1
Fifth stage
Gynaecology
Part-1
Prof.Ahmed
/ /2016
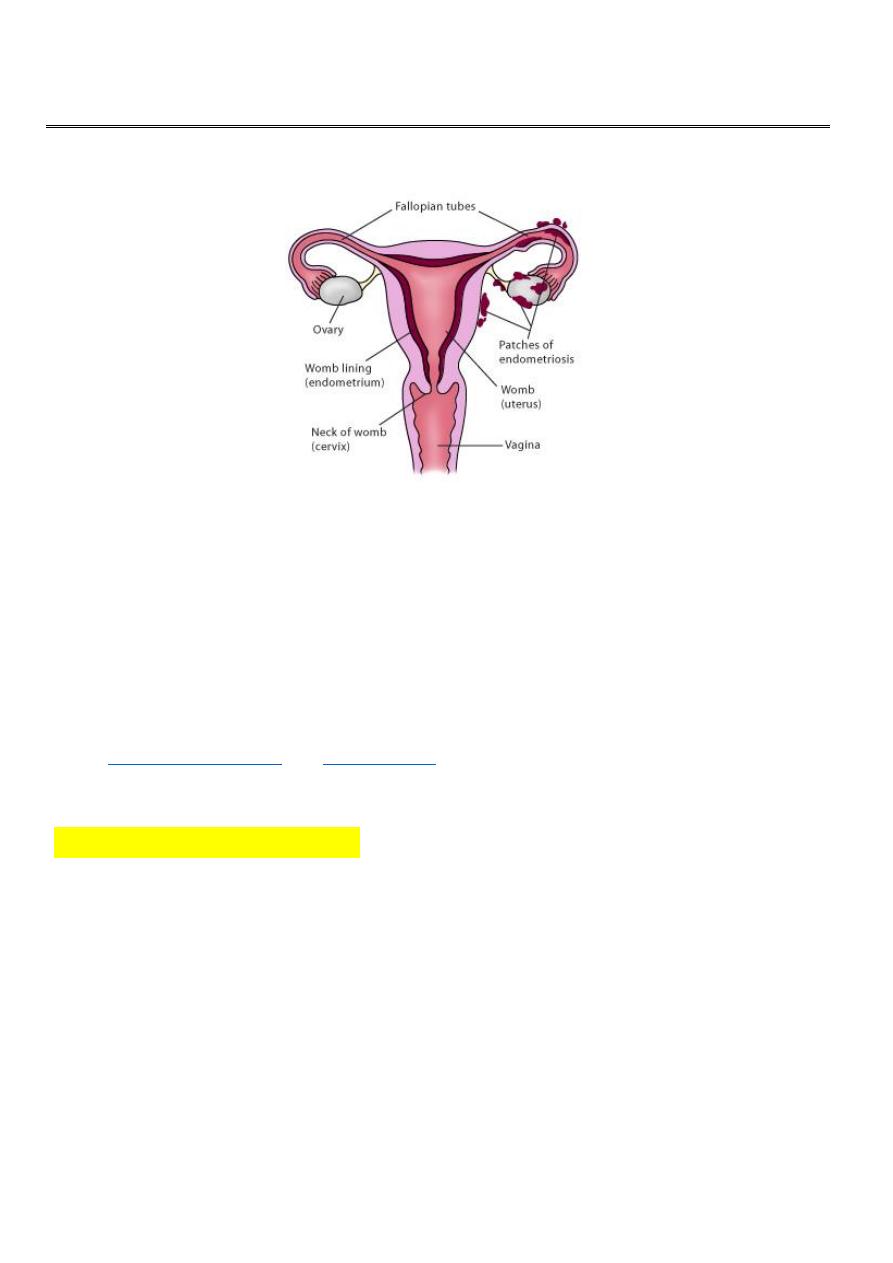
Endometriosis
Endometriosis is presence of viable endometrial tissue outside the lining of uterine cavity.
It is one of the commonest benign gynecological conditions and it is a chronic and
progressive disease.
Prevalence:
The exact prevalence of endometriosis is not known, since many women may have the
condition and have no symptoms. Endometriosis is estimated to affect from 3% to
18% of women. It is one of the leading causes of pelvic pain and reasons for
. .
Aetiology of endometriosis
The cause of endometriosis is unknown. Several theories exist to explain the process
through which endometriosis develops. These are:
1. Retrograde menstruation with implantation.
2. Coelomic epithelium transformation.
3. immunological factors.
Retrograde menstruation
4. Genetic predisposition. (more commonly in the 1st degree relatives of affected
women).
5. Vascular and lymphatic spread.(endometriosis in the brain and other organs distant
from the pelvis).
2
6.direct transfer of endometrial tissues during surgery.(
or
The most widely accepted explanation is:
Retrograde menstruation with implantation of endometrial fragments in conjunction with
peritoneal factors to stimulate cell growth.
Pathology:
Endometrium outside uterine cavity responds to cyclic changes from ovarian hormones.
During each menstrual cycle the endometrial deposit proliferates and then breaks down
and bleeds, causing a local inflammatory reaction which may followed by a prolonged
period of time by fibrosis.
Chronic repition of this process disrupts and distorts the affected tissue and typically
dense scar tissue and adhesion may form that can distort a woman’s internal anatomy. In
advanced stages, internal organs may fuse together, causing a condition known as a
"frozen pelvis."
The disease varies from a few, small lesions on otherwise normal pelvic organs to solid
infiltrating masses. The cells of endometriosis attach themselves to tissue outside the
uterus and are called endometriosis implants.
Endometriosis typically appears as superficial ‘powder-burn’ or ‘gunshot’ lesions, black,
dark-brown or bluish puckered lesions, nodules or small cysts containing old
haemorrhage surrounded by a variable extent of fibrosis on the ovaries, serosal surfaces
and peritoneum.
Atypical lesions are also common.
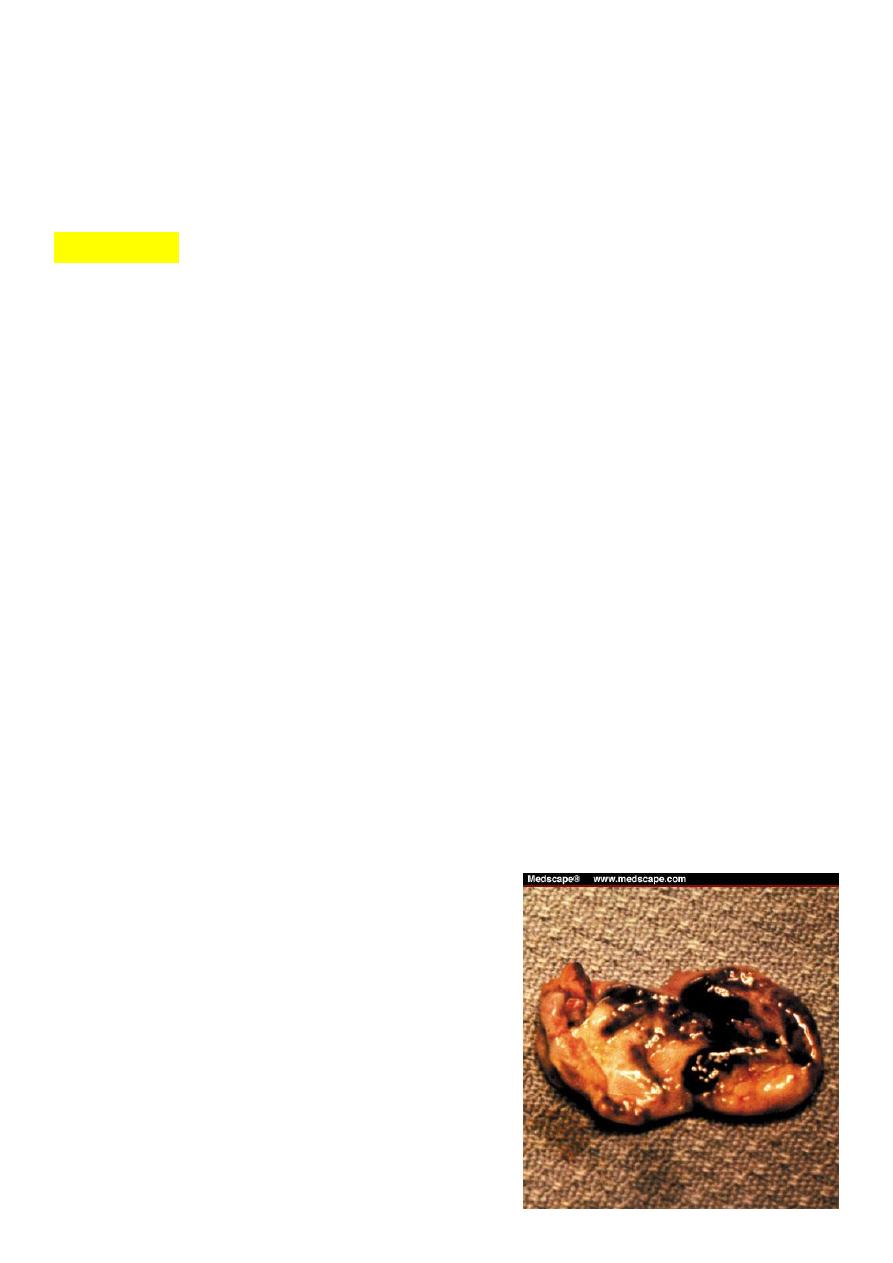
Endometriomas (chocolate cysts ):
Are retention cysts containing tary material that
develop as a consequence of ovarian endometriosis. It may be multiple and very large. It
responds to ovarian hormones, bleeding may occur in endometriosis forming small blood
cyst, in the ovary. It become large up to 10 cm and
tend to be bilateral.
Upon opening a chocolate cyst, irregular brown areas
are observed
3
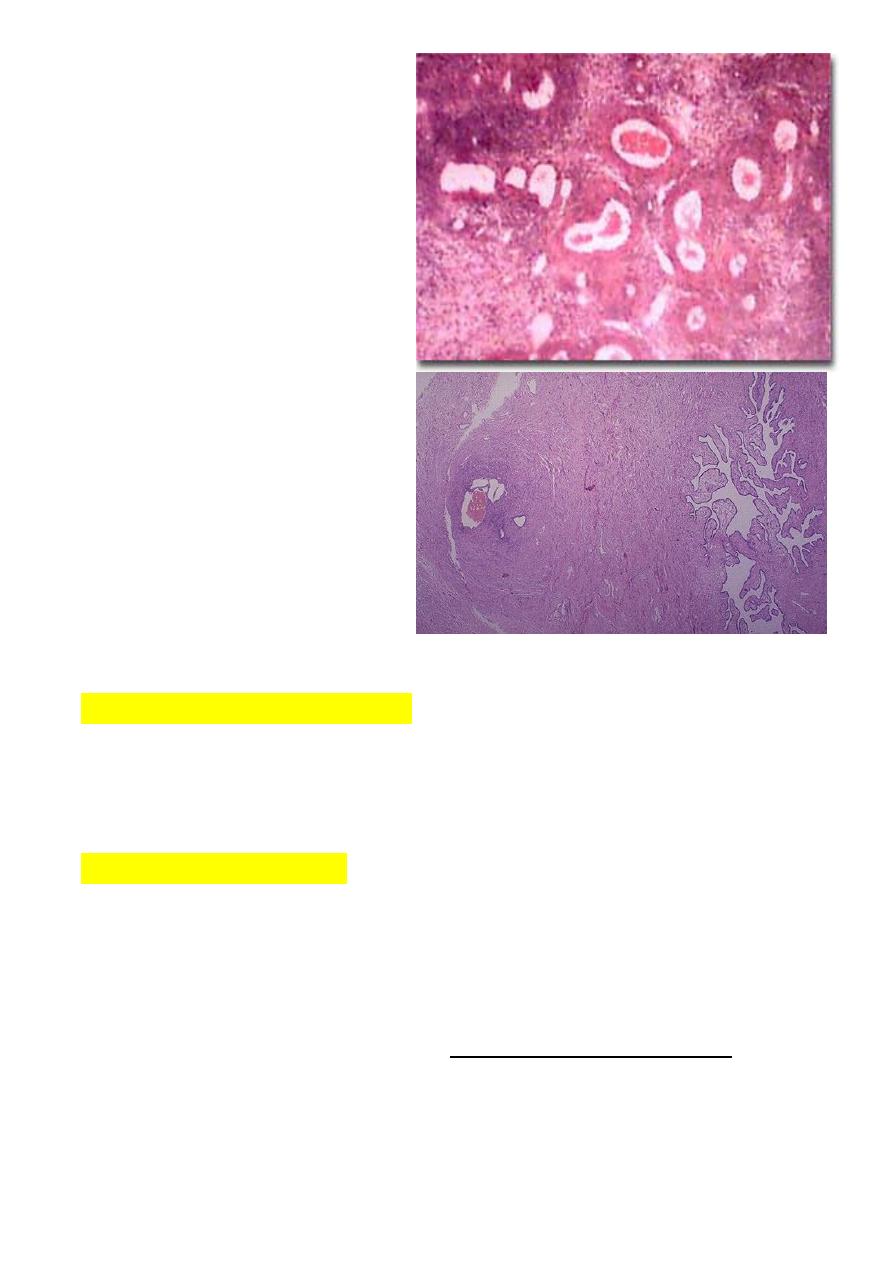
Microscopically:
Showed the typical endometrial
tubular glands and stroma cells.
a small cluster of endometrial glands
and stroma with hemorrhage are seen
at the left near the surface of the
fallopian tube. The lumen of the tube
is at the right. This is a focus of
endometriosis.
The squeal of endometriosis: It include:
1. chronic pelvic pain
2. severe dysmenorrhoea
3. infertility.
Sites of Endometriosis:
*
Endometriosis lesions most commonly found in the pelvic cavity.
on the surface of ovary, pelvic peritoneum, the fallopian tubes, on broad ligaments, the
pelvic sidewall, uterosacral ligaments, the Pouch of Douglas, and in the rectal-vaginal
septum.
*it can be found in caesarean-section scars,
laparoscopy or laparotomy scars, But these
locations are not so common.
*In even more rare cases, endometriosis has been found inside the vagina, inside the
bladder, bowel, intestines, colon, appendix, rectum, on the skin, even in the lung, spine,
and brain.
4
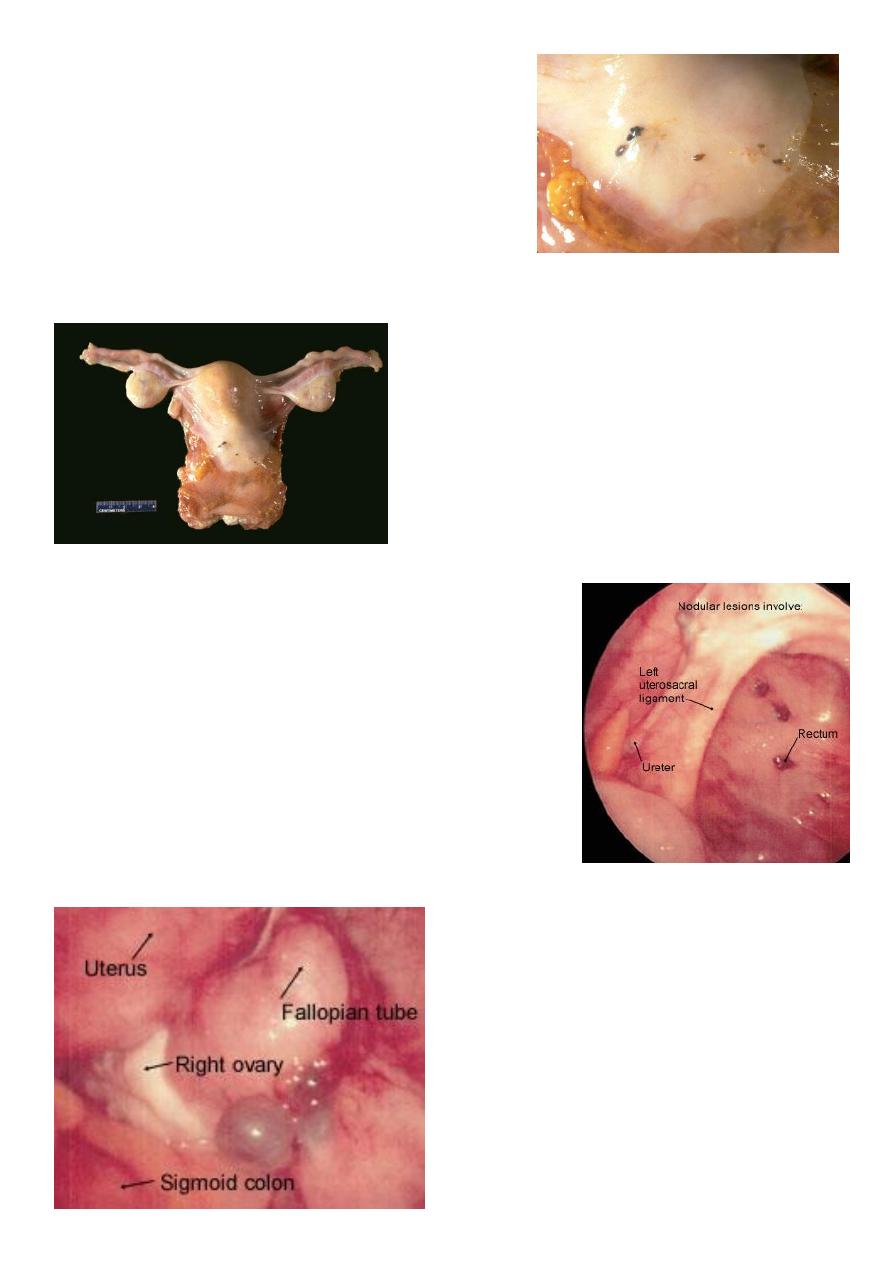
reddish-brown to bluish appearance.
the gross appearance of "powder burns". Small foci are seen
here just under the serosa of the posterior uterus in the
pouch of Douglas.
Nodular endometrial lesions in the posterior cul-de-sac.
Cystic implants adjacent to the right ovary; note bluish
appearance.
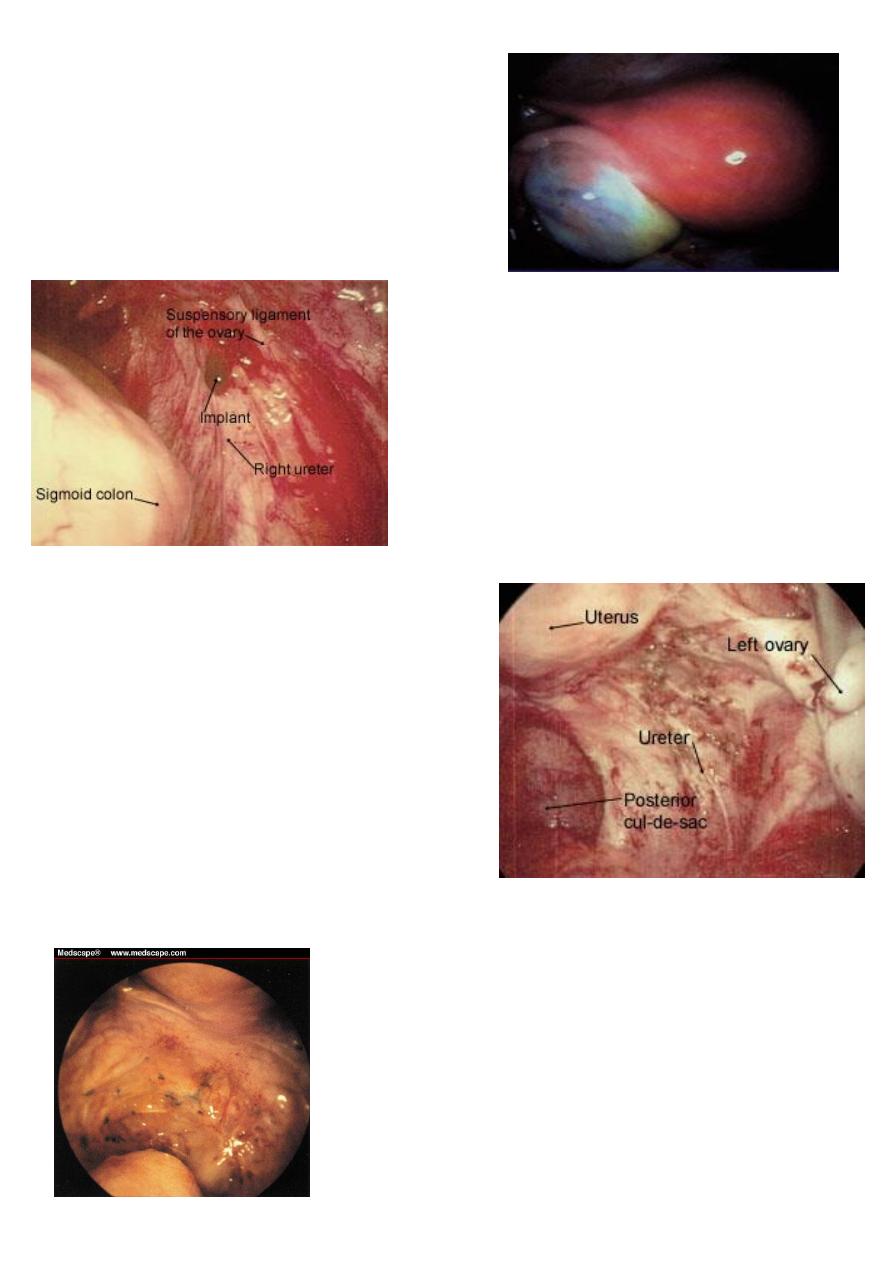
5
Ovary with endometrioma
Hemorrhagic lesions overlying the right ureter.
Extensive endometriosis in the ovarian fossa. Lesions have
a petechial appearance.
Diffuse endometriosis is seen in the cul-de-sac ,
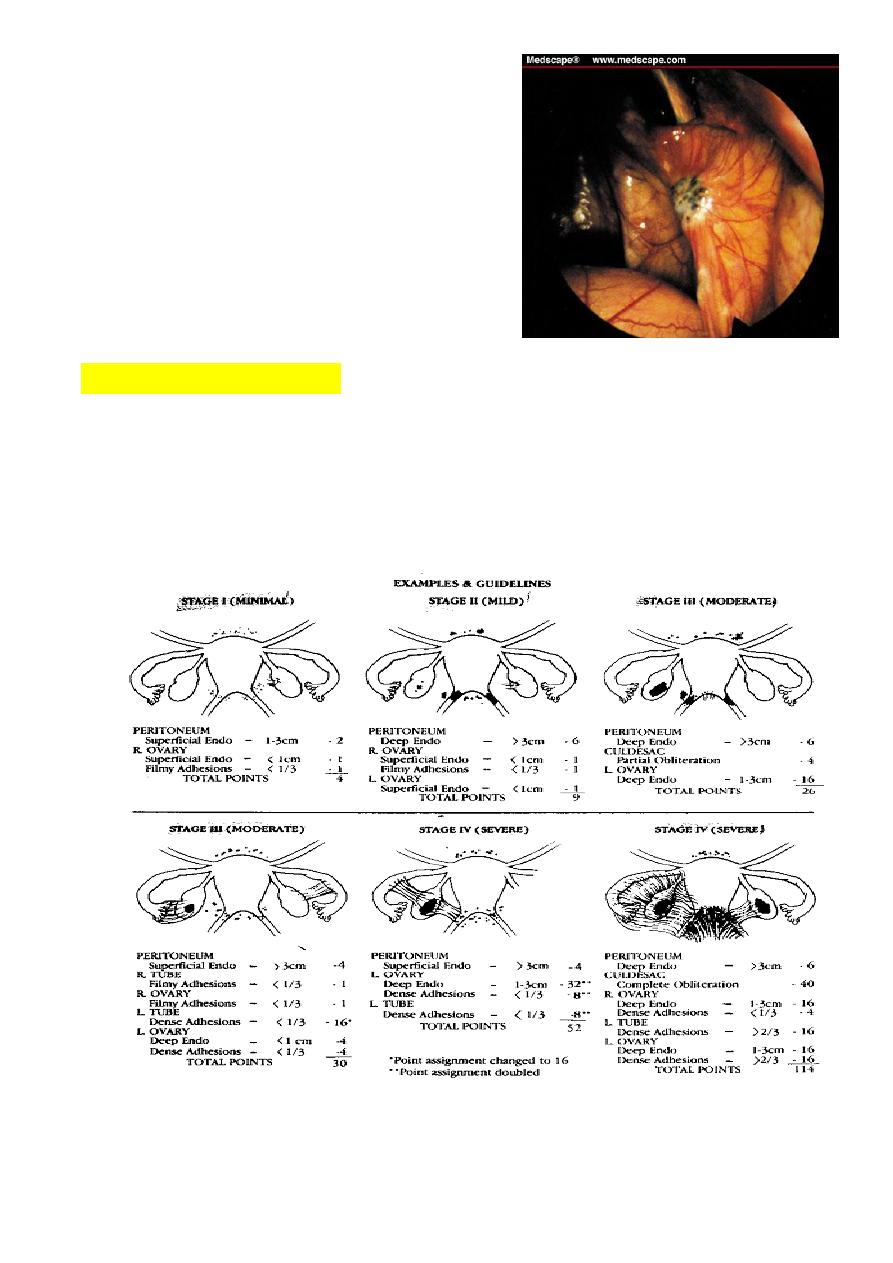
6
Puckered black lesions are typical of endometriosis
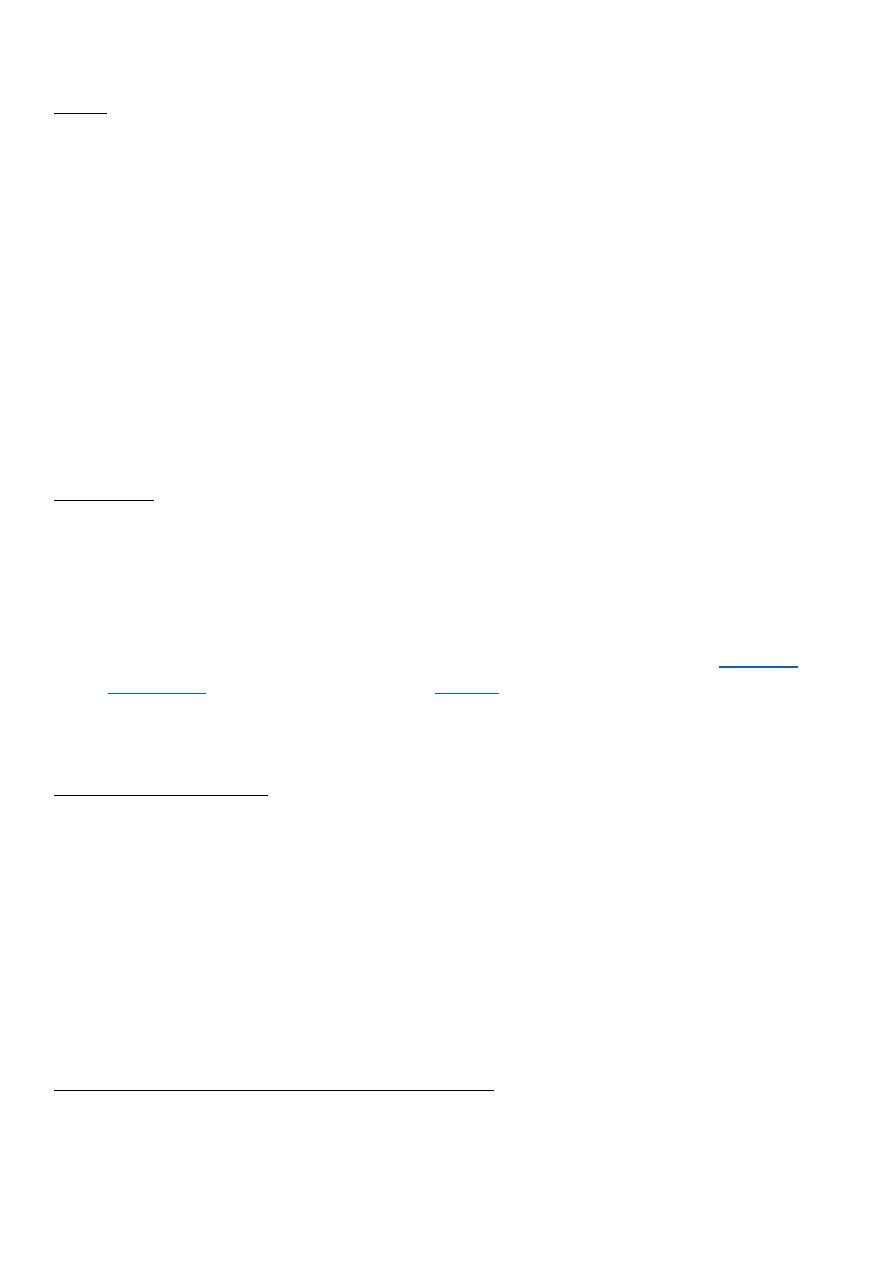
Classification systems:
The 4 stages (classification) of endometriosis (minimal, mild, moderate or severe) are
used to describe the anatomic location and the severity of the disorder. This system was
designed to assist in the prognosis and management of patients undergoing surgery for
infertility.

7
Risk Factors for Endometriosis:
A. Greater exposure to menstruation as in:
1. Increasing age (up to menopause).
2. Shorter menstrual cycle length (less than 27 days).
3. Longer duration of menstrual flow (greater than 7 days).
4. Heavy menstrual flow.
5. Delaying pregnancy until an older age.
6. Low or no parity.
B. First-degree relative (mother, sister, daughter) with endometriosis.
C. Increased peripheral body fat.
Factors which may be protective from developing endometriosis:
• Oral contraceptive use (current and recent) may be protective.
• Smoking.
• Exercise.
Clinical feature:
The typical patient with endometriosis is in her reproductive years, (commonly in her
30s) and characteristically are nulliparous, and infertile or delayed their child bearing.
Endometriosis never appears before puberty and it regresses after menopause.
Endometriosis is more commonly found in white women, tall, thin women with a low
body mass index (BMI).
Endometriosis is a common condition with many diverse manifestations and a clinical
course that is highly variable and unpredictable depending upon site and activity of the
disease.
Endometriosis should be suspected in any woman with the triad of dysmenorrhoea,
dysparunia and infertility.
Symptoms:
The symptoms of pelvic endometriosis depend on the site and the activity of the disease.
a. Asymptomatic:
many affected women are asymptomatic in which case the diagnosis is only made when
the pelvis is inspected for an unrelated reason, for example sterilization. One-third of
women with endometriosis are asymptomatic.
8
b. symptomatic:
1.Pain is the most common symptom, and many types of pain are found:
a. Severe secondary dysmenorrhoea.
b. severe deep dyspareunia.
c. ovulation pain is sometimes sever in mid cycle.
d. Pelvic discomfort, lower abdominal pain, backache.
e. acute abdominal pain in rupture ovarian endometriomas which leads to reactive
peritonitis which is acute abdominal emergency requiring laprotomy.
For many women, the pain of endometriosis is so severe and debilitating that it impacts
their lives in significant ways. The pain intensity can change from month to month, and
vary greatly among women. Some women experience progressive worsening of
symptoms, while others can have resolution of pain without treatment.
There is little correlation between disease stage and the type, nature and severity of pain
symptoms.
2. infertility may be the main complaint.
The reasons for a decrease in fertility are not completely understood, but might be due to
both:
a. The presence of endometriosis may distort normal anatomical structures, such as
fallopian tubes and may interfere with oocyte pick up.
b. production of hormones and substances that have a negative effect on
and/or implantation of the
Whether endometriosis causes subfertility or not is controversial. A causal relationship with
minimal–mild disease is much less certain.
3. Menstrual disturbance:
It can cause abnormal uterine bleeding:
a.Menorrhagia in case of :
adenomyosis
ovarian function is altered by bilateral endometriomas.
b. Irregular uterine bleeding.
c. Polymenorrohea. (short cycles)
d. Prolonged bleeding.
4. Other symptoms related to endometriosis include:

9
5. Rare symptoms of endometriosis include chest pain or coughing blood (haemoptisis) ?due
to endometriosis in the lungs and headache and/or seizures due to endometriosis in the brain.
Examination:
Physical examination should be performed during early menses, when implants are likely to
be largest and most tender.
A. most women with endometriosis have normal pelvic findings
B. The examination may reveal one or more of these which is suggestive of endometriosis:
*visible lesions (Bluish nodule) are seen in vagina or on cervix. Such nodules are reliably
detected when the examination is performed during menstruation. It confirm the diagnosis.
*adnexal and uterine tenderness.
*pelvic masses as Enlarged ovaries due to endometriomas.
*a fixed retroverted uterus (In advanced and destructive disease).
*nodularity and tenderness along the uterosacral ligaments.
*A rectovaginal examination is required to identify uterosacral, cul-de-sac or septal nodules.
Differential diagnosis:
1. Adenomyosis.
2. Pelvic Inflammatory Disease (PID).
3. Uterine fibroid .
4. Carcinoma of ovary.
5. Carcinoma of colon or rectum.
6. Pelvic congestion syndrome.
Differential diagnosis to Rupture of endometriotic cyst which
presents as an acute abdominal emergency are:
1. Rupture ectopic pregnancy.
2. Ovarian cyst torsion.
3. Ovarian cyst haemorrhage.
4. Acute salpingitis.
5. Other causes of acute abdomen.