1
Fifth stage
Dermatology
Lec-4
Dr.Omar
24/10/2016
Skin Infections
I. Bacterial skin infections
Why does skin get infected?
There are multiple types of bacteria which are normally present on the skin.
For example: Staphylococcus epidermidis and yeasts
The presence of bacteria does not automatically lead to a skin infection
What is the difference between colonisation and infections???
Colonisation: Bacteria are present, but causing no harm
Infection: Bacteria are present and causing harm.
A break in the epidermal integrity can allow organisms to enter and become pathogenic.
This can occur as a result of trauma, ulceration, fungal infection, skin disease such as
eczema
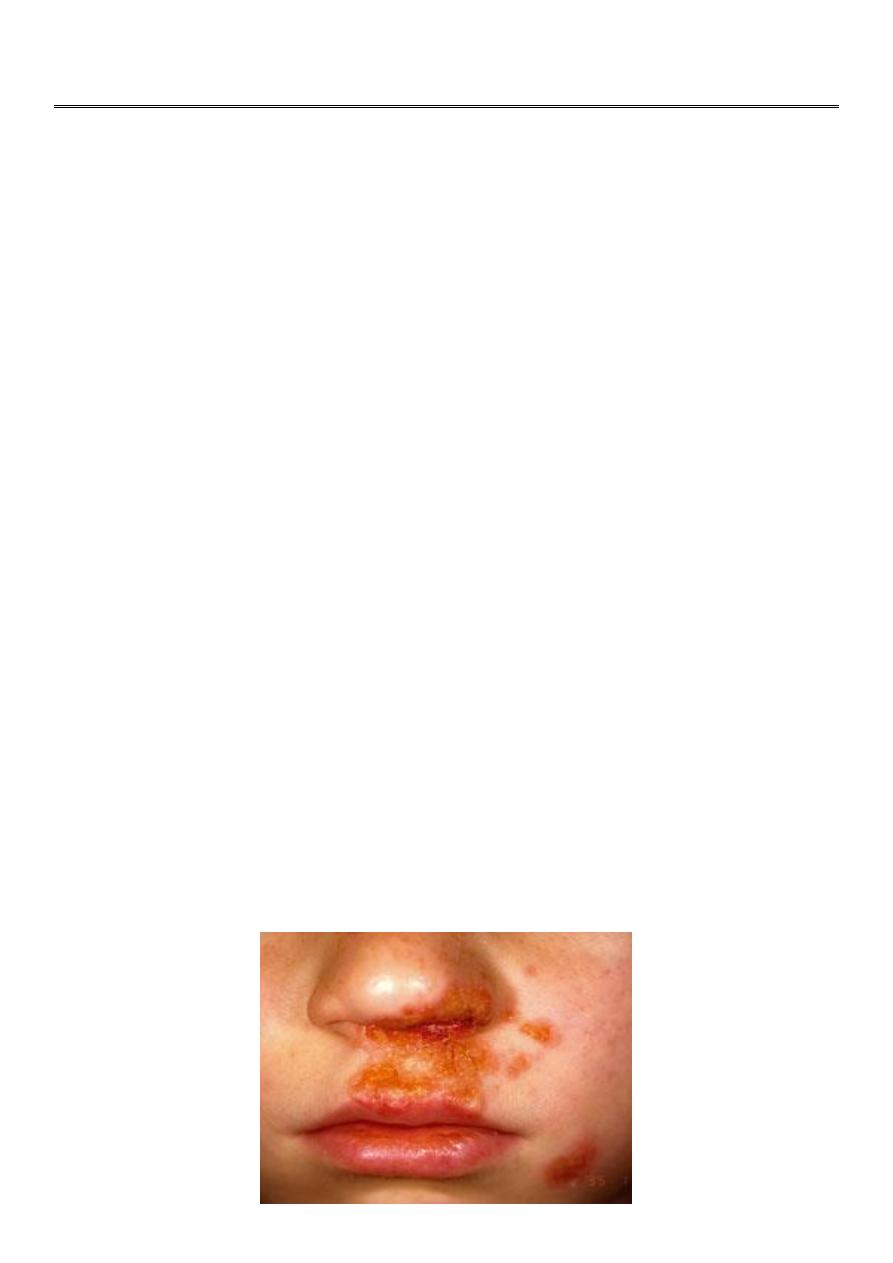
Impetigo
A highly infectious skin disease, which commonly occurs in children.

2
The causative organism is usually Staphylococcus Aureus (>90% cases
1
), but less often
can be strep pyogenes.
Begins as a vesicle, which may enlarge into a bulla.
Weeping, exudative area with characteristic honey coloured or golden, gummy crusts,
which leave denuded red areas when removed.
Usually on the face around the mouth, but any area could be affected.
Treatment:
Mild localised cases - use topical antibiotic Polyfax
Widespread or more severe infections – use systemic antibiotics, such as flucloxacillin
(or erythromycin if penicillin allergic)
Folliculitis
Inflammation of the hair follicle.
Presents as itchy or tender papules and pustules at the follicular openings.
Complications include abscess formation and cavernous sinus thrombosis if upper lip,
nose or eye affected.A
Most common cause is Staph Aureus.
Other organisms to consider include:
Gram negative bacteria – usually in patients with acne who are on broad spec
antibiotics
Pseudomonas (“Hot tub folliculitis”)
Yeasts (candida and pityrosporum)

3
Treatment
Topical antiseptics such as Chlorhexidine
Topical antibiotics, such as Fusidic acid or Mupirocin
More resistant cases may need oral antibioics such as Flucloxacillin
Hot tub folliculitis – ciprofloxacin
Gram negative – trimethoprim
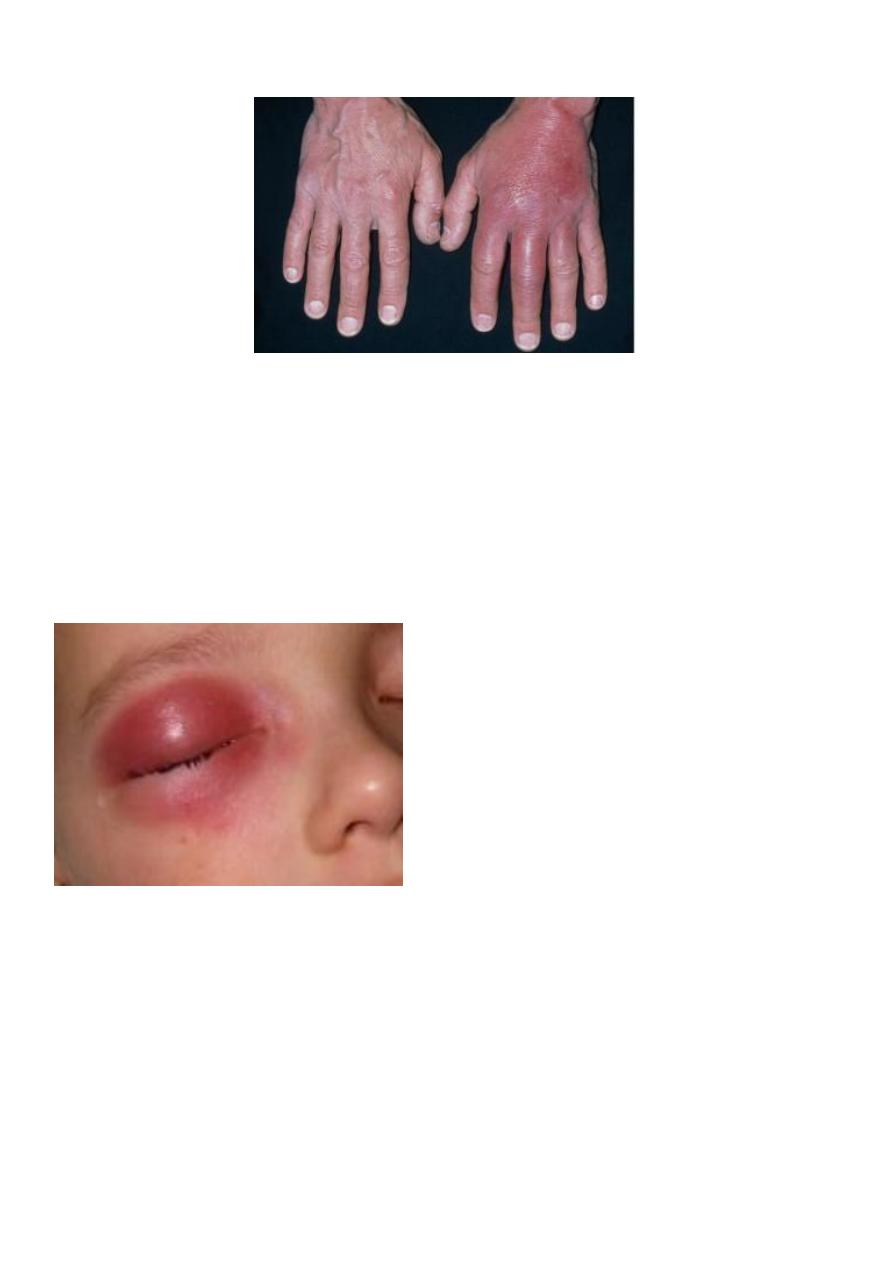
Cellulitis
Infection of the deep subcutaneous layer of the skin
Presents as a hot, tender area of confluent erythema of the skin
Can cause systemic infection with fever, headache and vomiting.
Erysipelas is more superficial and has a more well demarcated border
Cellulitis Erysipelas
Streptococcus – Group A Strep Pyogenes.
Others include Group B, C, D strep, Staphylococcus Aureus, haemophilus influenzae
(children) and anaerobic bacteria (e.g Pasteurella spp. After animal bites)
4
Treatment of cellulitis
Oral Flucloxacillin or erythromycin if allergic
Co-amoxiclav in facial cellulitis
If severe systemic upset, may require admission for IV antibiotics.
After the acute attack has settled, especially in recurrent episodes – consider the
underlying cause
Orbital cellulitis – refer urgently

5
Staphylococcal Scalded Skin Syndrome
A superficial blistering condition caused by exfoliative toxins of certain strains of
Staph Aureus
Usually in children less than 5 yrs old
Characterised by blistering and desquamation of the skin and Nikolsky's sign
(shearing of the epidermis with gentle pressure), even in areas that are not obviously
affected
begins with a prodrome of pyrexia and malaise, often with signs and symptoms of an
upper respiratory tract infection
discrete erythematous areas then develop and rapidly enlarge and coalesce, leading
to generalised erythema - often worse in the flexures with sparing of the mucous
membranes
large, fragile bullae form in the erythematous areas and then rupture
6
Complications include hypothermia, dehydration and secondary infection.
Treatment: ABC, refer urgently for IV antibiotics and fluids, may need referral to
tertiary burns centre
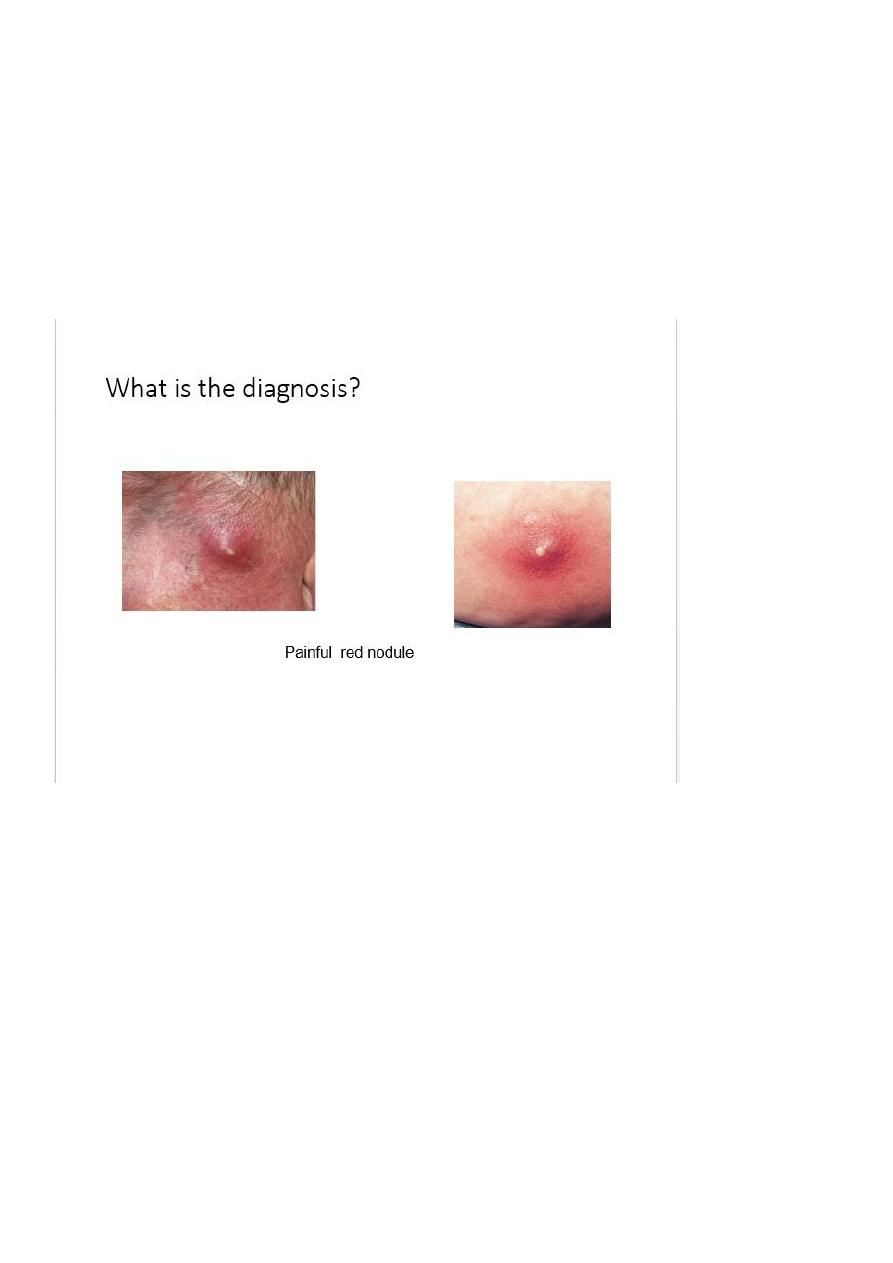
Furunculosis (boils) and carbuncles
• Deeper Staphylococcal abscess of the hair follicle
• Coalescence of boils leads to the formation of a carbuncle
• Treatment is with systemic antibiotics and may need incision and drainage.
• Consider looking for underlying causes, such as diabetes
7
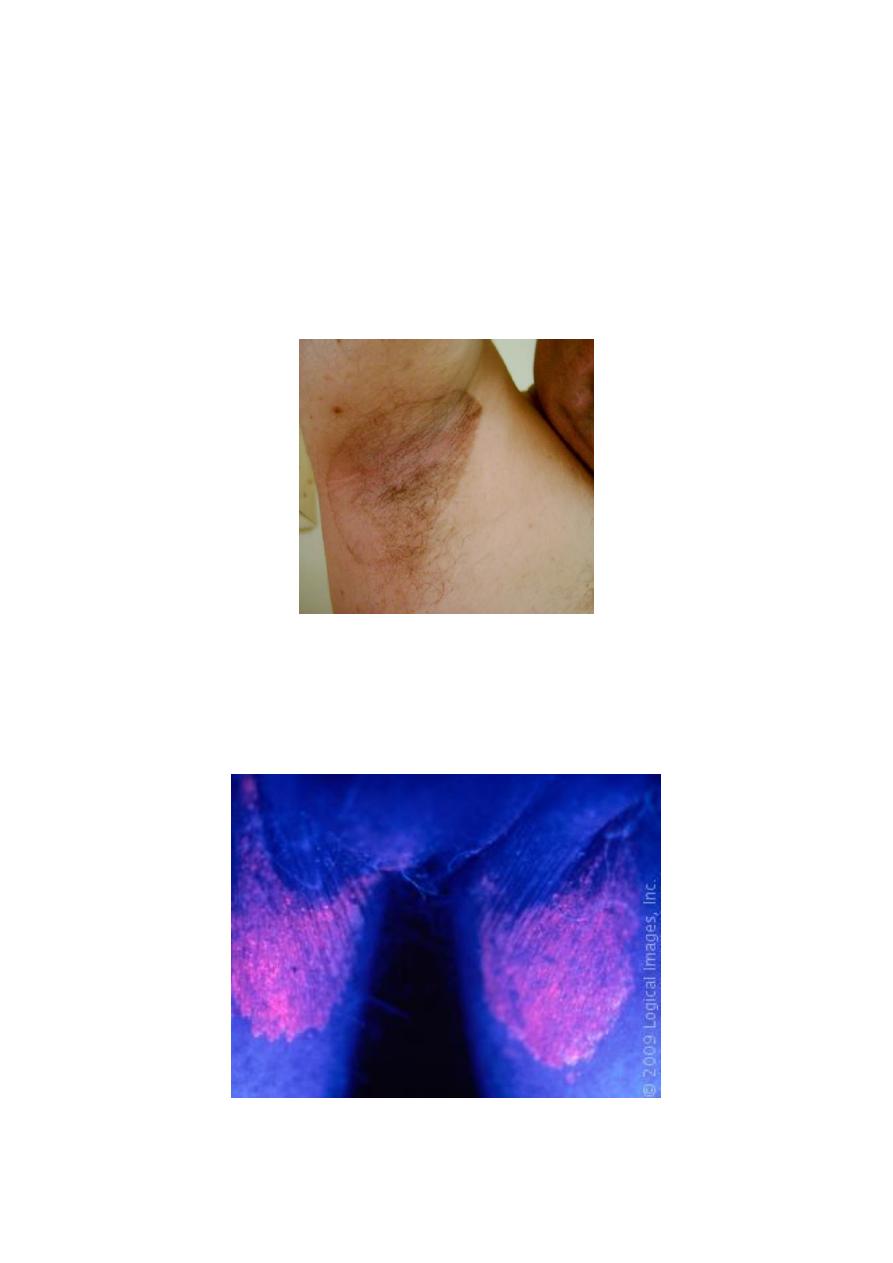
Erythrasma
Colonisation of axillae or groin with Corynebacterium Minutissimum.
Presents as a fine, reddish brown rash in the flexures, which is sharply marginated.
Often misdiagnosed as a fungal infection
Woods light illumination produces a characteristic coral-pink fluorescence.
Treatment is with topical fusidin cream.
• When you use the Wood’s light, the skin lesion shows a dramatic coral pink
fluorescence.

8
Viral Skin Infections
Viral warts and verrucas
Caused by human papilloma virus
Main types, common, plane and plantar
Very common
Disappear spontaneously eventually
• If treatment is needed, options include:
• Salicylic acid topically – needs daily treatment and can take months
• Cryotherapy
• Imiquimod cream
9
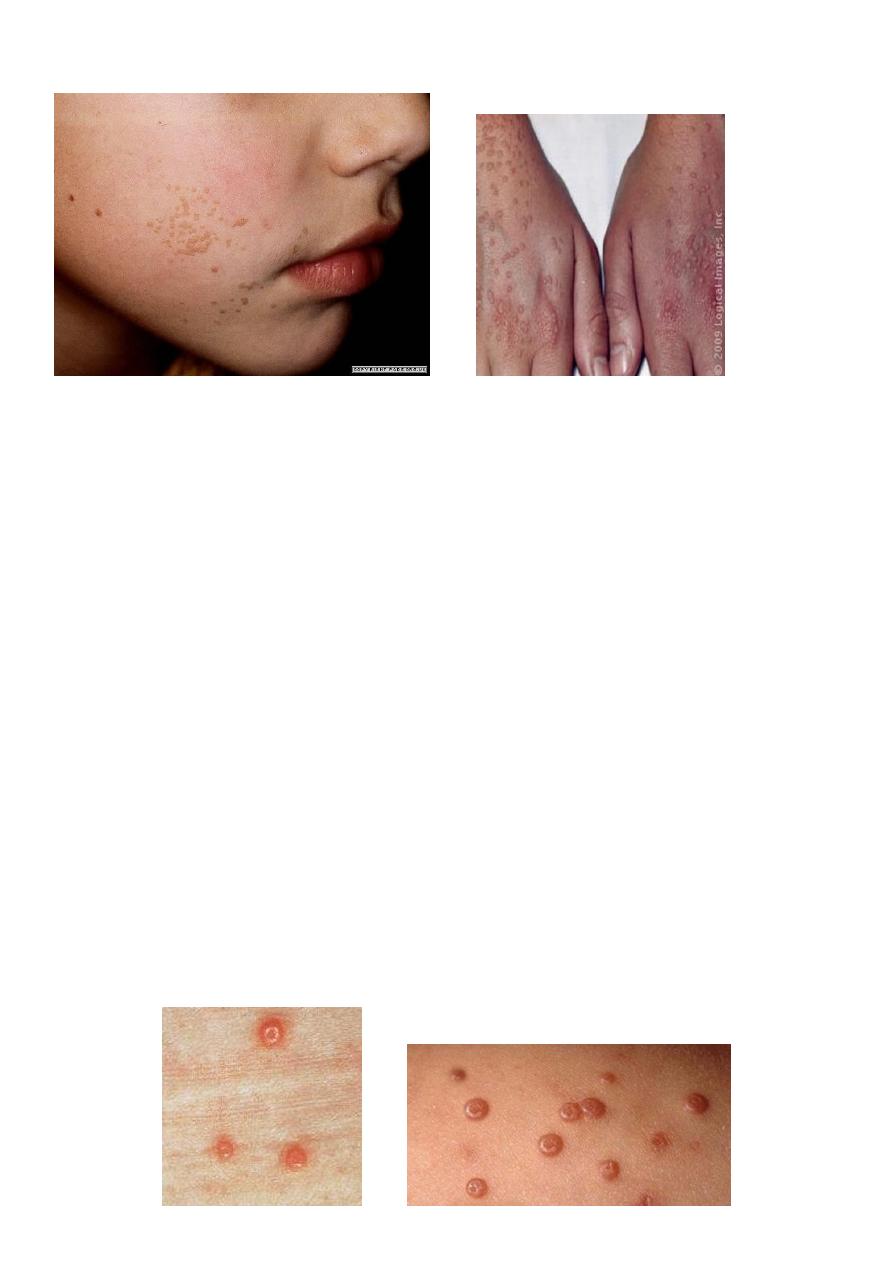
Molluscum contagiosum
Caused by DNA pox virus
Common in children, but can occur at any age
Spread by direct contact
Presents as multiple small, pearly, dome-shaped papules with central umbilication
Can occur at any site
Usually resolve spontaneously in 6-18 months
Resolution is heralded by the development of erythema around the lesions.
Treatment is not usually necessary – simple reassurance and advice about reducing
transmission.
• If treatment is necessary, options include:
• Piercing the lesion with an orange stick tipped with iodine
• Curretage
• imiquimod cream
11
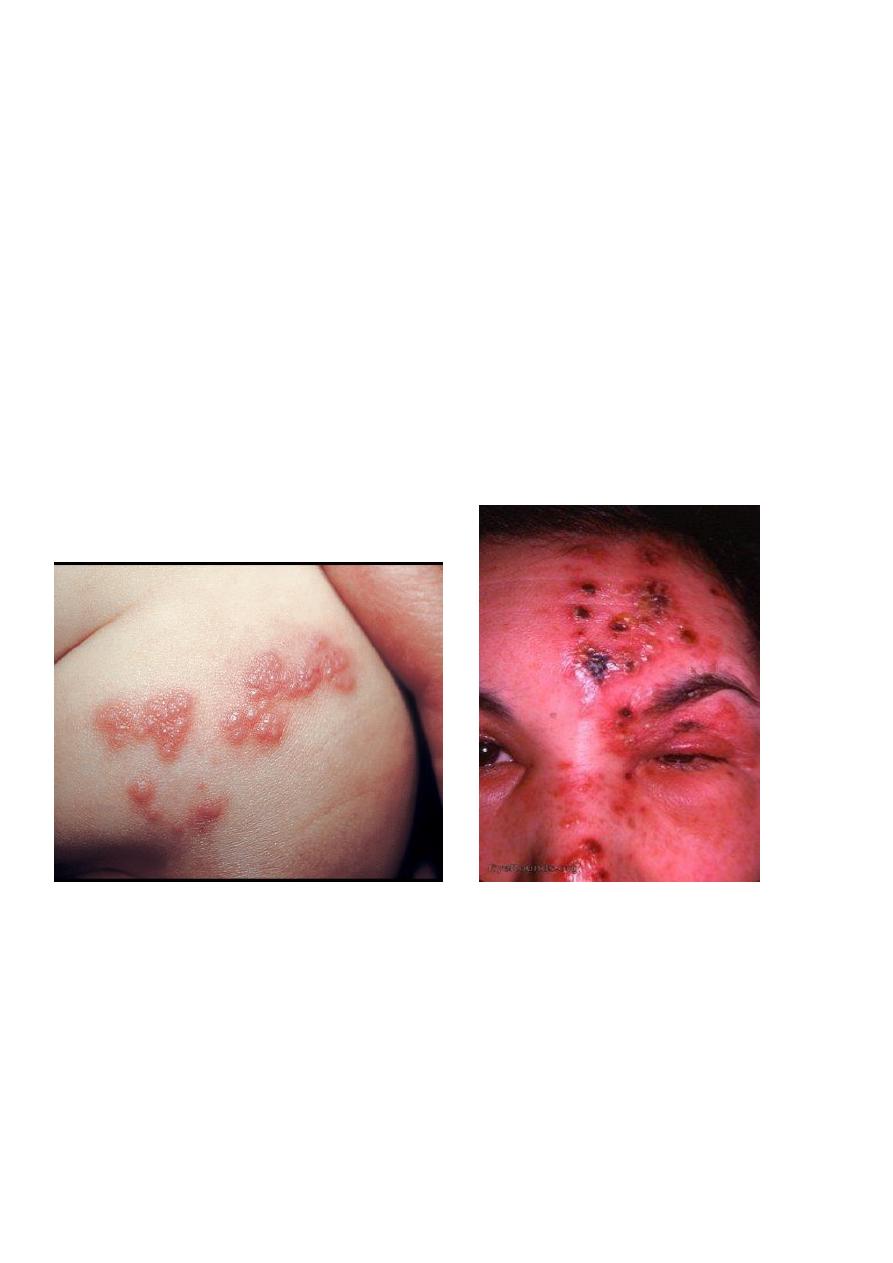
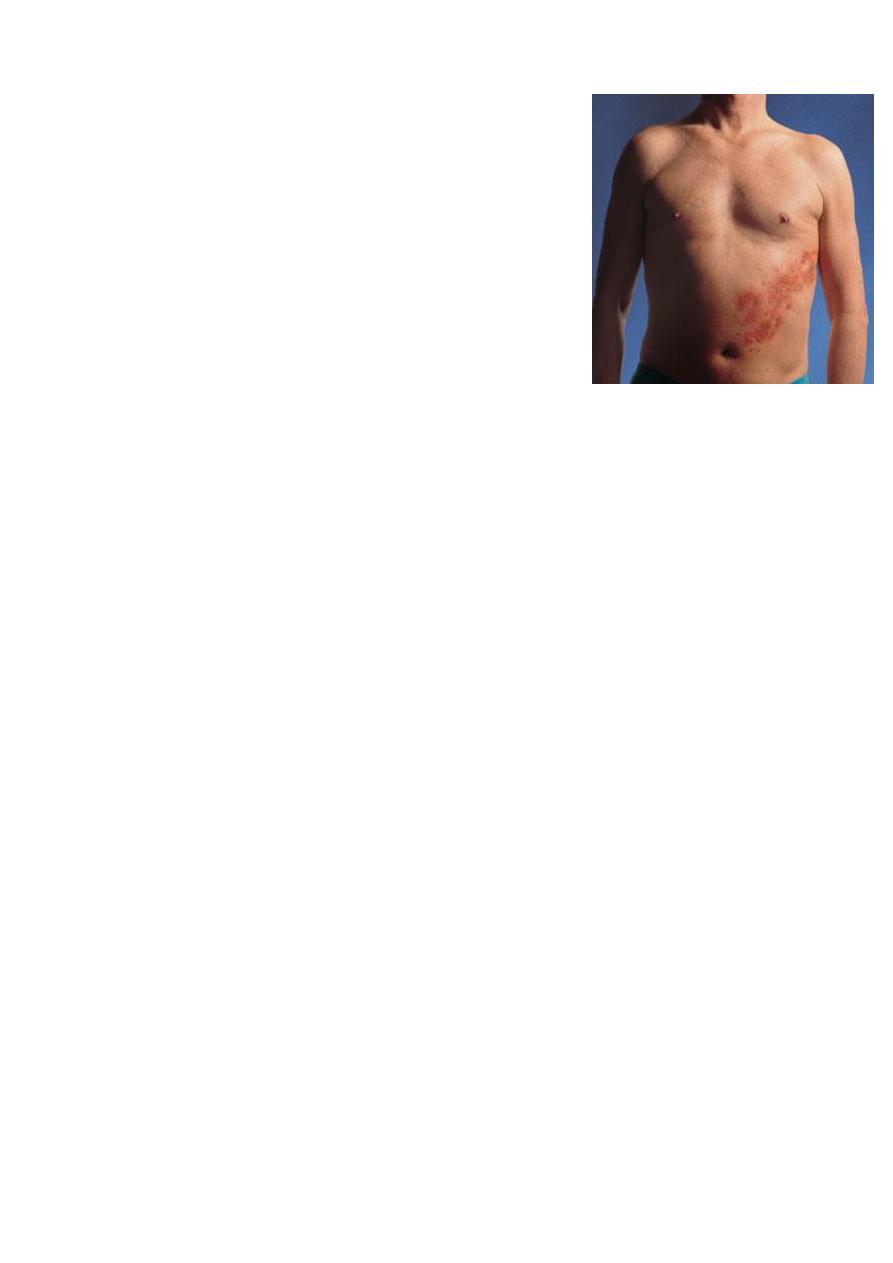
Herpes Zoster (Shingles )
• Caused by reactivation of the chickenpox virus which has lain dormant in the dorsal
root or cranial nerve ganglia
• Rash is preceded by a prodromal phase of up to 5 days of tingling or pain
• Then develop painful grouped vesicles/pustules on a red base in a dermatomal
distribution.
• Most common in thoracic and trigeminal areas
• Lesions become purulent, then crusted
• Healing takes place in 3-4 weeks
Shingles treatment
• Aciclovir 800mg 5 times daily, for 7 days
• Rest, analgesia
11
Complications include:
Post herpetic neuralgia
Secondary infection
Guillain Barre Syndrome
Occular disease
Post-herpetic Neuralgia
Pain lasting longer than 3 months after the rash.
The followings are risk factors for developing post-herpetic neuralgia?
A: Older age
B: More severe pain during the eruption
C: Severely inflamed rash
D: Prodromal pain in dermatome
Herpes Simplex Virus
• A highly contagious infection spread by direct contact
• HSV 1 : also commonly called “coldsore”
• HSV 2 usually presents on the genitalia
• Primary infection is usually asymptomatic.
•
Recuurent infection presents as acute, painful gingivo-stomatitis with multiple small
intra/peri-oral ulcers (but any site could be affected). Associated with fever, malaise
and lymphadenopathy
.

12
Genital herpes
Herpes Simplex Keratitis
Clinically: Grouped umbilicated vesicles/pustules on erythematous base.
Treatment:
• Topical aciclovir can be used: 5 times daily for 5 days. Reduces duration of attack and
duration of viral shedding.
• The correct dose of aciclovir for HSV is 200mg 5 times daily for 5 days
A.L.Y