
1
Fifth stage
radiology
Lec-1
د.هديل
28/11/2016
Bone disease
Bone Infection (Osteomytitis ) :
Osteomyelitis refers to inflammation of bone that is almost always due to infection,
typically bacterial. This article primarily deals with pyogenic osteomyelitis, which may be
acute or chronic .
Osteomyelitis can occur at any age. In those without specific risk factors, it is particularly
common between the ages of 2-12 years of age and is more common in males (M:F of
3:1)
.
In most instances, osteomyelitis results from haematogenous spread, although direct
extension from trauma and/or ulcers is also relatively common (especially in the feet of
diabetic patients) .
staphylococcus aureus: 80-90% of all infections .
Plain film being
positive only after 10-14 days from the initiation of the symptoms
Location
The location of osteomyelitis within a bone varies with age, on account of
changing blood supply
:
neonates: metaphysis and/or epiphysis
children: metaphysis
adults: epiphyses and subchondral regions .

2
Plain film
1.The earliest changes are seen in adjacent soft tissues +/- muscle outlines with swelling
and loss or blurring of normal fat planes.
2.changes may not be obvious until 5 to 7 days in children and 10 to 14 days in adults. After
this time a number of changes may be noted:
-
regional osteopaenia
-
periosteal reaction/thickening (periostitis): variable, and may appear aggressive including
formation of a Codman's triangle
focal bony lysis or cortical loss
-
endosteal scalloping
-
loss of bony trabecular architecture
- new bone apposition
In chronic or untreated cases
sequestrum dead bone represents deva scularization of a portion of bone
involucrum new bone formation represents a thick sheath of periosteal new bone
surrounding sequestrum
cloaca The cloaca is an opening in a involucrum which allows drainage of purulent and
necrotic material out of the dead bone. If the tract extends to the skin surface, the portion
extending beyond the involucrum to the skin surface is called a sinus tract

3
We have two special types of chronic OM :
Brodie’s abscess :A localized osteolytic lesion at the end of the long bone surrounded by
sclerosis
.
Gary’s osteomyelitis : Sclerosing osteomyelitis
.
Characterized by localized sclerosis in the shaft of long bone
.
DDX ostiod osteoma

4
Tuberculosis of the Bone:
-
Spread from infected joint.
-
Any bone affected but the spine is the most common site with predilection to the dorso
lumber area
.
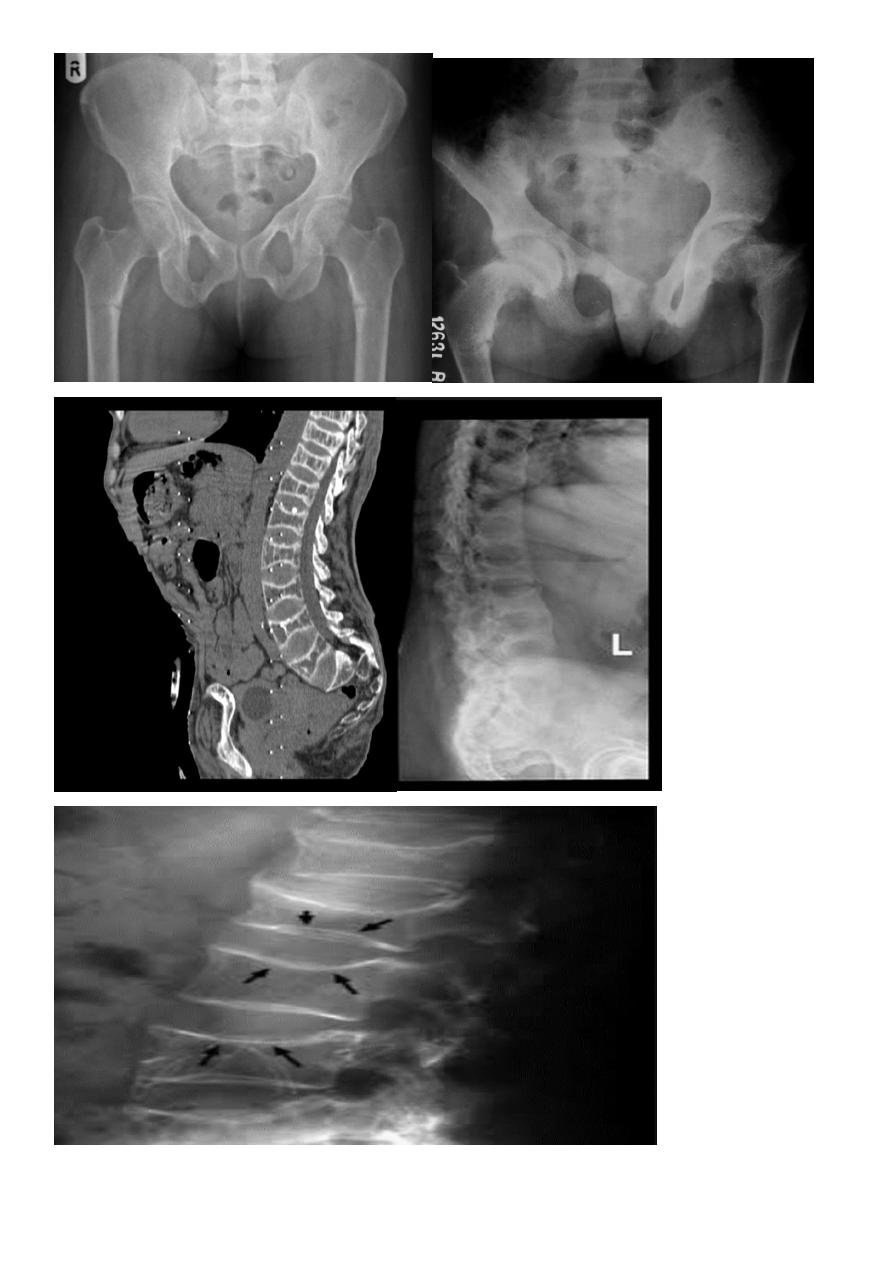
Findings in the spine (Pott’s Disease )
:
-Usually affect 2 adjacent vertebrae .
-There is erosion of the superior and inferior end plates .
-There is irregular narrowing of the joint space .
If not treated end with wedging of the vertebra (anterior loss of vertebral height)
End by angular kyphosis
.
-May be complicated with para –spinal cold abscess ,seen as a fusi form Para spinal soft
tissue on AP or PA view of the chest .
5
T.B of peripheral bone is not common and usually affect the small bones eg phalanx
T.B Dactylitis or spina ventosa
:
- There will be destruction of the phalanx - - expansion with soft tissue shadow around it .
Multiple Focal Bone Lesions:
Metastases
:
-Seen in bone with active haemopoiesis (spine, skull, ribs, pelvis, humeri ,
Femoral)
6
metastases site of predilections :
vertebral metastases (94%) causing primarily affection of the pedicle
.
intradural extramedullary metastases
(
5
%
)
intramedually metastases (1%)
Types of metastases
Osteolytic (most common causes) : neuroblastoma (in children), breast (adult female),
bronchus (adult male), thyroid, kidney, colon The vertebral pedicles are often involved.
Osteoblastic : prostate, breast , carcinoid , TCC of bladder,, neuroblastoma.
Mixed: breast, prostate, lymphoma.
Solitary expansile bubbly metastases with soft tissue involvement: thyroid, kidney.
Bone metastases with sun burst periosteal reactions: prostate, retinoblastoma and
neuroblastoma .
7
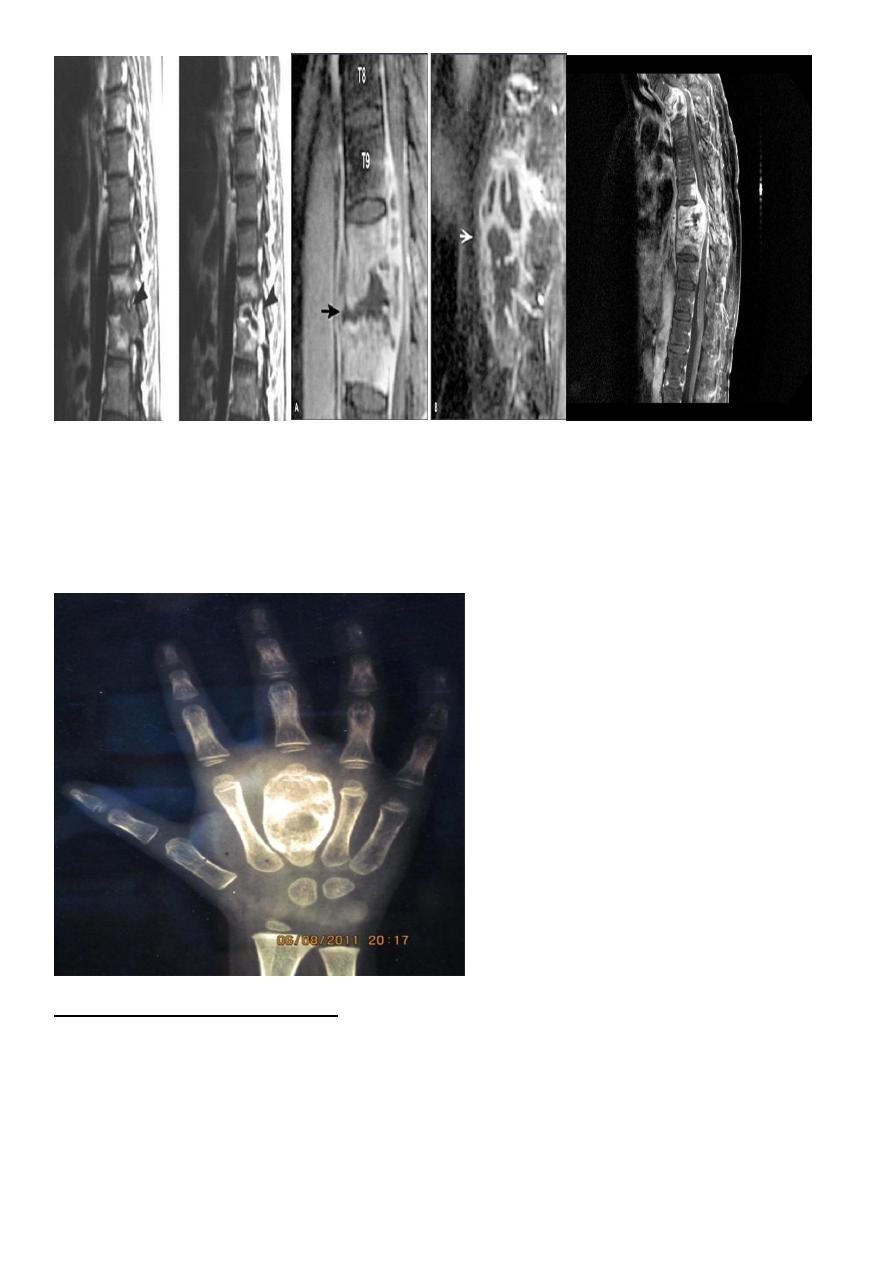
Multiple Myeloma
Site: axial skeleton.
Findings:
-Well demarcated lytic lesion occasionally with expansion of the bone.
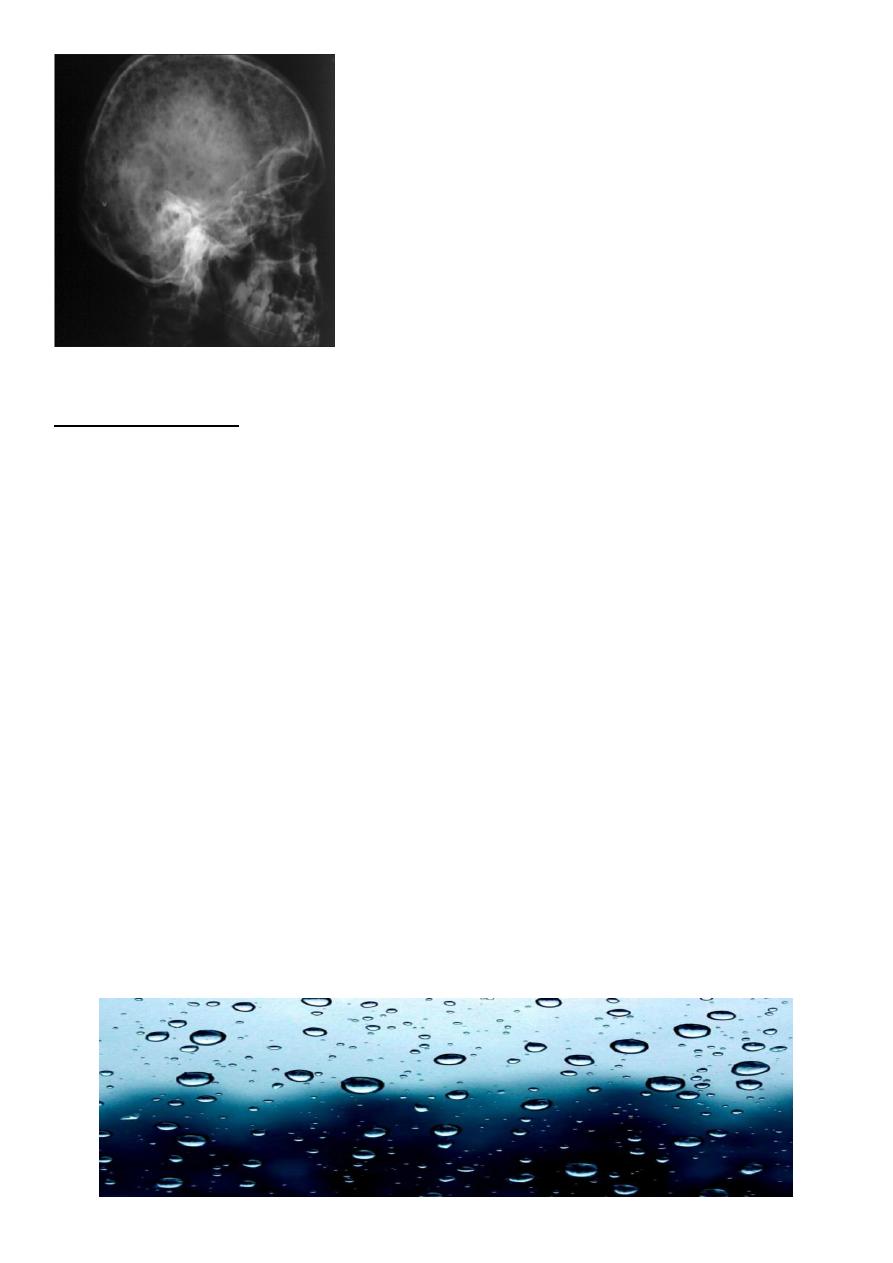
-In the skull called (rain drop) appearance (pathognomonic ).
-
In the spine Generalized form can resemble osteoporosis.
-
Solitary type (plasmacytoma) :
Represent early stage of MM; precede it by 1-20 years. Negative IgG spike in the serum. It
affects the thoracic, lumbar spine, pelvis, ribs, femora.
It is seen as expansile lytic ill-defined lesion with soft tissue mass.
-
Myeloma resembles metastases in everything except
:
it's more well defined, cause bone expansion and spares vertebral pedicle.
Rain drop appearance
8
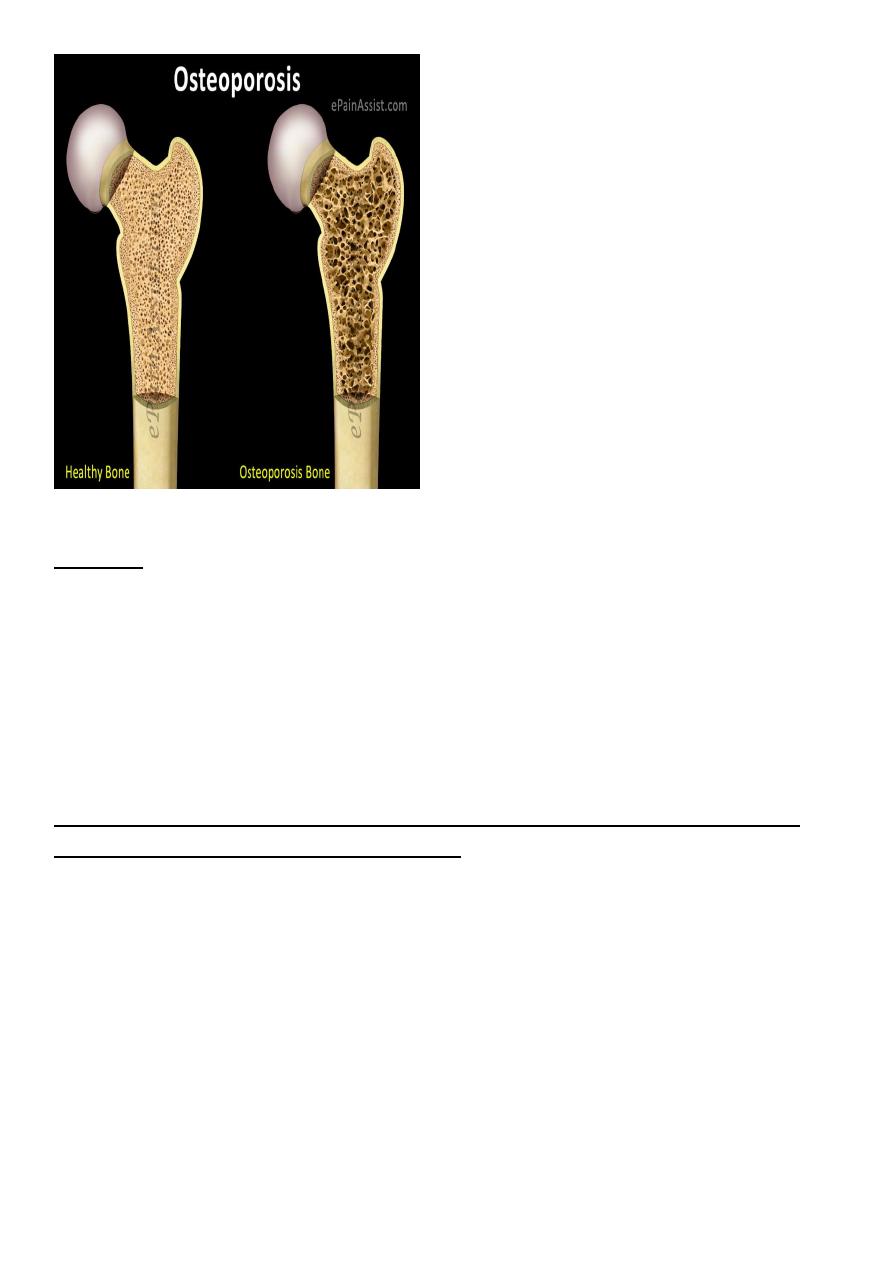
Osteoporosis
Pathophysiology: reduction in the bone matrix that subsequently results in reduced calcium
contents.
Causes:
-
Idiopathic: divided according to age of onset into juvenile, senile and post-menopausal
(most common). 50% of women over 60 years have osteoporosis.
-
Cushing syndrome & steroid therapy.
-
Disuse: occur after immobilization for fracture treatment or local pain.
- Sudeck's atrophy: disorder of the sympathetic nervous system where sever osteoporosis
and soft tissue edema occur disproportionate to the trauma or the degree of disuse.
9
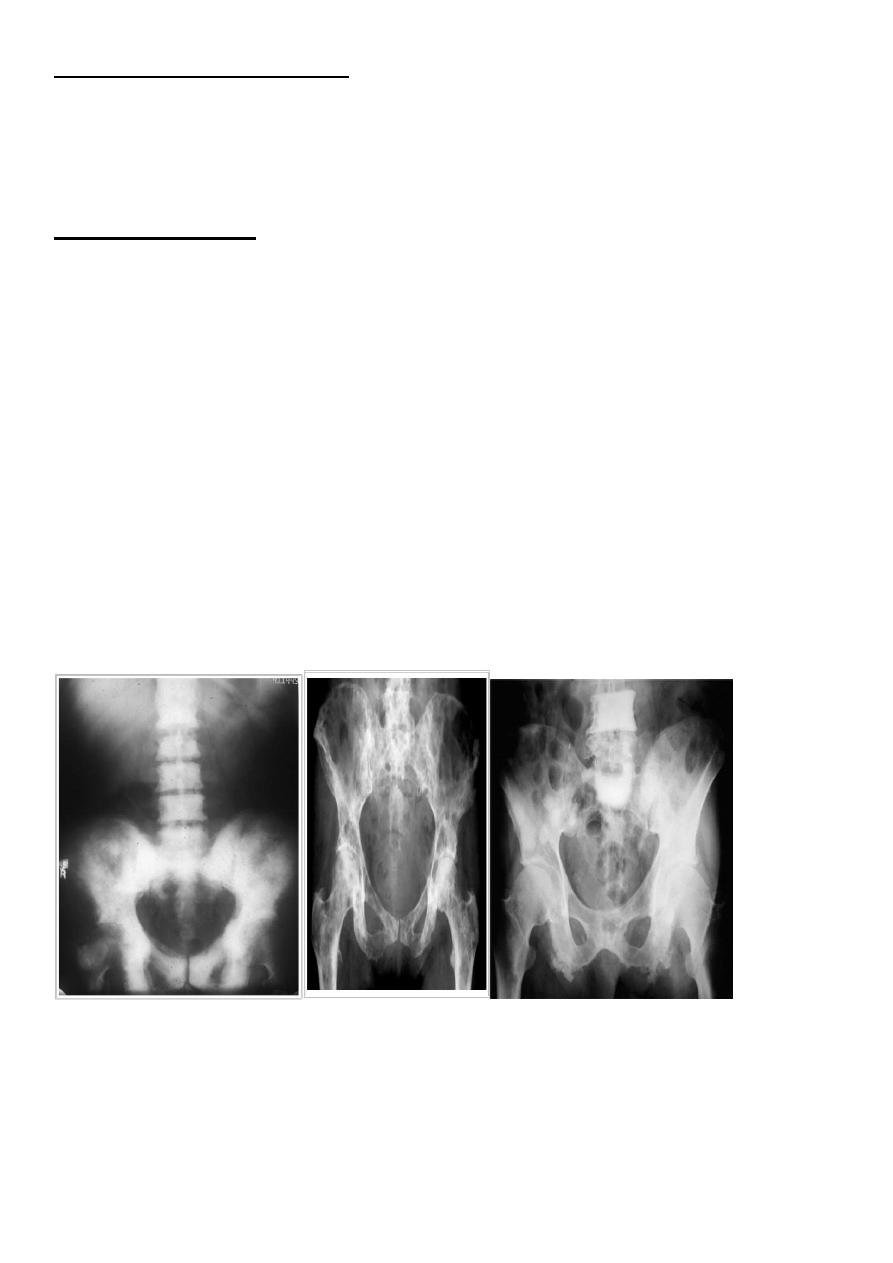
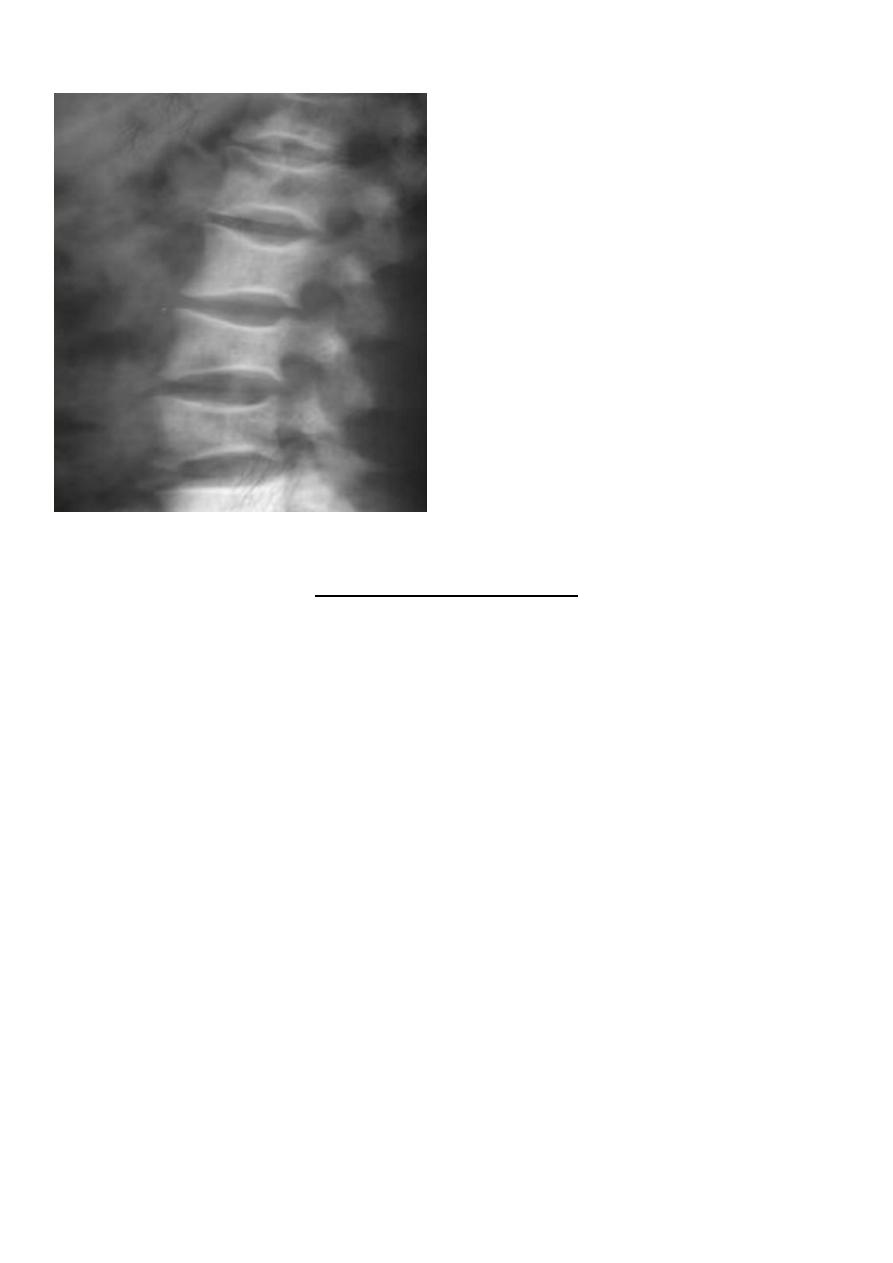
Findings:
-
the changes are best seen in the spine
-
Overall reduction in bone density with clear penciled in cortex.
-
Collapse of the vertebral bodies that represent compression fracture resulting In wedged
vertebra with widening of the disc space.
Long bones appear with thin cortex and resorption of many trabeculae but those that
remain stands out clearly.
The diagnosis of osteoporosis need to be made after the exclusion of other
possible causes of reduced bone density:
Metastatic carcinoma.
Multiple myeloma.
Hyperparathyroidism.
Osteomalacia.
Bone mass assessed by quantitative CT or by dual energy X-ray( DEXA scan )
11
Postmenopausal osteoporosis.
Rickets and Osteomalacia:
Pathophysiology: poor mineralization of osteoid. If occur before epiphyseal closure then it
is rickets, after that called osteomalacia.
Causes:
-Dietary deficiency of vit. D, lack of exposure to sun light.
-
Malabsorption.
-
Renal disorders.
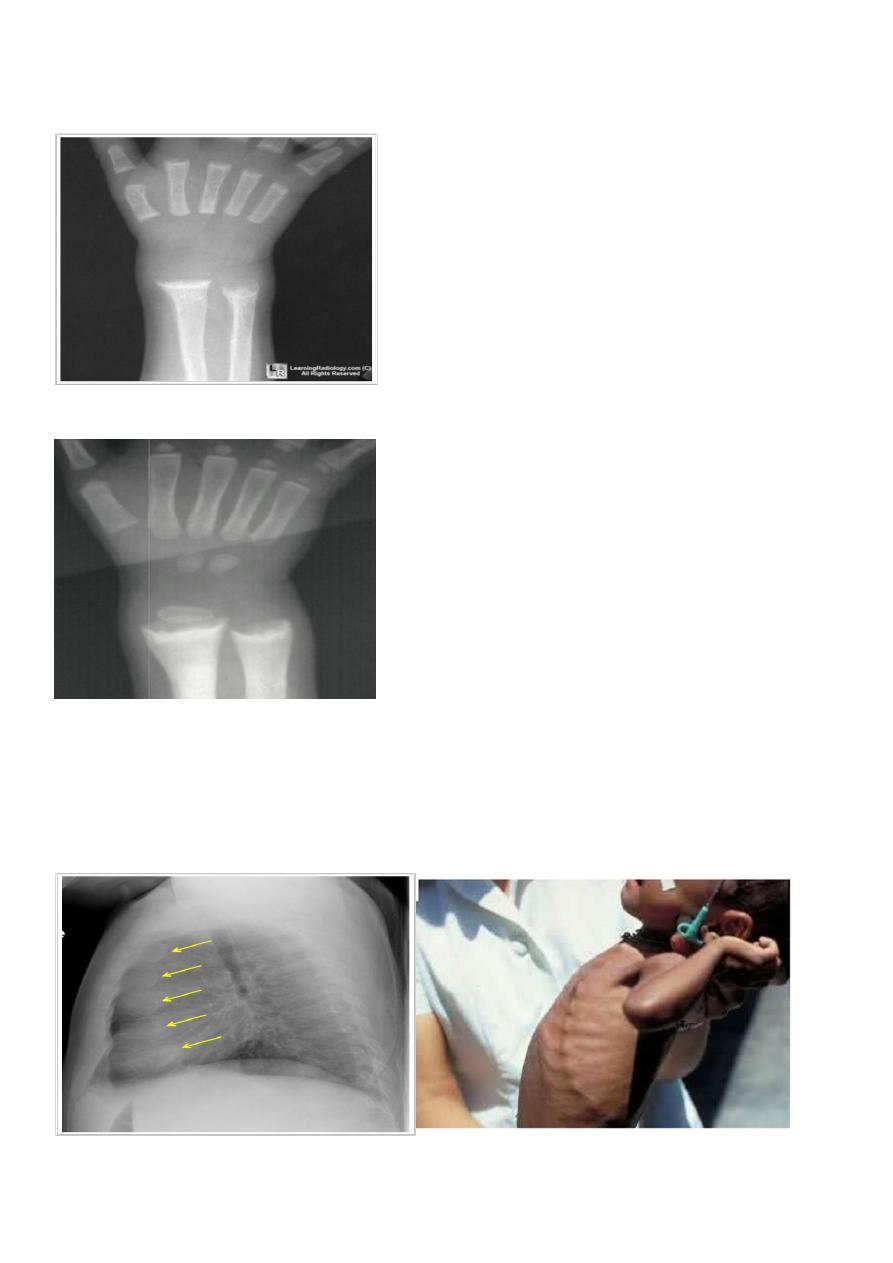
Findings in rickets : the findings are maximum at areas of bone growth so best seen at the
knee, wrist & ankles :
-Deficient zone of provisional calcification , the metaphysis is wide , irregularly mineralized
(frayed) and cupped
.
-Increased distance between the growing epiphysis & metaphysis.
-Generalized decrease in bone density.
-Deformity of bones due to softening (bossing and bowing ).
-Greenstick fractures are common.
-Rackety rosary of the ribs .
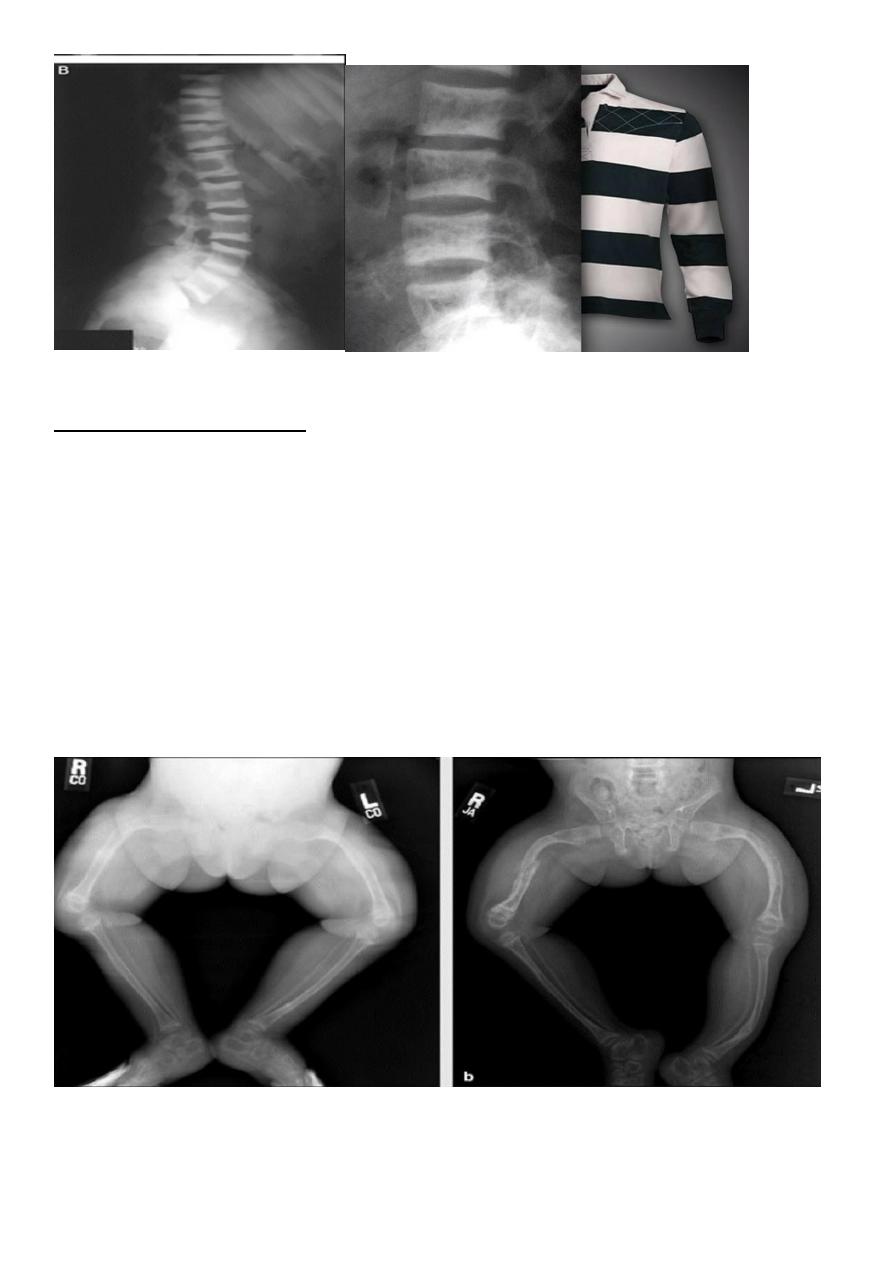
11
Rickets. There is splaying of all of the visible metaphysis, with
widening of the epiphyseal plates.
Rickets. There is obvious 'fraying' of the visible metaphysis
Rickety rosary. Widening of the anterior ribs is clearly demonsterated
(arrows)..
12
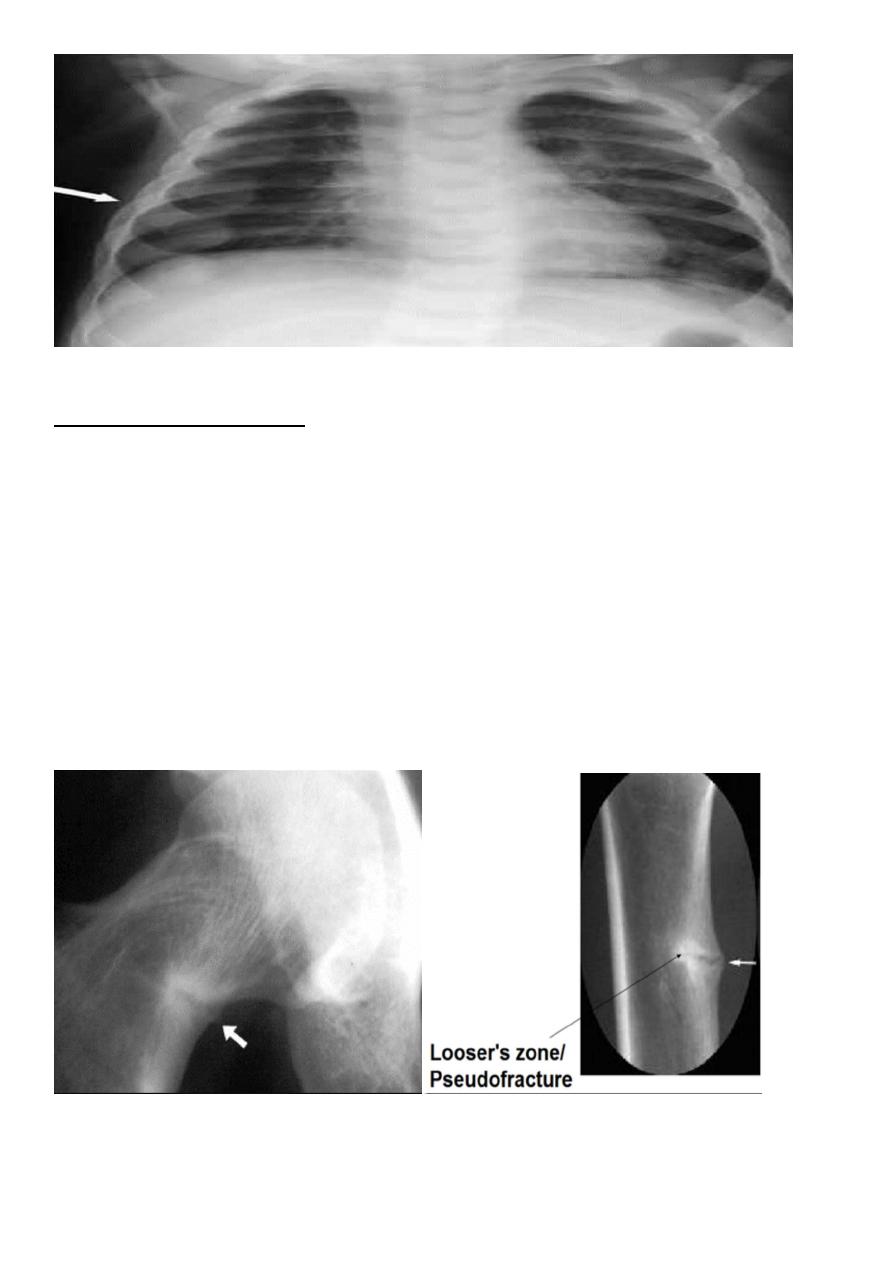
Findings in osteomalacia:
-
Decrease bone density.
-
Thin cortex & trabeculae.
-
Looser's zones: these are thin short lucent lines with sclerotic margins running across the
cortex at right angle, best seen in the scapula, medial aspect of the femoral neck & pubic
rami.
-
Vertebral collapse resulting in biconcave vertebra with widened disc (codfish appearance
).
-Bowing of the femur.
-In severe cases the pelvic side walls bend inwards resulting in tri radiate pelvis.
13

14
Hyperparathyroidism:
Tumors of the parathyroid glands cause
primary hyperparathyroidism
while patients with chronic renal failure will develop
secondary hyperparathyroidism.
Findings:
-Subperiosteal bone resorption, this is the hallmark of the disease seen particularly in the
radial aspect of the middle phalanges
-resorption of the terminal tuft of terminal phalanges & outer end of the clavicle.
-Decrease bone density with loss of corticomedullary differentiation.
-
Vascular calcification (more common in the secondary type) soft tissue calcification,
chondrocalcinosis.
Brown tumor: more common in the primary type seen as lytic expansile lesion in any bone
particularly the mandible & pelvis.
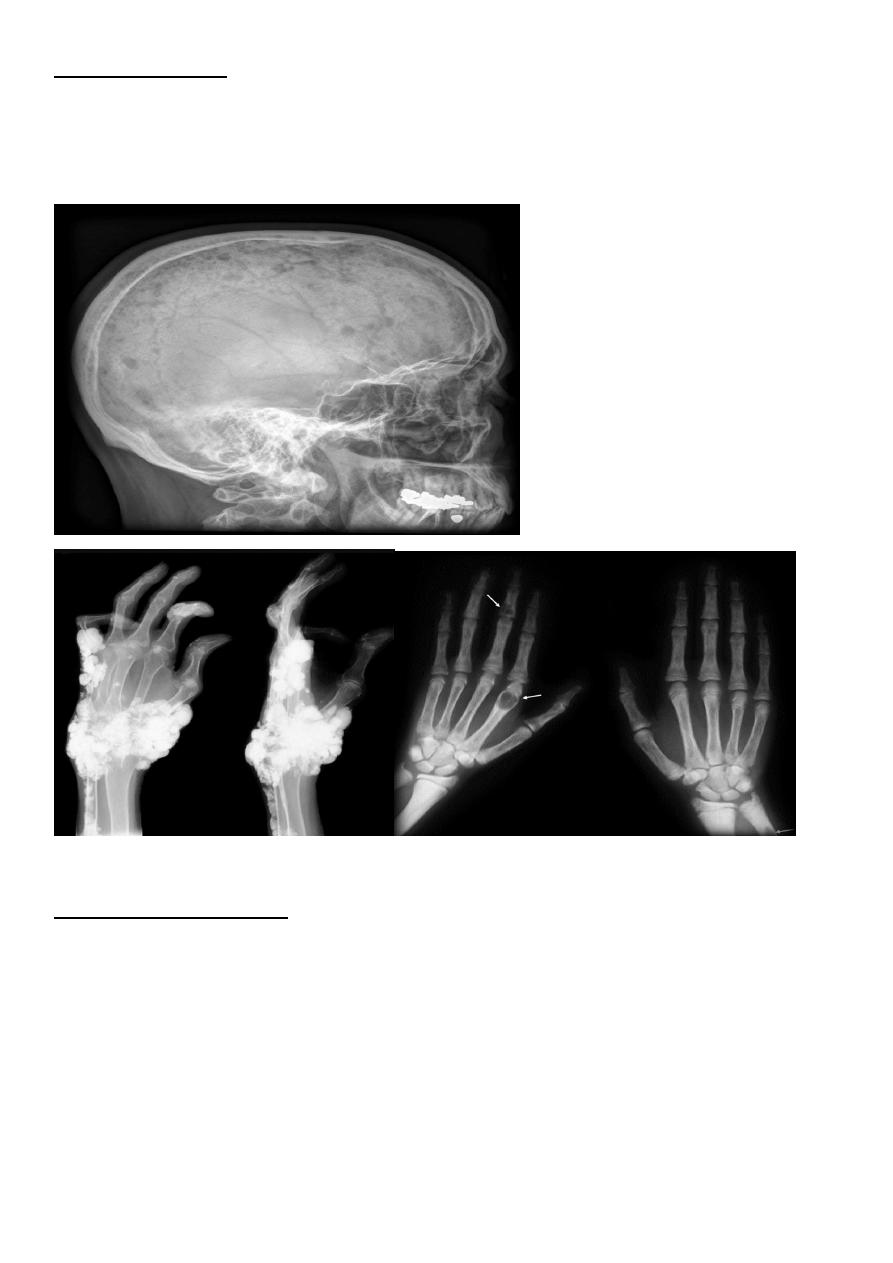
15
Salt and pepper sign
calvaria refers to multiple tiny hyper lucent areas in the skull vault caused by resorption of
trabecular bone .
There is loss of definition between the inner and outer tables of the skull and a ground-
glass appearance
Renal
Osteodystrophy:
Occurs in patients with chronic renal failure.
Findings:
Features of osteomalacia in adults & rickets in children.
Features of hyperparathyroidism.
Sclerosis: this is infrequent finding seen as bands of increased density in the spine named as
rugger jersey spine
&across the metaphysis of long bones.
16
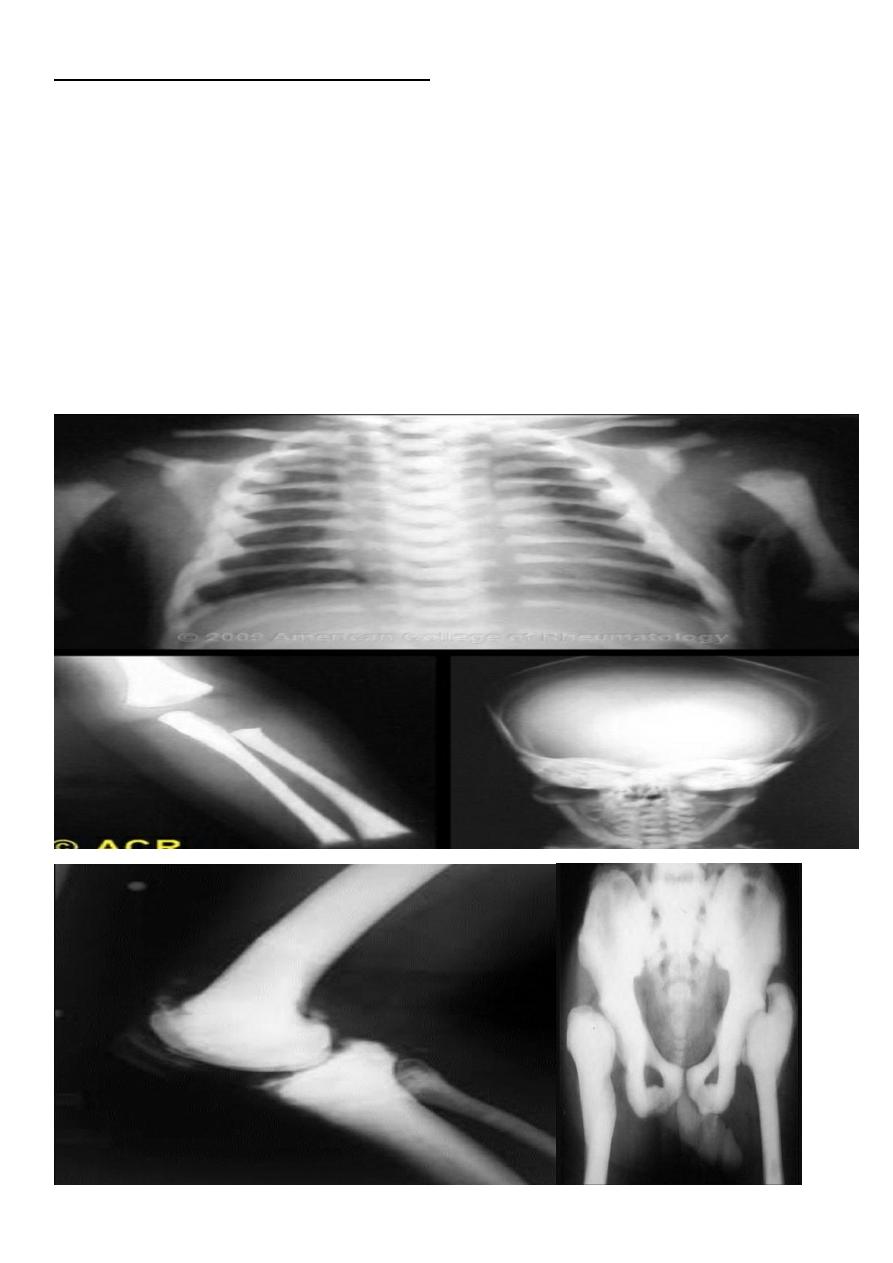
Osteogenisis imperficta :
Imperfect formation of the bone
.
Die within 2-3 years or still birth due to associated CHD.
*generalized decrease in bone density
*The medulla is very thin .
*Multiple bone deformity (large, small and flat bones ) due to multiple fractures and bizarre
healing
.
*widening of the sutures and (wormian bone formation )
Osteogenesis imperfecta. The child is stillborn. Multiple fractures
are demonstrated in the short and broad long bones, which are cystic
in appearance. Numerous rib fractures are seen.
17
Generalized increase in Bone Density:
-
Sclerotic metastases.
-
Osteopetrosis (Marble bone disease)
;
*congenital condition,
*the bone is brittle & easily fracture but heals normally.
Myelosclerosis :
-
Replacement of the bone marrow by fibrous tissue & progress to lay down new bone .
- Splenomegaly is invariably present.

18
Alteration in the Trabecular Pattern:
Hemolytic anemia
Thalassemia and sickle cell anemia result in bone hyperplasia.
Sickle cell anemia in addition causes infection & infarction.
Bone marrow hyperplasia(Thalassemia):
Thinning of cortex.
Increase thickness of bone with resorption of some trabeculae & increase, thickness of the
remaining.
Increase diploic space thickness with vertical striation resulting in hair on end appearance.
Enlargement of ribs, widening of the phalanges.
Infarction:
Infarction of the bone ends results in sclerosis and flattening of the femoral & humeral
heads
Medullary infarction appears as lytic areas with or without periosteal reaction. Healing
appears later as areas of irregular medullary calcification.

19
Changes in Bone Shape:
Achondroplasia:
Defective ossifications of bones formed in cartilages.
Shortening of the shaft of the long bones with distal metaphyseal flaring
.
Deformity of the pelvis (contracted pelvis).
Bullets like vertebrae due to anterior beaking
.
Diaphyseal achlasia
:
Multiple bony projections arise from the bone covered by cap that may calcify.
In the long bones they arise near the metaphysis & grow away from the nearby joint.
Transformation into chondro sarcoma suspected when there is rapid increase in size, pain,
ill-defined edge, extensive calcification in the soft tissue.

21
Acromegaly
The bone changes are maximum at the hands, feet & face.
Increase joint space due to overgrowth of cartilage.
Enlargement of the tufts of the terminal phalanges.
Enlargement of the pituitary fossa double floor sign.
Widening of the skull vault.
Enlargement of the sinuses & mastoid air cells.
Prognathisim : widening of angle between the body and ramus of the mandible.