1
Fifth stage
Radiology
Lec-2
د.هديل
5/12/2016
Bone Diseases
Imaging tools in bone diseases :
Plain bone radiographs
Radiological signs of bone diseases need longer time to develop in adults than in children .
Normal X-ray of the bone does not exclude the presence of pathology for example
osteomyelitis in children and scaphoid fracture in the first week.
Conventional radiological signs of bone diseases:
1-decreased bone density:
Focal : lytic area or area of bone destruction ,
Generalized : osteopenia (either osteoporosis or osteomalacia).
2-Increase bone density : sclerosis (focal or generalized).
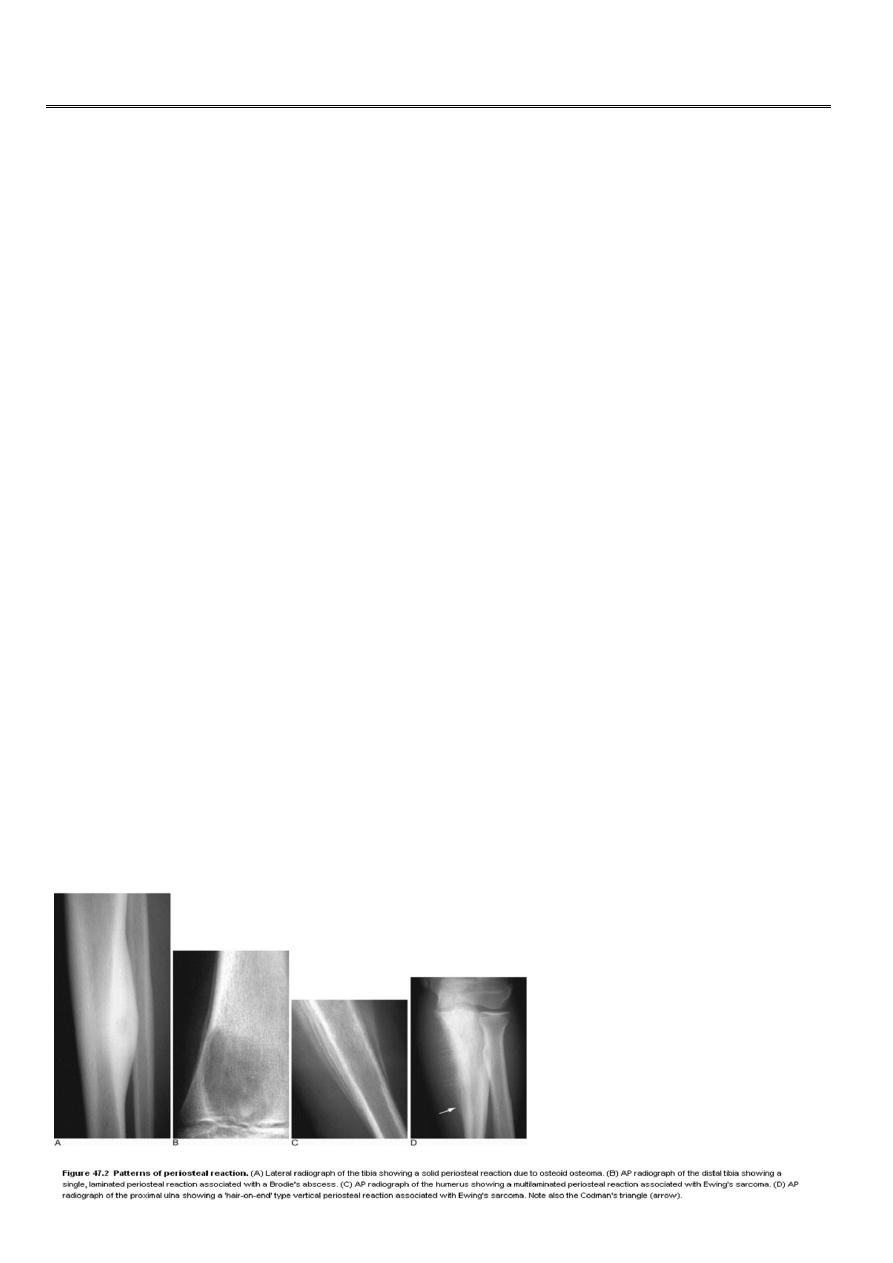
3 -
periosteal reaction
:
Definition : new bone formation by the periosteum ,
Normal periosteum is not visible.
The type of periosteal reaction does not correlate with specific diagnosis for e.g.
Codman's triangle seen in osteosarcoma may be seen in other aggressive lesions.

2
Causes of periosteal reaction :
Trauma
Infection
Inflammation
Tumors
Metabolic: ( thyroid achropachy, hypertrophic osteoarthropathy, hypervitaminosis A.)
Vascular ( venous stasis )
physiological (in 35% of infants between 1-6 m )
Congenital (syphilis, osteogenesis imperfecta. )
4- Cortical thickening :
Cortical thickening caused by lying down of new bone by the periosteum for long duration
of time,
It indicates slow process. The thickened cortex appears irregular and dense,
Causes: chronic osteomyelitis, stress fracture, healed trauma, and bone tumors as osteoid
osteoma.
5-Alteration of trabecular pattern:
Definition: reduction in the number of trabeculae with alteration in the remaining
trabeculae,
In osteoporosis, there is cortical thinning and trabeculae that remain become more
prominent than usual
In Paget's disease the trabeculae are thickened and extend into the compact cortex that
normally devoid of trabeculae.
6 -
Alteration in the shape of the bone:
As in osteogenesis imperfecta, acromegaly & expanding bone tumors.
3
7 -
Alteration of bone age:
The best site of assessment of bone age is at the wrist, hands, and in newborn the knee
joint
.
In cretinism there is delayed appearance of the epiphyseal bone centers.
Radionuclide bone scan
Tc99m- labelled with phosphate complex is a bone seeking agent, however it is also taken
up by soft tissue calcifications, areas of tissue damage, soft tissue tumors.
Given IV and excreted in urine.
Positive scan shown as increased uptake (hot areas): seen in ,
trauma, tumor, infection, infarction and Paget's disease.
Correlation with plain radiograph is frequently essential.
4
Indications: Tc m 99 Phosph
1-Detection of metastases.
2-Detection of osteomyelitis.
3-Determination if the lesion is solitary or multiple.
4-Investigation of clinically suspected bone lesion despite normal radiographs (this may
occur with metastases, trauma/stress injury, osteoid osteoma or early osteomyelitis).
5- Investigation of painful hip prosthesis.
6-Determination ( in equivocal cases) of whether an abnormality seen on radiograph is
significant or not (a positive bone scan makes it likely that a true bone lesion exists and a
negative one reduces the probability of disease considerably).
CT scan :
bone window setting is required
(Window width \window level 3000\450 ) for optimum results (for specific bone details)
.
- Reserved for selected cases :
1 -
Abnormality in complex bones as the spine, pelvis, face and skull.
2 -Determination of the local extent of bone tumor within & outside the bone when
planning conservative surgery.
3- 3D is useful in planning corrective surgery for fracture & bone deformity.
4- As a guide for bone biopsy.
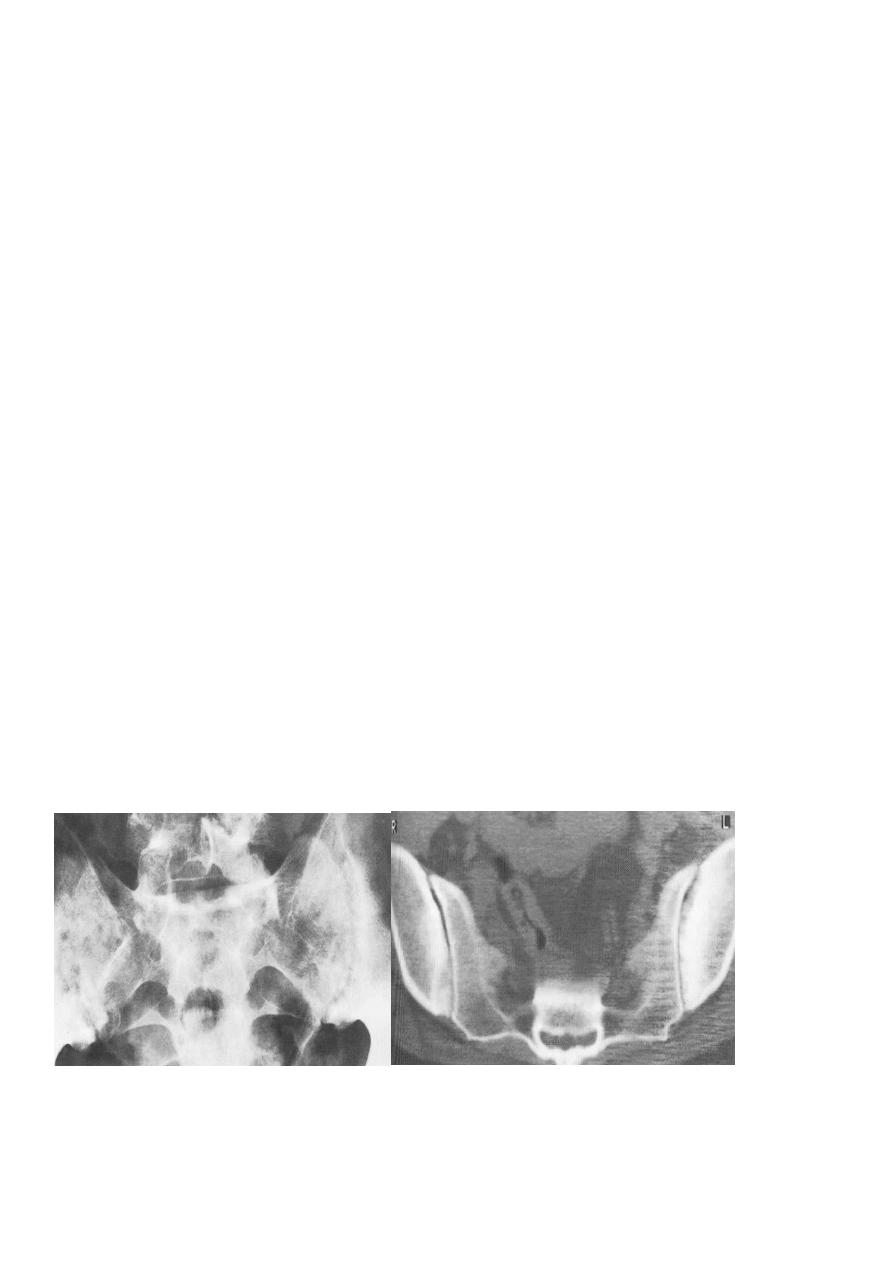
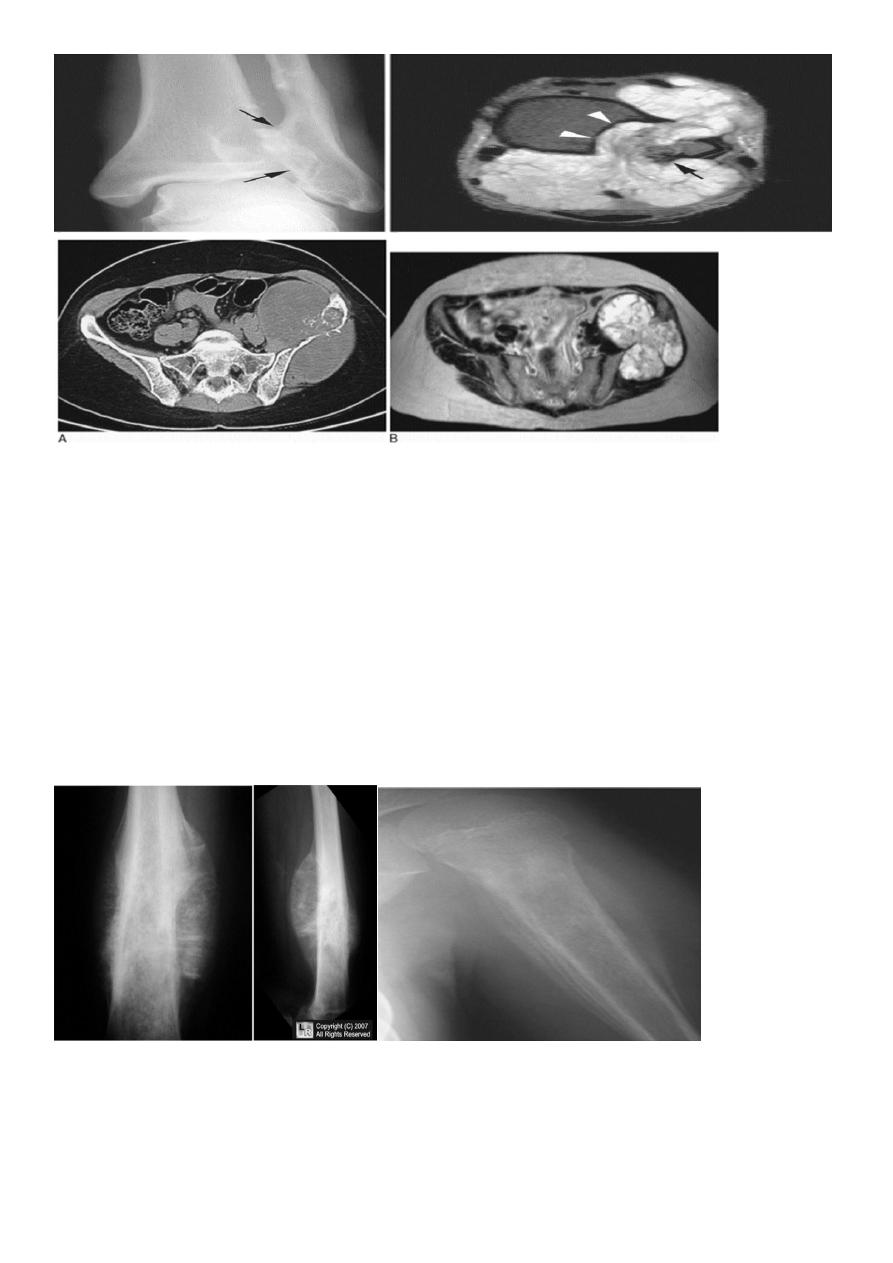
Ankylosing spondylitis-early
(A) Serrated margins
of sacroiliac joints and peri articular sclerosis.
(B) CT scanning demonstrates bilateral sacroiliitis
5
MRI :
Calcified structures produce signal void areas on MRI
Indications:
1 -
Excellent in showing the intra and extra-osseous extent of bone pathology .
2 -
Investigation of disc herniation and spinal stenosis.
3 -
Assessment of soft tissue masses.
4 -
Assessment of cartilage, ligaments and meniscal injury.
5- Diagnosis and assessment of avascular necrosis.
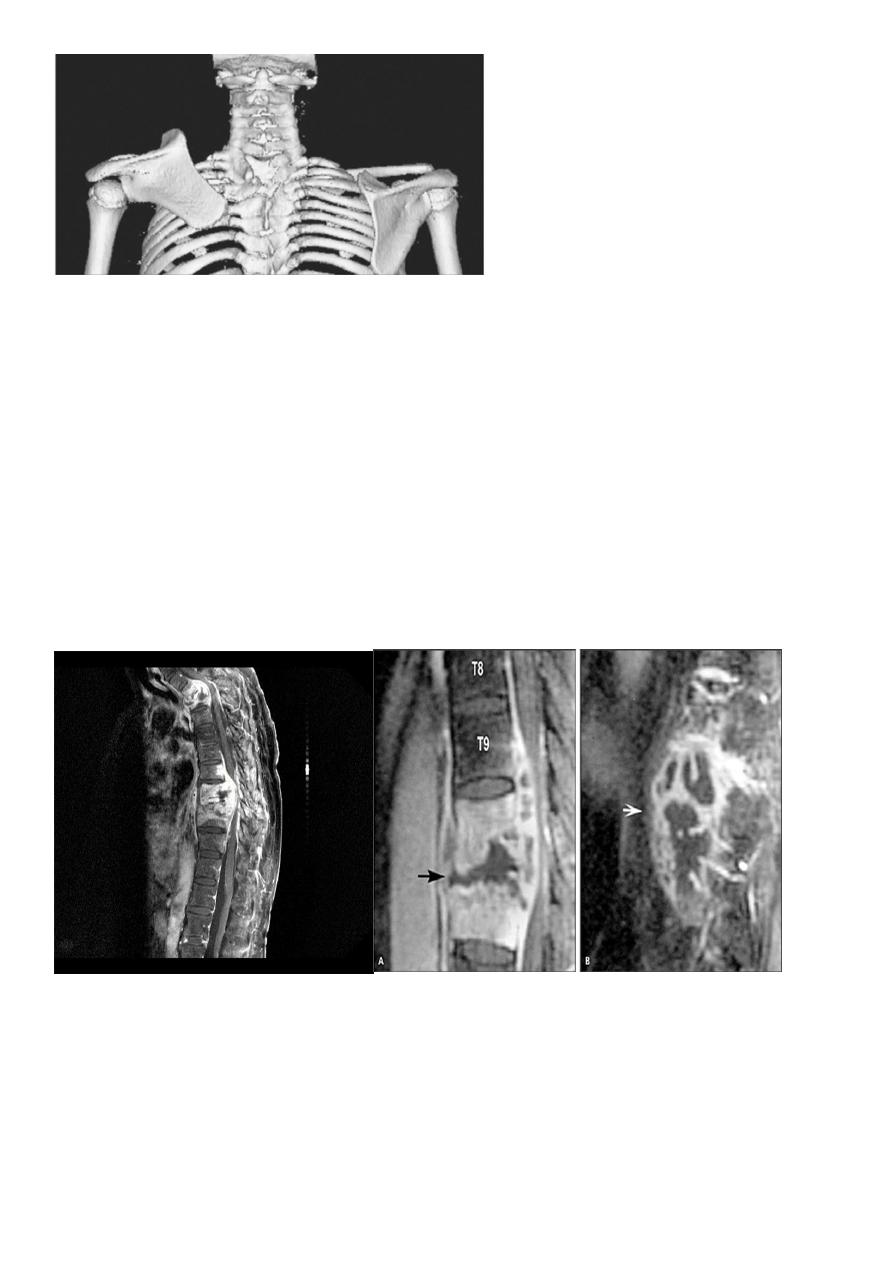
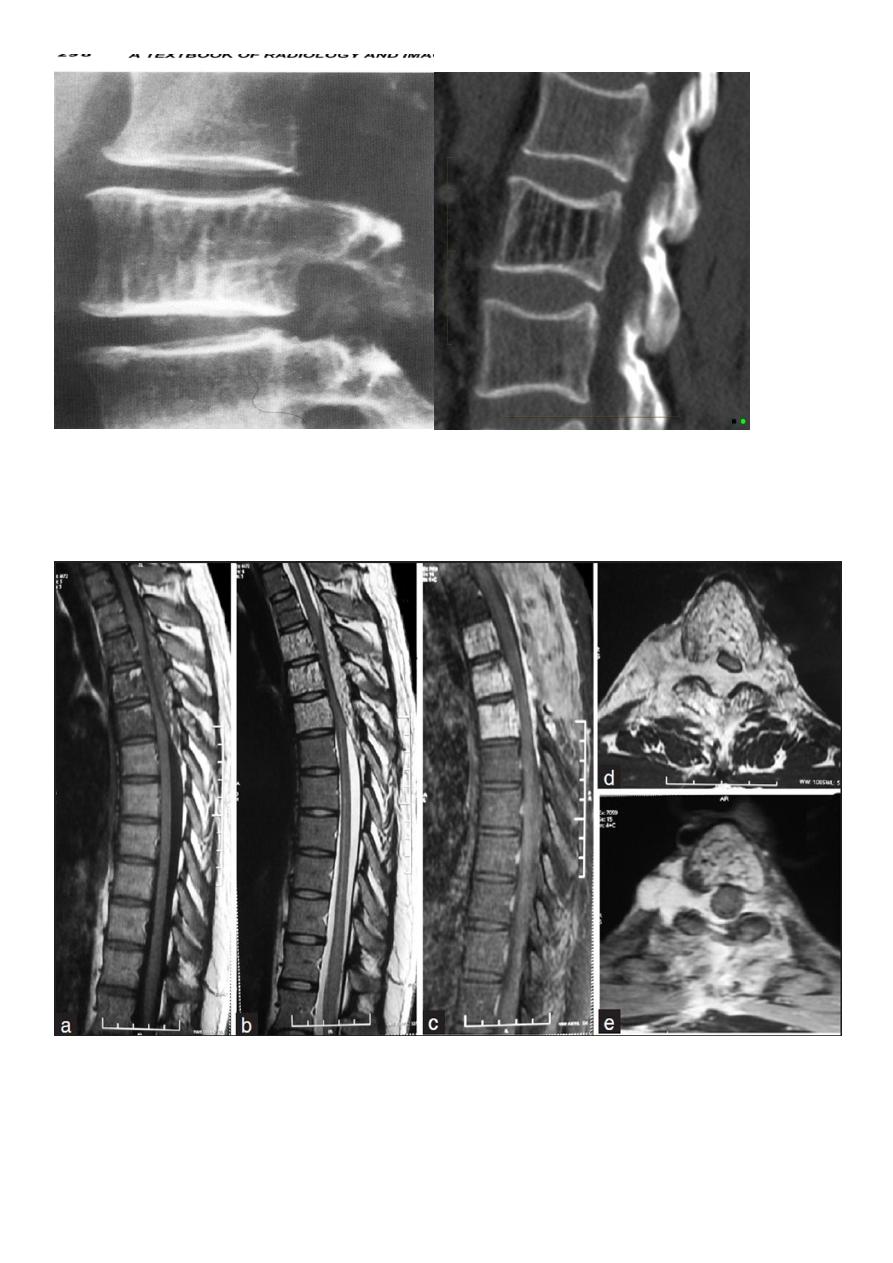
Sagittal MR image of the thoracic spine
demonstrates destruction of the intervertebral disc at the point where the paraspinal widening i s
maximal and this change is associated with alteration of
signal from the vertebrae.

6
Solitary Bone Lesion:
Causes:
1 -
Bone tumors (benign, malignant).
2 -
Tumor like conditions (fibrous cortical defect, fibrous dysplasia, bone cyst).
3 -
Osteomyelitis.
4- Conditions of uncertain origin (Langerhans histiocytosis and osteoid osteoma).
Assessment of radiologicaI findings in bone lesion:
Before we look to the lesion we check the age of the patient, it is of almost importance as
some conditions tend to occur in specific age group. Then
,
1 -
site
:
Meta physeal lesion as osteo myelitis.
Sub articular as giant cell tumor.
Appendiculer skeleton as in primary bone tumor.
Axial skeleton as multiple myeloma and metastases.
2 -
Edge ( zone of transition )
Well defined clear cut with narrow zone of transition indicates benign or slowly growing
lesion.
Ill-defined wide zone of transition indicates aggressive rapidly growing lesion as osteo
myelitis and malignant tumors.
Metastases & myeloma lie in the middle of the spectrum (well defined lytic lesion with no
sclerotic margin).
7
Wide Zone of Transition Narrow Zone of Transition.
3 -
Adjacent cortex:
Cortical destruction, aggressive lesions as in osteomyelitis & malignant tumors.
Cortical expansion with no destruction in benign conditions as fibrous dysplasia or
enchondroma.
4 -
Periosteal reaction :
in the absence of trauma periosteal reaction indicates aggressive lesion:
Osteomyelitis.
Malignant tumors: osteosarcoma, Ewing's sarcoma ,
Metastasis (not uncommen) particularly Neuroblastoma
5
- Calcification:
Well defined, patchy popcorn indicates cartilaginous origin.
Ill-defined speckles indicate osteoid forming tumors as in osteosarcoma
6
- Soft tissue swelling:
Ill-defined swelling with blurring of the tissue fat planes due to edema seen in inflammation
as osteomyelitis.
Well defined swelling with displacement of clear cut fat planes seen in tumors.

8
Malignant Bone Tumors:
Secondary bone tumors : (metastases)
:
are the commonest malignant tumors affecting the bone.
Osteo sarcoma is the commonest primary malignant bone tumor in young adults,
Conventional X-ray is satisfactory modality for the initial diagnosis
CT & MRI are useful to show the extent within the bone marrow & soft tissue involvement.
General features on X-ray are
:
Area of bone destruction or sclerosis with ill-defined margins, wide zone of transition &
periosteal reaction with or without cortical destruction & soft tissue swelling.
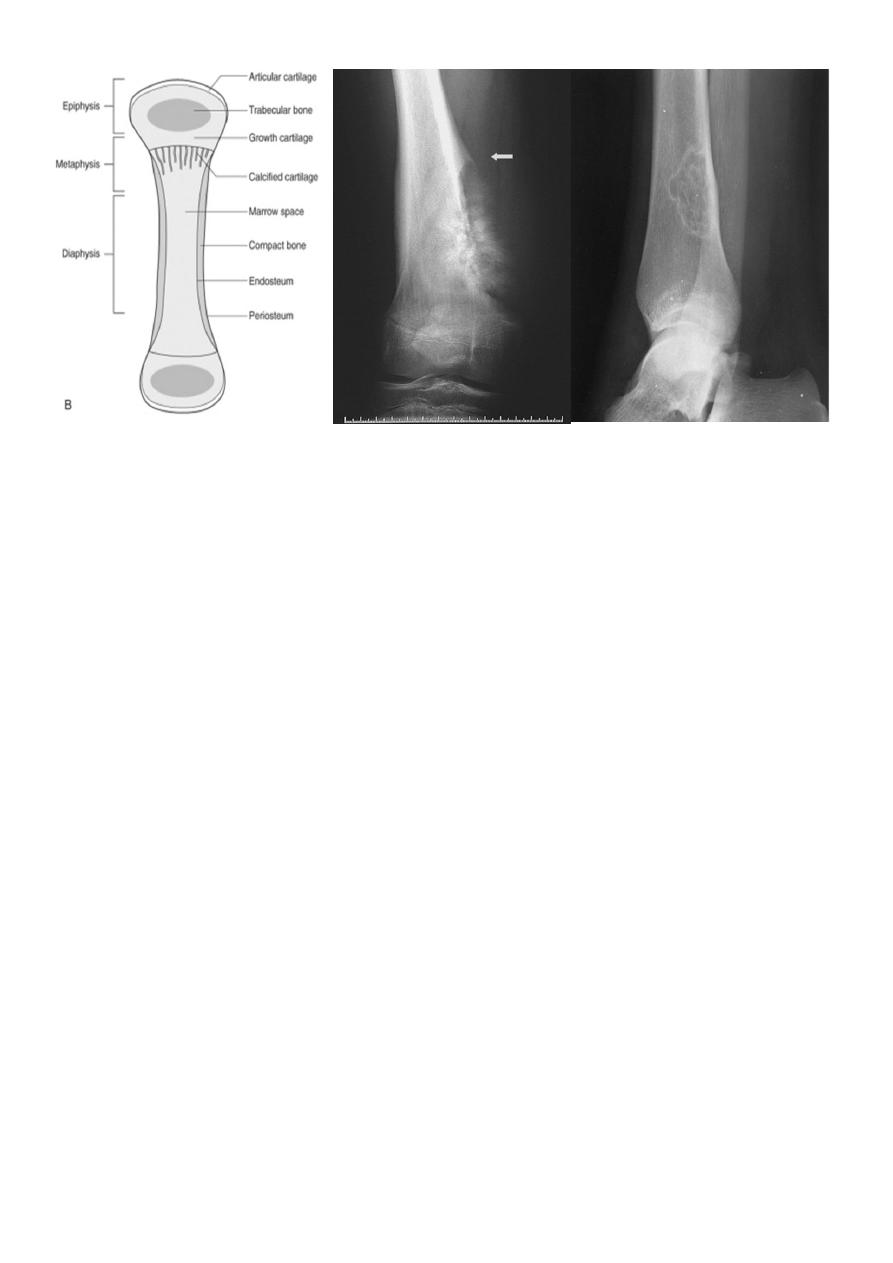
Osteosarcoma :
Age: 5-20-yrs, elderly with Paget's disease.
Site: metaphyseal around the knee joint.
Findings:
Lytic
Blastic
Mixed
Poorly defined bony destruction.
Sun ray speculation (periosteal reaction).
Elevation of the periosteum at the margin producing the so called Codman's triangle.
Cortical destruction.
Soft tissue swelling.
9
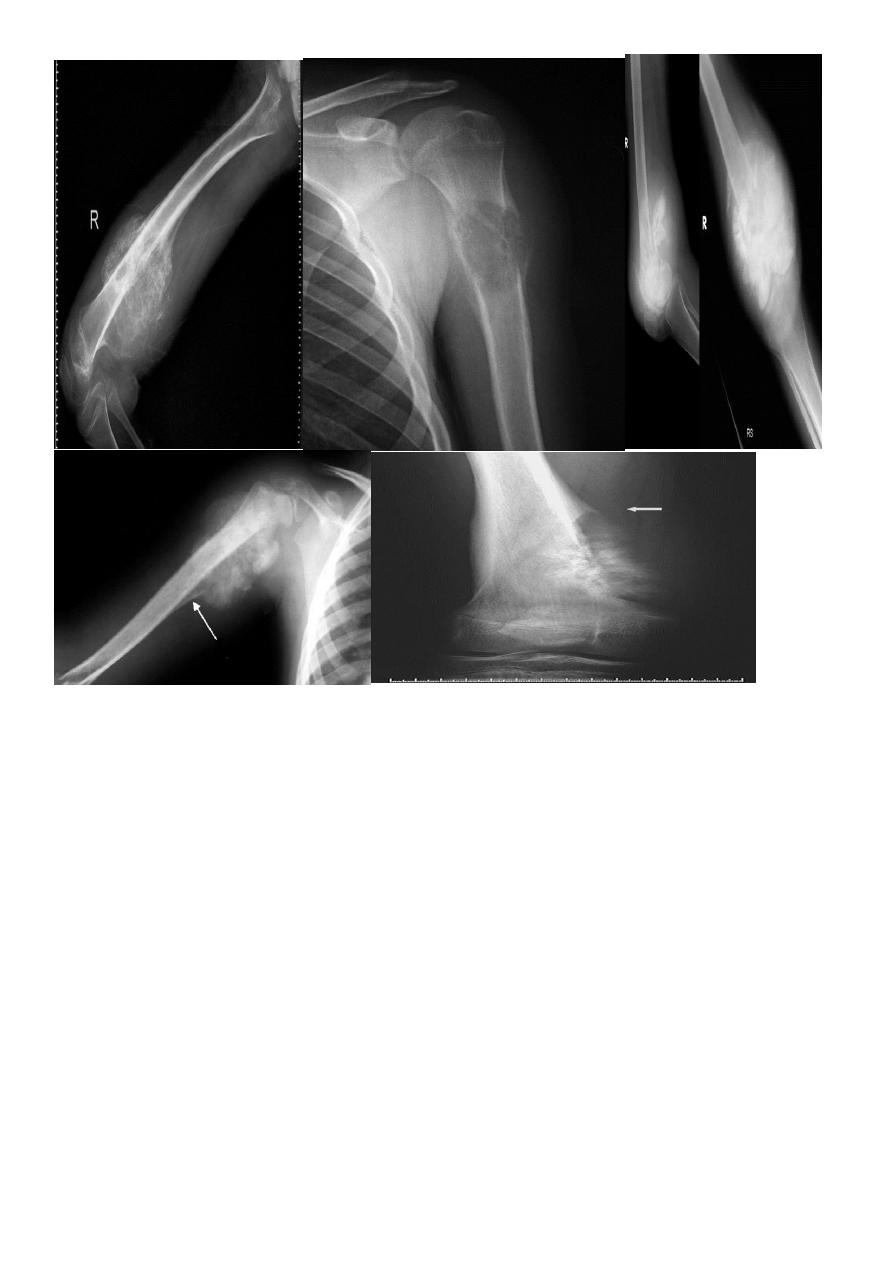
Chondrosarcoma :
Age: 30-50yrs.
Site: pelvic bones, scapula, humerus, femur.
May arise as malignant degeneration in cartilage cap of osteochondroma (1%) and in its
benign counterpart enchondroma
.
Findings:
Ill-defined expanding lytic lesion
Flecks of calcification.
May have periosteal reaction.
Large extra osseous component.
11
Ewings Sarcoma
Highly malignant with tendency to metastasize.
Age: children.
Site: shaft of long bone.
Findings :
ill-defined destruction with onion peal periosteal reaction.
Ewing's sarcoma. Sunray speculation Onion peel appearance
11
Giant cell tumor:
Slowly growing , locally invasive, rarely metastasize.
Age: after closure of epiphysis (20-40 years).
Site: around knee & wrist joints.
Findings:
lytic, expansile lesion ,
Sub articular in location,
Not clearly defined margin,
thinning of the cortex (sometimes with destruction of cortex)
Benign Bone Tumors & Tumor like conditions:
Features of benign tumors in X-ray film :
- Well demarcated.
- Cortical expansion but no destruction unless pathological fracture occurred.
- No periosteal reaction (unless pathological fracture developed).
- No soft tissue mass.
- No or little increase in uptake on bone scan (unless pathological fracture developed).

12
OSTEOCHONDROMA (EXOSTOSIS)
Cartilage-covered bony projection (exostosis) on the external surface of a bone .
Most common benign bone lesion. Osteochondromas have their own growth plate
and stop growing with skeletal maturity .
Age: < 20 years (adolescence)
Location: most commonly (85%): tibia, femur ,
humerus .
Malignant transformation (in < 1%). Suspect if :
Pain in the absence of fracture, bursitis, or nerve compression
Growth of lesion after skeletal maturation
>
1
cm of cartilaginous cap by CT, > 2 cm by MRJ
Dispersed calcifications in the cap
Enlargement of lesion
Increased uptake on bone scan
Radiographic features:
Two types :
*Pedunculated: slender pedicle directed away from growth plate
*Sessile (broad base)
Characteristic findings :
*Continuous with parent bone :
Uninterrupted cortex
Continuous medullary bone
* Calcification in the chondrous portion of cap; may be cauliflower-like
*Metaphyseal location (cartilaginous origin)
Lesion grows away from joint
* Multiple osteochondromas are seen in Diaphyseal aclasia.
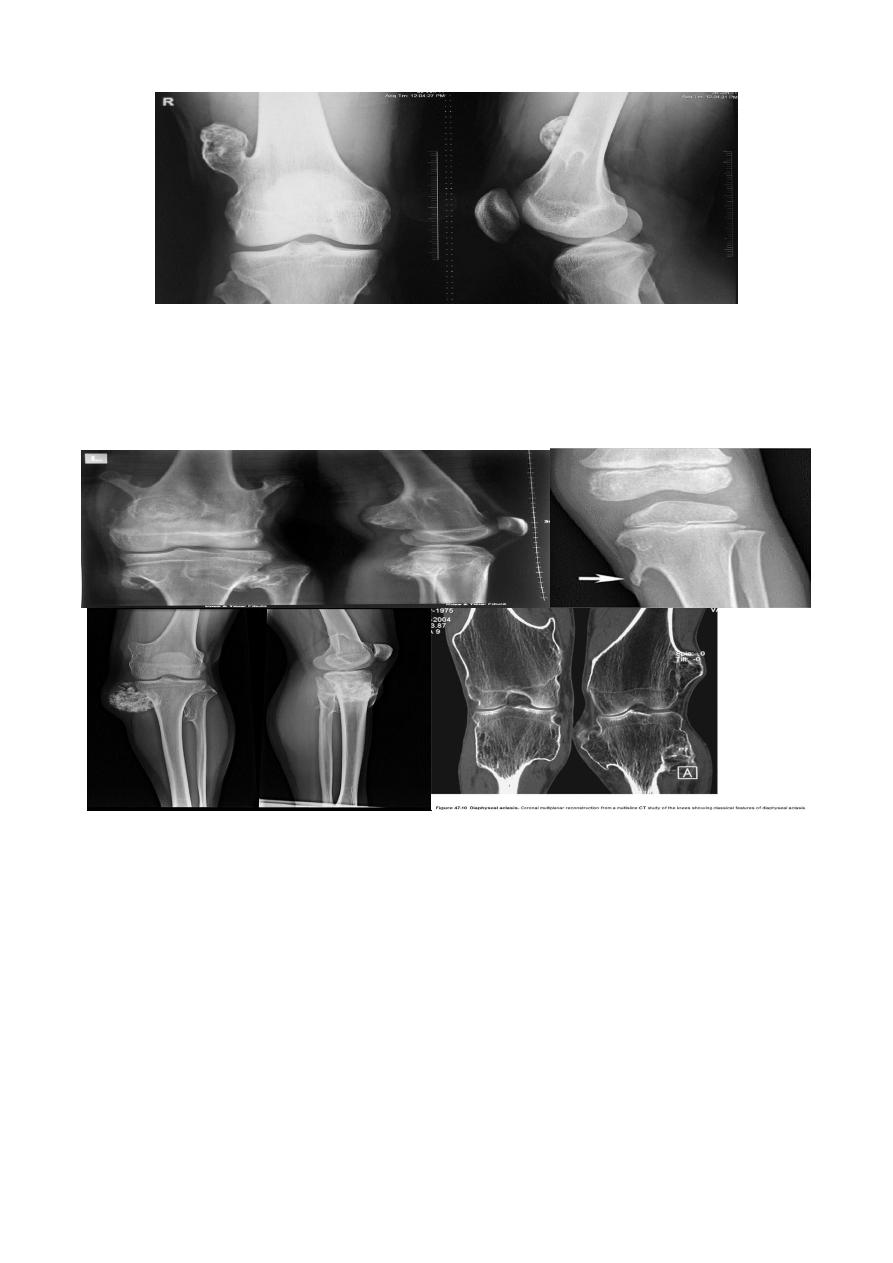
13
Osteochondroma of the distal femur .
The cortex is continuous with that of the underlying bone and trabecular bone merges with that of the
femur. A well-defined cartilage cap contains calcification and is directed
away from the joint.
Diaphyseal aclasia .
Multiple osteochondromas
Enchondroma :
Site : small bones of the hands & feet
Clinical features : painless asymptomatic swelling.
Findings : lytic lesion with expansion & thinning of the cortex, no periosteal reaction unless
pathological fracture develops.
1
% risk of malignant transformation in solitary type
Multiple enchondromatosis (Ollier's disease) affect long bones & carry 10% risk of
malignant transformation.
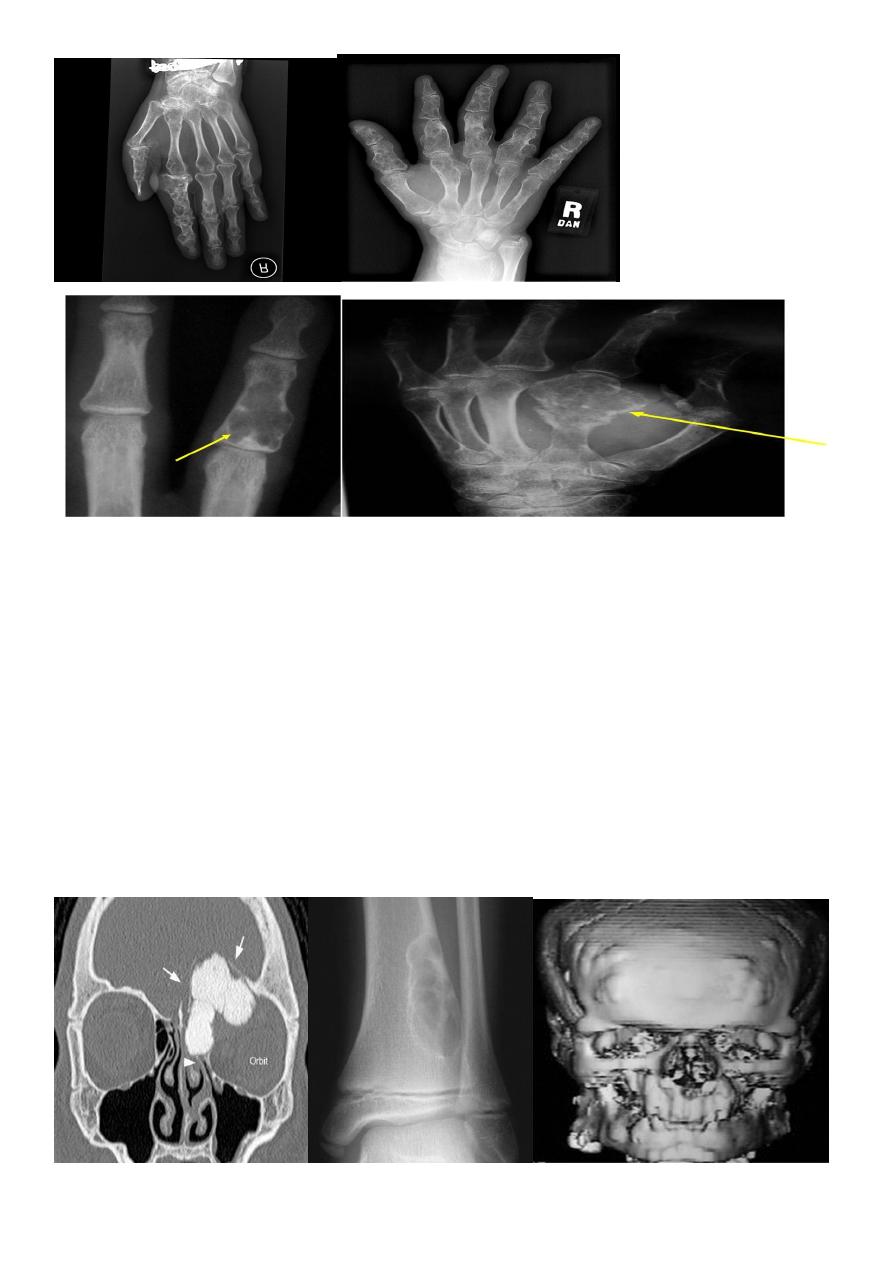
14
Multiple chondromas in the hand
Osteoma
Localized masses of mature bone on the endosteal or periosteal surface of cortex,
commonly in the skull or paranasal sinuses. Associated with Gardner's syndrome.
Fibrous Cortical Defect & Non ossifing Fibroma (NOF):
Common incidental findings in children.
Site: affect diaphysis of long bone.
Findings: well defined lucent areas in cortex with sclerosed margin .

15
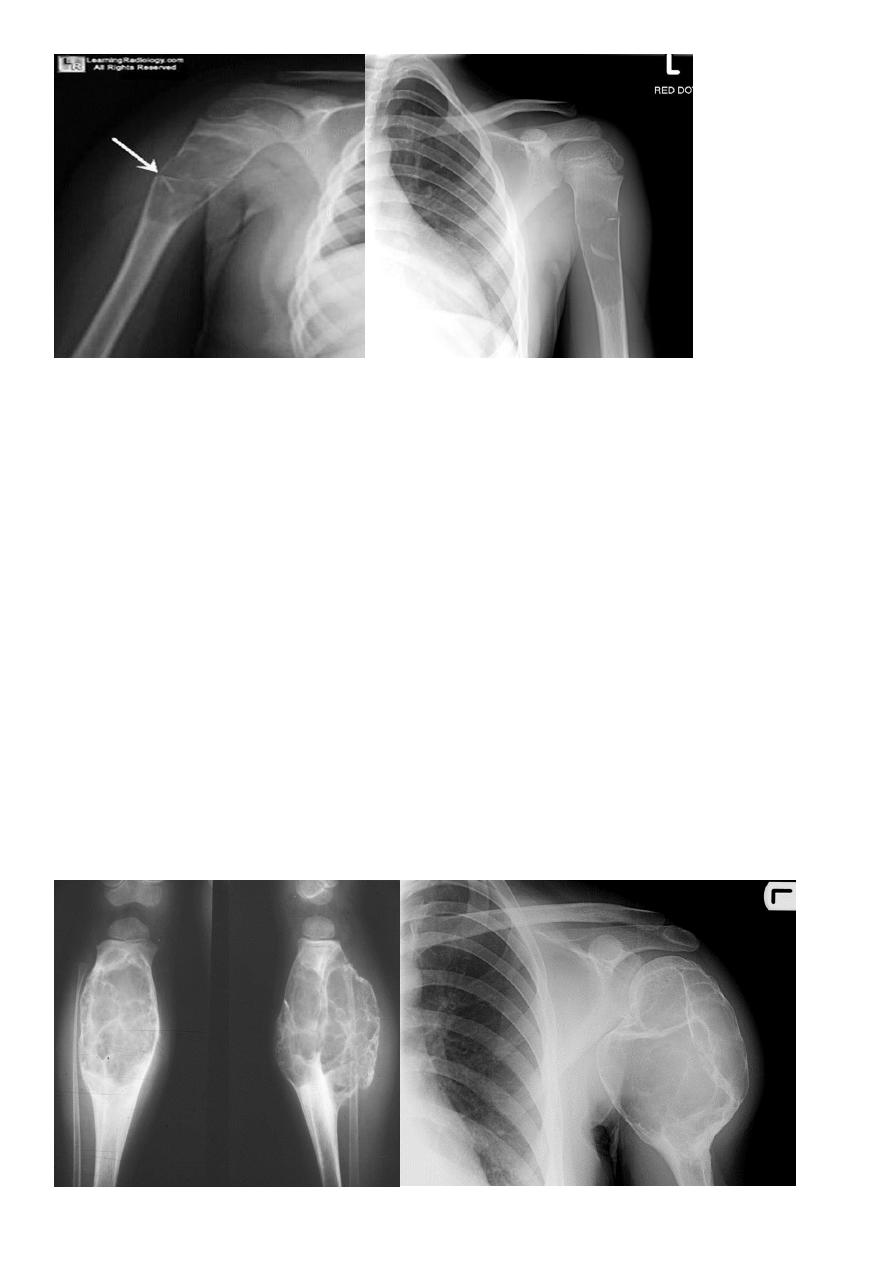
Fibrous Dysplasia :
Defect in the osteoblastic development and maturation as a result of mutation.
Types: monostotic & polystotic
Monostotic
Age: 10~30yrs .
Site: ribs, proximal femur, craniofacial bones.
Usually asymptomatic.
Polystotic
Age: at first decade .
Usually unilateral, asymptomatic.
Site: femur, tibia, pelvis, cranial bones, spine, feet.
It causes leg length discrepancy,
shepherd crook deformity, facial asymmetry, rib deformity, tibial bowing. Associated with
hyperparathyroidism, acromegaly, DM.
• Findings: lytic expansile lesion with typical ground-glass matrix mineralization and
sclerosed margin .
Fibrous dysplasia .
AP radiograph of the proximal femur showing a well-defined expanded lesion with typical
ground-glass matrix mineralization and a thick, sclerotic margin .

16
Fibrous dysplasia .
A multilocular, partly cystic, expansile lesion
of the midshaft femur is surrounded by a thick rim of reactive sclerosis.
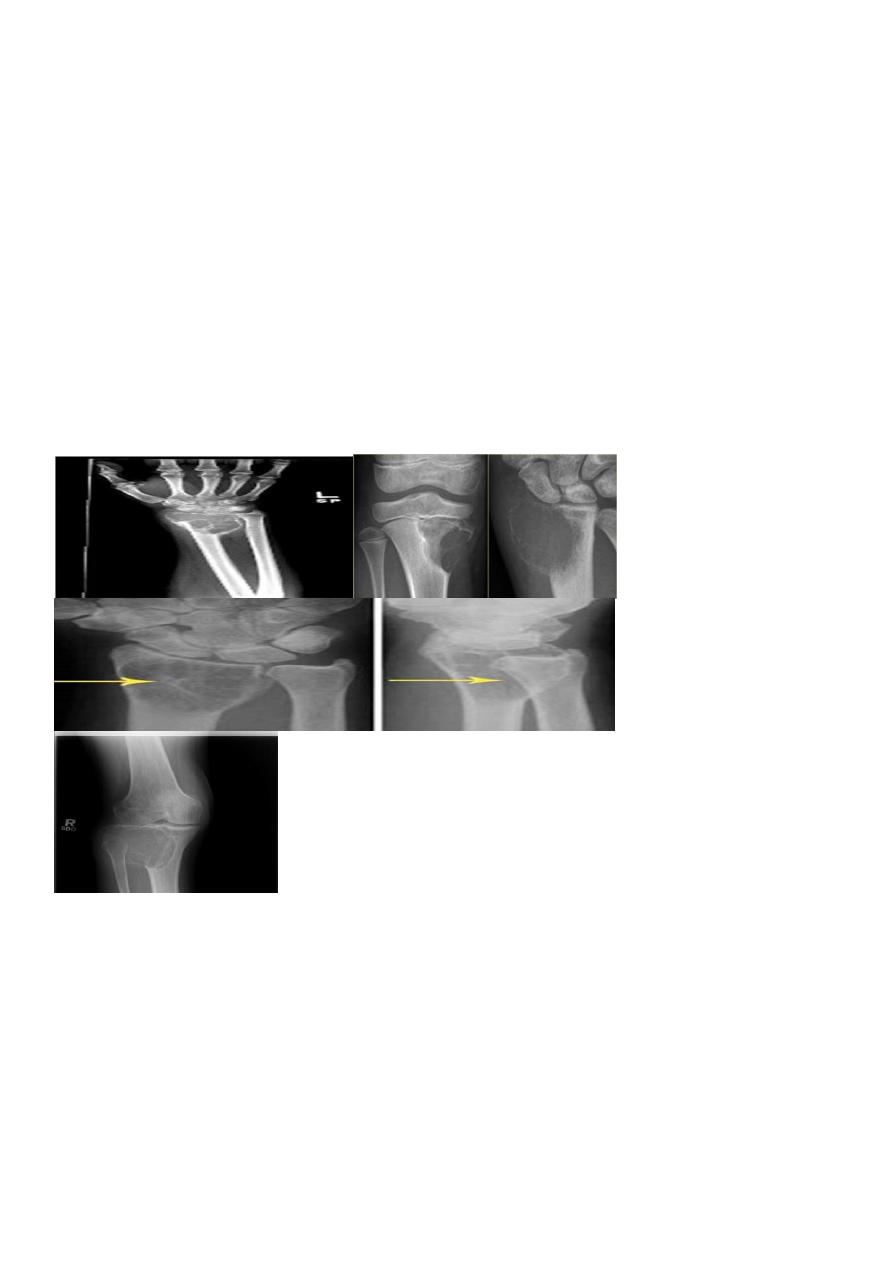
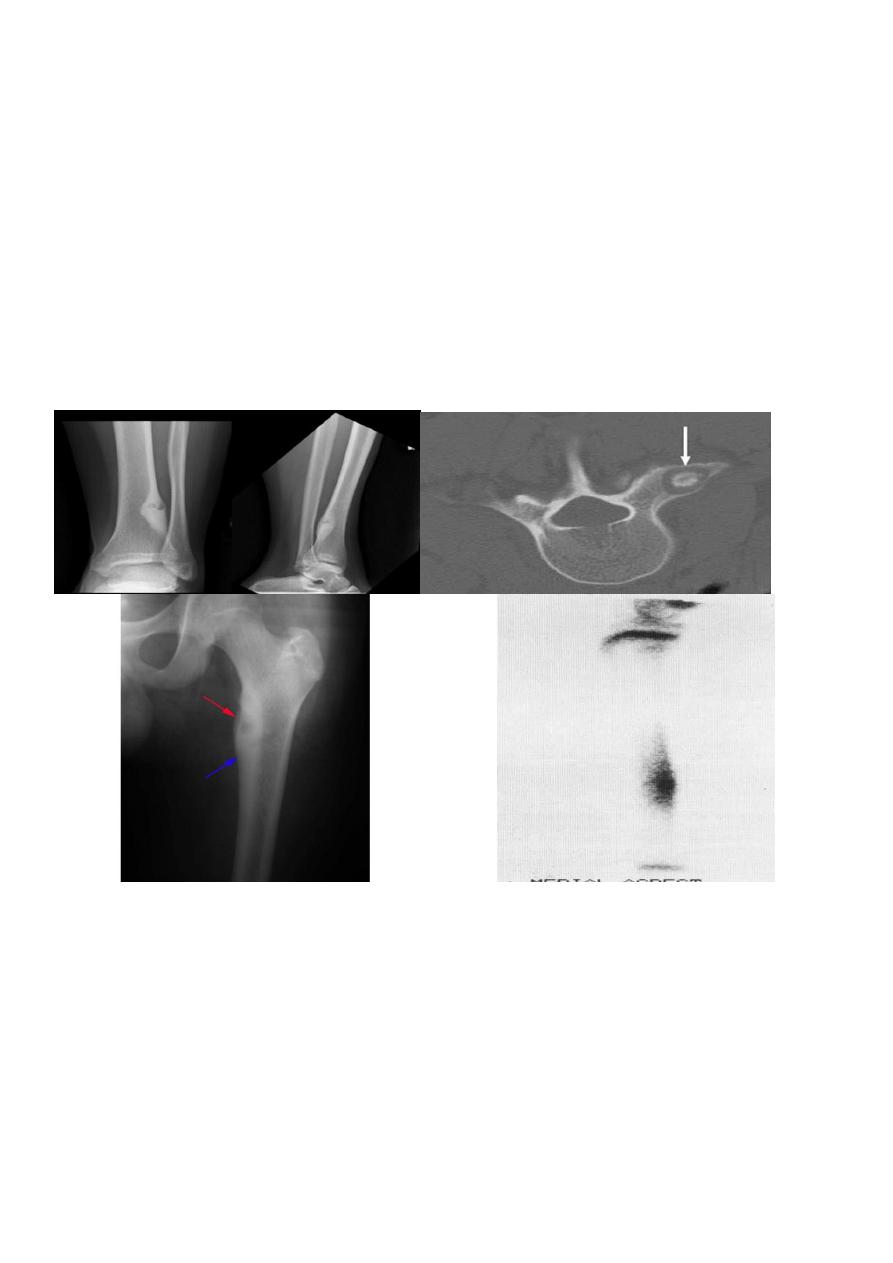
Solitary bone cyst:
Age: young adults & children.
Site: long bones.
Findings: well-defined expanding lytic lesion.
A piece of cortical bone has broken off and descended through the serous fluid contained
within the lesion and can be seen in the dependent portion of the lesion (arrow) as
a fallen fragment sign .
A fallen fragment sign is said to be pathgnomonic for
a unicameral bone cyst
17
Fallen fragment sign
Aneurysmal bone cyst :
Benign but may be aggressive in appearance.
Age: children &young adults
Site: spine, long bones, pelvis
Findings: purely lytic lesion, massive cortical expansion.
(CT and MRI show blood pools (fluid -fluid levels within the cyst.
D.Dx: giant cell tumor.
18
Osteoid osteoma:
Age: young adults
Site: tibia, femur
Findings: lucent area surrounded by calcification
nidus surrounded by sclerotic rim with or without periosteal reaction.
Radionuclide bone scan : area of increased uptake
19
Haemangioma of the vertebral body of L3 .
The whole body is marked by the characteristic vertical striation
The body of thoracic v. appeared as an area of high signal intensity on T1-T2-weighted
images (a and b)