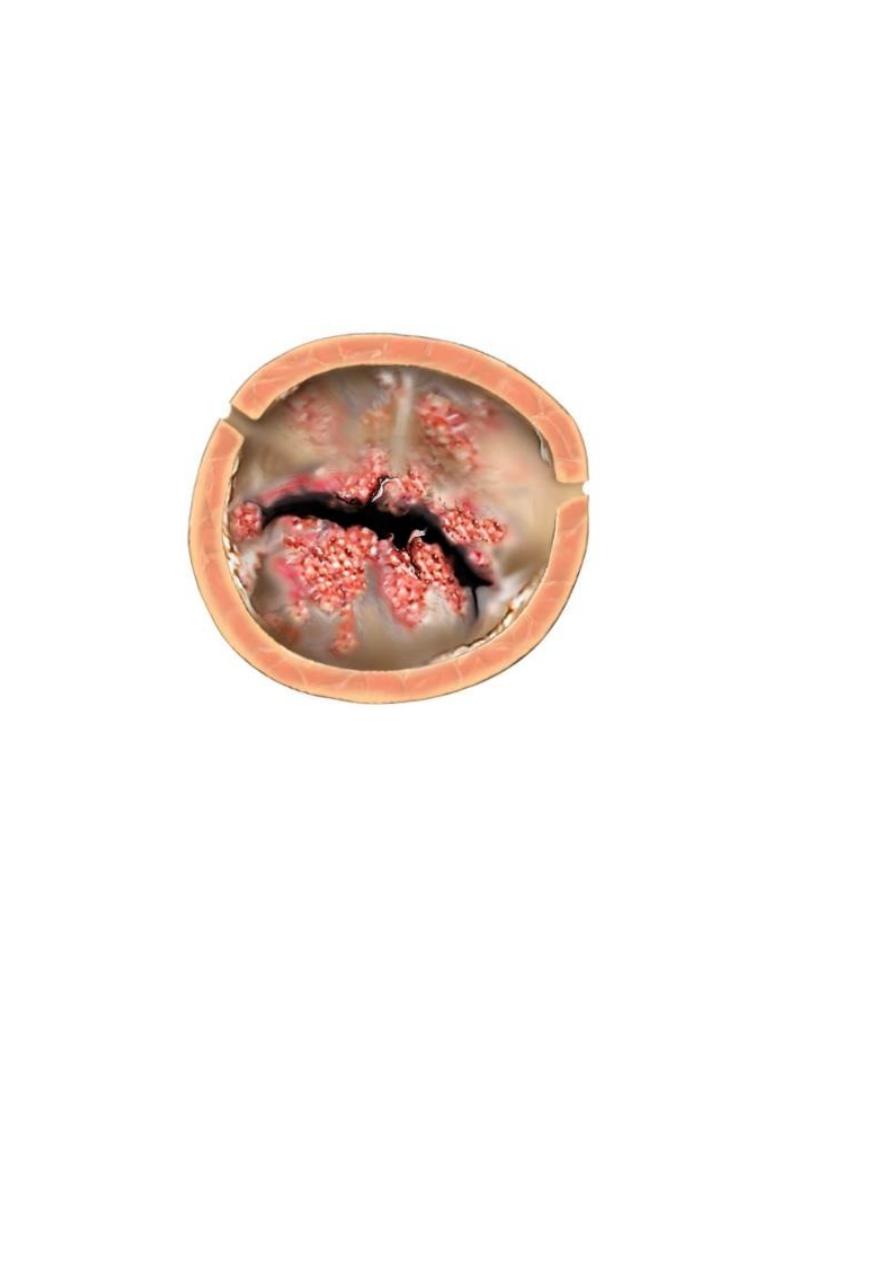
the lines of valves closure, these acute
changes may resolve without sequelae or
progress to chronic scarring and valvular
deformities.
Chronic rheumatic heart disease is
characterized by irreversible deformity of
one or more cardiac valves, scarring of the
valve leaflets may cause:-
1- Reduction in the diameters of valve
orifice (stenosis).

2- Prevent proper closure of valve leaflets
resulting in regurgitation of blood during
diastole.
3- Both stenosis and regurgitation.
Complications of rheumatic heart
diseases:
1- Valvular stenosis and regurgitation
increase the demands on the myocardium
because of increase pressure load or
volume load or both and cause heart
failure.
2- Damage to the valves predispose to
infective endocaridtis.
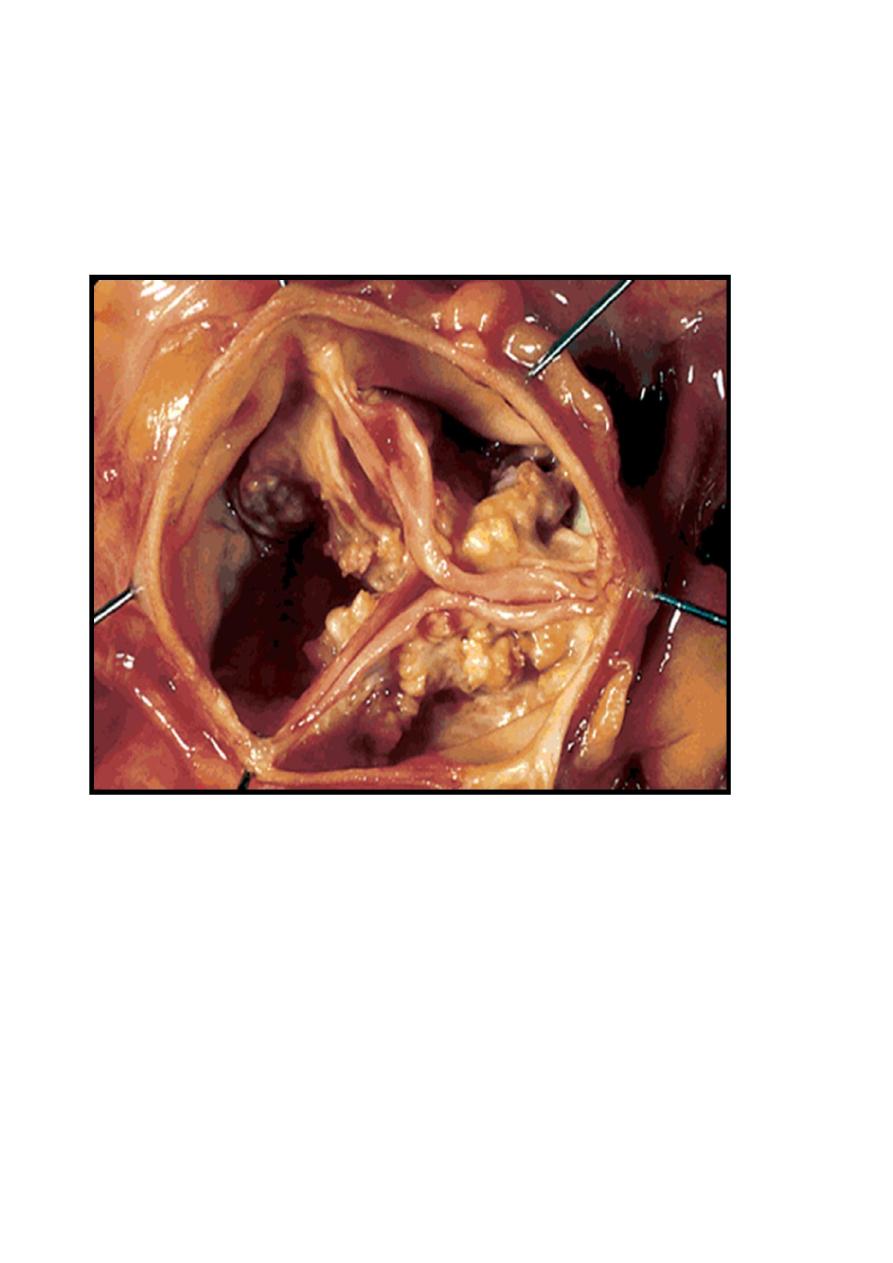
Chronic rheumatic mitral valvulitis:-
Stenosis is more than regurgitation and is
most common cause of mitral stenosis, the
valve leaflets and chordae tendineae are
thick, rigid and interadherent and orifice
narrowed to a slit-like channel, have a" fish-
mouth deformity", the left atrium is dilated
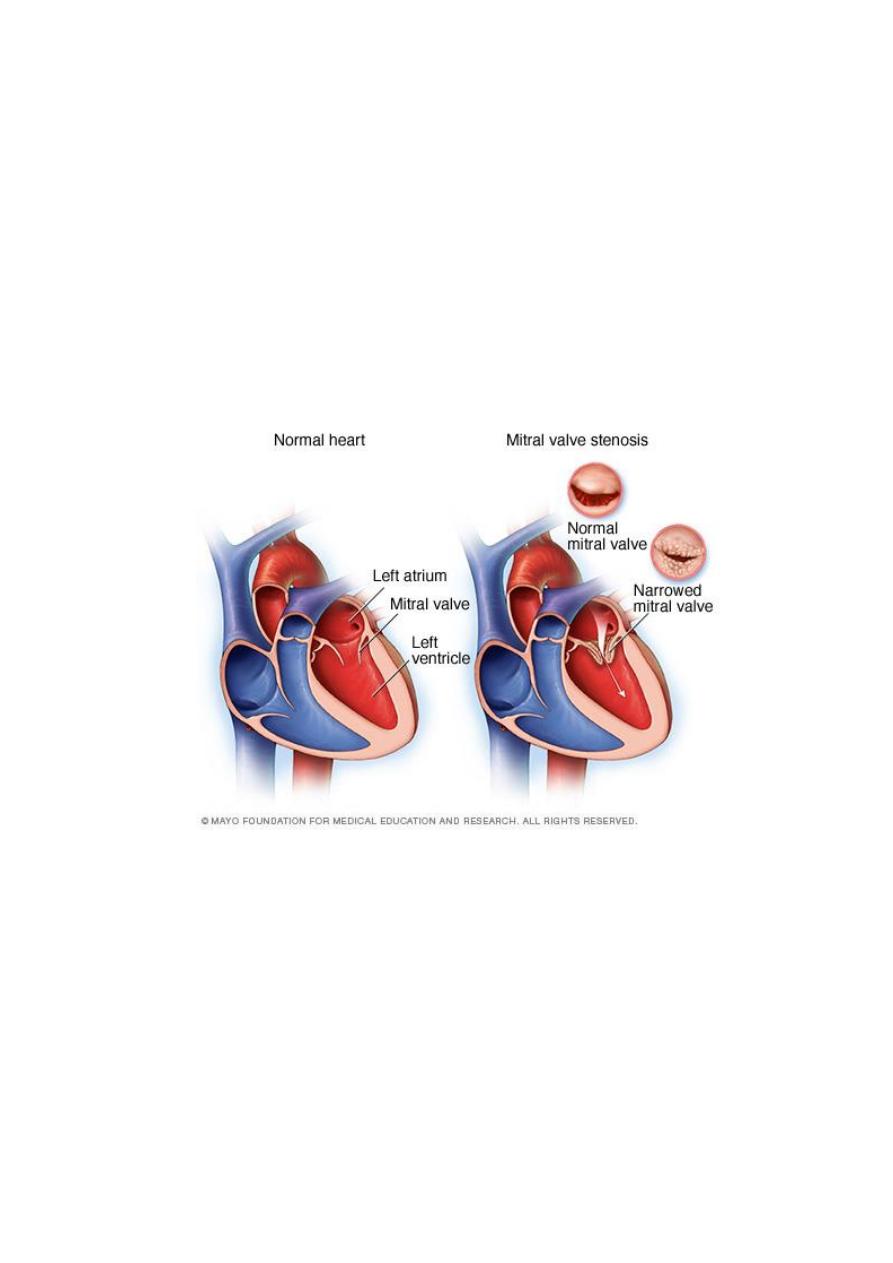
and hypertrophied, mural thrombi may be
present which's source of systemic emboli.
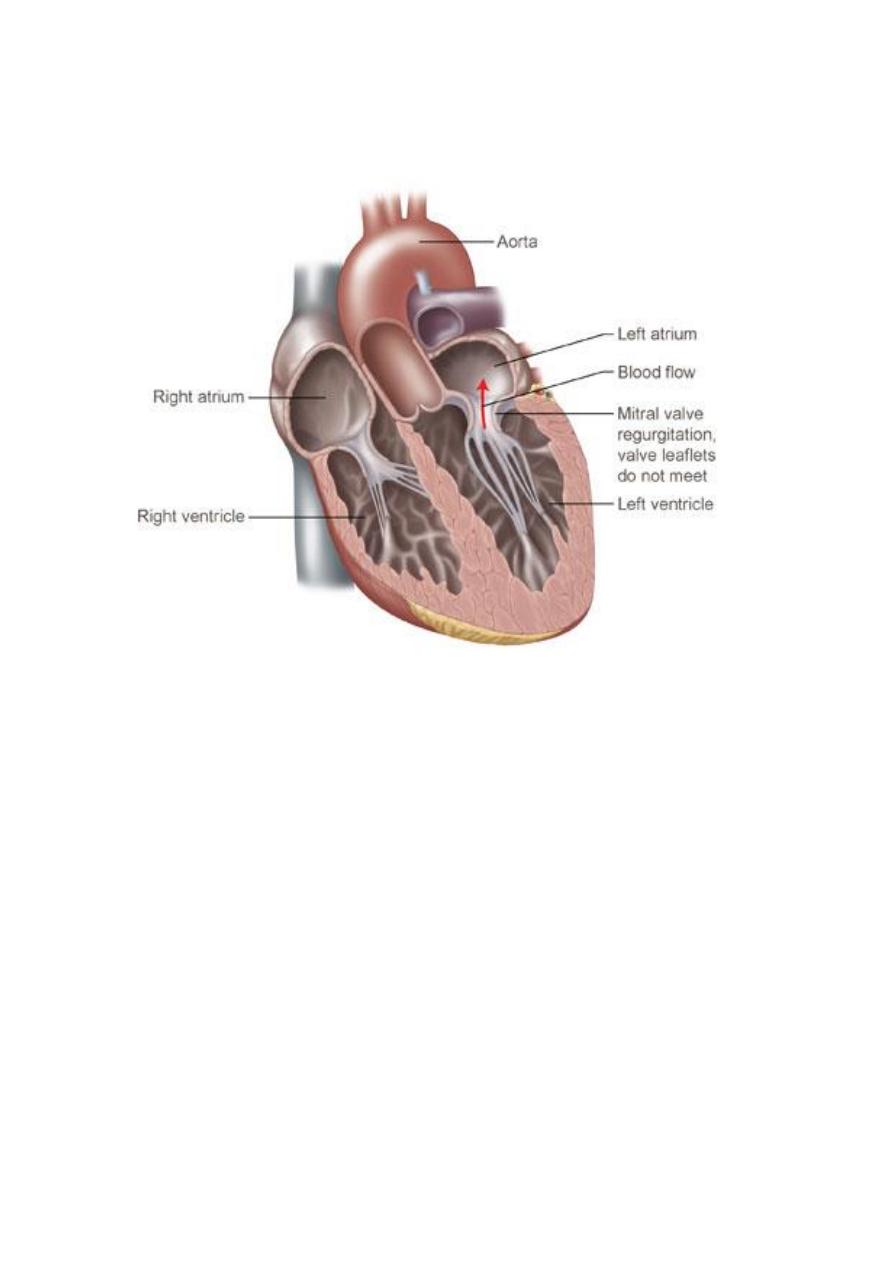
In mitral regurgitation, the deformed mitral
leaflets are retracted and the added volume
load on the left ventricle causes left
ventricular dilation and hypertrophy.
Chronic aortic valvulitis:-
The valve cusps are thickened, firm and
adherent to each other, the orifice reduced
to a rigid, triangular channel.
Aortic stenosis places a pressure load on the
left ventricle, so undergoes concentric
hypertrophy, fibrosis of the valve leaflets
may also cause them to retract toward the
aortic wall result in aortic regurgitation.