Atherosclerosis
Saadeldeen majeedProfessor of cardiology and internal medicine
2
Pathogenesis of Atherosclerosis
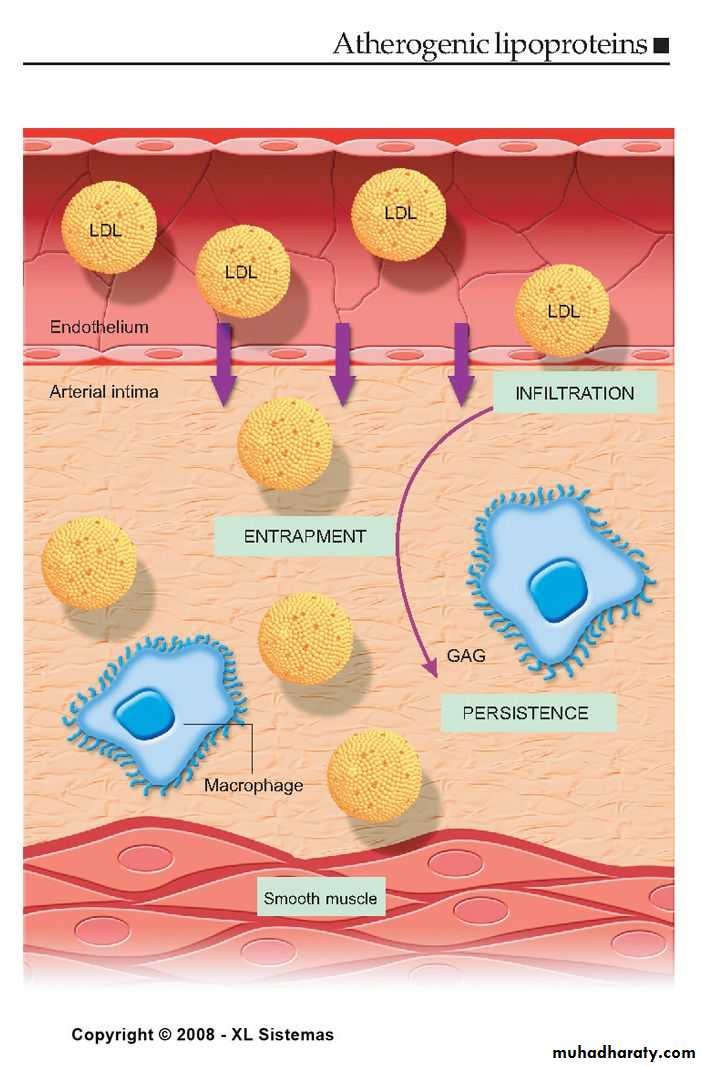
According to injury hypothesis considers atherosclerosis to be a diffuse, slowly progressing, chronic inflammatory response of the arterial wall initiated by injury:
3
Pathogenesis of Atherosclerosis
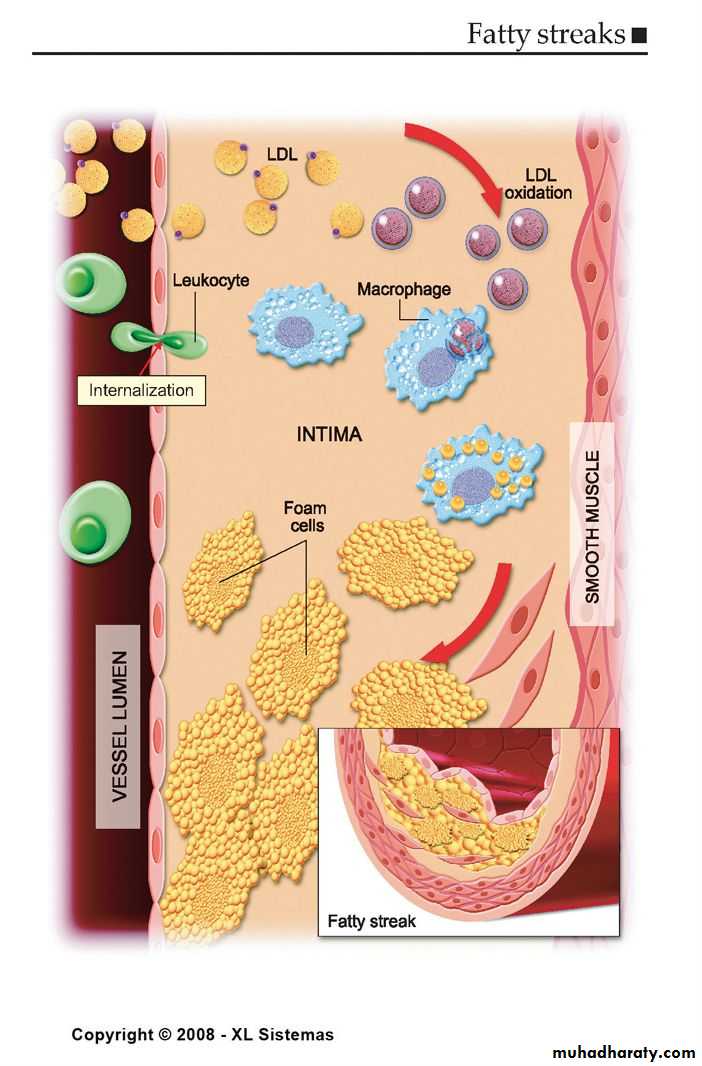
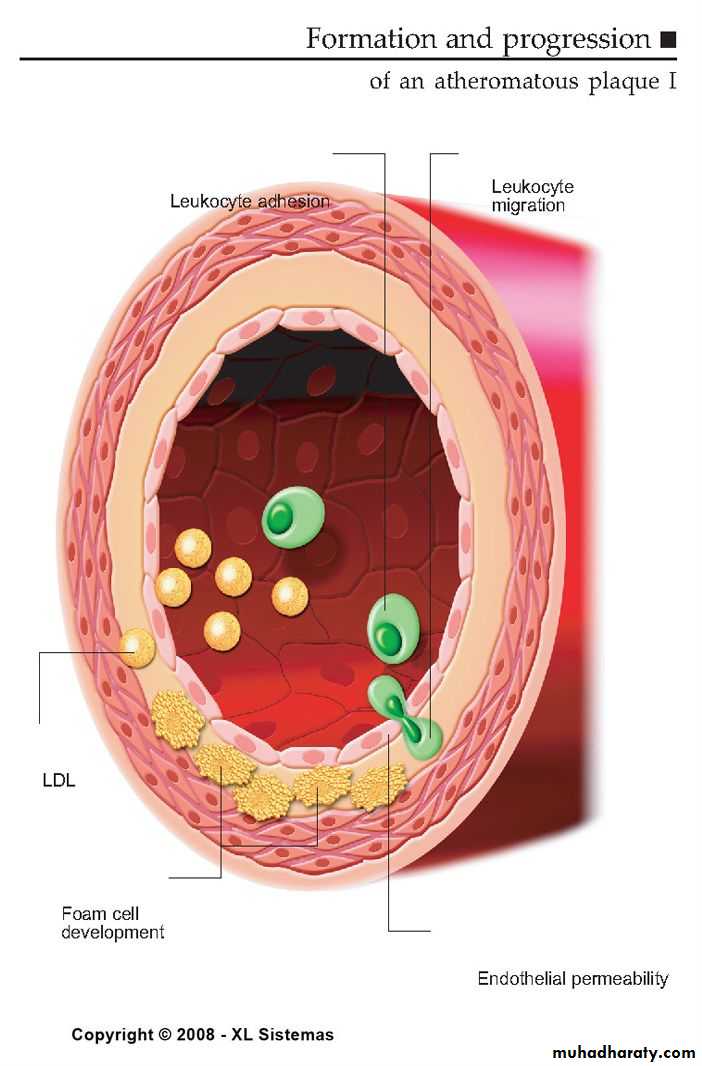
1. Chronic endothelial injury.
2 .Insudation of lipoproteins [LDL].
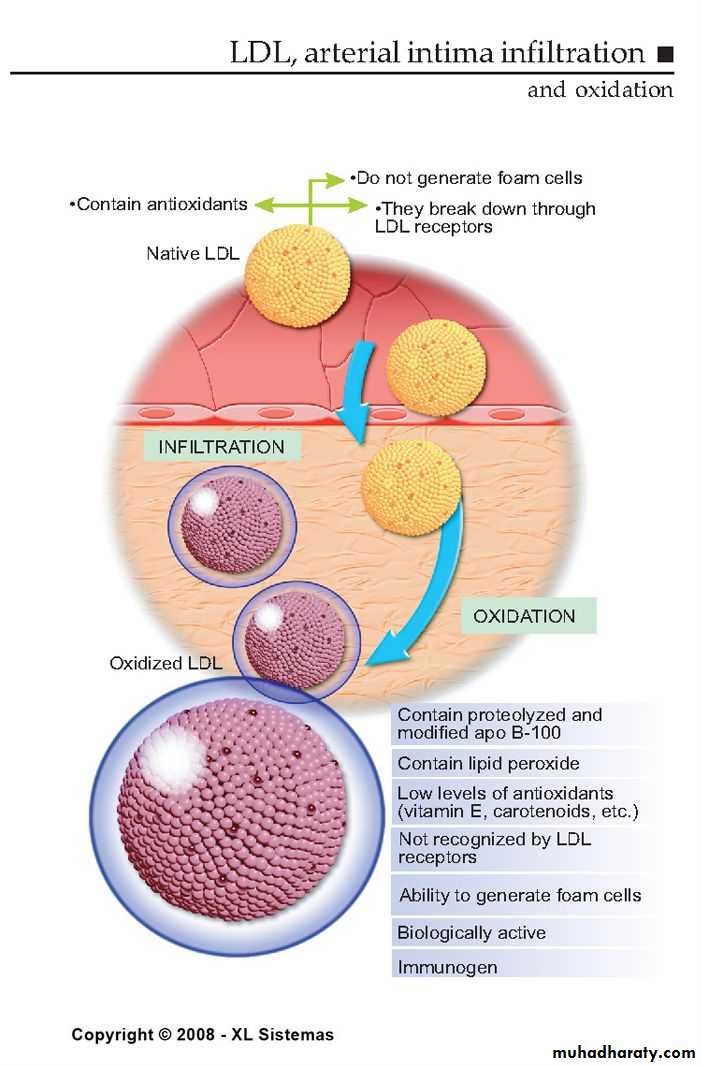
3. Modification of lipoproteins by oxidation.
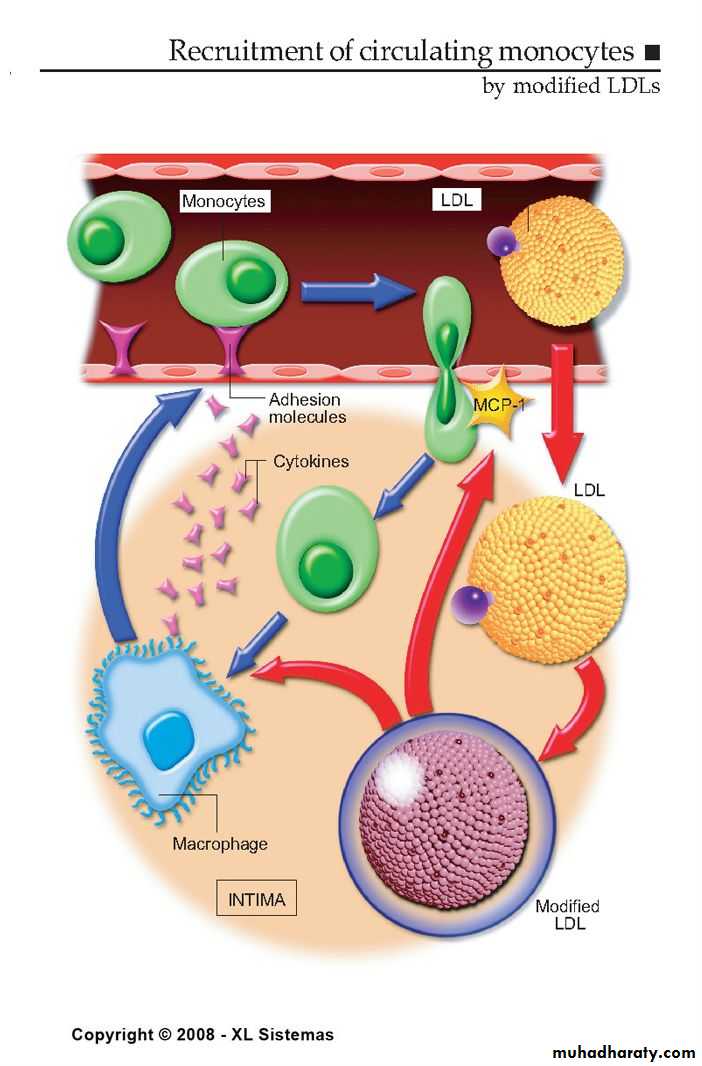
4. Adhesion of blood monocytes.
5. Adhesion of platelets.
4
Pathogenesis of Atherosclerosis
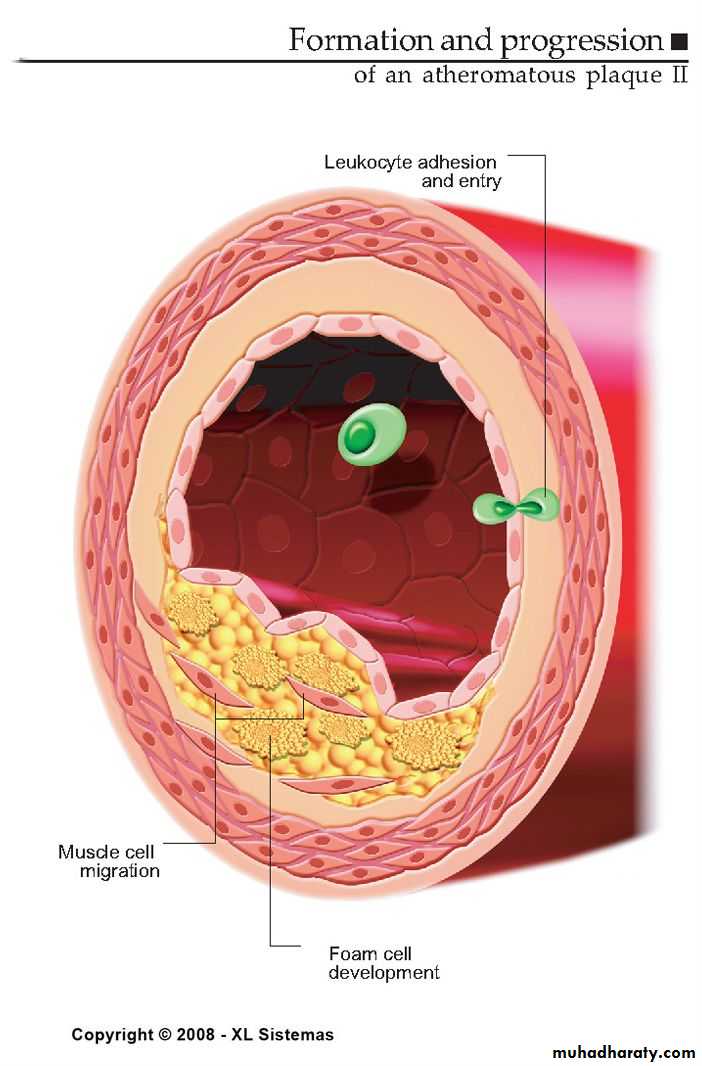
6. migration of smooth muscle cells
from the media into the intima.
7. proliferation of smooth muscle cells
in the intima.
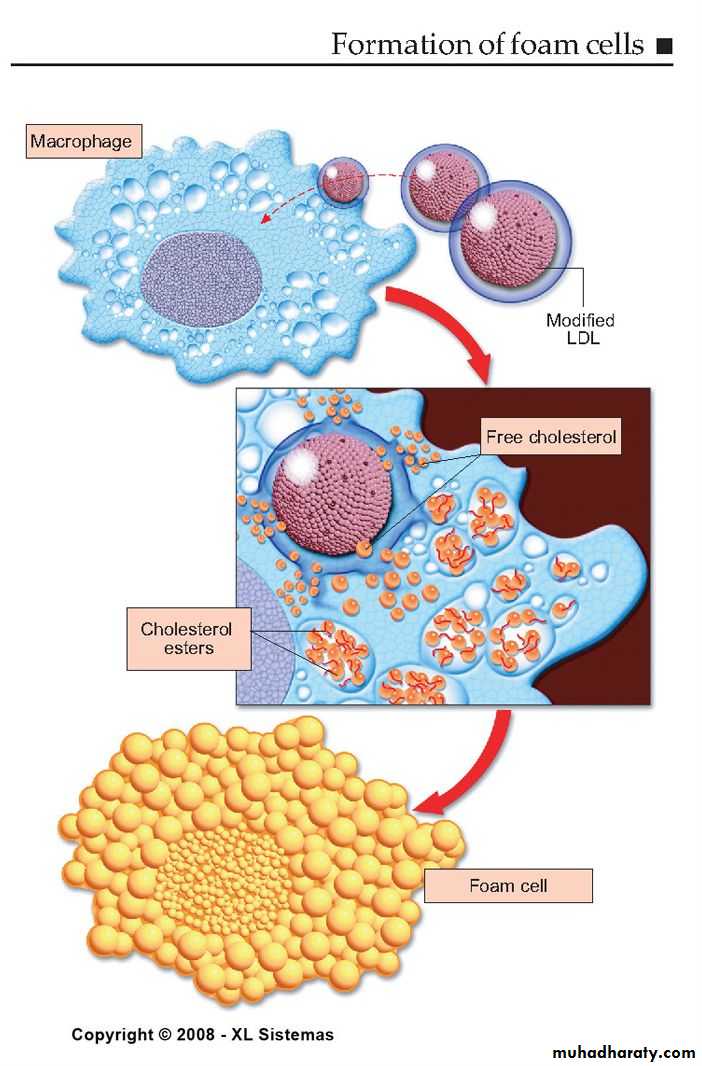
8. enhanced accumulation of intra and
extra cellular lipids.
5
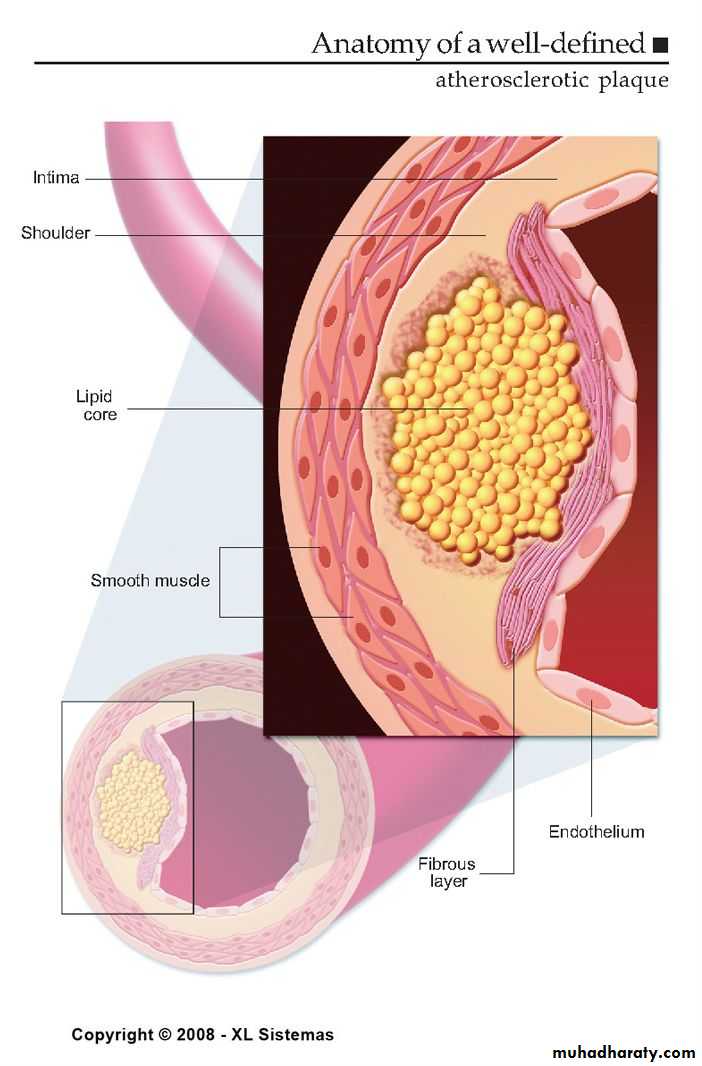
ATHEROSCLEROTIC PLAQUE
The change of the large arterial intima is called atherosclerotic plaque or atheroma
atherosclerotic plaque is the intimal thickening with lipid accumulation
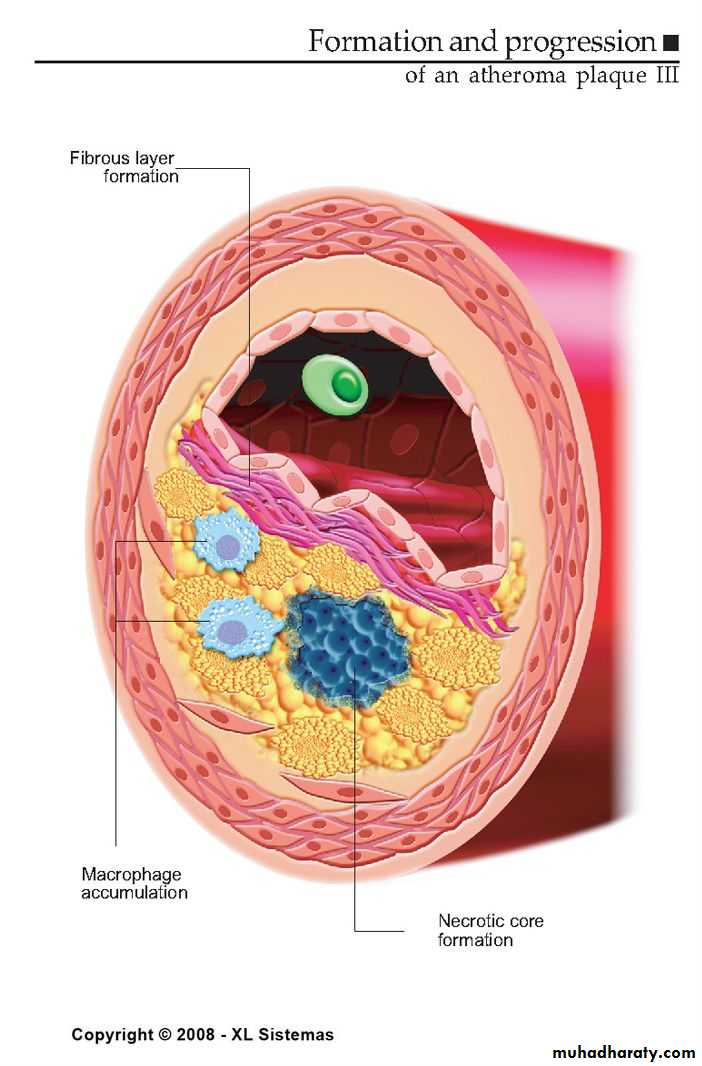
It consists of fibrous cap, necrotic core and fibrous basis.
6Atherosclerotic plaque
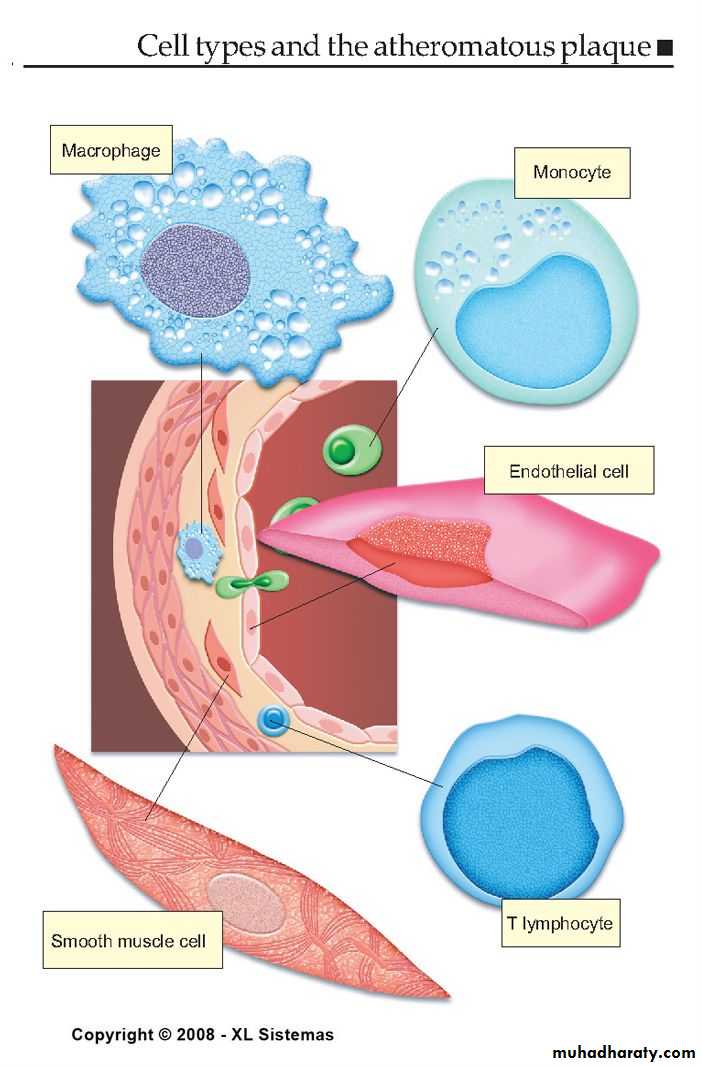
• It has three principle components:
• 1- cells –smooth muscle cells, macrophages,
• other leukocytes.
• 2 - Extra cellular matrix- collagen, elastic fibers,
• and proteoglycans.
• 3 - Intra cellular and extra cellular lipids.
Normal coronary artery
Lumen has been distended at a pressure of 100mmHg with 10% formal saline
used with permission from
M.J. Davies
Atlas of Coronary Artery Disease 1998
Lippincott-Raven Publishers
used with permission from
M.J. DaviesAtlas of Coronary Artery Disease 1998
Lippincott-Raven Publishers
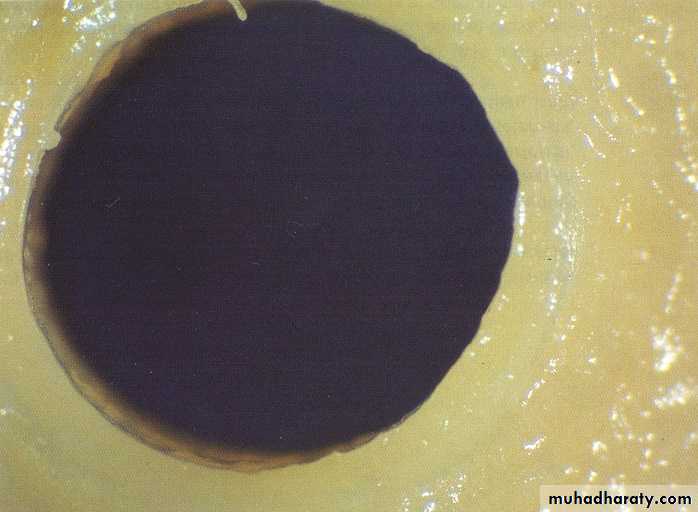
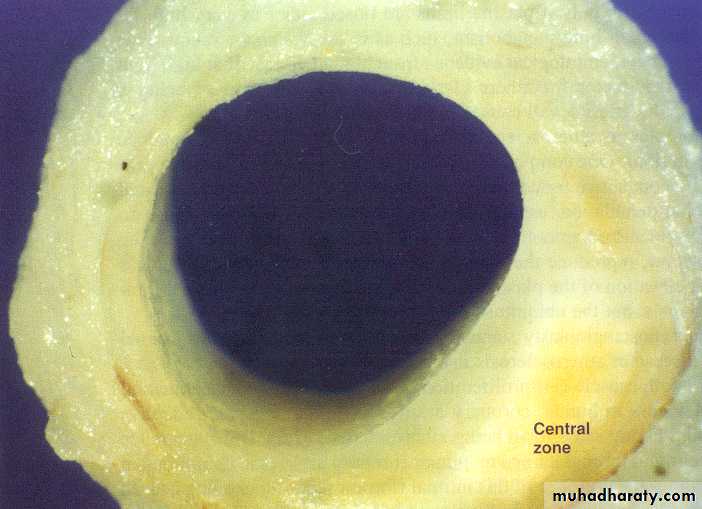
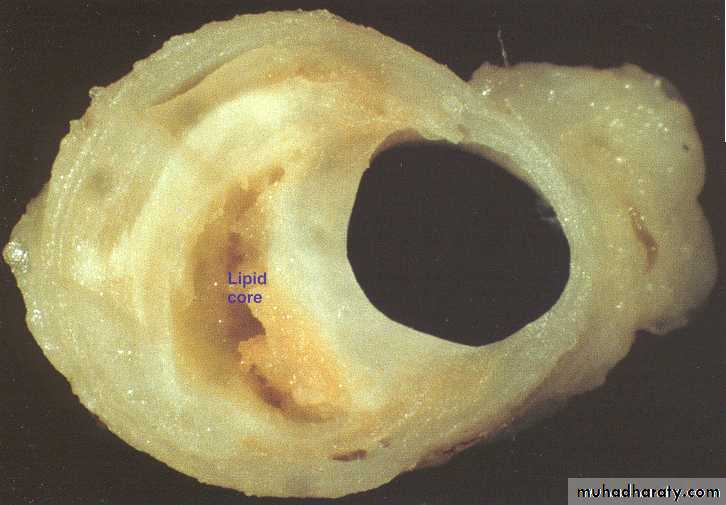
Early coronary atherosclerosis
Eccentric plaque with a central zone containing yellow lipid
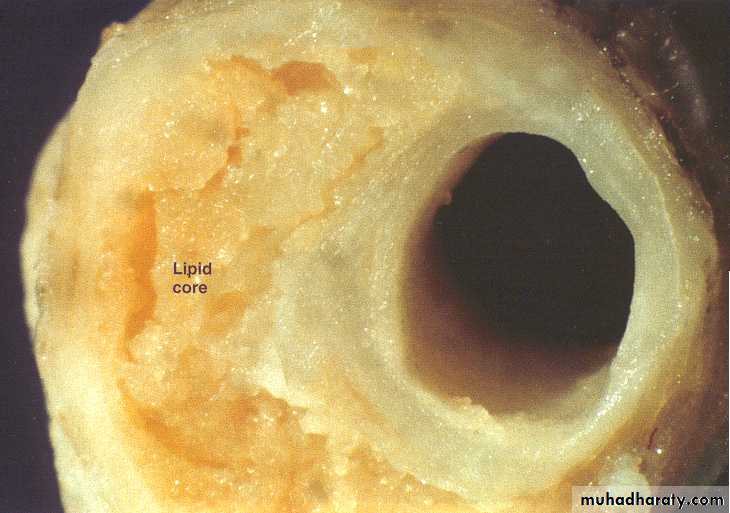
Stable angina. Eccentric coronary stenosis
used with permission fromM.J. Davies
Atlas of Coronary Artery Disease 1998
Lippincott-Raven Publishers
Stable angina. Eccentric coronary stenosis
used with permission from M.J. DaviesAtlas of Coronary Artery Disease 1998
Lippincott-Raven Publishers
thick cap

Unstable angina with
plaque disruptionused with permission from M.J. Davies
Atlas of Coronary Artery Disease 1998
Lippincott-Raven Publishers

Unstable angina with plaque disruption
used with permission fromM.J. Davies
Atlas of Coronary Artery Disease 1998
Lippincott-Raven Publishers
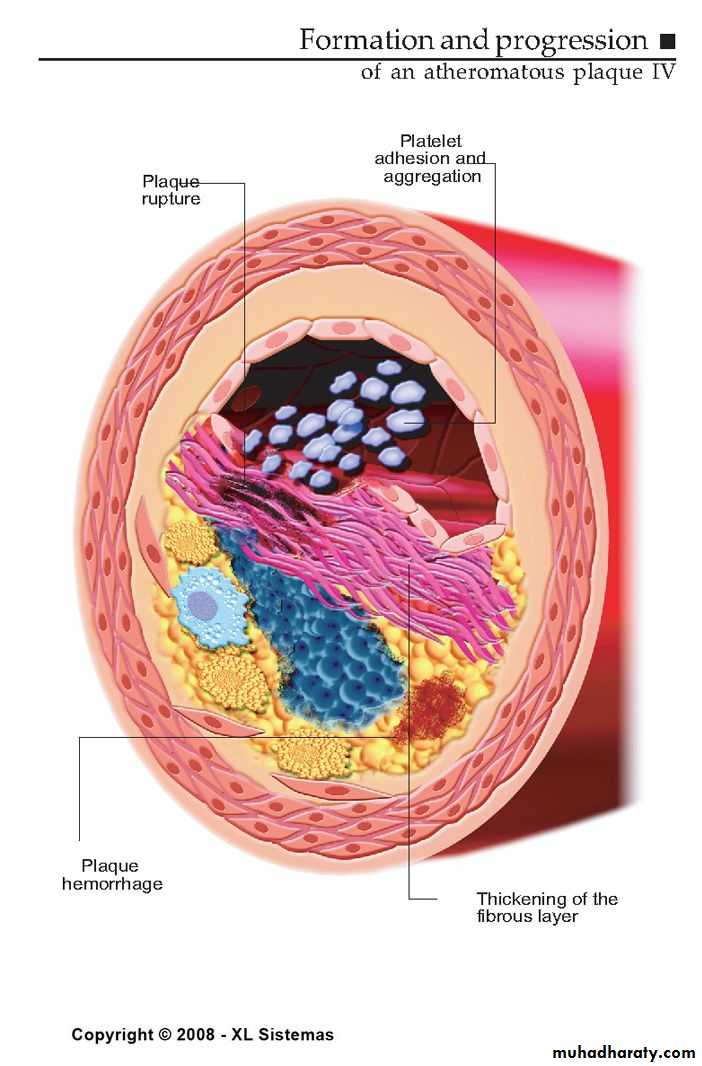
The plaque cap is torn,
projects into the lumen, exposing a mass of thrombus filling the lipid core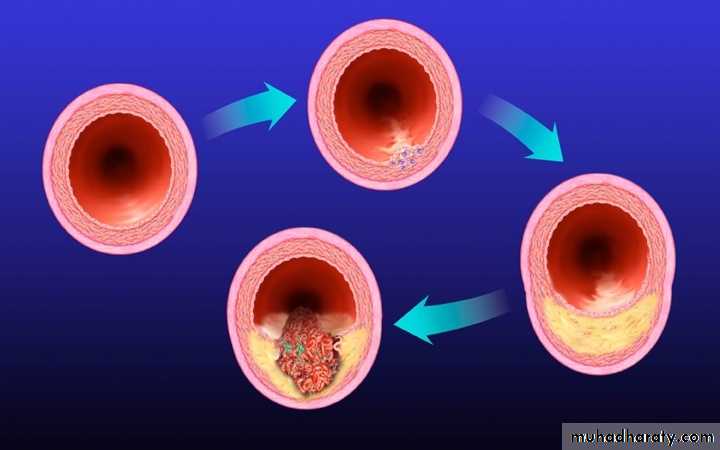
Development of Atherosclerotic Plaques
NormalFatty streak
Foam cells
Lipid-rich plaque
Lipid core
Fibrous cap
Thrombus
Ross R. Nature. 1993;362:801-809.
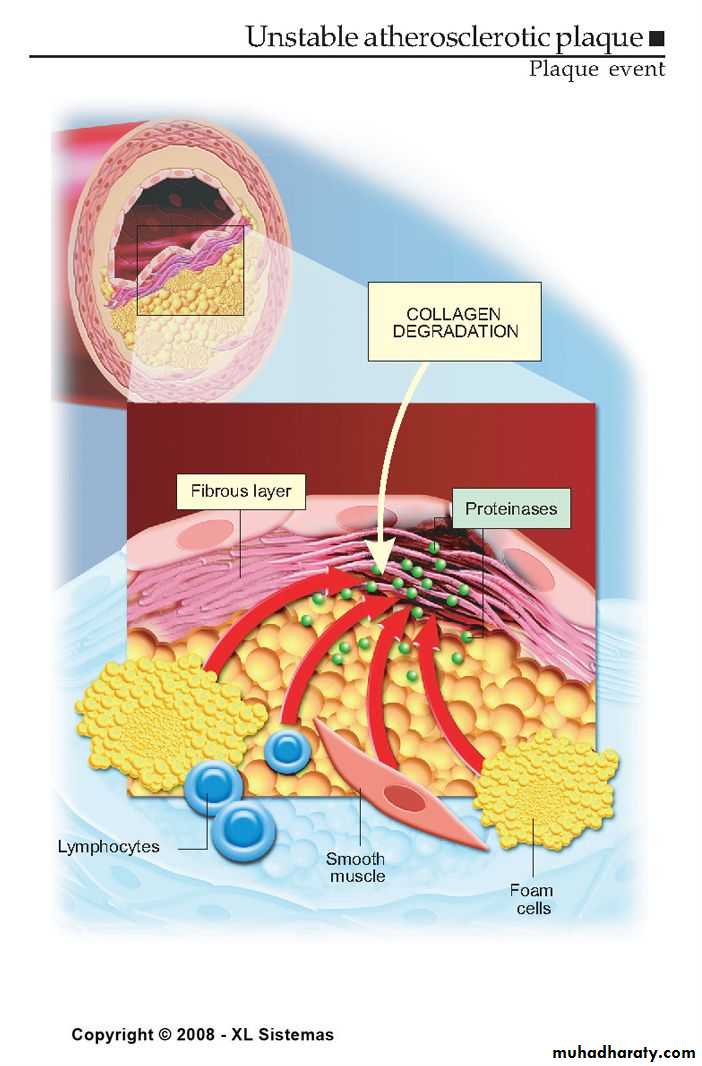
Libby P. Circulation. 1995;91:2844-2850.Vulnerable Plaque
Thin fibrous cap
Inflammatory cell infiltrates:
proteolytic activity
Lipid-rich plaque
Lumen
Lipid
Core
Fibrous Cap
Thick fibrous capSmooth muscle cells: more extracellular matrix
Lipid-poor plaque
Stable Plaque
Lumen
LipidCore
Fibrous Cap
Vulnerable Versus Stable Atherosclerotic Plaques
Major modifiable Risk FactorsCigarette smoking (passive smoking?)
Elevated total or LDL-cholesterol
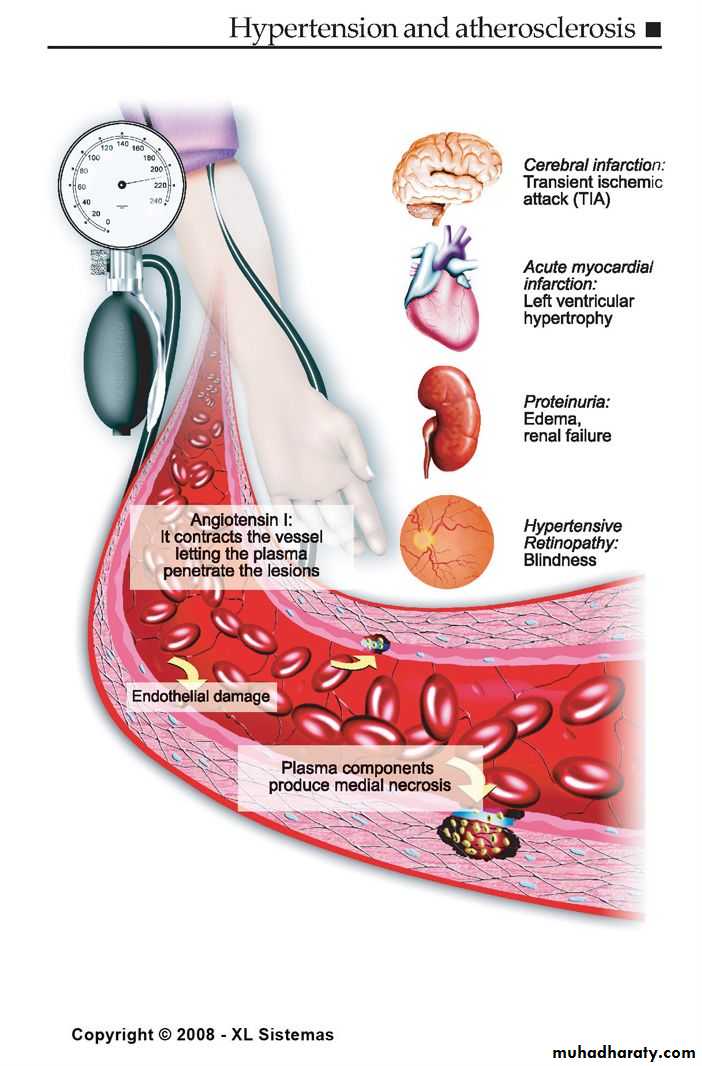
Hypertension (BP 140/90 mmHg or on antihypertensive medication)
.. Low HDL cholesterol (<40 mg/dL)†
Obesity: Body Mass Index (BMI)
Weight (kg)/height (m2)
Weight (lb)/height (in2) x 703
Obesity BMI >30 kg/m2 with overweight defined as 25-<30 kg/m 2
Abdominal obesity involves waist circumference >40 in. in men, >35 in. in women
Physical inactivity: most experts recommend at least 30 minutes moderate activity at least 4-5 days/week
• † HDL cholesterol 60 mg/dL counts as a “negative” risk factor; its presence removes one risk factor from the total count.
Nonmodifiable Risk Factors
Age- Age (men 45 years; women 55 years)the older you get, the greater the chance.
Sex- males have a greater rate even after women pass menopause.
Race- minorities have a greater chance.
Family history- if family members have had CHD, there is a greater chance. Family history of premature CHD
• CHD in male first degree relative <55 years
• CHD in female first degree relative <65 years
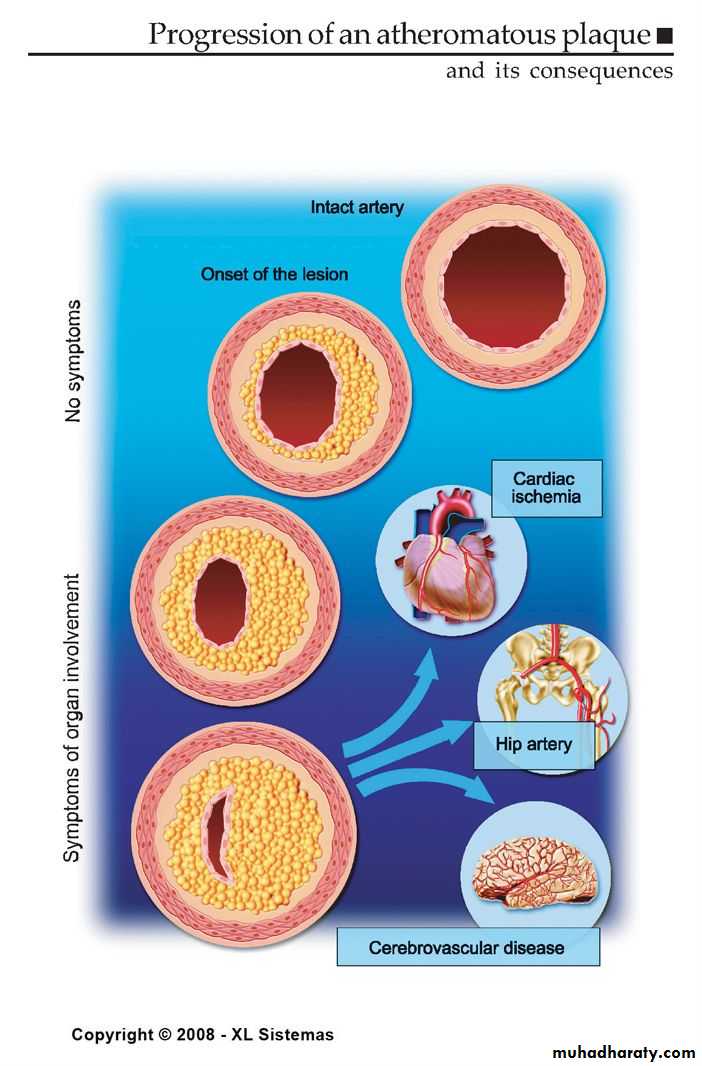
Clinical Manifestations of Atherosclerosis
Coronary heart diseaseStable angina, acute myocardial infarction, sudden death, unstable angina
Cerebrovascular disease
Stroke, TIAs
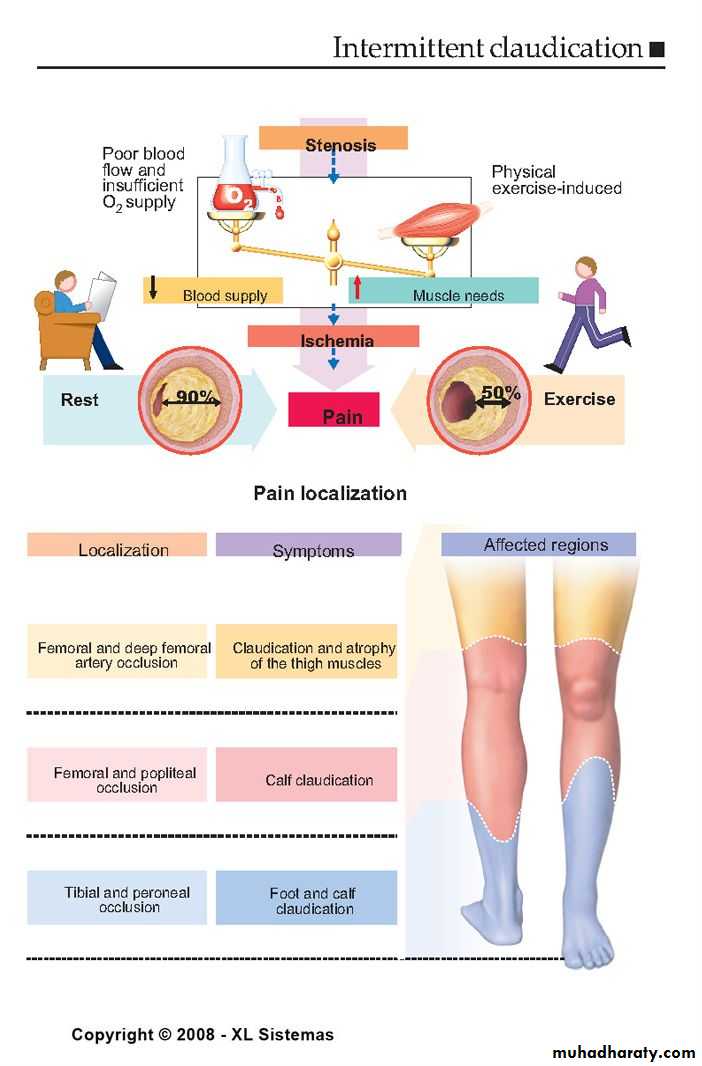
Peripheral arterial disease
Intermittent claudication, increased risk of death from heart attack and stroke
American Heart Association, 2000.
31
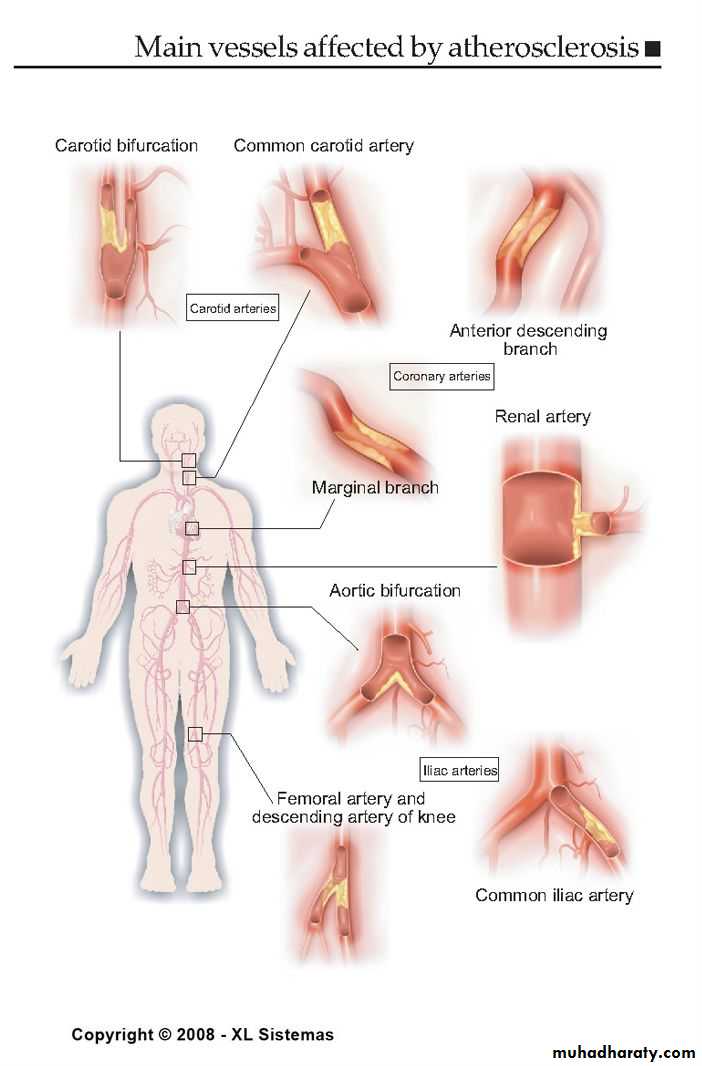
FORMS OF ATHEROSCLEROSIS
CEREBRAL ARTERIES INJURY
CARDIAC ARTERIES INJURY
RENAL ARTERIES INJURY
AORTA INJURY
INTESTINAL ARTERIES INJURY
EXTREMITY ARTERIES INJURY
What Does It Look Like?
The coronary artery is narrowed reducing the flow of oxygen to the heart.It is easier for plaque to get inside a narrower artery.
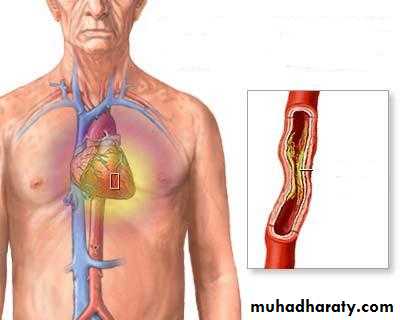
34
CEREBRAL FORM OF ATHEROSCLEROSIS
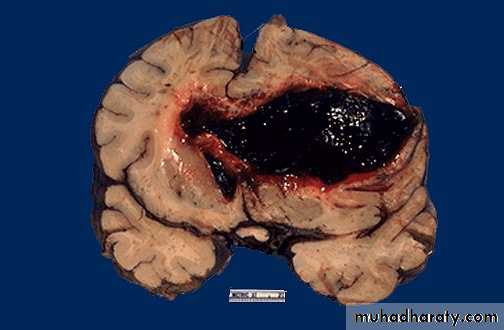
Acute form may be as Hemorrhage within
The brain due to rupture
Of atherosclerotic aneurism
35
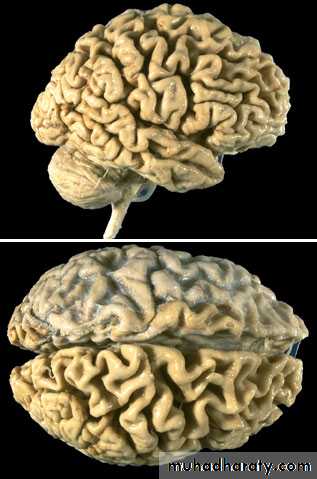
CEREBRAL FORM OF ATHEROSCLEROSIS
Chronic form may be as encephalopathy
With cerebral atrophy (decreasing memory)
36
Extremity form of atherosclerosis
Acute form may be as gangrenous necrosis.

38
Aortic form of atherosclerosis

Various forms of aorta lesion
39RENAL FORM OF ATHEROSCLEROSIS
Acute form may be as infarction
Chronic form is called
AtheroscleroticNephrosclerosis or
Primary contracted
kidney


40
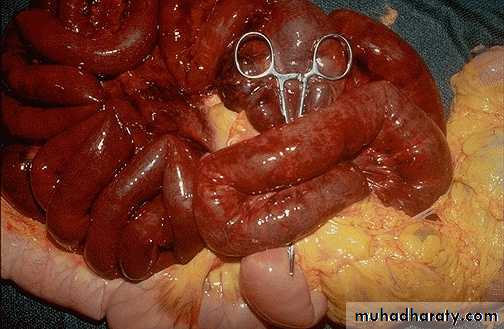
Intestinal form of atherosclerosis
Acute form may be as gangrenous necrosis of the intestine
Chronic form may be as ischemic enterocolitis

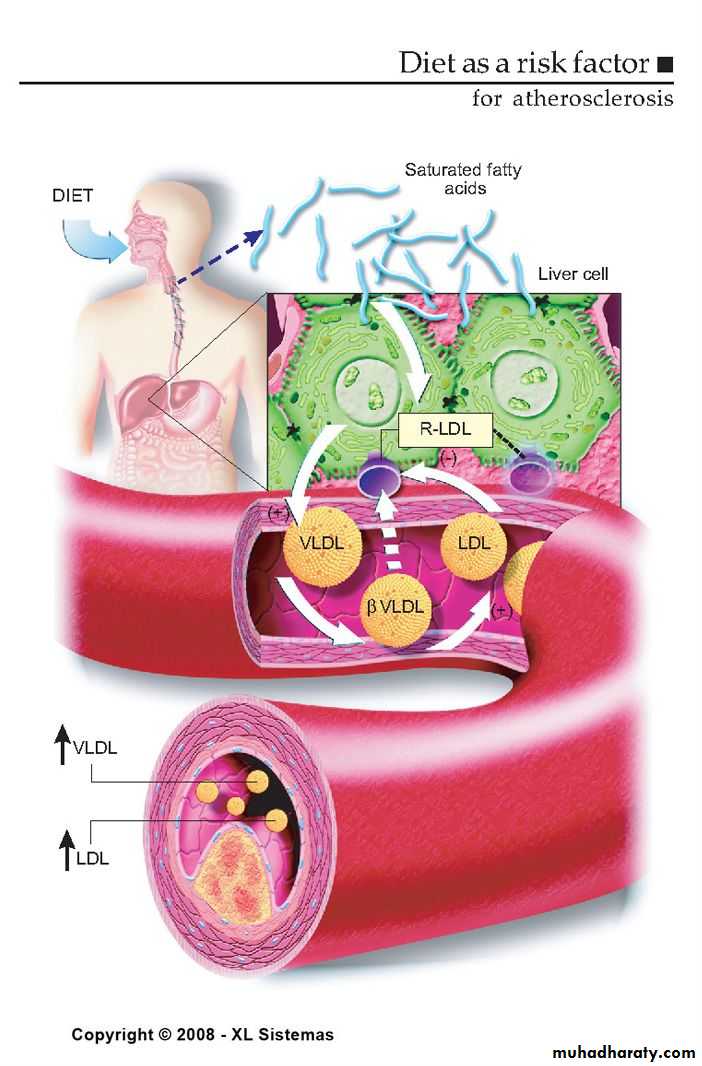

The Skinny on Fat
Saturated fats- basically means the fat is saturated with hydrogen, they are solid at room temperature. Examples are lard and butter.Why are they bad for you? They increase levels of LDL , decrease HDL and increase total cholesterol.
The Skinny on Fat
What are monounsaturated fats?
They are liquid at room temperature but start to solidify in the refrigerator.
Decrease total cholesterol and lower LDL levels.
The Skinny on Fat
What are trans fatty acids? They are unsaturated fats but they tend to raise total and bad cholesterol.Where do you find them?
In fast-food restaurants
Commercial baked goods. Examples: doughnuts, potato chips, cupcakes.
What about Omega 3?
Type of polyunsaturated fat.Consistently lowers serum triglycerides and may also have an effect on lowering blood pressure.
Found in oily fish such as salmon, tuna, and herring.
Is available as a supplement.
Physical Inactivity
Increasing physical activity has been shown to decrease blood pressure.
Moderate to intense physical activity for 30-45 minutes on most days of the week is recommended.
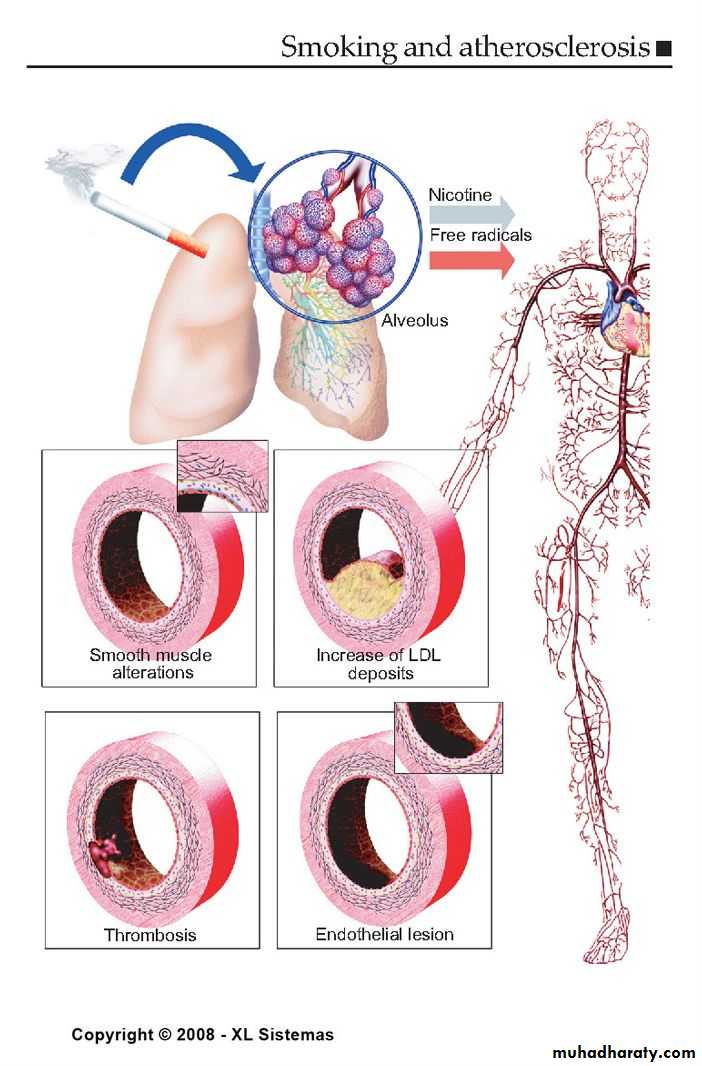
Cigarette Smoking
Causes an increase in blood pressureUsually have lower levels of HDL
Within 1 year of quitting, CHD risk decreases, within 2 years it reaches the level of a nonsmoker.
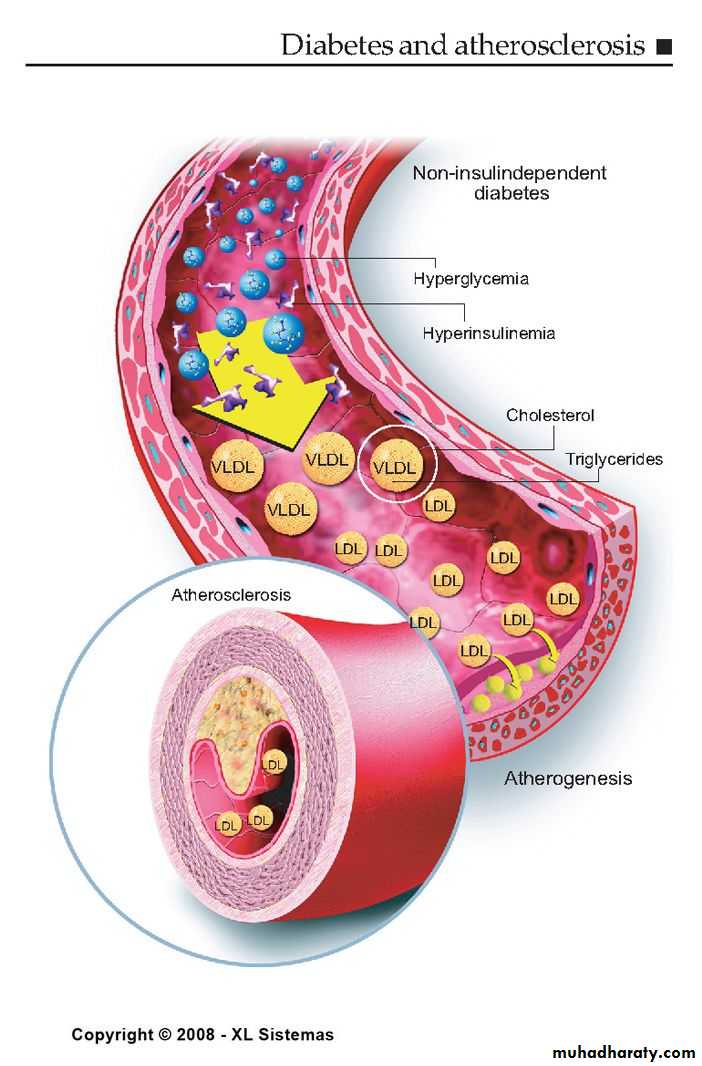
Diabetes Mellitus
At any given cholesterol level, diabetic persons have a 2 or 3 x higher risk of atherosclerosis!Insulin is required to maintain adequate levels of lipoprotein lipase, an enzyme needed to break down bad cholesterols.
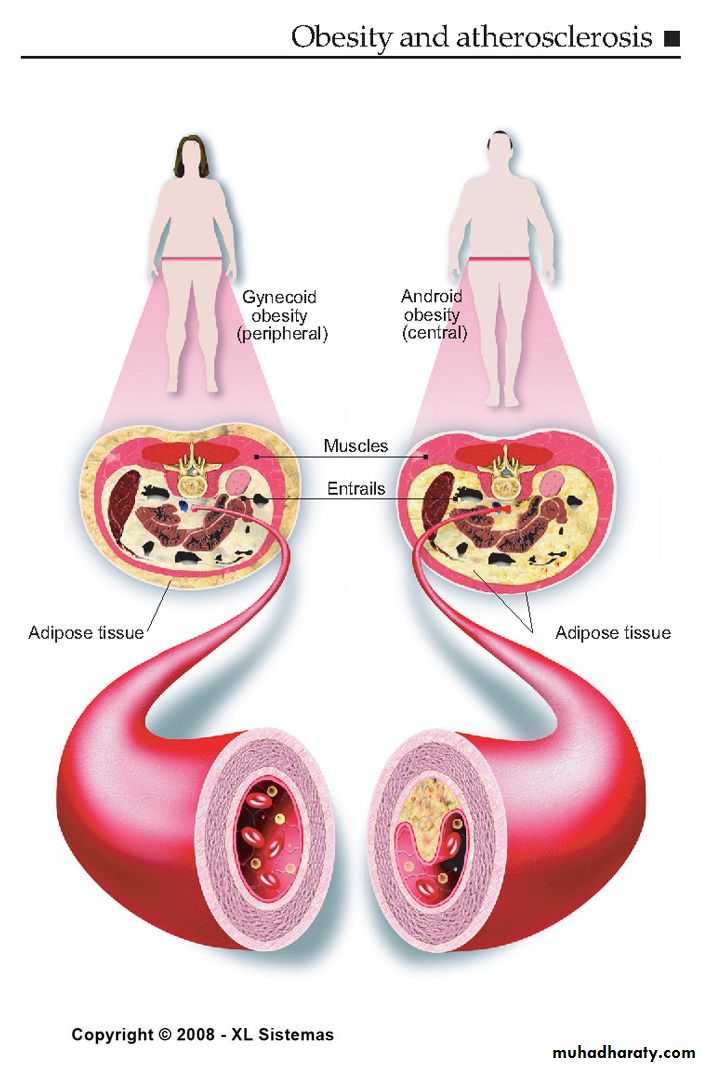
Obesity
People who are obese have 2 to 6 times the risk of developing hypertension.Location of the body fat is significant.
Pears of apples?
Approaches to Primary and Secondary Prevention
Primary prevention involves prevention of onset of disease in persons without symptoms.Primordial prevention involves the prevention of risk factors causative o the disease, thereby reducing the likelihood of development of the disease.
Secondary prevention refers to the prevention of death or recurrence of disease in those who are already symptomatic
Prevention
Get regular medical checkups.
Control your blood pressure.
Check your cholesterol.
Don’t smoke.
Exercise regularly.
Maintain a healthy weight.
Eat a heart-healthy diet.
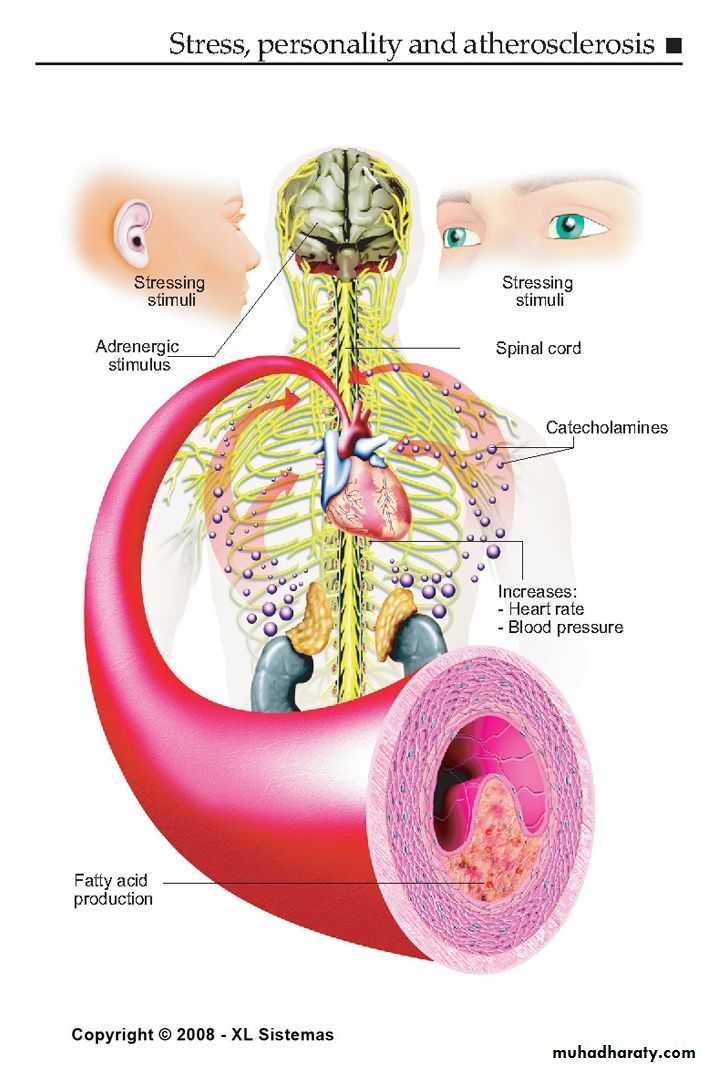
Manage stress.