1
Edwards' syndrome
Edwards' syndrome (trisomy 18):
It is the second most common autosomal trisomy, occurring in approximately 1 in 7500
live births.
Greater than 95% of conceptuses with trisomy 18 are spontaneously aborted in the
first trimester.
Trisomy 18 is usually lethal, less than 10% of affected infants survive until their first
birthday.
The diagnosis is confirmed by chromosome analysis.
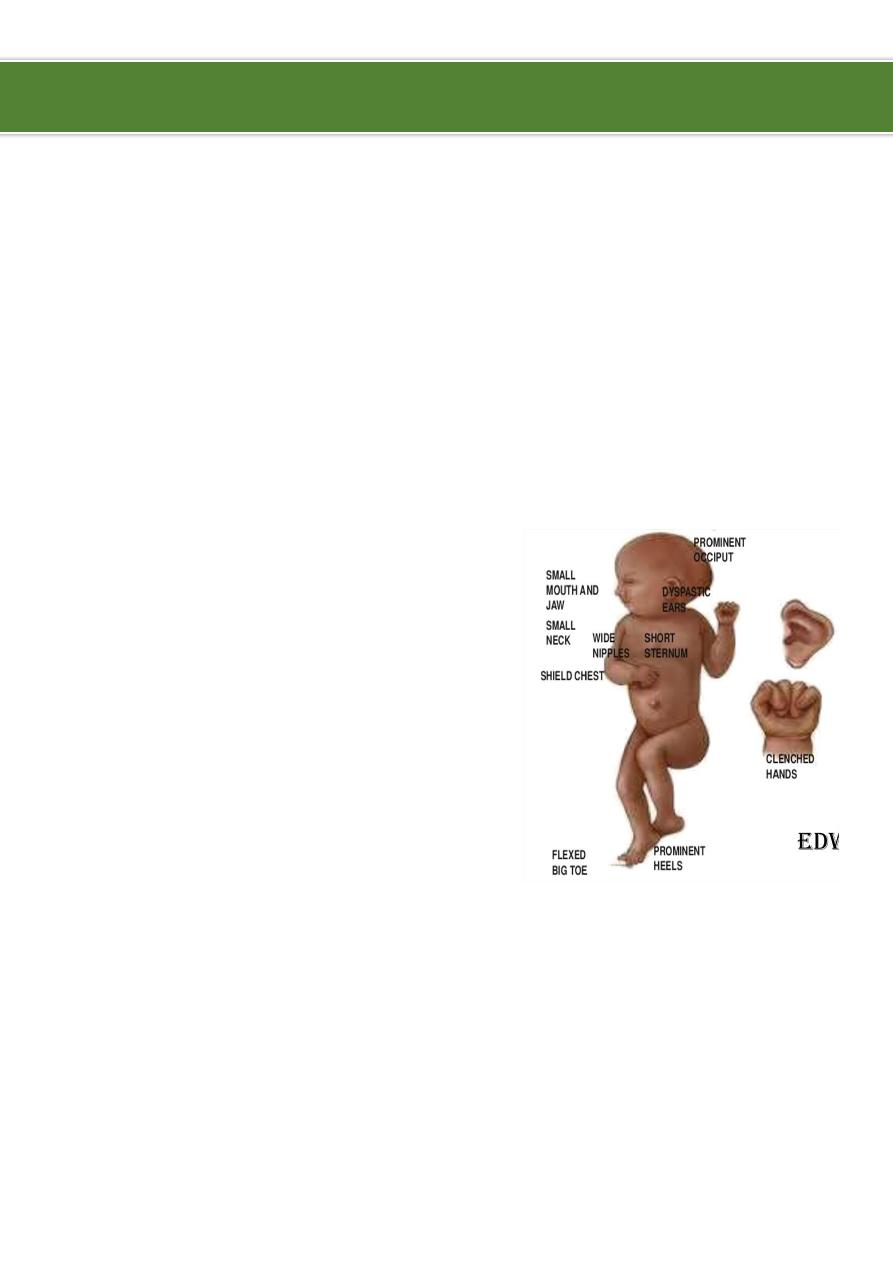
Clinical Features:
Low birth weight.
Prominent occiput.
Small mouth and chin.
Cleft lip or palate.
Low set & malformed ears.
Short sternum.
Flexed, overlapping fingers.
Rocker-bottom feet.
Cardiac and renal malformations.
Severe developmental delays.
Management:
Neonatal intensive care (NICU) management:
o
Resuscitation, respiratory support, and surgical procedures.
Medical care:
o
A goal-directed management plan based on careful risk-benefit assessment for the
individual patient and developed collaboratively between health professionals and
parents is recommended.
o
Treat infections as appropriate (RTI, UTI, Sepsis).
o
Provide nasogastric and gastrostomy supplementation for feeding problems.
o
Orthopedic management of scoliosis may be needed secondary to hemivertebrae.
Ibnlatef
Notes
Pediatrics

2
Cardiac management is primarily medical:
o
Most of these children require a diuretic and digoxin for congestive heart failure.
o
Intensive cardiac management with pharmacological intervention for ductal
patency (indomethacin and/or mefenamic acid for closure, and prostaglandin E1 for
maintenance).
o
Palliative and corrective cardiac surgery was demonstrated to improve survival.
Genetic counseling:
o
Recurrence risk is 1% or less for full trisomy 18.
o
If a parent is a balanced carrier of a structural rearrangement, the risk is
substantially high.
o
Patients with large 18q duplications or "partial trisomy 18" could benefit from the
same routine ultrasonographic screening for Wilms tumor as those with full trisomy
18, because early detection is essential to optimizing survival.
Psychosocial management:
o
Parents need information about the syndrome, including its cause, implications,
and possible outcomes.
o
Support services within the hospital and in the community should be made
available to the family.
Surgical care:
o
Because of the extremely poor prognosis, surgical repair of severe congenital
anomalies such as esophageal atresia or congenital heart defects may not be
considered and should be discussed with parents.
Diet:
o
No special diet is required.
Activity:
o
Activities are limited because of profound mental retardation and physical
handicaps.
----------------------------------------------------------------------------------------------
www.facebook.com/ibnlatef
https://goo.gl/RpvNsl